
4 results
Clostridioides difficile infection (CDI) treatment outcomes and recurrence factor at a pediatric hospital
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s28
-
- Article
-
- You have access
- Open access
- Export citation
Healthcare-Associated Viral Respiratory Infections in a Pediatric Intensive Care Unit and Cardiovascular Intensive Care Unit
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, pp. s75-s76
-
- Article
-
- You have access
- Open access
- Export citation
-
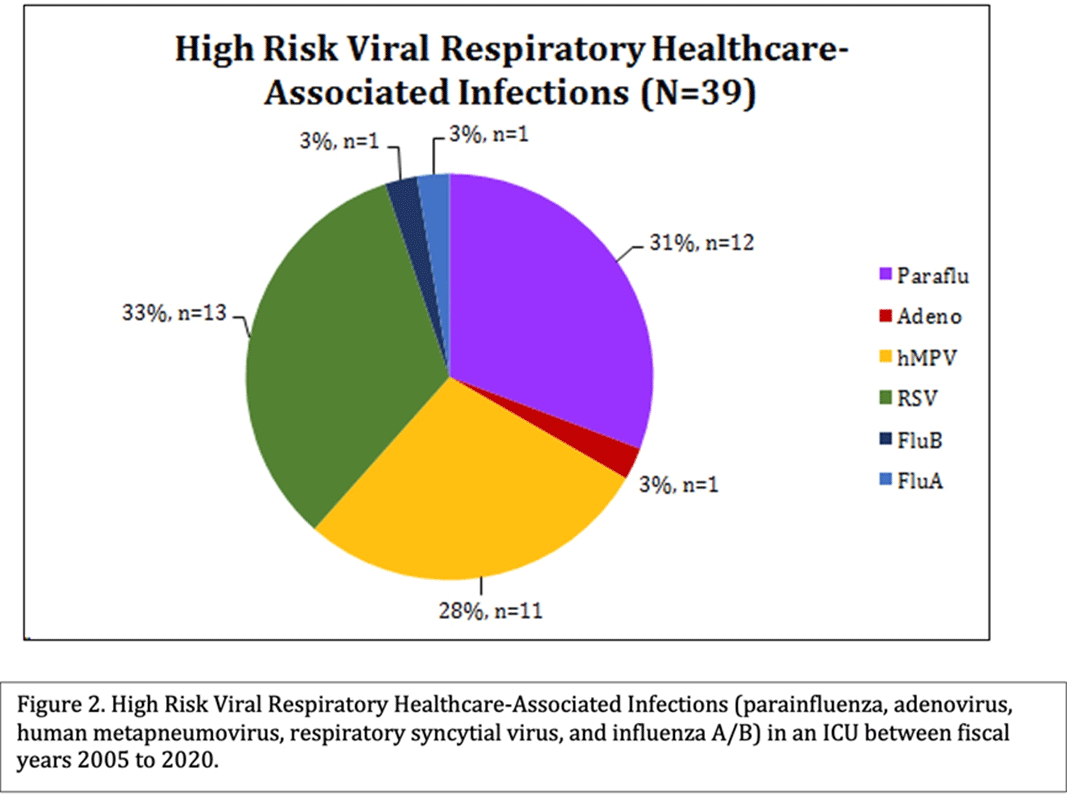
Background: Healthcare-associated infections (HAIs) affect patient health and are tracked closely by infection prevention. Patients in a pediatric intensive care unit (PICU) acquired viral respiratory infections had longer use of respiratory support. We sought to determine the types of viral respiratory HAIs (VR-HAIs) acquired in the PICU and the characteristics of those affected. Methods: CHOC Children’s Hospital is a 334-bed tertiary-care center. Charts were reviewed on patients with VR-HAIs from fiscal years (FY) 2005–2020. High-risk VR-HAI (HR-VR-HAI) were influenza A and B, respiratory syncytial virus (RSV), adenovirus, parainfluenza, and human metapneumovirus (hMPV, added in FY 2014). Patients in the PICU, cardiovascular ICU (CVICU), and oncology ICU (OICU) with HR-VR-HAIs were reviewed. Patients were categorized according to underlying pathology, immunosuppression, and isolation prior to HR-VR-HAI. Increased respiratory support was defined as any increase from a patient’s baseline support ±24 hours of viral diagnosis: increase in oxygen flow or transition from nasal cannula to high-flow nasal cannula or ventilator support. Antibiotic escalation, defined as initiation of antibiotic therapy for ≥2 days ±24 hours of viral diagnosis or broadening the spectrum of antimicrobials for ≥2 days ±24 hours of viral diagnosis. Results: During FY 2005–2020, there were 204 VR-HAIs: 143 HR-VR-HAIs (70%), of which 39 (27.2%) occurred in ICUs (Figure 1). Most of the HR-VR-HAIs were RSV, parainfluenza, and hMPV (Figure 2). Of 39 patients, 10 (25.6%) had underlying oncologic conditions, 9 of whom were immunosuppressed. Of 39 patients, 16 (41%) had structural cardiac disease, 4 (10.3%) had pulmonary disease, 5 (12.8%) had neurologic disease, and the remaining 4 (10.3%) had other comorbidities. Of 39 patients, 12 (31%) required an increase in respiratory support and 13 (33%) had escalation of antibiotics. Of 39 HR-VR-HAI patients, 2 died within 2 weeks of acquisition. Conclusions: HR-VR-HAIs are uncommon in ICUs. RSV, parainfluenza, and hMPV are the most common, and 1 of 3 of patients required escalation in respiratory support and/or escalation in antibiotics. All patients had underlying comorbidities. In our series, there were 2 deaths within 2 weeks of infection.
