
Contents
Oral Presentation
MDR GNR
How Does Antimicrobial Resistance Increase Medical Costs in Community-Acquired Acute Pyelonephritis?
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s23
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: The proportion of antimicrobial-resistant Enterobacterales that are causative pathogens for community-acquired acute pyelonephritis (CA-APN) has been increasing. We examined the effect of antimicrobial resistance on medical costs in CA-APN. Methods: A single-center retrospective cohort study was conducted at a tertiary-care hospital in Korea between January 2018 to December 2019. All hospitalized patients aged ≥19 years who were diagnosed with CA-APN were recruited, and those with Enterobacterales as a causative pathogen were included. Comparisons between CA-APN caused by extended-spectrum β-lactamase (ESBL)–producing pathogens (ESBL+ group) and those by non–ESBL-producing organisms (ESBL– group) as well as CA-APN caused by ciprofloxacin-resistant pathogens (CIP-R group) and those by ciprofloxacin-sensitive pathogens (CIP-S group) were performed. Log-linear regression was performed to determine the risk factors for medical costs. Results: In total, 241 patients were included in this study. Of these, 75 (31.1%) had an ESBL-producing pathogen and 87 (36.1%) had a ciprofloxacin-resistant pathogen. The overall medical costs were significantly higher in the ESBL+ group compared with the ESBL− group (US$3,730.18 vs US$3,119.32) P <0.001) as well as in CIP-R group compared with CIP-S group (3,730.18 USD vs. 3,119.32 USD, P =0.005). In addition, length of stay was longer in ESBL+ group compared with ESBL-group (11 vs. 8 days, P <0.001) as well as in CIP-R group compared with CIP-S group (11 vs. 8 days, P <0.001). There were no significant difference in the proportion of clinical failure between ESBL+ and ESBL- groups; CIP-R and CIP-S groups. Based on the log-linear regression model, the costs associated with ESBL-producing Enterobacterales as the causative pathogen would be, on average, 27% higher or US$1,211 higher than its counterpart (P = .026). By the same token, a patient who is a year older would incur US$23 higher cost (P = .040). Having any structural problem in urinary tract would incur US$1,231 higher cost (P = .015). A unit increase in Pitt score would incur US$767 USD higher cost (P < 0.001) higher cost, all other things constant. Conclusions: Medical costs for hospitalized patients with CA-APN are increased by the existence of ESBL-producing Enterobacterales but not by the existence of ciprofloxacin-resistant Enterobacterales.
Funding: No
Disclosures: None
Figure 1.
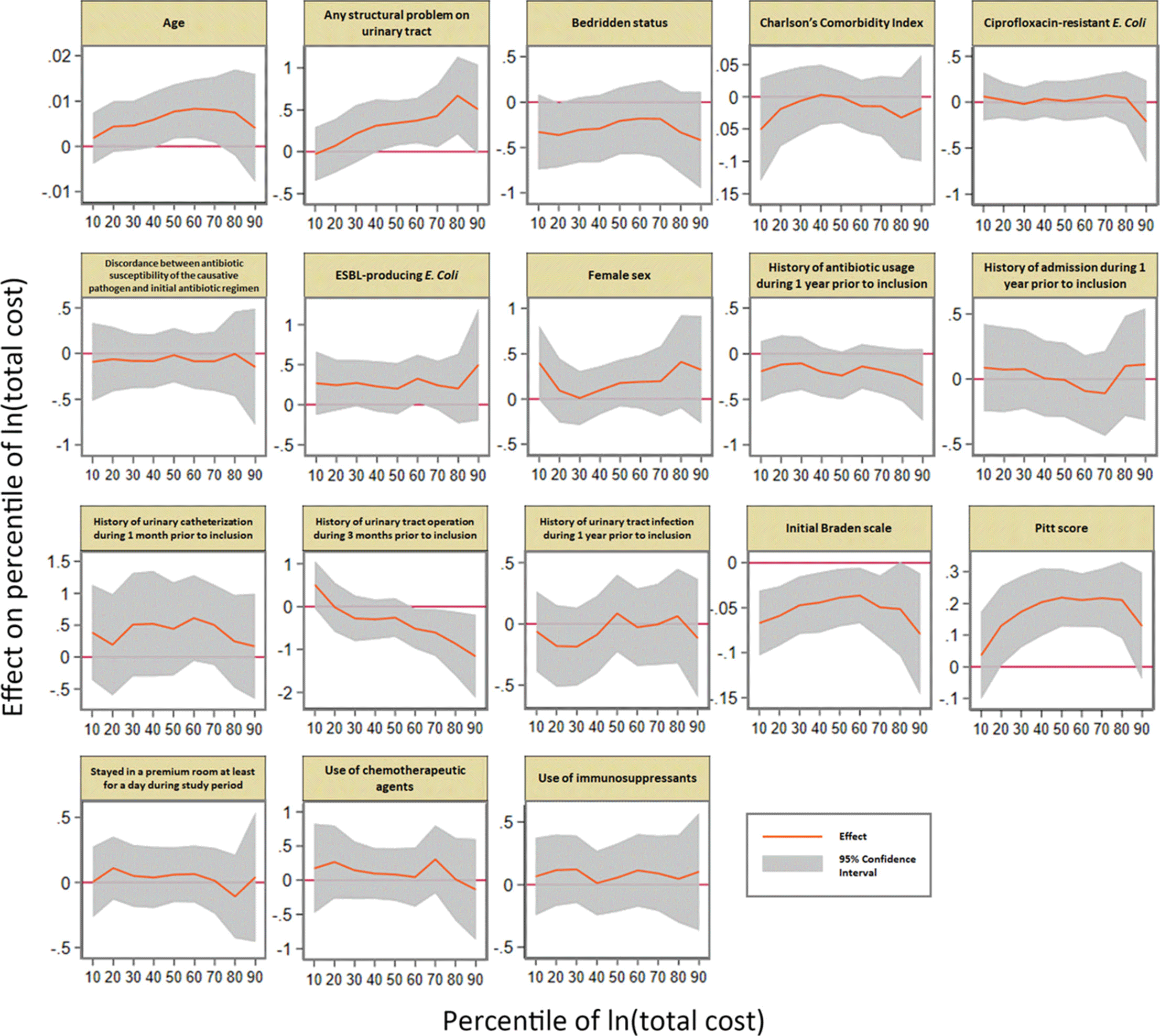
Table 1. 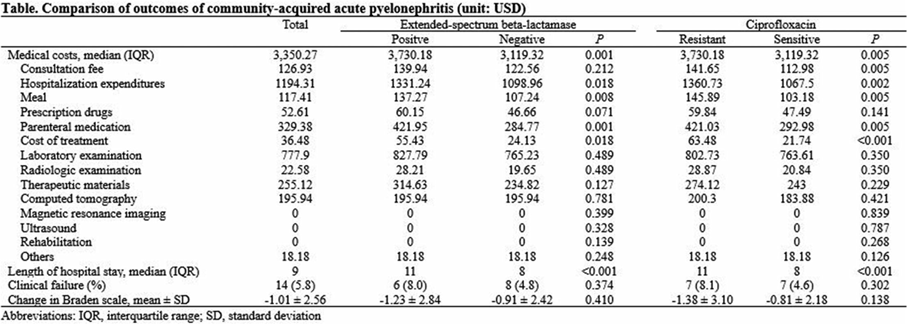
Table 2. 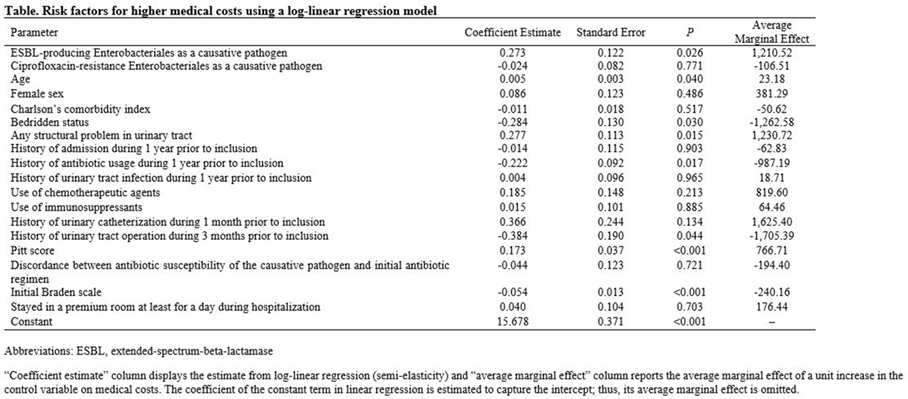



