
184 results
Natural Language Processing (NLP) Accurately Identifies LTCF Exposure from Clinical Notes: A Proof-of-Principle Study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s13-s14
-
- Article
-
- You have access
- Open access
- Export citation
-
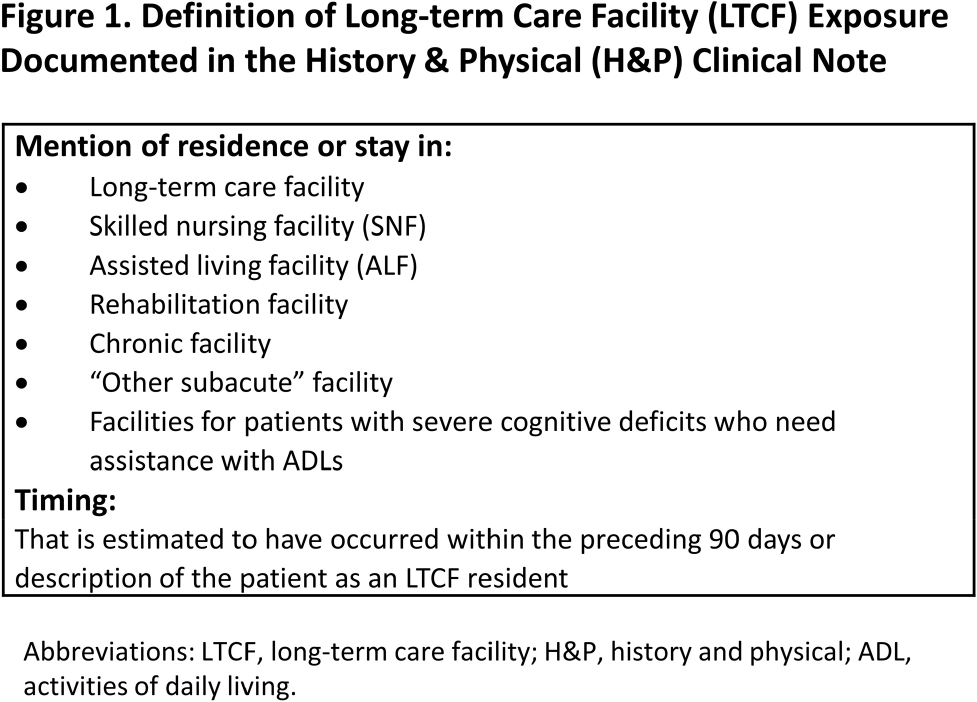
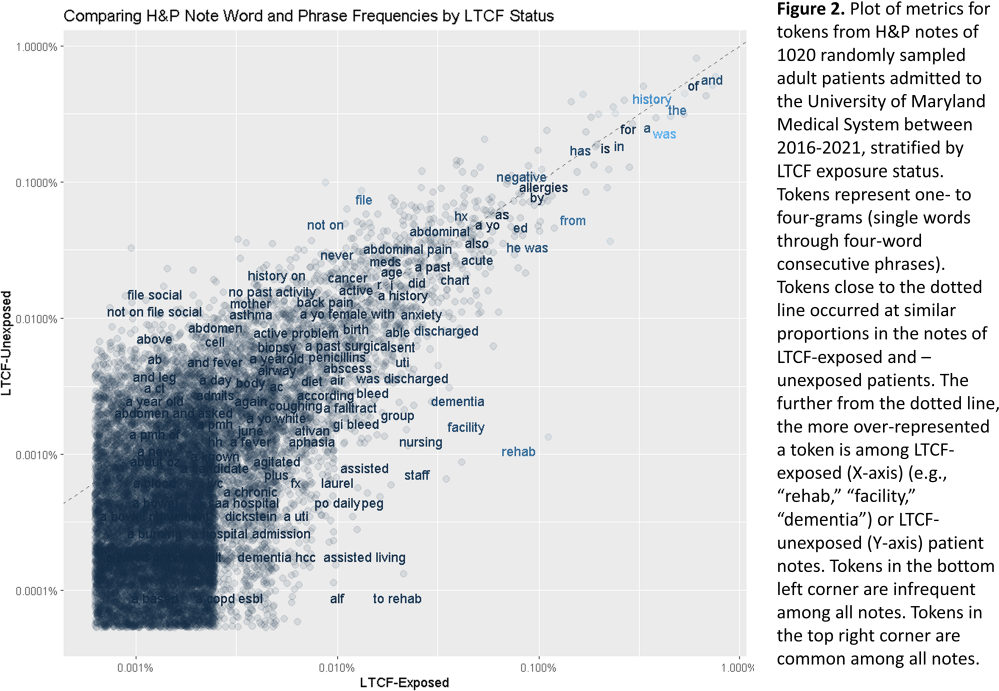
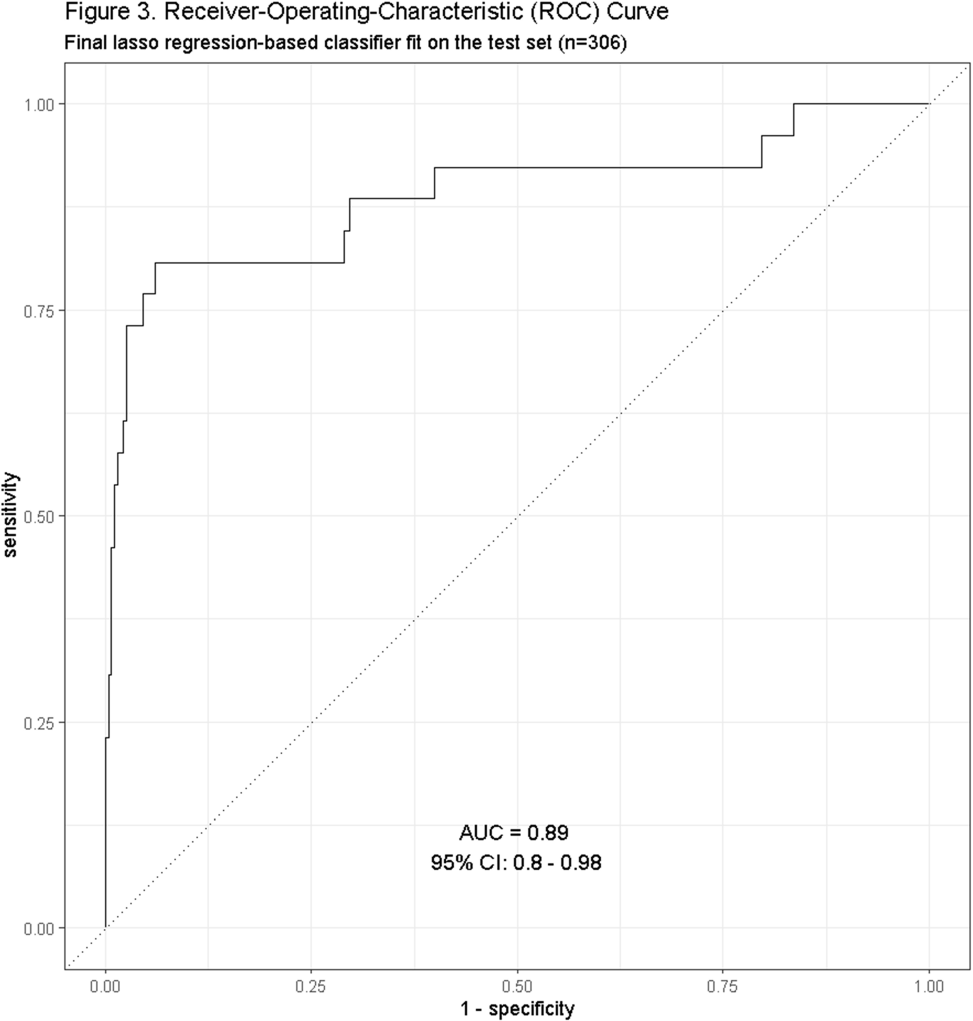
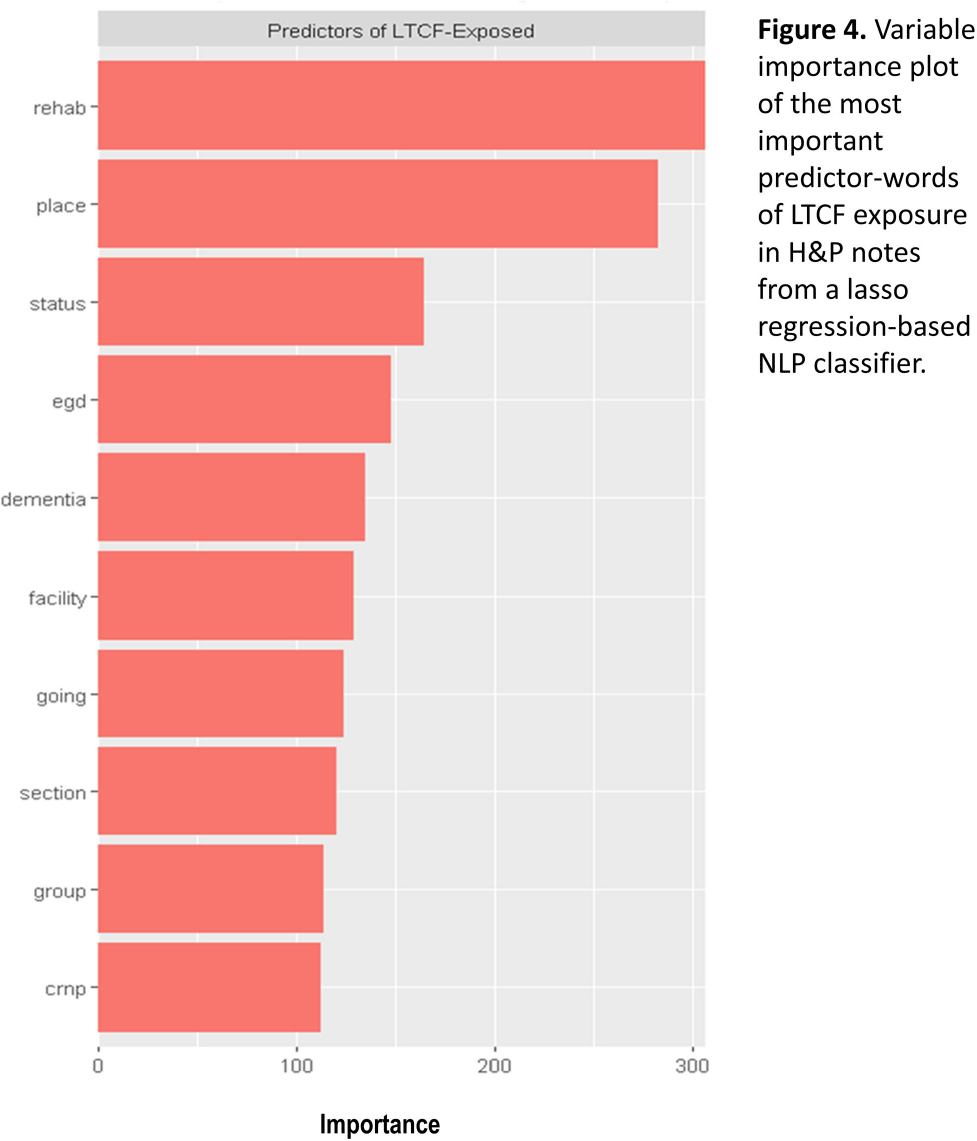
Background: Residence or recent stay in a long-term care facility (LTCF) is one of the most important risk factors for multidrug-resistant organism (MDRO) carriage and infection, making reliable identification of LTCF-exposed inpatients a critical priority for infection control day-to-day practice and research. However, because most hospital electronic health records (EHRs) do not include a dedicated field for documenting LTCF exposure, absent manual review of patient charts, identifying LTCF-exposed inpatients is challenging. We aimed to develop an automated, natural language processing (NLP)-based classifier for identifying LTCF exposure from clinical notes. Methods: We randomly sampled 1020 adult admissions from 2016-2021 across the 12-hospital University of Maryland Medical System and manually reviewed each admission’s history & physical (H&P) note for mention of LTCF exposure (Figure 1). After H&P pre-processing, we calculated feature representations for documents based on term frequencies and visually explored between-group (LTCF-exposed vs. LTCF-unexposed) feature differences. To predict LTCF status from the H&P notes, we trained and tuned a LASSO regression-based classifier on 70% of