Funding: No
Disclosures: None
Figure 1.
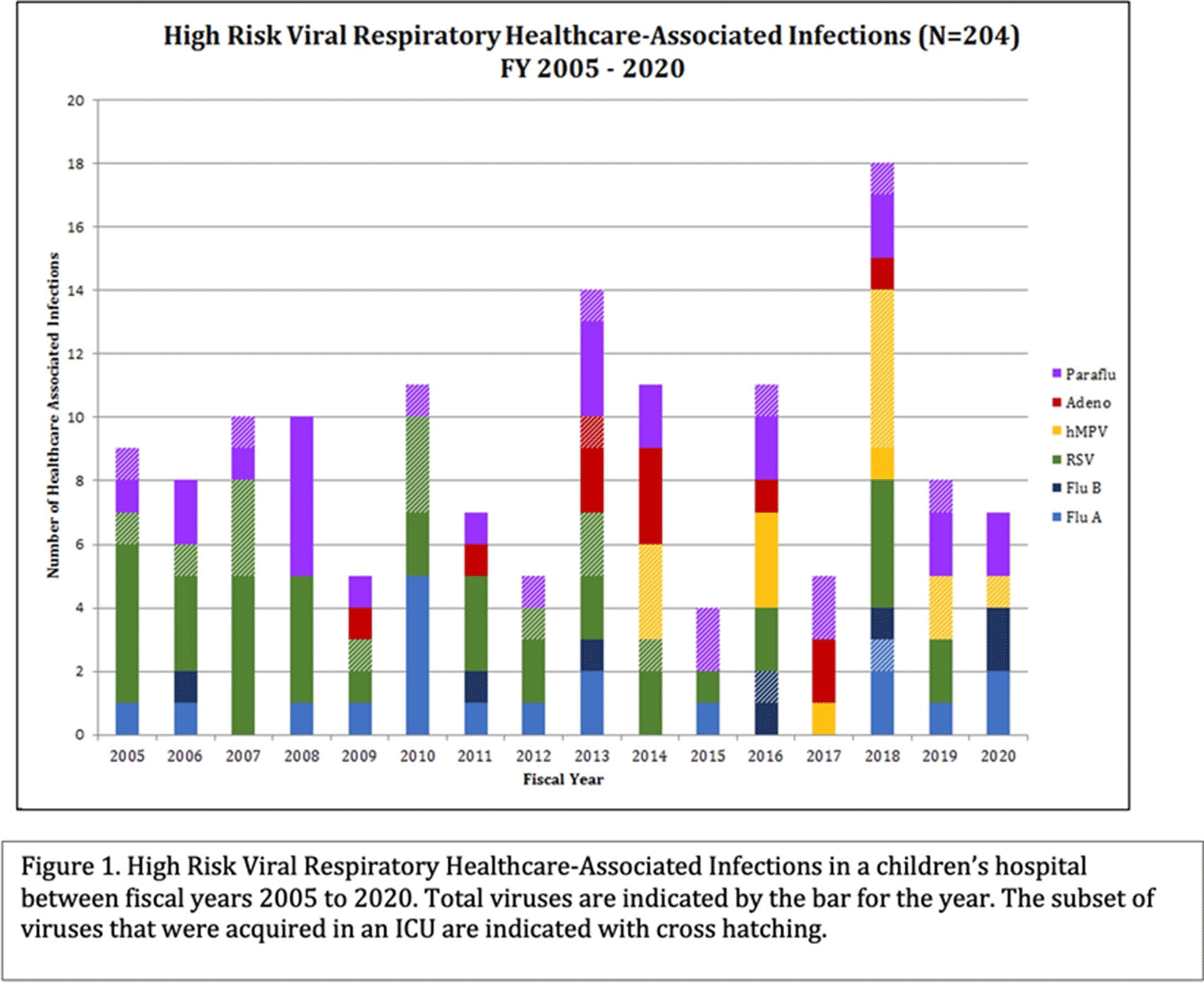
Figure 2.


No Device, No Problem? Healthcare-Associated Bloodstream and Urinary Tract Infections in a Children’s Hospital
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s73-s74
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Prevention of Central Venous Catheter-Associated Bloodstream Infections in Pediatric Intensive Care Units A Performance Improvement Collaborative
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 30 / Issue 7 / July 2009
- Published online by Cambridge University Press:
- 02 January 2015, pp. 645-651
- Print publication:
- July 2009
-
- Article
- Export citation