Medical Informatics
Automated Nationwide Benchmarking Dashboard for Antimicrobial Stewardship Programs within the Veterans’ Health Administration
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s23-s24
-
- Article
-
- You have access
- Open access
- Export citation
-
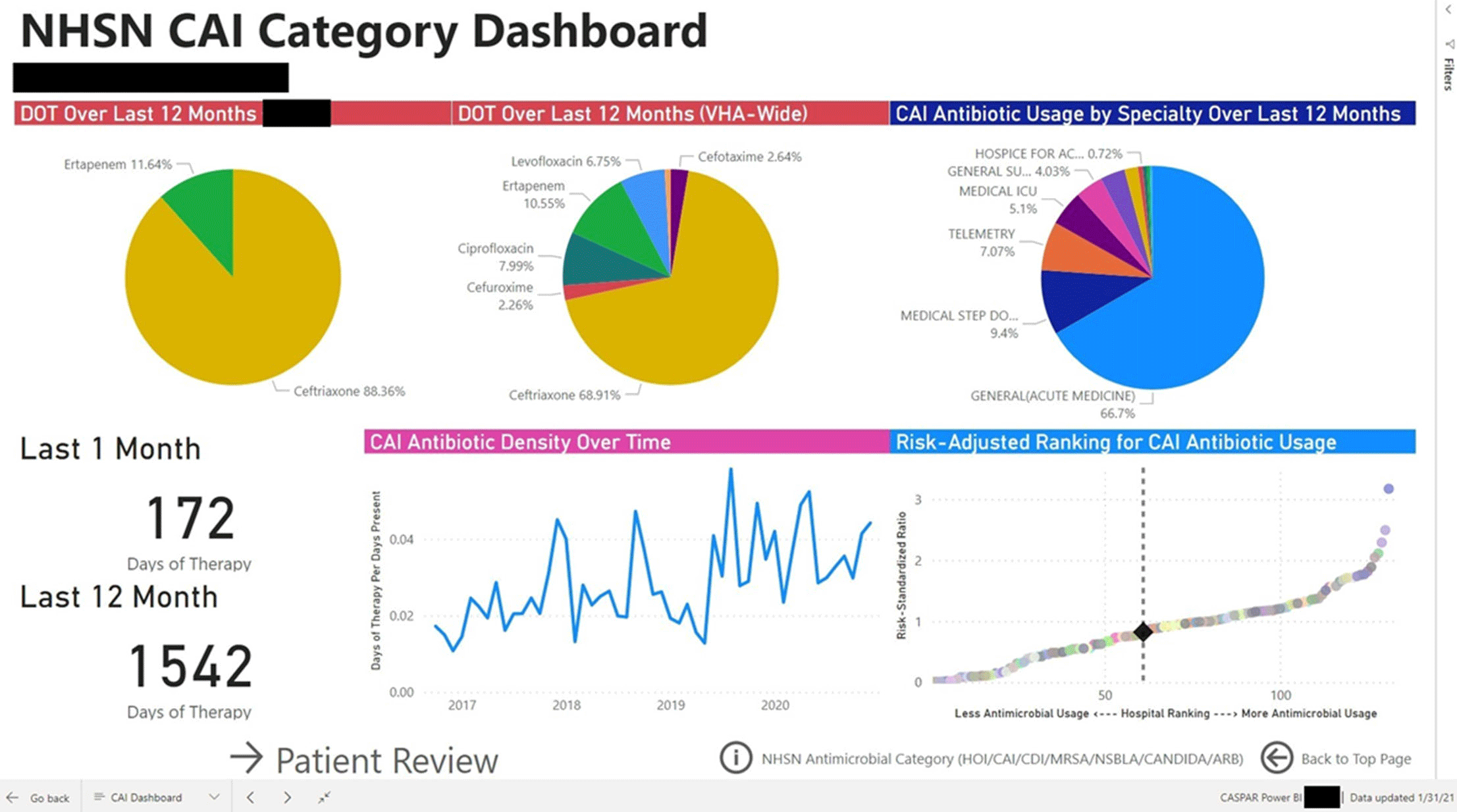
Group Name: VHA Center for Antimicrobial Stewardship and Prevention of Antimicrobial Resistance (CASPAR) Background: Antimicrobial stewardship programs (ASPs) are advised to measure antimicrobial consumption as a metric for audit and feedback. However, most ASPs lack the tools necessary for appropriate risk adjustment and standardized data collection, which are critical for peer-program benchmarking. We created a system that automatically extracts antimicrobial use data and patient-level factors for risk-adjustment and a dashboard to present risk-adjusted benchmarking metrics for ASP within the Veterans’ Health Administration (VHA). Methods: We built a system to extract patient-level data for antimicrobial use, procedures, demographics, and comorbidities for acute inpatient and long-term care units at all VHA hospitals utilizing the VHA’s Corporate Data Warehouse (CDW). We built baseline negative binomial regression models to perform risk-adjustments based on patient- and unit-level factors using records dated between October 2016 and September 2018. These models were then leveraged both retrospectively and prospectively to calculate observed-to-expected ratios of antimicrobial use for each hospital and for specific units within each hospital. Data transformation and applications of risk-adjustment models were automatically performed within the CDW database server, followed by monthly scheduled data transfer from the CDW to the Microsoft Power BI server for interactive data visualization. Frontline antimicrobial stewards at 10 VHA hospitals participated in the project as pilot users. Results: Separate baseline risk-adjustment models to predict days of therapy (DOT) for all antibacterial agents were created for acute-care and long-term care units based on 15,941,972 patient days and 3,011,788 DOT between October 2016 and September 2018 at 134 VHA hospitals. Risk adjustment models include month, unit types (eg, intensive care unit [ICU] vs non-ICU for acute care), specialty, age, gender, comorbidities (50 and 30 factors for acute care and long-term care, respectively), and preceding procedures (45 and 24 procedures for acute care and long-term care, respectively). We created additional models for each antimicrobial category based on National Healthcare Safety Network definitions. For each hospital, risk-adjusted benchmarking metrics and a monthly ranking within the VHA system were visualized and presented to end users through the dashboard (an example screenshot in Figure 1). Conclusions: Developing an automated surveillance system for antimicrobial consumption and risk-adjustment benchmarking using an electronic medical record data warehouse is feasible and can potentially provide valuable tools for ASPs, especially at hospitals with no or limited local informatics expertise. Future efforts will evaluate the effectiveness of dashboards in these settings.
Funding: No
Disclosures: None
Figure 1.
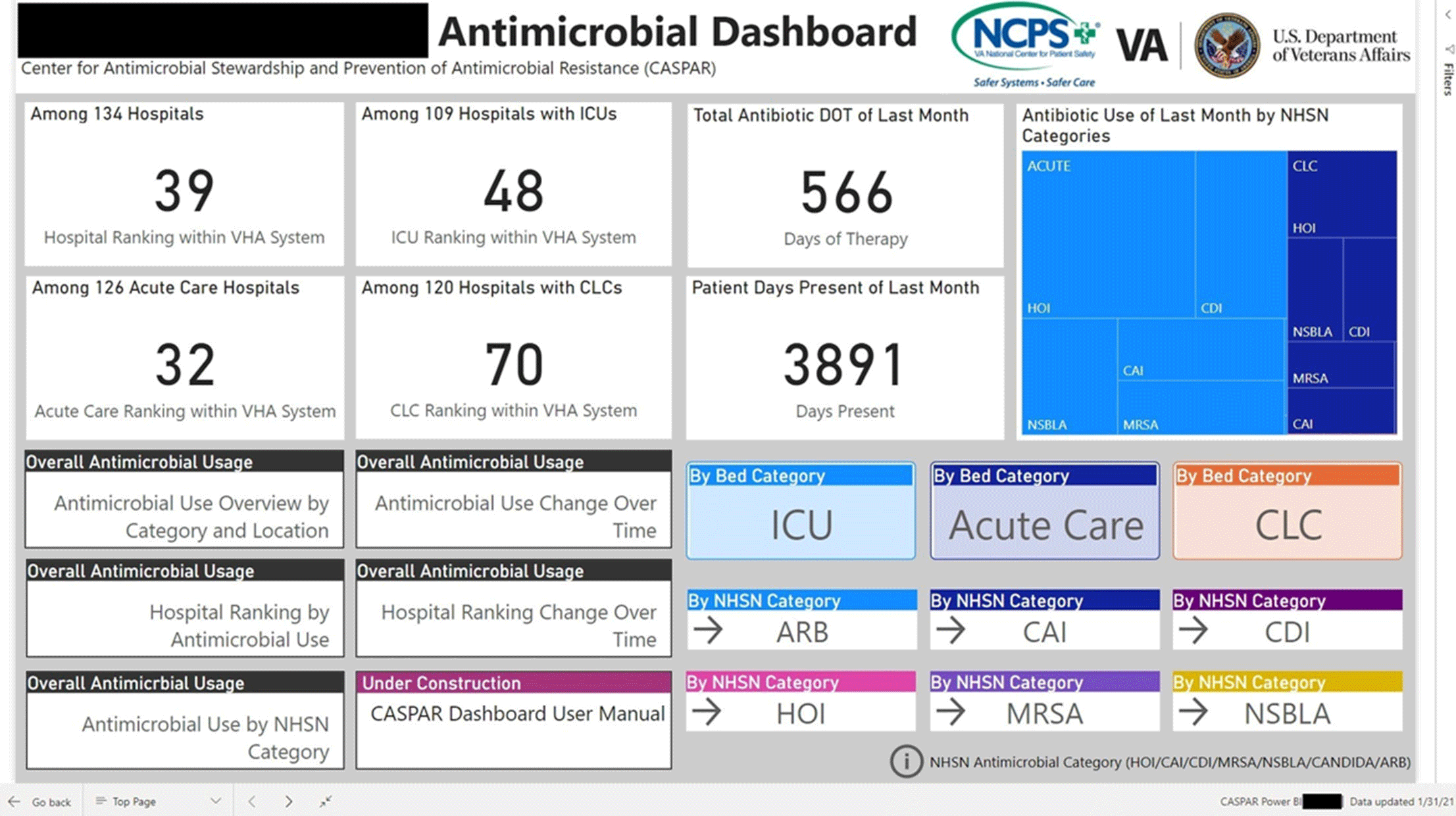
Figure 2.
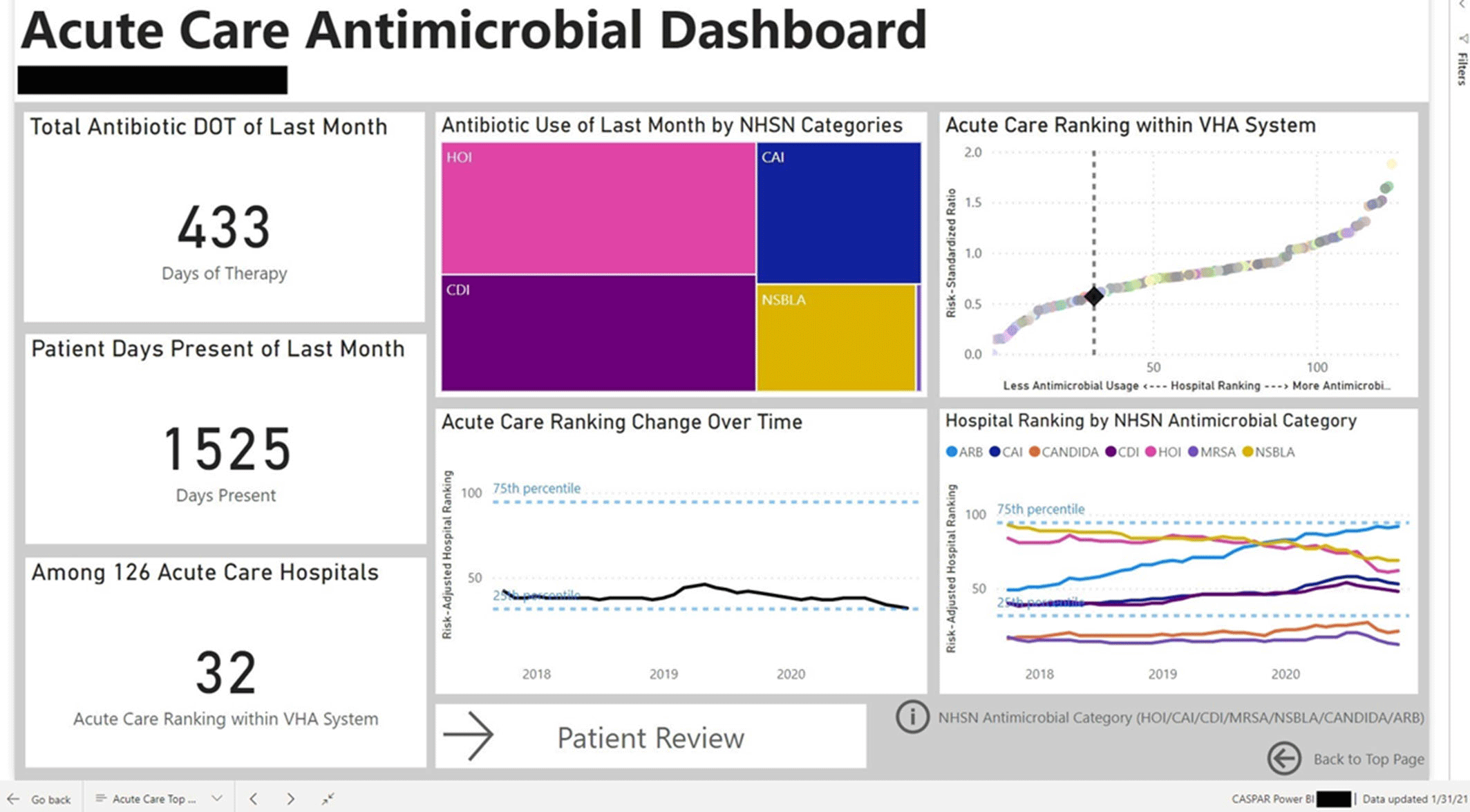
Figure 3.



