
14 results
PP129 Health Technology Assessment Adaptation: Pharyngolaryngeal Biopsies (OLB) For People with Suspected Head and Neck Cancer in the Outpatient Setting
-
- Journal:
- International Journal of Technology Assessment in Health Care / Volume 39 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 14 December 2023, p. S86
-
- Article
-
- You have access
- Export citation
Attribution of nosocomial seeding to long-term care facility COVID-19 outbreaks
-
- Journal:
- Epidemiology & Infection / Volume 151 / 2023
- Published online by Cambridge University Press:
- 25 October 2023, e191
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
PP72 SARS-CoV-2: A Rapid Review On The Effectiveness Of Face Coverings To Reduce Transmission
-
- Journal:
- International Journal of Technology Assessment in Health Care / Volume 38 / Issue S1 / December 2022
- Published online by Cambridge University Press:
- 23 December 2022, pp. S63-S64
-
- Article
-
- You have access
- Export citation
Public health impact of mass sporting and cultural events in a rising COVID-19 prevalence in England
- Part of
-
- Journal:
- Epidemiology & Infection / Volume 150 / 2022
- Published online by Cambridge University Press:
- 31 January 2022, e42
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Antimicrobial Stewardship-Driven Monoclonal Antibody Treatment Program for COVID-19 Patients in the Bronx, New York
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s57
-
- Article
-
- You have access
- Open access
- Export citation
-
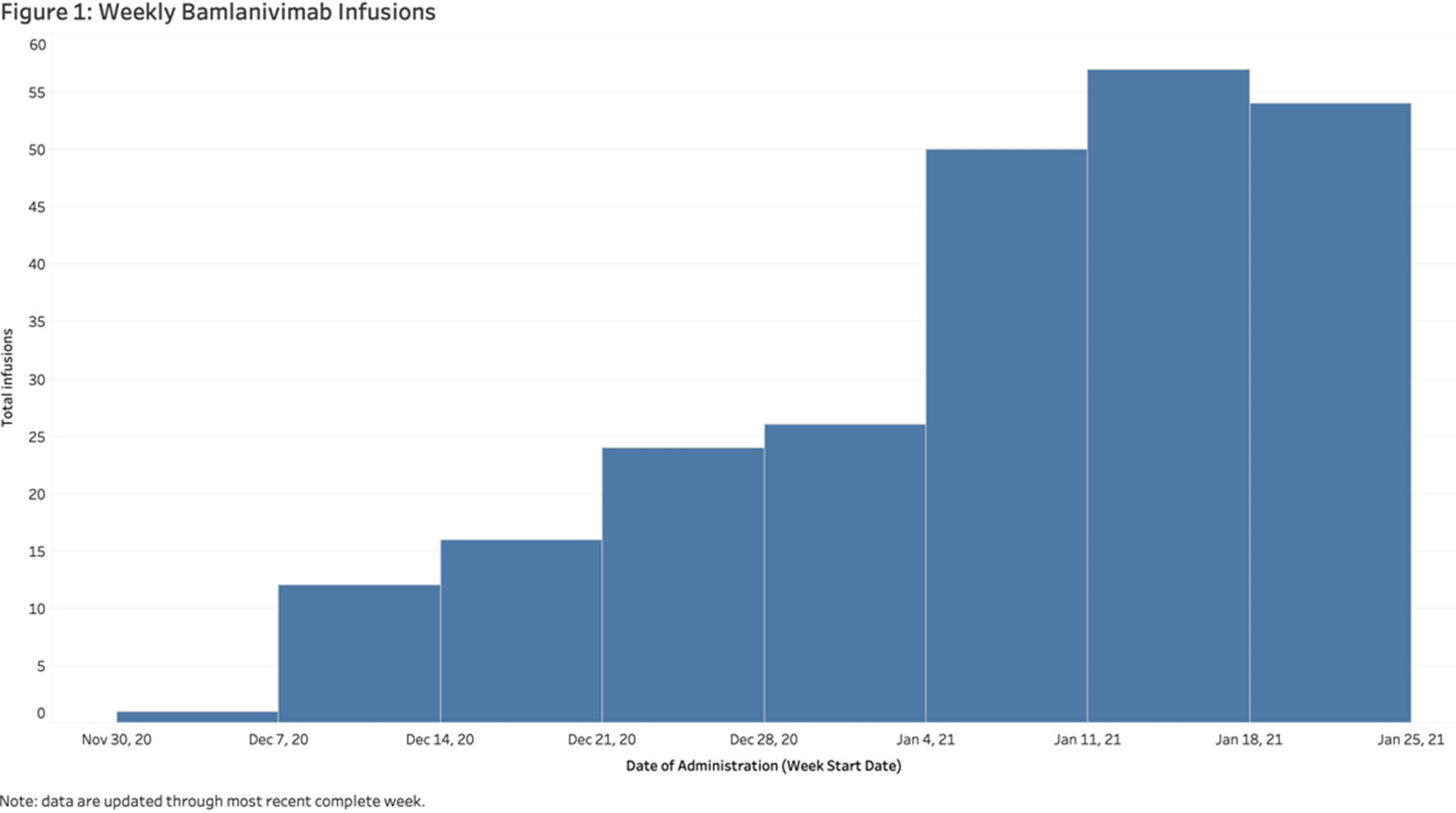
Background: In November 2020, bamlanivimab received emergency use authorization (EUA) to treat patients with early, mild-to-moderate COVID-19 who are at high risk of progression. Montefiore Medical Center serves an economically underserved community of >1.4 million residents in the Bronx, New York. Montefiore’s antimicrobial stewardship team (AST) developed a multidisciplinary treatment pathway for patients meeting EUA criteria: (1) outpatients and hospital associates and (2) acute-care patients (EDs or inpatient). Methods: The Montefiore AST established a centralized process for screening high-risk COVID-19 patients 7 days a week. Referrals were sent by e-mail from occupational health, primary care practices, specialty practices, emergency departments, and urgent care centers. Patients were screened in real time and were treated in the ED or a newly established infusion center within 24 hours. After infusion, all patients received phone calls from nurses and had an infectious diseases televisit. Demographics, clinical symptoms, subsequent ED visit or hospital admission, and timing from infusion to ED or hospitalization were obtained from the electronic health record. Results: In total, 281 high-risk patients (median age, 62 years; 57% female) received bamlanivimab at the infusion center or in the acute-care setting between December 2, 2020, and January 27, 2021 (Table 1). The number of treated patients increased weekly (Figure 1). Also, 62% were Hispanic or black, and 96% met EUA criteria. Furthermore, 51 (18%) were referred from occupational health, 205 (73%) were referred from the community, and 25 (9%) were inpatients (https://www.fda.gov/media/143605/download). All patients were successfully infused without adverse reactions. In addition, 23 patients (8.2%) were