the data with 3-fold cross-validation and 1:1 up-sampling to address class imbalance. The final classifier was evaluated on the 30% held-out sample (not up-sampled), with calculation of the C-statistic (area-under-the-curve, AUC) with bootstrapped 95% confidence intervals, and construction of receiver-operating-characteristic and variable importance plots (R Version 4.3.2). Results: 7% (n=76 cases) of H&P notes documented LTCF exposure. In our visual analysis, the H&P words and phrases that were over-represented among LTCF patients had high face validity (Figure 2). The final LASSO-regression-based classifier achieved a C-statistic of 0.89 (95% CI: 0.80–0.98) on the held-out data for identifying LTCF exposure from the H&P notes (Figure 3). The most important model predictors (i.e., words) for distinguishing LTCF-exposed from LTCF-unexposed patients are reflected in Figure 4. The most important predictor-words of LTCF-exposure were “rehab,” “place,” “status,” “egd,” and “dementia.” Conclusion: In this multi-center study, even a simple NLP classifier demonstrated very strong discrimination for identifying LTCF exposure status from H&P notes, which could substantially reduce the manual review time required to identify LTCF-exposed inpatients. If automated in the electronic health record, it could also inform real-time MDRO screening decisions. Future research is planned to build more sophisticated classifiers using machine learning best practices, to build classifiers for additional MDRO risk factors, and to externally validate NLP classifiers on notes from an external healthcare system.