Presentation Type: Oral Presentation
MRSA/VRE
Discontinuation of Contact Precautions in Patients with Nosocomial MRSA and VRE Infections During the COVID-19 Pandemic
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s24
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Gaps exist in the evidence supporting the benefits of contact precautions for the prevention of methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant enterococci (VRE). The Centers for Disease Control and Prevention allow suspending contact precautions for MRSA and VRE in cases of gown shortages, as we have seen during the COVID-19 pandemic. We evaluated the impact of discontinuing isolation precautions in hospitalized patients with MRSA and VRE infection, due to gown shortage, on the rate of hospital-acquired (HA) MRSA and VRE infections. Methods: A retrospective chart review was performed on adult patients (n = 2,200) with established MRSA or VRE infection at 5 hospitals in CommonSpirit Health, Texas Division, from March 2019 to October 2020. Data including demographics, infection site, documented symptoms, and antibiotic use were stratified based on patient location (floor vs ICU). Rates of hospital-acquired MRSA and VRE infection before and after the discontinuation of isolation (implemented in March 2020) were compared. Incidence density rate was used to assess differences in the rate of MRSA and VRE infections between pre- and postintervention groups. Results: The rate of hospital-acquired (HA) MRSA infection per 10,000 patient days before the intervention (March 19–February 20) was 12.19, compared to 10.64 after the intervention (March 20–July 20) (P = .038). The rates of HA MRSA bacteremia were 1.13 and 0.93 for the pre- and postintervention groups, respectively (P = .074). The rates of HA VRE per 10,000 patient days were 3.53 and 4.44 for the pre- and postintervention groups, respectively (P = .274). The hand hygiene rates were 0.93 before the intervention and 0.97 after the intervention (P = .028). Conclusions: Discontinuing isolation from MRSA and VRE in the hospital setting did not lead to a statistically significant increase in hospital-acquired MRSA or VRE infections. In fact, rates of hospital-acquired MRSA decreased, likely secondary to improvements in hand hygiene during this period. These results support the implementation of policies for discontinuing contact isolation for hospitalized patients with documented MRSA or VRE infection, particularly during shortages of gowns.
Funding: No
Disclosures: None
Figure 1.
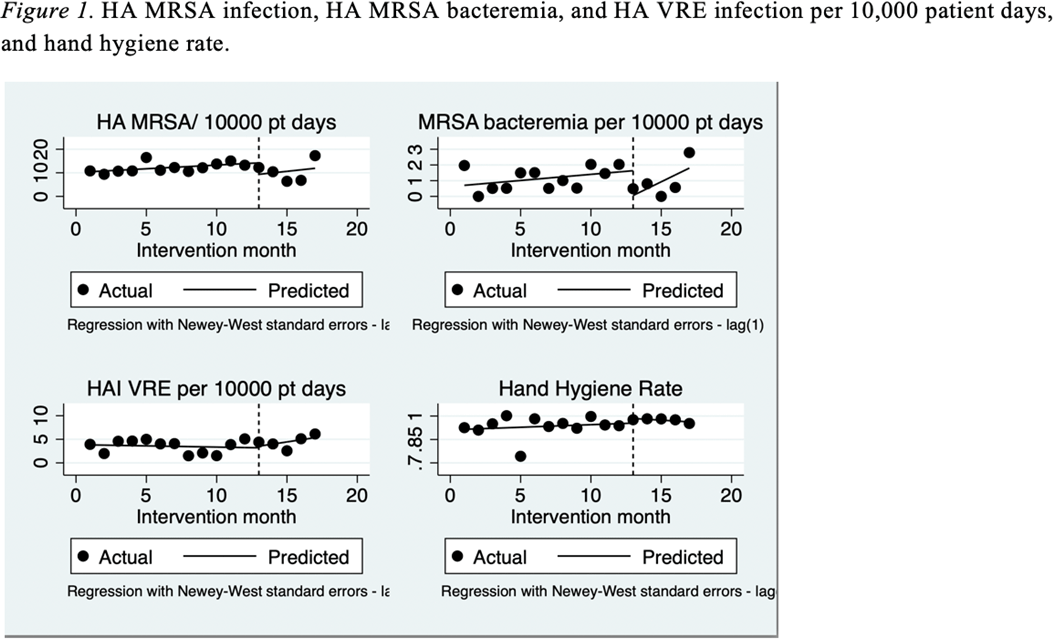
Table 1. 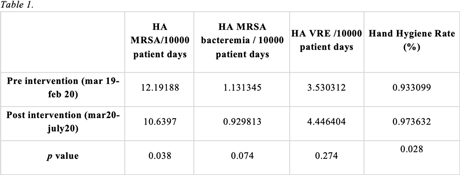


Oral Presentation
Outbreaks
Mycobacterium abscessus Surgical Site Infections Due to Modular Cooler-Heater Units in Cardiac Surgery
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s25
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: In the spring of 2020, we identified 3 patients with organ-space surgical site infections (SSIs) secondary to Mycobacterium abscessus (Table 1). All 3 patients underwent cardiac surgery in the same operating room (OR) during which the CardioQuip Modular Cooler-Heaters (MCHs) were used. We describe key aspects of our cluster investigation, which ultimately led to release of a national safety alert by the Food and Drug Administration (FDA). Methods: For environmental cultures, we obtained samples from 9 MCHs in circulation; 2 scrub sink samples; ice from the OR ice machine; water samples from sinks in the cardiovascular critical care unit, and water samples from floors above the cardiac ORs. All samples were sent for molecular genotyping. For pathway studies, an external environmental engineering team was consulted who conducted smoke pathway tests in 3 different ORs. The team also conducted a particle generator experiment, simulating the set-up of a cardiac bypass surgery case. To assess disinfection practices, we reviewed the manufacturer instructions for use (IFU) protocol of the MCHs and audited our own policies and procedures to ensure compliance. Results: For environmental cultures, molecular typing from 5 of 9 MCHs and all 3 patient SSI isolates returned positive for the identical hybrid species M. abscessus bolleti. All other samples with mycobacterial growth returned with different species. For pathway studies, the particle-generator experiment demonstrated particle movement from the MCH to the sterile field with facilities-guidelines–compliant OR ventilation and despite MCH manufacturing design. For disinfection practices, despite compliance with the stated IFU, and in consultation with experts, we implemented disinfection of associated Quick-connect devices (otherwise not stated in the IFU), and we also initiated a precleaning step prior to disinfection. Conclusions: Our investigation concluded that 3 patients developed SSIs with Mycobacterium abscessus that was aerosolized from the CardioQuip MCH. This finding led to the national FDA safety report alerting providers to risks associated with the device and the need for continued vigilance around disinfection. In addition, we implemented other control measures including placement of MCHs outside all ORs; creation of a separate MCH fleet for non-OR use; and use of modified disinfection protocols. To date, no additional cases have been identified.
Funding: No
Disclosures: None
Table 1. 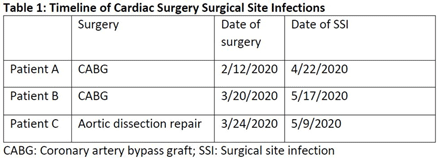

Outbreak of Pseudomonas aeruginosa Bacteremia Infections among Stem-Cell Transplant Patients Related to Change in Prophylaxis
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s25-s26
-
- Article
-
- You have access
- Open access
- Export citation
-
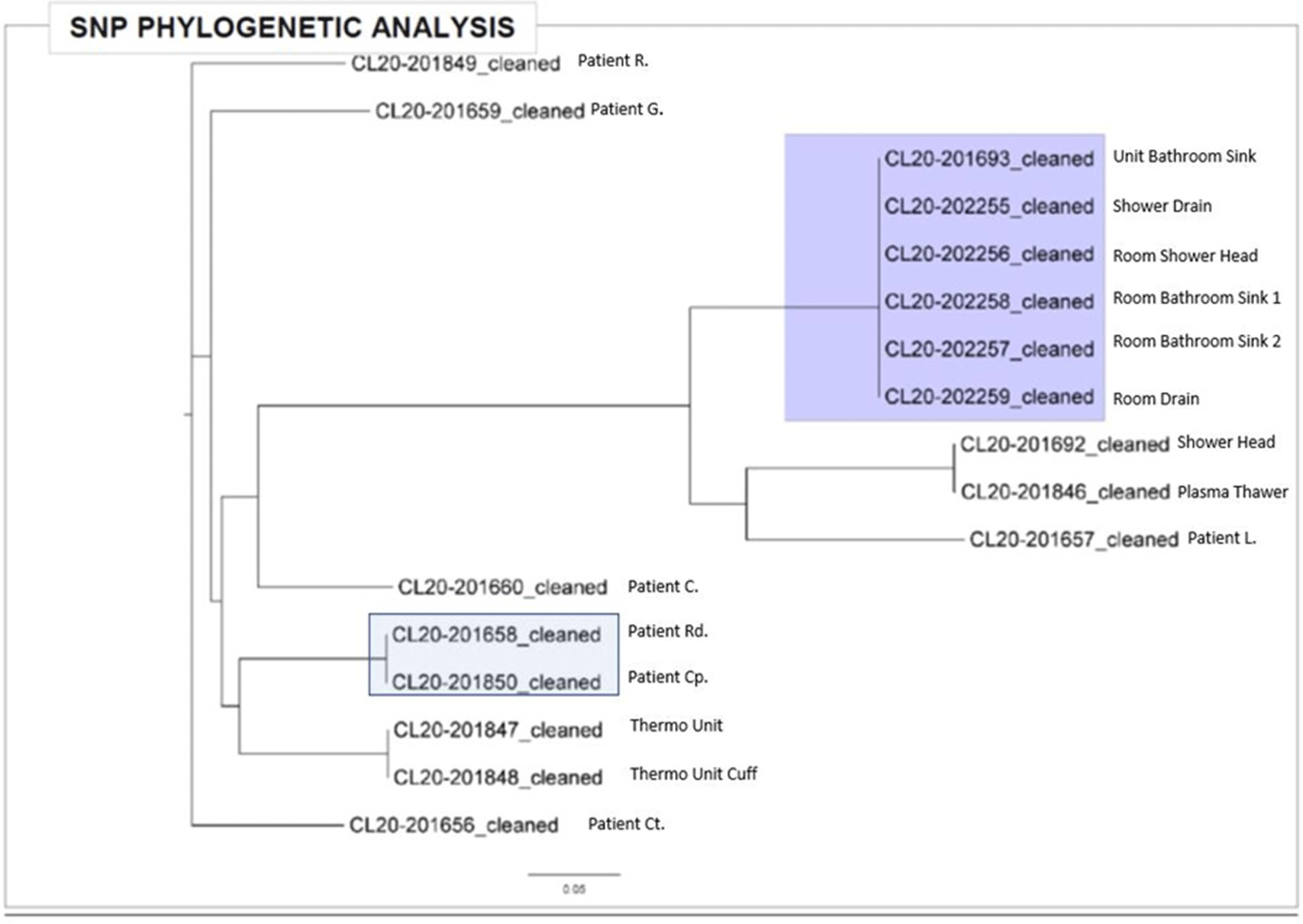
Background:Pseudomonas aeruginosa outbreaks can originate from various sources and can cause severe complications in posttransplant patients. Antibiotic prophylaxis can decrease posttransplant infections; however, consideration must be given to P. aeruginosa coverage as we outline an outbreak among the stem-cell transplant (SCT) population. Methods: A multidisciplinary outbreak investigation was conducted to evaluate sources of contamination and changes in clinical processes. Positive blood cultures from SCT patients and environmental isolates were analyzed using whole-genome sequencing (WGS). Incidence density rates for P. aeruginosa blood cultures from January 2019 through October 2020 were calculated per 10,000 patient days and stratified by unit, specimen, and transplant type. Statistical analysis was calculated with significance at p < 0.05. Results: A cluster of 8 SCT patients was identified between May and September 2020. Moreover, 10 environmental samples were positive for P. aeruginosa including drains, water sources prior to the point-of-use (POU) filter and blood-bank thaw machines. Phylogenetic analysis revealed 1 cluster of 2 patients who shared the same room, 5 patients with unique P. aeruginosa isolates, and 2 separate clusters of environmental isolates with relatedness only to each other. Review of clinical processes showed a change from fluoroquinolone prophylaxis to cephalosporin in the spring of 2020. Also, 5 P. aeruginosa bacteremia infections occurred prior to June (11.78 cases per 10,000 patient days). During the period of cephalosporin use, 8 infections were identified (58.27 cases per 10,000 patient days) (P = .006). Following the restart of fluoroquinolone, zero infections have occurred to date, as of January 28, 2021. Conclusions: Discontinuation of fluoroquinolone prophylaxis was associated with P. aeruginosa bacteremia infections in SCT patients. Use of fluoroquinolone prophylaxis in SCT patients is protective from P. aeruginosa bacteremia infections. There have been no further infections in the following 3 months after the change back to the use of fluoroquinolone. Additionally, WGS showed that most patient isolates did not have a common source, suggesting that P. aeruginosa gastrointestinal colonization may play a role in seeding these bacteremia infections.
Funding: No
Disclosures: None
Figure 1.
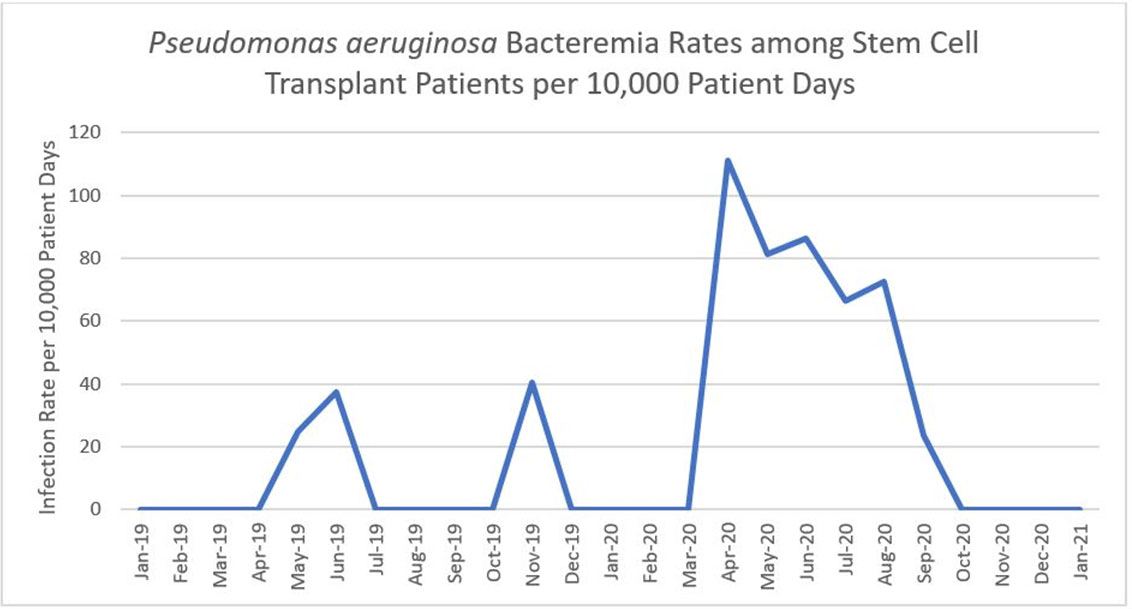
Figure 2.