hospitalized and 6 (2.1%) visited EDs within 30 days of treatment. The average number of days between symptom onset and infusion was 4.9. The median age of admitted versus nonadmitted patients was 68 years versus 61.5 years (P = .07). Conclusions: An AST-coordinated bamlanivimab treatment program successfully treated multiple high-risk COVID-19 patients and potentially reduced hospitalizations. However, the effort, personnel, and resources required are significant. Dedicated hospital investment is necessary for maximal success.
Funding: No
Disclosures: None
Table 1. 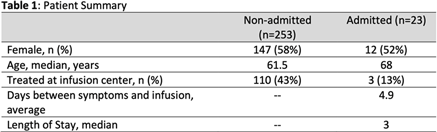
Figure 1.


A Ten-Year Review of Carbapenemase Producing Enterobacterales (CPE) in London, United Kingdom
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s6-s7
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
113 Dasotraline for the Treatment of Moderate to Severe Binge Eating Disorder in Adults: Results From a Randomized, Double-Blind, Placebo-Controlled Study
-
- Journal:
- CNS Spectrums / Volume 23 / Issue 1 / February 2018
- Published online by Cambridge University Press:
- 15 June 2018, pp. 72-73
-
- Article
-
- You have access
- Export citation
Understanding the Impact of Interventions to Prevent Antimicrobial Resistant Infections in the Long-Term Care Facility: A Review and Practical Guide to Mathematical Modeling
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 38 / Issue 2 / February 2017
- Published online by Cambridge University Press:
- 19 December 2016, pp. 216-225
- Print publication:
- February 2017
-
- Article
- Export citation
Chapter 20 - Microbiology
- from 9 - Microbiology
-
-
- Book:
- MRCOG Part One
- Published online:
- 27 January 2017
- Print publication:
- 13 October 2016, pp 317-342
-
- Chapter
- Export citation
Gene × Environment effects of serotonin transporter, dopamine receptor D4, and monoamine oxidase A genes with contextual and parenting risk factors on symptoms of oppositional defiant disorder, anxiety, and depression in a community sample of 4-year-old children
-
- Journal:
- Development and Psychopathology / Volume 25 / Issue 2 / May 2013
- Published online by Cambridge University Press:
- 30 April 2013, pp. 555-575
-
- Article
- Export citation
Contributors
-
-
- Book:
- The Cambridge Dictionary of Christianity
- Published online:
- 05 August 2012
- Print publication:
- 20 September 2010, pp xi-xliv
-
- Chapter
- Export citation
8 - Vertebrate life at high altitude
-
-
- Book:
- Respiratory Physiology of Vertebrates
- Published online:
- 05 June 2012
- Print publication:
- 28 January 2010, pp 265-299
-
- Chapter
- Export citation
Healthcare-Associated Staphylococcus aureus Bacteremia and the Risk for Methicillin Resistance: Is the Centers for Disease Control and Prevention Definition for Community-Acquired Bacteremia Still Appropriate?
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 26 / Issue 2 / February 2005
- Published online by Cambridge University Press:
- 21 June 2016, pp. 204-209
- Print publication:
- February 2005
-
- Article
- Export citation
Simplified Surveillance for Nosocomial Bloodstream Infections
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 19 / Issue 9 / September 1998
- Published online by Cambridge University Press:
- 02 January 2015, pp. 657-660
- Print publication:
- September 1998
-
- Article
- Export citation