CLABSIs aren’t just for inpatients: the need to identify CLABSI burden among outpatients
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 12 September 2024, e132
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Chlorhexidine gluconate skin levels and organism decolonization: what we know and what we don’t know
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 08 August 2024, pp. 1-2
-
- Article
- Export citation
Healthcare personnel opinions regarding the feasibility of a risk-tailored approach to contact precautions for methicillin-resistant Staphylococcus aureus in the acute care setting
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 22 April 2024, pp. 1-3
-
- Article
- Export citation
A multi-center validation of the electronic health record admission source and discharge location fields against the clinical notes for identifying inpatients with long-term care facility exposure
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 18 April 2024, pp. 1-6
-
- Article
- Export citation
Research agenda for transmission prevention within the Veterans Health Administration, 2024–2028
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 11 April 2024, pp. 1-10
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Factors associated with patient-to-healthcare personnel (HCP) and HCP-to-subsequent patient transmission of methicillin-resistant Staphylococcus aureus
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 5 / May 2024
- Published online by Cambridge University Press:
- 18 January 2024, pp. 583-589
- Print publication:
- May 2024
-
- Article
- Export citation
Alcohol-based decontamination of gloved hands: A randomized controlled trial
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 4 / April 2024
- Published online by Cambridge University Press:
- 23 November 2023, pp. 467-473
- Print publication:
- April 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Active surveillance and contact precautions for preventing MRSA healthcare-associated infections during the COVID-19 pandemic
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s117-s118
-
- Article
-
- You have access
- Open access
- Export citation
-
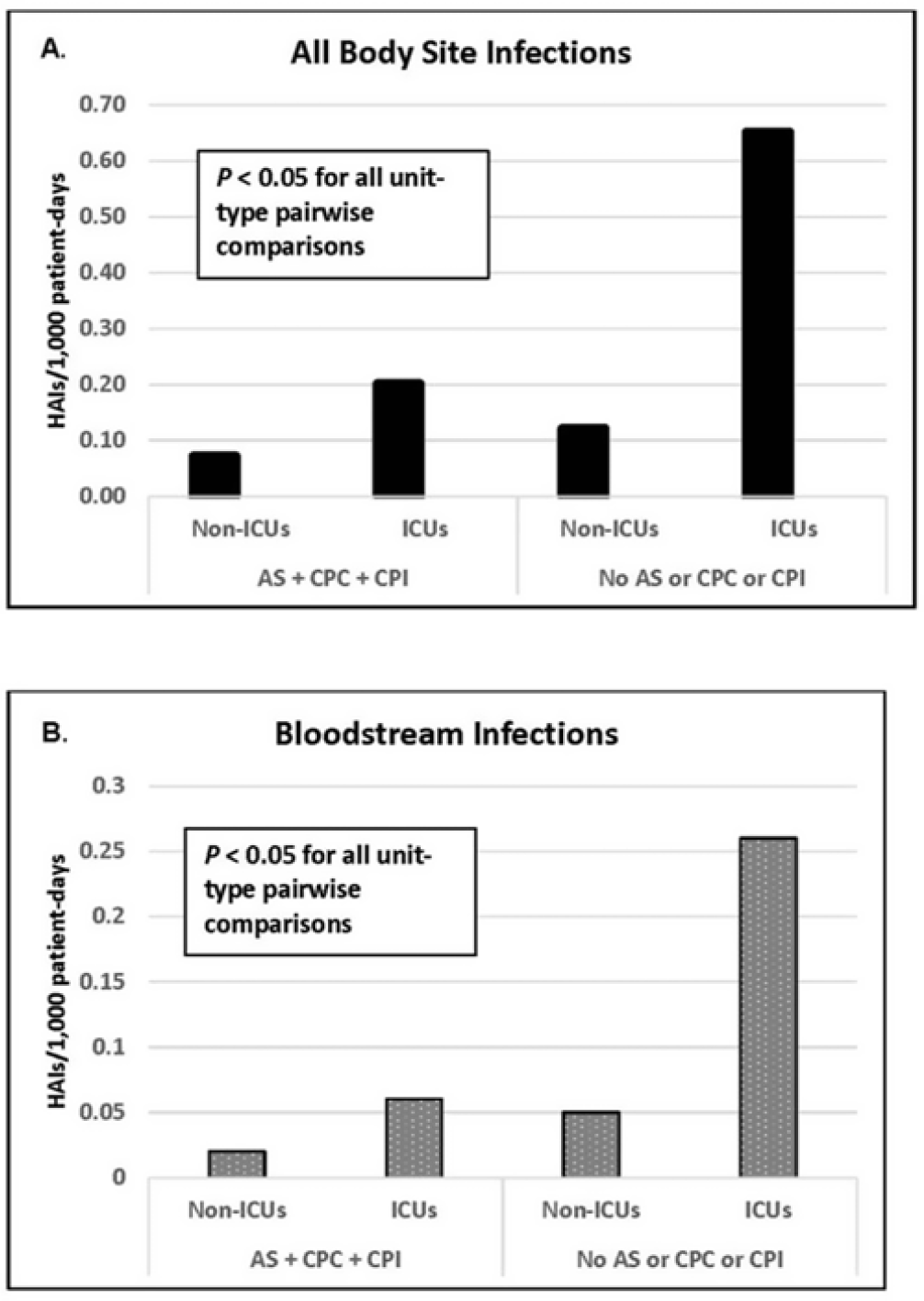
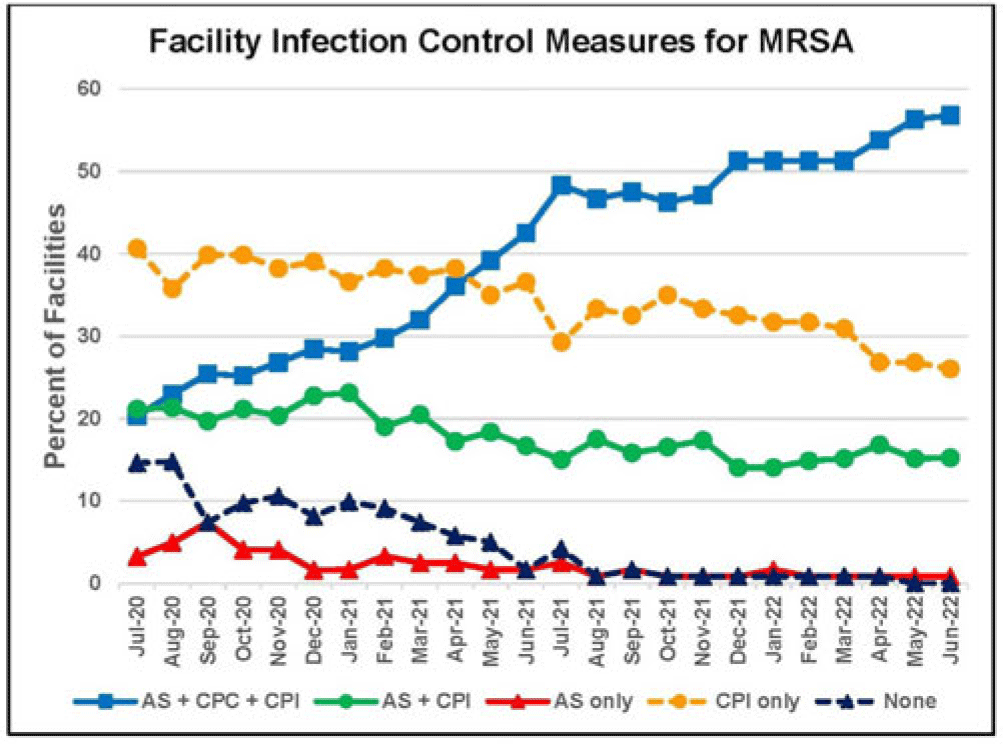
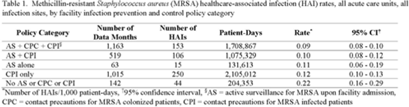
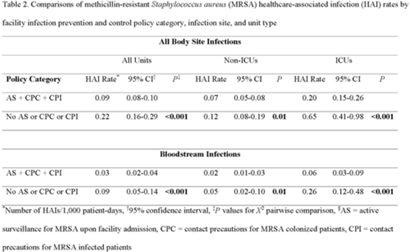
Background: Statistically significant decreases in methicillin-resistant Staphylococcus aureus (MRSA) healthcare-associated infections (HAIs) occurred in Veterans Health Administration (VA) facilities from 2007 to 2019 using active surveillance for facility admissions and contact precautions for patients colonized (CPC) or infected (CPI) with MRSA, but the value of these interventions is controversial. Objective: To determine the impact of active surveillance, CPC, and CPI on prevention MRSA HAIs, we conducted a prospective cohort study between July 2020 and June 2022 in all 123 acute-care VA medical facilities. In April 2020, all facilities were given the option to suspend any combination of active surveillance, CPC, or CPI to free up laboratory resources for COVID-19 testing and conserve personal protective equipment. We measured MRSA HAIs (cases per 1,000 patient days) in intensive care units (ICUs) and non-ICUs by the infection