Verona Integron-Encoded Metallo-Beta-Lactamase (VIM)–Producing Pseudomonas aeruginosa Outbreak Associated with Acute Care
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s26
-
- Article
-
- You have access
- Open access
- Export citation
Successful Control of Human Parainfluenza Type 3 Outbreak in a Level IV Neonatal Intensive Care Unit
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s26-s27
-
- Article
-
- You have access
- Open access
- Export citation
-
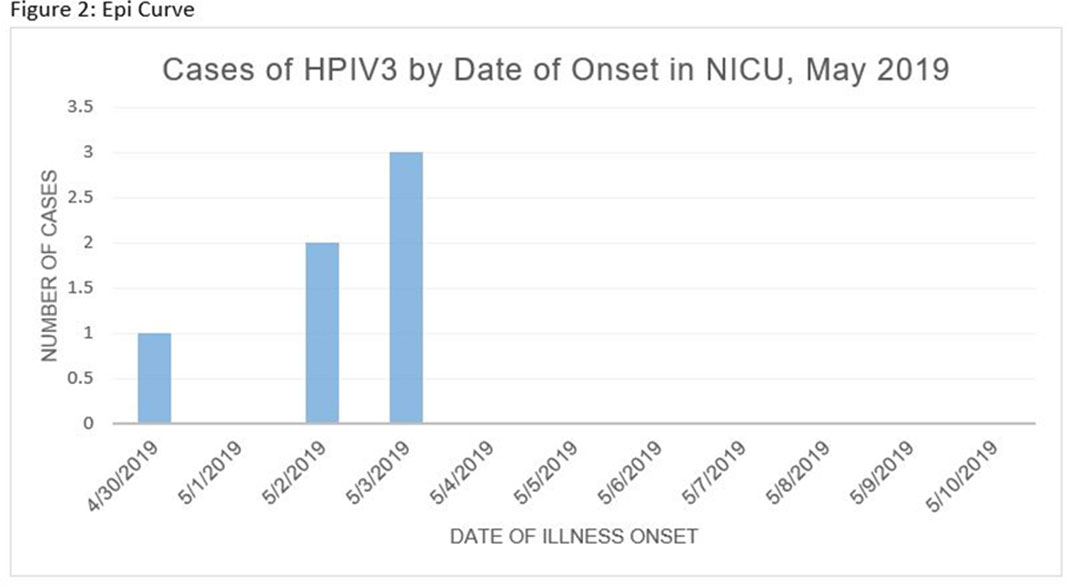
Human parainfluenza (HPIV) is a common cause for upper respiratory tract illnesses (URTI) and lower respiratory tract illnesses (LRTI) in infants and young children. Here, we describe successful control of an HPIV type 3 (HPIV3) outbreak in a neonatal intensive care unit (NICU). NICU babies with new-onset clinical signs or symptoms of RTI and positive HPIV-3 nasopharyngeal specimen by respiratory pathogen panel (RPP) test on hospital day 14 or later were diagnosed with hospital-onset (HO) HPIV-3 infection. After 3 NICU babies were diagnosed with HO HPIV-3, an outbreak investigation was initiated on May 3, 2019, and continued for 2 incubation periods since the last identified case. Enhanced infection prevention measures were immediately implemented. All positive cases were placed in a cohort in a single pod of the NICU and were placed on contact precautions with droplet isolation precautions. Dedicated staffing and equipment were assigned. Environmental cleaning and disinfection with hospital-approved disinfectant wipes was performed daily. Visitors were restricted in the NICU. All employees entering the NICU underwent daily symptom screening for respiratory tract illness. All NICU babies were screened daily for respiratory tract illness with prompt isolation and RPP testing on positive screen. To determine the source of the HPIV3 outbreak, all HPIV3-positive specimens from the NICU and available temporally associated community-onset (CO) controls collected from non-NICU units were sent to the Centers for Disease Control and Prevention (CDC) for whole-genome sequencing (WGS) analysis. The first and last cases of HPIV-3 were diagnosed on May 1 and May 5, 2019, respectively. In total, 7 HO HPIV3 cases were reported: 1 in newborn nursery (NBN) and 6 in NICU. The case from the NBN was determined to be unrelated to the outbreak and the source was linked to a sick visitor. Of the 6 NICU babies, 5 had an LRTI and 1 had a URTI. Average time from admission to diagnosis was 71 days (range, 24–112). None had severe illnesses requiring intubation, and all had full recovery. No CO HPIV3 cases were reported from the NICU during the investigation. A maximum likelihood phylogenetic tree of HPIV3 WGS (Figure 1) showed that sequences from the 6 HO cases clustered together separately from the 3 CO controls, suggesting a single source of transmission, and 3 CO cases were not related to the HO cases or source of the outbreak. Early diagnosis and isolation of respiratory tract viral infections is important to prevent an outbreak. Successful control of outbreak in NICU requires prompt implementation of infection prevention measures with focus on symptom screening, cohorting, and disinfection practices.
Funding: No
Disclosures: None
Figure 1.
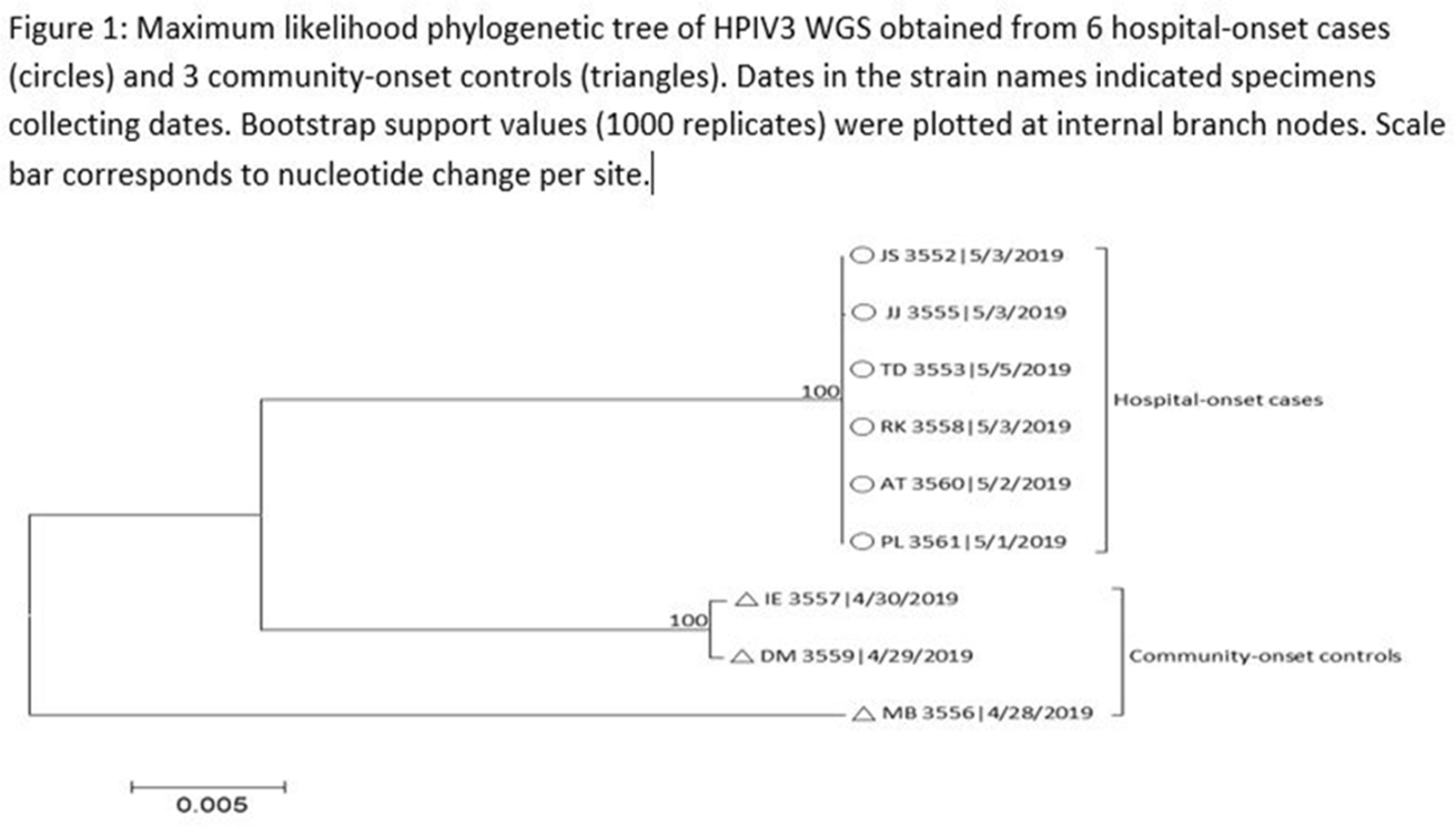
Figure 2.