control policy. Results: During the analysis period, there were 917,591 admissions, 5,225,174 patient days, and 568 MRSA HAIs. Only 20% of facilities continued all 3 MRSA infection control measures in July 2020, but this rate increased to 57% by June 2022. The MRSA HAI rate for all infection sites in non-ICUs was 0.07 (95% CI, 0.05–0.08) for facilities practicing active surveillance plus CPC plus CPI compared to 0.12 (95% CI, 0.08–0.19; P = .01) for those not practicing any of these strategies, and in ICUs the MRSA HAI rates were 0.20 (95% CI, 0.15–0.26) and 0.65 (95% CI, 0.41–0.98; P < .001) for the respective policies. Similar differences were seen when the analyses were restricted to MRSA bloodstream HAIs. Accounting for monthly COVID-19 admissions to facilities over the analysis period using a negative binomial regression model did not change the relationships between facility policy and MRSA HAI rates in the ICUs or non-ICUs. There was no statistically significant difference in monthly facility urinary catheter-associated infection rates, a nonequivalent dependent variable, in the categories during the analysis period in either ICUs or non-ICUs. Conclusions: In Veterans Affairs medical centers, there were fewer MRSA HAIs when facilities practiced active surveillance and contact precautions for colonized or infected patients during the COVID-19 pandemic. The effect was greater in ICUs than non-ICUs.
Disclosures: None




Evidence of housing instability identified by addresses, clinical notes, and diagnostic codes in a real-world population with substance use disorders