Pediatrics
Results of a Multicenter Diagnostic Stewardship Collaborative to Optimize Blood Culture Use in Critically Ill Children
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s27
-
- Article
-
- You have access
- Open access
- Export citation
-
Group Name: Bright STAR Authorship Group
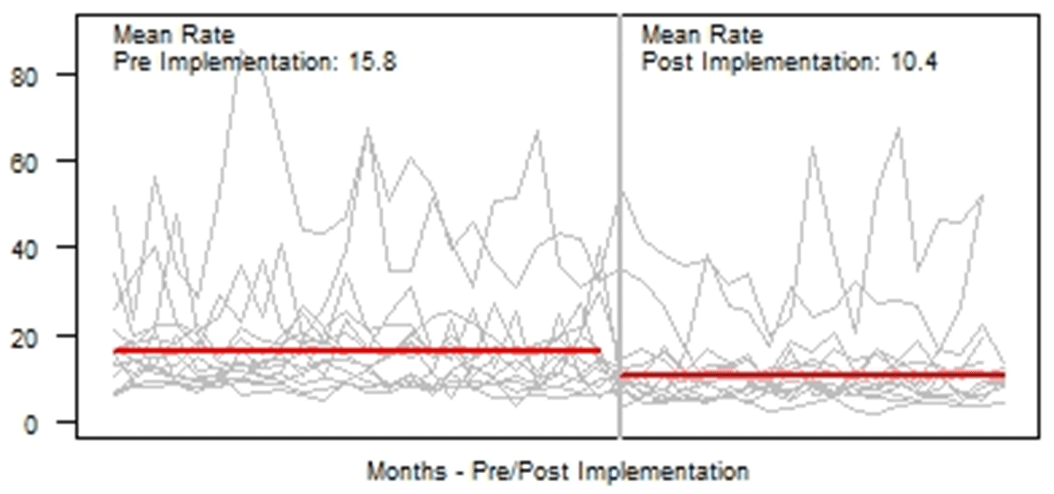
Background: Blood cultures are fundamental in the diagnosis and treatment of sepsis. Culture practices vary widely, and overuse can lead to false-positive results and unnecessary antibiotics. Our objective was to describe the implementation of a multisite quality improvement collaborative to reduce unnecessary blood cultures in pediatric intensive care unit (PICU) patients, and its 18-month impact on blood culture rates and safety metrics. Methods: In 2018, 14 PICUs joined the Blood Culture Improvement Guidelines and Diagnostic Stewardship for Antibiotic Reduction in Critically Ill Children (Bright STAR) Collaborative, designed to understand and improve blood culture practices in critically ill children. Guided by a centralized multidisciplinary study team, sites first reviewed existing evidence for safe reduction of unnecessary blood cultures and assessed local practices and barriers to change. Subsequently, local champions developed and implemented clinical decision-support tools informed by local patient needs to guide new blood-culture practices. The coordinating study team facilitated regular evaluations and discussions of project progress through monthly phone calls, site visits if requested by sites or the study team, and collaborative-wide teleconferences. The study team collected monthly blood culture rates and monitored for possible delays in obtaining blood cultures using a standardized review process as a safety balancing metric. We compared 24 months of baseline data to 18 months of postimplementation using a Poisson regression model accounting for the site-specific patient days and correlation of culture use within a site over time. Results: Across the 14 sites, before implementation, 41,768 blood cultures were collected over 259,701 PICU patient days. The mean preimplementation site-specific blood culture rate was 15.7 cultures per 100 patient days (rate range, 9.6–48.2 cultures per 100 patient days). After implementation, 22,397 blood cultures were collected over 208,171 PICU patient days. The mean postimplementation rate was 10.4 cultures per 100 patient days (rate range, 4.7–28.3 cultures per 100 patient days), which was 33.6% lower than the preimplementation (relative rate 0.66; 95% CI, 0.65–0.68 p <0.01). In 18 months post-implementation, sites reviewed 793 positive blood cultures, and identified only one suspected delay in culture collection possibly attributable to the site’s blood culture reduction program. Conclusions: Multidisciplinary quality improvement teams safely facilitated a 33.6% average reduction in blood culture use in critically ill children at 14 hospitals. Future collaborative work will determine the impact of blood culture diagnostic stewardship on antibiotic use and other important patient safety outcomes.
Funding: No
Disclosures: None
Figure 1.

Association of Antibiotic Duration and Outcomes among NICU Infants with Invasive Staphylococcus aureus Infections
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s27-s28
-
- Article
-
- You have access
- Open access
- Export citation
-
Background:Staphylococcus aureus is the second-leading cause of late-onset sepsis among infants in US neonatal intensive care units (NICUs). Management of S. aureus bacteremia and meningitis in infants varies widely due to the lack of standardized guidelines. We examined the association between initial antibiotic duration and recurrent S. aureus infection or death among NICU infants with S. aureus bacteremia and/or meningitis. Methods: We conducted a retrospective cohort study of infants in Pediatrix Medical Group NICUs from 1997 to 2018 with first episode of S. aureus bacteremia and/or meningitis, identified as having at least 1 blood or cerebrospinal fluid (CSF) culture growing only S. aureus at any point during their NICU stay. Excluded infants were those not started on antistaphylococcal therapy within 2 days of positive culture, those with had endocarditis or osteomyelitis, or those who died or were discharged during or up to 1 day after antibiotic cessation. Antibiotic cessation was defined as last day of antibiotic given if followed by at least 3 days without antibiotics. Multivariable logistic regression was used to analyze the association between antibiotic duration categorized as <14 or ≥14 days) and recurrent SA infection (within 12 weeks of antibiotic cessation, prior to hospital discharge), or death (within 7 days of antibiotic cessation and at discharge). Results: Of 4,086 infants included, 3,991 (98%) had S. aureus bacteremia only and 95 (2%) had meningitis ± bacteremia. Of those with bacteremia only, 2,017 (50.5%), and 17 (18%) of those with meningitis received <14 days antibiotics (Figure 1). Longer antibiotic duration was associated with lower gestational age, methicillin-resistance, severe illness and bacteremia duration of ≥4 days (Table 1). There was a significant association between <14 days antibiotics and recurrent infection (p = 0.04) and 7-day mortality (p = 0.02) in the meningitis cohort. Infants with SA bacteremia who received ≥14 days antibiotics had reduced odds of recurrent SA infection (OR 0.24, 95% CI 0.18-0.32) and death (OR 0.33, 95% CI 0.25-0.44), adjusting for post-natal age, gestational age, sex, methicillin-resistance, severe illness and duration of bacteremia (Table 2). Conclusions: In the largest study thus far examining antibiotic duration among hospitalized infants with S. aureus bacteremia and/or meningitis, ≥14 days antibiotics was associated with decreased odds of recurrent infection or death. Further studies are needed to define the optimal treatment duration and identify clinical factors distinguishing infants able to safely receive a shorter antibiotic duration.
Funding: No
Disclosures: None
Figure 1.
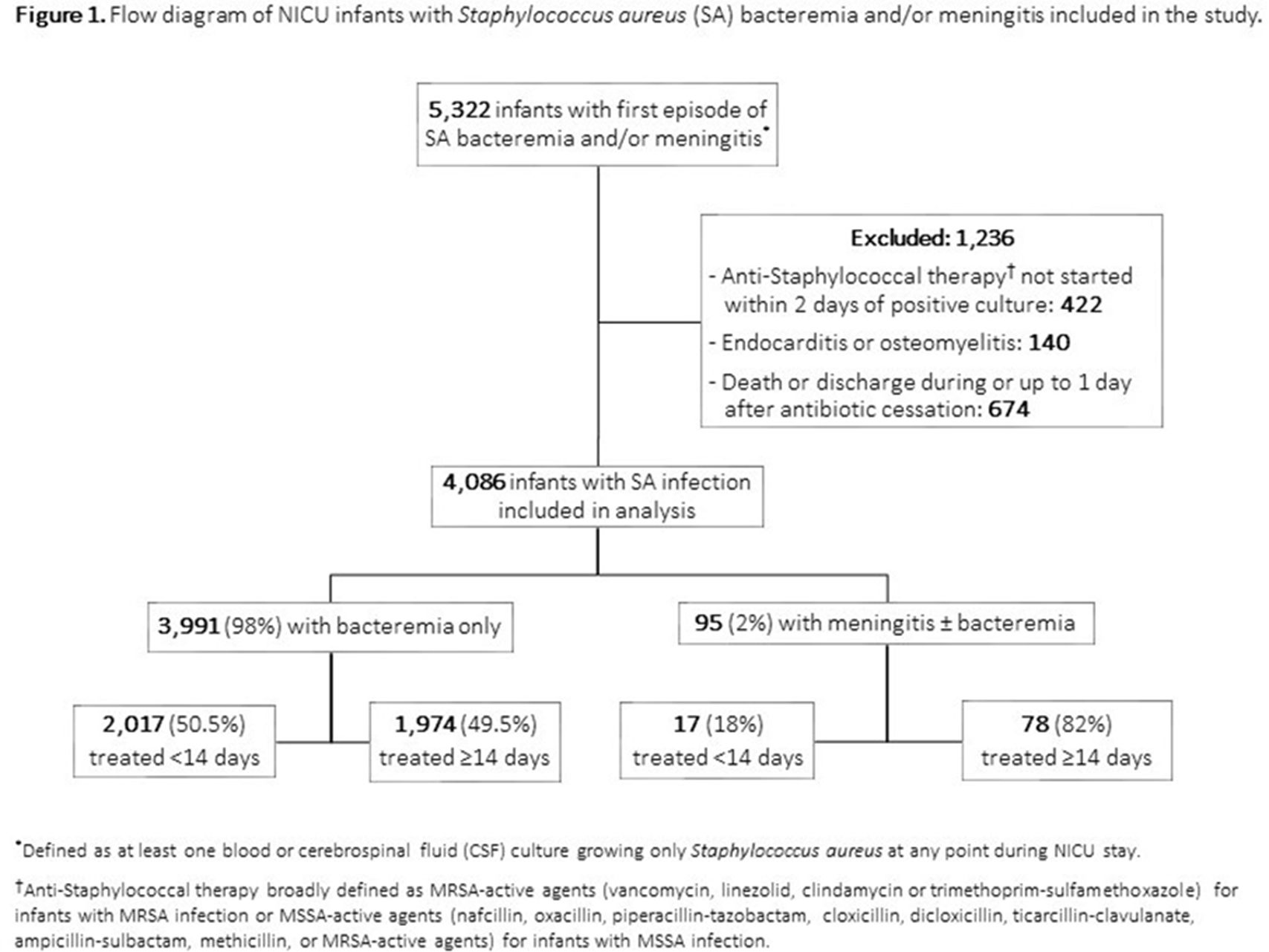
Table 1. 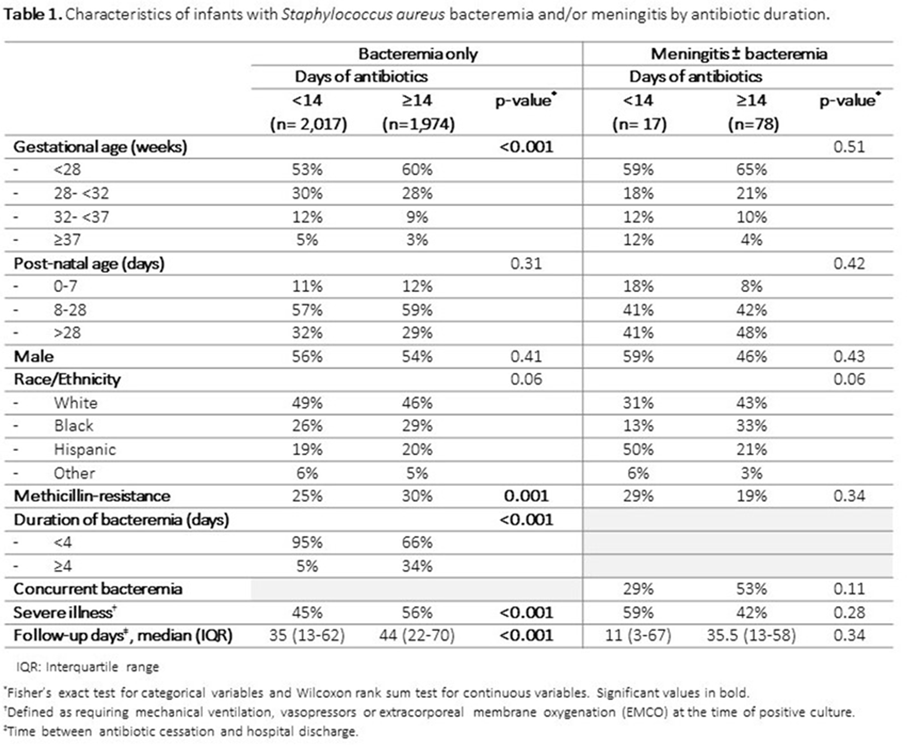
Table 2. 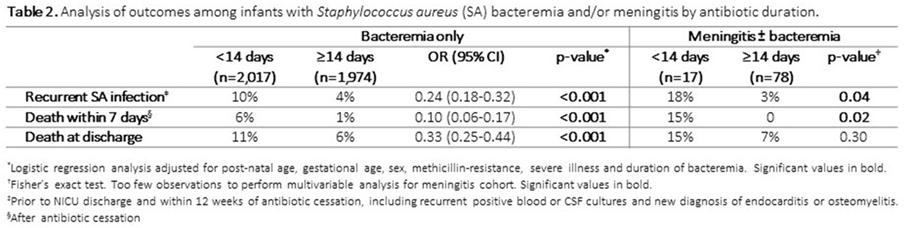