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 04 September 2023, e196
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Developing a diagnosis calculator to estimate the probability of bacterial pneumonia
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 07 August 2023, e137
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Efficacy of a continuously active disinfectant wipe on the environmental bioburden in the intensive care unit: A randomized controlled study
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 03 July 2023, pp. 2036-2043
- Print publication:
- December 2023
-
- Article
- Export citation
SHEA/IDSA/APIC Practice Recommendation: Strategies to prevent methicillin-resistant Staphylococcus aureus transmission and infection in acute-care hospitals: 2022 Update
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 7 / July 2023
- Published online by Cambridge University Press:
- 29 June 2023, pp. 1039-1067
- Print publication:
- July 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Comparison of two swab types for recovery of Staphylococcus aureus and Candida auris from gloves and gowns
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 11 / November 2023
- Published online by Cambridge University Press:
- 04 May 2023, pp. 1870-1872
- Print publication:
- November 2023
-
- Article
- Export citation
Diagnostic stewardship to support optimal use of multiplex molecular respiratory panels: A survey from the Society for Healthcare Epidemiology of America Research Network
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 11 / November 2023
- Published online by Cambridge University Press:
- 02 May 2023, pp. 1823-1828
- Print publication:
- November 2023
-
- Article
- Export citation
Contact precautions for the control of endemic pathogens: Finding the middle path
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 24 March 2023, e57
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Infection prevention and antibiotic stewardship program needs and practices in 2021: A survey of the Society for Healthcare Epidemiology of America Research Network
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 14 March 2023, pp. 948-950
- Print publication:
- June 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Comorbidities associated with 30-day readmission following index coronavirus disease 2019 (COVID-19) hospitalization: A retrospective cohort study of 331,136 patients in the United States
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 8 / August 2023
- Published online by Cambridge University Press:
- 03 October 2022, pp. 1325-1333
- Print publication:
- August 2023
-
- Article
- Export citation
Molecular concordance of methicillin-resistant Staphylococcus aureus isolates from healthcare workers and patients
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 4 / April 2023
- Published online by Cambridge University Press:
- 30 September 2022, pp. 578-588
- Print publication:
- April 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Social Networks among Indigenous Peoples in Mexico
-
- Journal:
- Latin American Research Review / Volume 45 / Issue 2 / 2010
- Published online by Cambridge University Press:
- 05 September 2022, pp. 49-67
-
- Article
-
- You have access
- Export citation