Surveillance/Public Health
Admission and Discharge Sampling Underestimates Multidrug-Resistant Organism (MDRO) Acquisition in an Intensive Care Unit
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s28
-
- Article
-
- You have access
- Open access
- Export citation
-
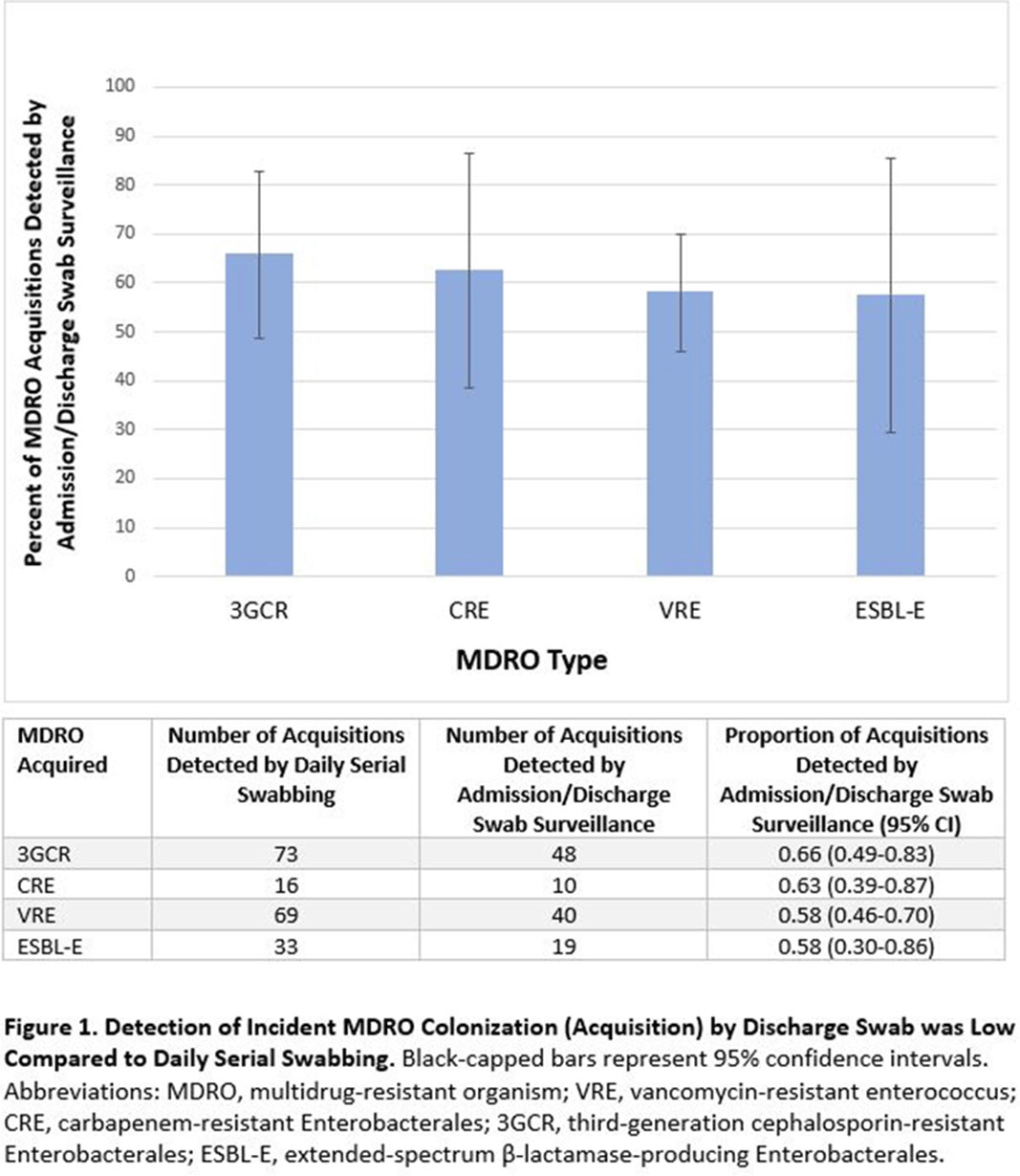
Background: Identification of hospitalized patients with enteric multidrug-resistant organism (MDRO) carriage, combined with implementation of targeted infection control interventions, may help reduce MDRO transmission. However, the optimal surveillance approach has not been defined. We sought to determine whether daily serial rectal surveillance for MDROs detects more incident cases (acquisition) of MDRO colonization in medical intensive care unit (MICU) patients than admission and discharge surveillance alone. Methods: Prospective longitudinal observational single-center study from January 11, 2017, to January 11, 2018. Inclusion criteria were ≥3 consecutive MICU days and ≥2 rectal or stool swabs per MICU admission. Daily rectal or stool swabs were collected from patients and cultured for MDROs, including vancomycin-resistant Enterococcus (VRE), carbapenem-resistant Enterobacterales (CRE), third-generation cephalosporin-resistant Enterobacterales (3GCR), and extended-spectrum β-lactamase–producing Enterobacterales (ESBL-E) (as a subset of 3GCR). MDRO detection at any time during the MICU stay was used to calculate prevalent colonization. Incident colonization (acquisition) was defined as new detection of an MDRO after at least 1 prior negative swab. We then determined the proportion of prevalent and incident cases detected by daily testing that were also detected when only first swabs (admission) and last swabs (discharge) were tested. Data were analyzed using SAS version 9.4 software. Results: In total, 939 MICU stays of 842 patients were analyzed. Patient characteristics were median age 64 years (interquartile range [IQR], 51–74), median MICU length of stay 5 days (IQR, 3–8), median number of samples per admission 3 (IQR, 2–5), and median Charlson index 4 (IQR, 2–7). Prevalent colonization with any MDRO was detected by daily swabbing in 401 stays (42.7%). Compared to daily serial swabbing, an admission- and discharge-only approach detected ≥86% of MDRO cases (ie, overall prevalent MDRO colonization). Detection of incident MDRO colonization by an admission- or discharge-only approach would have detected fewer cases than daily swabbing (Figure 1); ≥34% of total MDRO acquisitions would have been missed. Conclusions: Testing patients upon admission and discharge to an MICU may fail to detect MDRO acquisition in more than one-third of patients, thereby reducing the effectiveness of MDRO control programs that are targeted against known MDRO carriers. The poor performance of a single discharge swab may be due to intermittent or low-level MDRO shedding, inadequate sampling, or transient MDRO colonization. Additional research is needed to determine the optimal surveillance approach of enteric MDRO carriage.
Funding: No
Disclosures: None
Figure 1.

Poster Presentation
Antibiotic Stewardship
Periprocedural Testing and Antimicrobial Prophylaxis for Ureteral Stent Removal: An Opportunity for Antimicrobial Stewardship
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s29
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: The American Urologic Association’s 2019 Best Practices Statement highlights the importance of procedural and host factors in optimizing antimicrobial prophylaxis for urologic procedures. For ureteral stent removal, a procedure considered low risk, the recommendation for prophylaxis is uncertain and is dependent primarily on patient factors. We examined periprocedural practices and outcomes for both low-risk and intermediate- to high-risk patients undergoing this procedure in a county hospital. Methods: A retrospective cohort study was performed on all patients who underwent stent removal from January to December 2019. Patients were classified as being low risk if they met the following criteria: age 48 hours within the previous 30 days, absence of external urinary catheters, no intermittent catheterization, absence of prosthetic cardiac valves, not pregnant, and not immunocompromised. All other patients were classified as intermediate to high risk. We assessed periprocedural urine testing, antimicrobial prophylaxis, and clinical outcomes. Results: Of 158 unique patients, 84 (53%) were classified as low risk. As shown in Table 1, preprocedural urine cultures were performed in 55% of low-risk versus 69% of intermediate- to high-risk patients. For the patients for whom urine cultures were performed, cultures were positive in 22% of low-risk versus 55% of intermediate- to high-risk patients (p < .0001). All patients received antimicrobial prophylaxis, most often a single dose after the procedure. None of the low risk patients had a positive urine culture or hospitalization within 30 days post procedure. Conclusions: Overall, 53% of patients undergoing stent removal were considered low-risk hosts, yet 100% of patients received antimicrobial prophylaxis. Future studies are needed to evaluate interventions to reduce unnecessary antimicrobial prophylaxis and standardize preprocedural testing in low-risk patients undergoing stent removal.
Funding: No
Disclosures: None
Table 1. 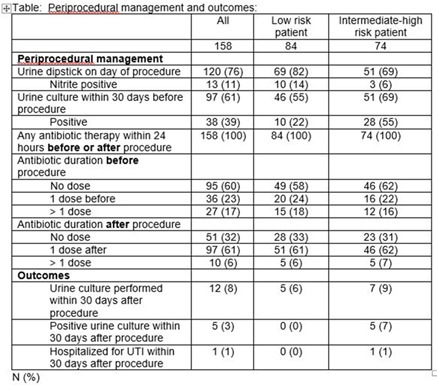

Promoting Antimicrobial Stewardship Education Among Pediatricians Through a Maintenance of Certification Part 4 Quality Impro
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s29
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: The rise of antimicrobial resistance has made it critical for clinicians to understand antimicrobial stewardship principles. We sought to determine whether the opportunity to participate in an American Board of Pediatrics Maintenance of Certification Part 4 (MOC4) quality improvement (QI) project would engage pediatricians and improve their knowledge about antimicrobial stewardship. Methods: In August 2019, a new clinical algorithm for acute appendicitis, spearheaded by the antimicrobial stewardship program (ASP), was implemented at UCSF Benioff Children’s Hospital Oakland to standardize care and optimize antimicrobial use. Medical staff were invited to participate in a QI project evaluating the impact of this algorithm. Data were collected for the 2 quarters preceding implementation (baseline), for the quarter of implementation (transition period), and for the quarter after implementation. Participants were offered MOC4 credit for reviewing these 3 cycles of data and associated materials highlighting information about antimicrobial stewardship. An initial survey was given to participants to assess their baseline knowledge via 4 questions about antimicrobial use in surgical patients (Table 1). At the conclusion of the QI project, another survey was conducted to reassess participant knowledge and to evaluate overall satisfaction with the project. Results: In total, 150 clinicians completed the initial survey. Of these, 44% were general pediatricians and 56% were pediatric subspecialists. Based on years out of training, their levels of experience varied: >20 years in 24%, 11–20 years in 32.7%, 0–10 years in 34.7%, and currently in training in 8.7%. Of the 150 initial participants, 133 (89%) completed the QI project and the second survey. Between surveys, there was significant improvement in knowledge about the appropriate timing and duration of surgical antibiotic prophylaxis (Table 1). Moreover, 88% of participants responded that the QI project was extremely effective in helping them learn about antimicrobial stewardship principles and about ASP interventions. Conclusions: Participation in this MOC4 QI project resulted in significant improvement in knowledge about antimicrobial use in surgical patients, and the activity was perceived as a highly effective way to learn about antimicrobial stewardship. QI projects that leverage MOC4 credit can be a powerful tool for engaging pediatricians and disseminating education about antimicrobial stewardship.
Funding: No
Disclosures: None
Table 1. 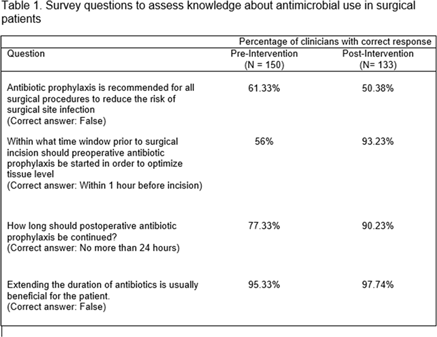

Appropriateness of Antibiotic Duration at the Time of Hospital Discharge
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s30
-
- Article
-
- You have access
- Open access
- Export citation
-
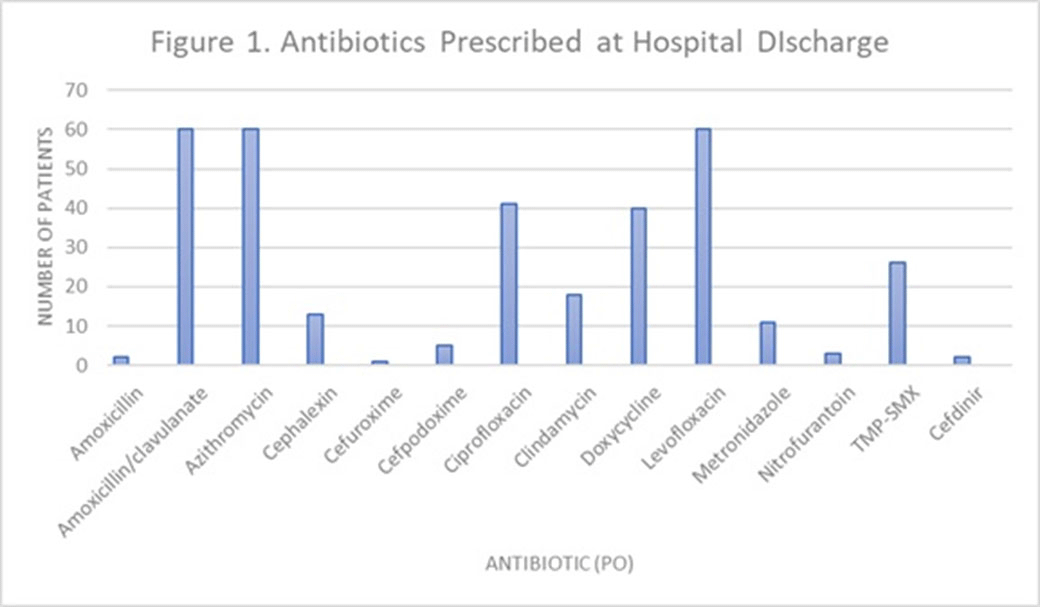
Background: Antimicrobial stewardship initiatives usually occur in the inpatient setting, and they are often lacking at transitions of care (TOC), including hospital discharge. We assessed the appropriateness of antibiotic treatment duration at the time of discharge from our institution. Methods: This retrospective chart review included 300 adult patients discharged on oral antibiotics for acute infections during a 3-month period in 2019. The primary outcome was the duration of antibiotic therapy (DOT). To assess appropriateness, we compared the prescribed DOT (1) to that recommended by clinical guidelines, (2) to the minimum supported by clinical trials, and (3) to the period beyond the point of clinical stability, defined as normal vital signs with improvement in symptoms present from diagnosis. Each indication and antibiotic was assessed using standards appropriate for the combination. Results: Results are shown in Tables 1 and 2 and Figure 1. Conclusions: Antibiotics were often given longer than necessary on hospital discharge. In this study, patients received a median 2 days of excess antibiotics compared to recommended guidelines and 6 days after reaching clinical stability. A pilot TOC stewardship program was initiated to address this problem.
Funding: No
Disclosures: None
Table 1. 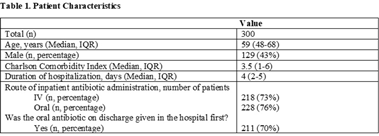
Table 2. 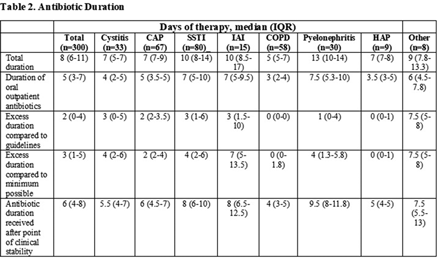
Figure 1.



Adherence to Antibiotic Stewardship Program Associated with Shorter Course of Treatment and Fewer Adverse Events
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s30-s31
-
- Article
-
- You have access
- Open access
- Export citation
-
Group Name: NorthShore University HealthSystem
Background: Prolonged antibiotic use has been attributed to an increased incidence of adverse drug events (ADEs). Cessation of unnecessary antibiotics would decrease length of treatment and may help prevent these adverse events. We evaluated whether an antibiotic stewardship intervention aimed at stopping unnecessary antibiotic usage would both shorten the duration of treatment and reduce ADEs. Methods: At NorthShore University HealthSystem, a 4-hospital, 832-bed system, we identified patients who were started on empiric antibiotics during a hospital admission between May 2, 2016, and June 30, 2018. Within 24 hours of antibiotic initiation, an infectious disease (ID) physician reviewed each patient chart. If the patient was unlikely to have a symptomatic bacterial infection, the ID physician left a note in the electronic medical record (EMR) recommending antibiotic cessation. Two physician reviewers retrospectively reviewed whether the treatment team accepted these recommendations and assessed potential ADEs for 30 days after the recommendation through inpatient and outpatient notes in the EMR. These ADEs were defined using previously published criteria. If the 2 reviewers disagreed on the presence of an ADE, an ID physician acted as the tie breaker. We compared the number of antibiotic days and the number of ADEs between cases in which the recommendations were followed and cases in which they were not. Results: We reviewed 168 cases: 78 (46.43%) followed recommendations and 90 (53.57%) did not. There were no significant differences in baseline patient characteristics between the 2 groups. There was a significant difference in total ADEs between the 2 groups: in 6 cases (7.69%) the recommendations were followed, and 21 (23.33%) they were not followed (P = .011). There was also a significant difference in antibiotic days between cases in which recommendations were followed (1.40 days) versus those in which they were not followed (1.99 days) (p < 0.001). Conclusions: Antibiotic-associated adverse events can cause harm to patients and increase healthcare costs, particularly when used for patients who are unlikely to have a bacterial infection. An antibiotic stewardship program to identify patients in an EMR who are unlikely to benefit from antibiotic use can decrease the length of total antibiotic usage and help prevent adverse events.
Funding: No
Disclosures: None
Table 1. 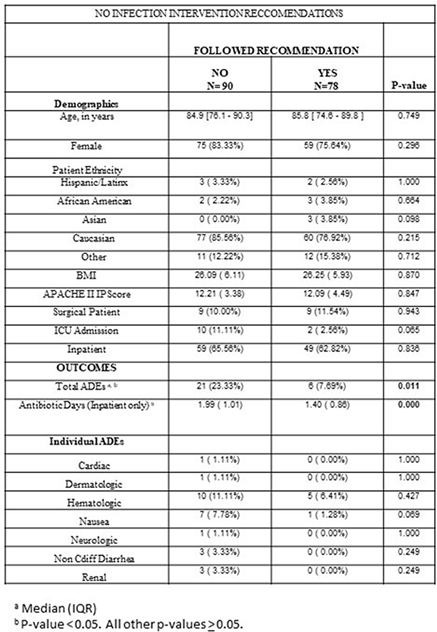

Successful Treatment of Invasive MRSA Infections in Children Using Area Under the Vancomycin Concentration-Time Curve Divided by the Minimum Inhibitory Concentration (AUC/MIC) to Measure Vancomycin Exposure
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s31
-
- Article
-
- You have access
- Open access
- Export citation
-
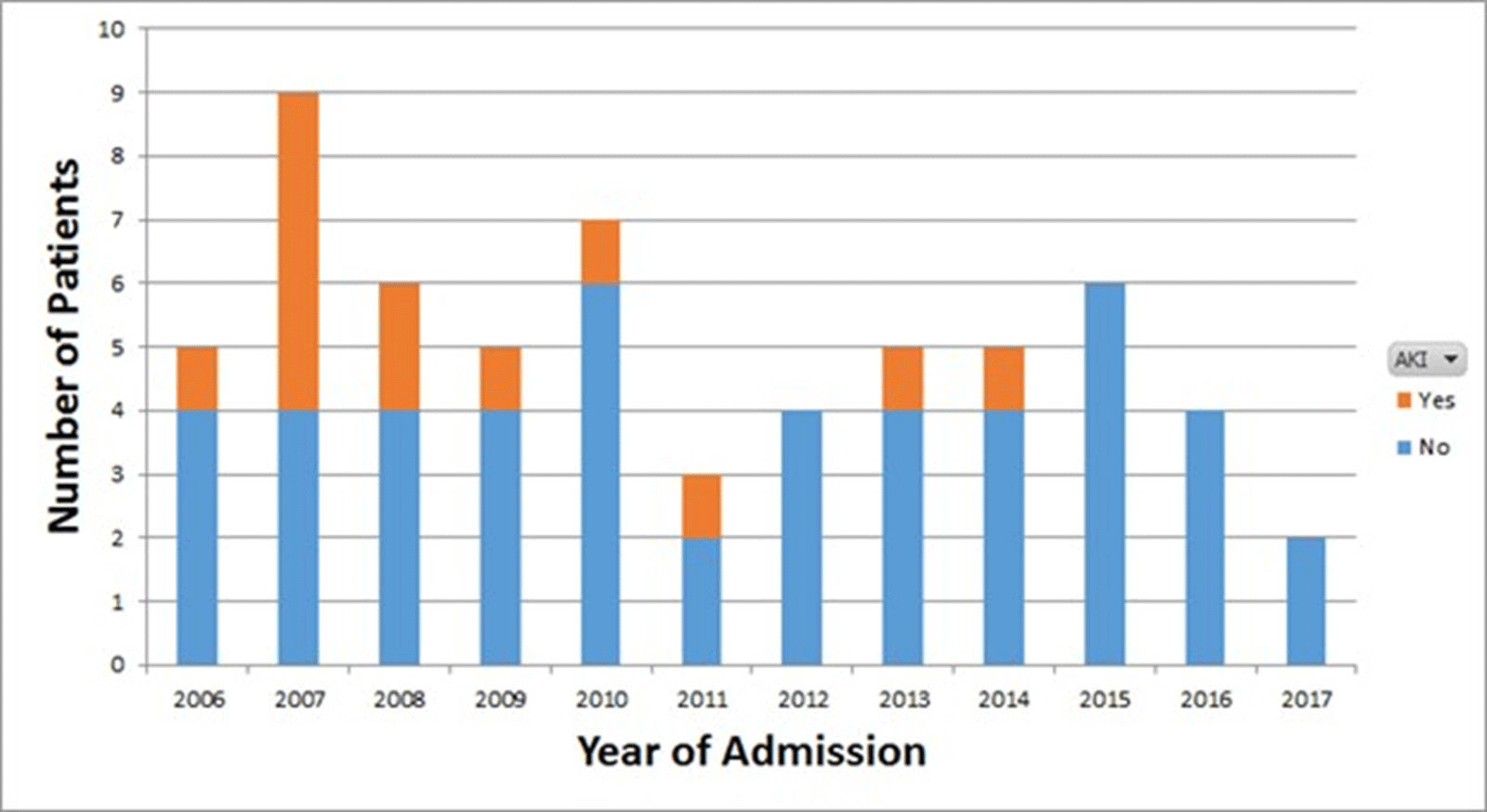
Background: Vancomycin is the treatment of choice for invasive methicillin-resistant Staphylococcus aureus (MRSA) infections. Previous guidelines issued by the Infectious Diseases Society of America (IDSA) recommended targeting vancomycin serum trough concentrations of 15–20 mg/L; however, troughs <15 mg/L are also associated with increased odds of renal toxicity. To minimize toxicity, recently updated ASHP/IDSA/PIDS vancomycin dosing guidelines recommend the use of an area under the vancomycin concentration-time curve divided by the minimum inhibitory concentration (AUC/MIC) pharmacodynamic index to measure vancomycin exposure, with an AUC/MIC ratio >400 correlating with clinical efficacy. However, data on vancomycin therapeutic drug monitoring (TDM) in children are limited. Our institutional practice since January 2009 has been to use AUC/MIC, rather than serum trough concentrations, to guide vancomycin dosing. In this study, we describe clinical outcomes in vancomycin-treated children with invasive MRSA infections using this dosing method. Methods: We performed a retrospective chart review of children hospitalized with invasive MRSA infections between 2006 and 2019 at Rady Children’s Hospital in San Diego, California. Clinical, microbiologic, and pharmacologic data including the site of MRSA infection, clinical failure or cure, occurrence of acute kidney injury (AKI), vancomycin MIC, vancomycin AUC, and serum trough concentrations were collected. Results: In total, 61 invasive MRSA cases were reviewed: 20 were admitted January 2016 through December 2008, and 41 were admitted January 2009 through June 2019 (Figure 1). Most patients did not have medical comorbidities. The most common types of infections were primary bacteremia (34%) and osteomyelitis (32%). Of 61 children, 50 (82%) had positive clinical outcomes regardless of vancomycin dosing method. Of 20 patients, 8 (40%) admitted prior to January 2009 developed AKI, compared with 5 (12%) of 41 patients admitted after January 2009. Conclusions: In our retrospective review, most patients had clinically successful outcomes regardless of which dosing strategy was used. We found higher rates of renal toxicity in patients who were admitted prior to 2009, with TDM based on measuring peak and trough concentrations, compared with those using AUC/MIC for TDM. Our findings suggest that AUC/MIC TDM for invasive MRSA infections may be associated with lower rates of renal toxicity.
Funding: No
Disclosures: None
Figure 1.

Diagnostic Stewardship in Lower Respiratory Tract Infections Using Procalcitonin
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s31-s32
-
- Article
-
- You have access
- Open access
- Export citation
Antimicrobial Stewardship in Acute-Care Hospitals: A Report of the California Healthcare-Associated Infections Honor Roll
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s32
-
- Article
-
- You have access
- Open access
- Export citation
Identification of Potentially Unnecessary Micafungin Use Patterns: Opportunities for Antifungal Stewardship Interventions
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s32-s33
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Echinocandins are used as first-line therapy for suspected and confirmed Candida spp, and its indiscriminate use may drive selection for echinocandin resistance. We evaluated patterns of use of micafungin to identify opportunities for antifungal stewardship. Methods: We identified all micafungin completed orders and microbiological test result data from July 2018 to November 2020 among hospitalized patients in Barnes-Jewish Hospital. Continuous micafungin courses with <48 hours of interruption were considered independent courses. We evaluated micafungin use in 3 scenarios in which its use may be unnecessary: (1) patients with blood cultures negative for Candida spp, (2) patients with recovery of yeast or Candida spp from tracheal aspirates, and (3) patients with recovery of yeast or Candida spp from urine cultures. We only included micafungin courses if they were initiated within 5 days of blood culture collection or up to 4 days after tracheal or urine culture collection to account for incubation and decision to initiate treatment. Results: We found 3,381 micafungin courses in 3,287 admissions. Of these, 2,532 courses had blood culture collection around micafungin initiation and were included in the first analysis: 1,879 (74%) were negative, 149 (6%) had Candida spp isolated in the blood, and 504 (20%) had positive blood cultures for other organisms. Micafungin was given for a median duration of 3 days (IQR, 2–7) to those with negative blood cultures and for 3 days (IQR, 1–5) to those with positive blood cultures without candidemia (p < 0.001), and prolonged durations of more than 5 days was seen in 768/1879 (41%) and 143/504 (28%) of courses, respectively (p <0.001). A total of 487 micafungin courses were initiated after tracheal aspirate culture collection. Those with yeast isolated (n = 100, 21%) received similar micafungin duration compared to those that had no yeast isolated [3 (2-7 IQR) vs. 3 (2-7) days, respectively; p = 0.56). Finally, a total of 844 micafungin courses started after urine culture collection. A total of 49 (6%) had yeast isolated from the urine and treatment duration was similar to those that did not [3 (1-6 IQR) vs. 3 (2-6) days, respectively; p = 0.87). Conclusions: Echinocandin treatment courses did not differ when a yeast was identified from a tracheal isolate or urine specimen. However, a substantial proportion of treatment courses were prolonged in those with negative Candida spp in the blood, suggesting opportunities for antifungal stewardship interventions.
Funding: No
Disclosures: None
Table 1. 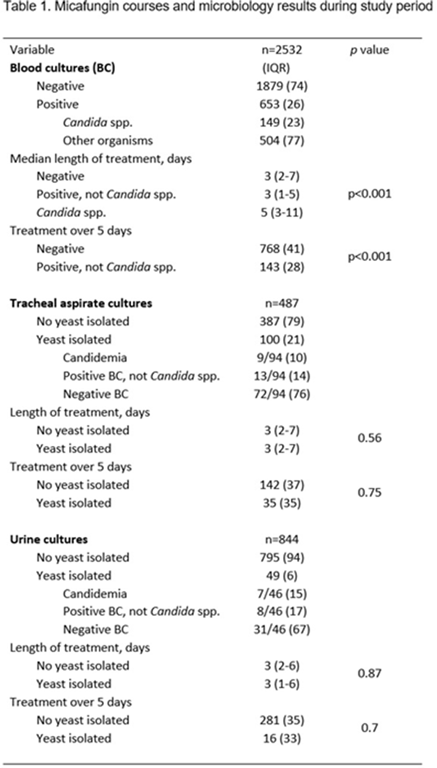

Veteran Satisfaction for Upper Respiratory-Tract Infection (URI) Visits Is Not Associated with Antibiotic Receipt But Is Associated with Antibiotic Expectation
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s33
-
- Article
-
- You have access
- Open access
- Export citation
-
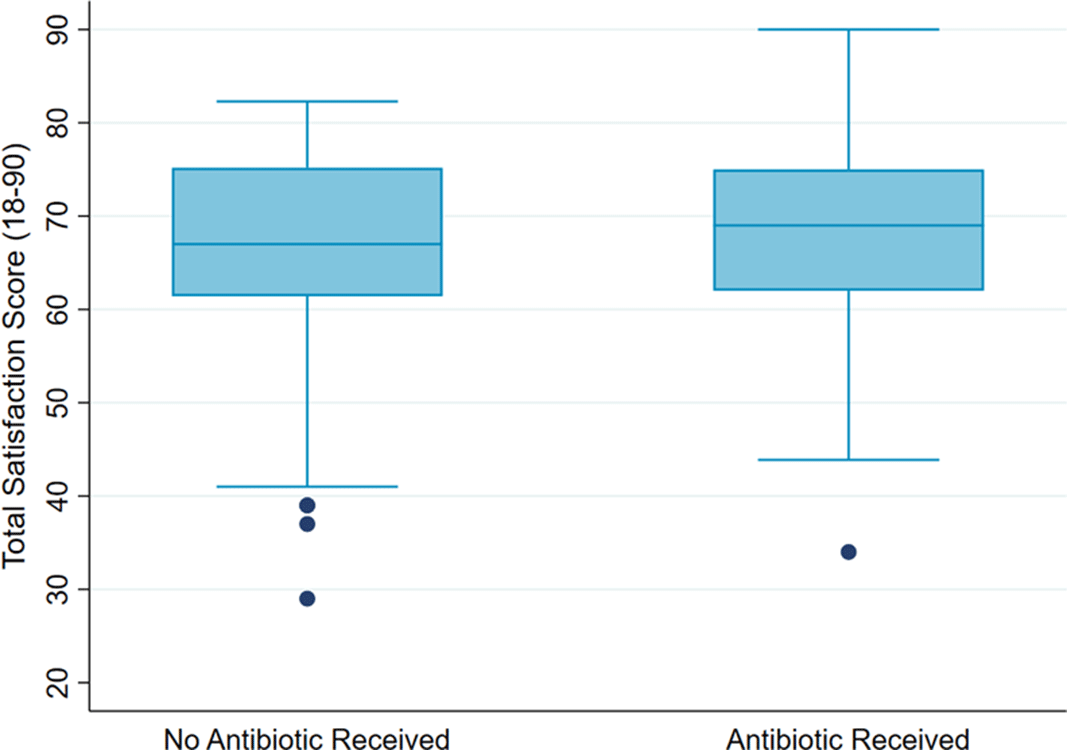
Background: Antibiotics are not recommended but are often prescribed for upper respiratory-tract infections (URIs). Prescribers cite patient expectation as a driver of inappropriate antibiotic prescribing; prior literature has demonstrated higher satisfaction scores in patients who receive antibiotics compared to those who do not. We assessed whether veteran satisfaction at URI visits was associated with antibiotic receipt or with reported expectation for antibiotics. Methods: We surveyed veterans with documented URI encounters in the Veterans’ Affairs Tennessee Valley Healthcare System between January 1, 2018, and December 31, 2019. Patients not evaluated in person, with documented dementia, or who died prior to the study start date were excluded. Veterans were asked to recall their URI visit and to complete the Patient Safety Questionnaire (PSQ)-18 (Rand Corporation) and questions assessing antibiotic expectations. The PSQ-18, an 18-item survey that assesses patient satisfaction, uses a 5-point Likert scale (ie, strongly disagree, disagree, uncertain, agree, strongly agree), yielding a composite score of 18–90. Higher scores represent more satisfaction with care. Demographic and visit-specific information were extracted via chart review. We used multivariable linear regression to assess differences in composite PSQ-18 satisfaction scores between those who did and did not receive an antibiotic, adjusted for patient and visit characteristics, and to assess differences in satisfaction scores for those who did and did not report expecting antibiotics, adjusted for antibiotic receipt. Results: We identified 1,435 patients seen for URI at 17 sites. After exclusions, 1,343 veterans were eligible for chart abstraction. After excluding 42 responders who responded after study close or returned blank surveys, the final analytic cohort included 432 (32.2%) of 1,343 responders; 225 (52.1%) received an antibiotic and 207 (47.9%) did not. Mean total satisfaction for veterans who received an antibiotic was 67.8 (SD, ±9.4) compared to 66.7 (SD, ±9.7) for those who did not (Figure 1). Increased total satisfaction was not significantly associated with antibiotic receipt (0.65; 95% CI, −2.0 to 3.3). Most veterans (72.0%) disagreed that visit satisfaction depended on antibiotic receipt. However, only 30.8% reported that they would not expect an antibiotic for URI visits. A significant reduction in total satisfaction (−4.1; 95% CI, −6.3 to −1.9) was associated with expecting compared to not expecting an antibiotic. Conclusions: Our findings suggest that prescribing an antibiotic is not associated with increased veteran satisfaction for URI visits but is associated with expecting an antibiotic. Future work will evaluate methods to change veteran antibiotic expectations.
Funding: No
Disclosures: None
Figure 1.

Evaluation of Procalcitonin Use in Patients Discharged from the Emergency Department with Acute Respiratory Infection
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s33-s34
-
- Article
-
- You have access
- Open access
- Export citation