
54 results
4 Risk Factor and Biomarker Correlates of FLAIR White Matter Hyperintensities in Former American Football Players
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 608-610
-
- Article
-
- You have access
- Export citation
53 Change in Cerebral Metabolite Concentrations Following Bariatric Surgery
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 462-463
-
- Article
-
- You have access
- Export citation
EMS Calls for Service at Adult Detention Centers–A Descriptive Study
-
- Journal:
- Prehospital and Disaster Medicine / Volume 38 / Issue S1 / May 2023
- Published online by Cambridge University Press:
- 13 July 2023, p. s136
- Print publication:
- May 2023
-
- Article
-
- You have access
- Export citation
Immediate Medical Care Rendered by U.S. Law Enforcement Officers After Officer-Involved Shootings – An Open-Access Public Domain Video Analysis
-
- Journal:
- Prehospital and Disaster Medicine / Volume 38 / Issue S1 / May 2023
- Published online by Cambridge University Press:
- 13 July 2023, p. s46
- Print publication:
- May 2023
-
- Article
-
- You have access
- Export citation
Developing Prepositioned Burn Care-Specific Disaster Resources for a BMCI
-
- Journal:
- Prehospital and Disaster Medicine / Volume 38 / Issue S1 / May 2023
- Published online by Cambridge University Press:
- 13 July 2023, pp. s46-s47
- Print publication:
- May 2023
-
- Article
-
- You have access
- Export citation
Immediate Medical Care Rendered by US Law Enforcement Officers after Officer-Involved Shootings – An Open-Access Public Domain Video Analysis
-
- Journal:
- Prehospital and Disaster Medicine / Volume 38 / Issue 2 / April 2023
- Published online by Cambridge University Press:
- 06 March 2023, pp. 168-173
- Print publication:
- April 2023
-
- Article
- Export citation
Mixed-methods process evaluation of a respiratory-culture diagnostic stewardship intervention
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 2 / February 2023
- Published online by Cambridge University Press:
- 03 January 2023, pp. 191-199
- Print publication:
- February 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Precise Limb Tourniquet Arterial Occlusion Pressure Determination using Real-Time Ultrasonography and a Capacitive-Based Force Sensor
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 18 October 2022, pp. 772-777
- Print publication:
- December 2022
-
- Article
- Export citation
The Composition and Distribution of Ethnic Groups in Belize: Immigration and Emigration Patterns, 1980-1991
-
- Journal:
- Latin American Research Review / Volume 32 / Issue 3 / 1997
- Published online by Cambridge University Press:
- 05 October 2022, pp. 63-88
-
- Article
-
- You have access
- Export citation
Empirically-identified subgroups of children with autism spectrum disorder and their response to two types of cognitive behavioral therapy
-
- Journal:
- Development and Psychopathology / Volume 35 / Issue 3 / August 2023
- Published online by Cambridge University Press:
- 06 December 2021, pp. 1188-1202
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Staffing in a Level 1 Trauma Center: Quantifying Capacity for Preparedness
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 16 / Issue 5 / October 2022
- Published online by Cambridge University Press:
- 15 September 2021, pp. 1990-1996
-
- Article
- Export citation
Indications for and Utility of Tracheal Aspirate Cultures for the Diagnosis of VAI
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, pp. s60-s61
-
- Article
-
- You have access
- Open access
- Export citation
-
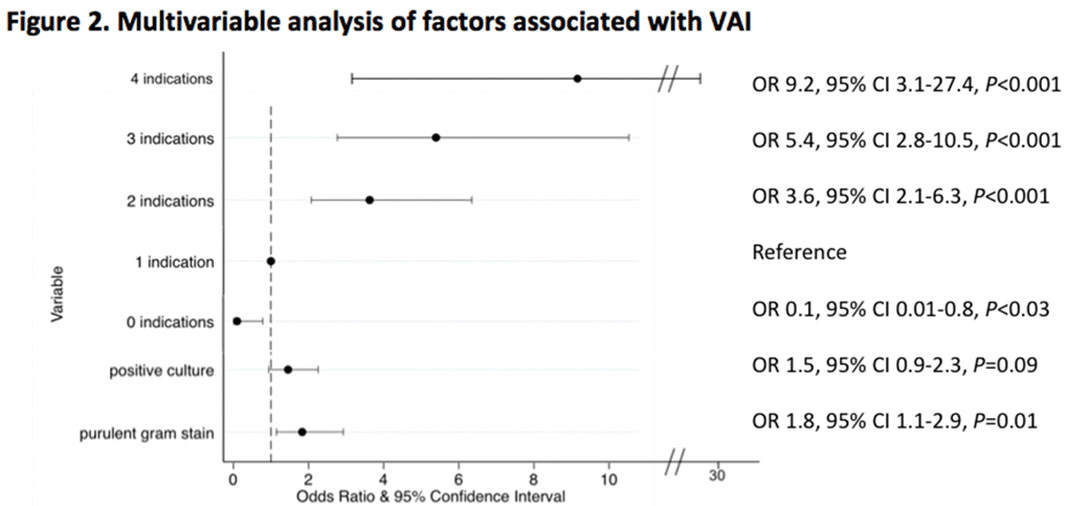
Background: Tracheal aspirate bacterial cultures are routinely collected in mechanically ventilated children for the evaluation of ventilator-associated infections (VAIs). However, frequent bacterial colonization of endotracheal and tracheostomy tubes contribute to the marginal performance characteristics of the test for diagnosing VAI. Published literature characterizing drivers of culture collection and the predictive value of positive cultures are limited. Methods: This single-center, retrospective cohort study included children admitted to the pediatric intensive care unit who were receiving mechanical ventilation for at least 48 hours and had 1 or more semiquantitative tracheal aspirate cultures collected between September 1, 2019, and August 31, 2020. Indications for culture collection were determined through medical record review and included fever, hypothermia, tracheal secretion changes, radiographic pneumonia, increased oxygen requirement, and/or increased positive end-expiratory pressure (PEEP). A positive culture was defined as moderate or heavy growth of a noncommensal bacterial organism. A purulent Gram stain was defined as detection of moderate or many white blood cells. Diagnosis of VAI was based on treating-clinician documentation and was ascertained through medical record review. Logistic regression accounting for clustering by patient was performed to estimate the association between indications for culture collection and (1) culture positivity, (2) purulent Gram stain, and (3) diagnosis of VAI. Results: In total, 625 tracheal aspirate cultures were performed in 261 unique patients. Common indications for culture collection included isolated fever or hypothermia (n = 124, 20%), fever with an increase in oxygen requirement or PEEP (n = 71, 11%), isolated increase in oxygen requirement or PEEP (n = 67, 11%), or isolated secretion change (n = 54, 9%) (Figure 1). Overall, 230 cultures (37%) were positive and 218 (35%) Gram stains were purulent. There were no associations between culture indications and a positive culture. Presence of isolated fever was negatively associated with a purulent Gram stain (odds ratio [OR], 0.49; 95% CI, 0.30–0.81; P = .005); otherwise, there were no associations between indication and purulent Gram stain. Finally, in a multivariable model, odds of VAI diagnosis increased with both the number of indications for culture collection and purulent Gram stain, but not with positive culture (Figure 2). Conclusions: Number and type of clinical signs were not associated with tracheal aspirate culture positivity or purulence on Gram stain, but they were associated with a clinical diagnosis of VAI. These findings suggest that positive tracheal aspirate cultures may not aid clinicians in the diagnosis of VAI, and they highlight the opportunity for improved diagnostic stewardship.
Funding: No
Disclosures: None
Figure 1.
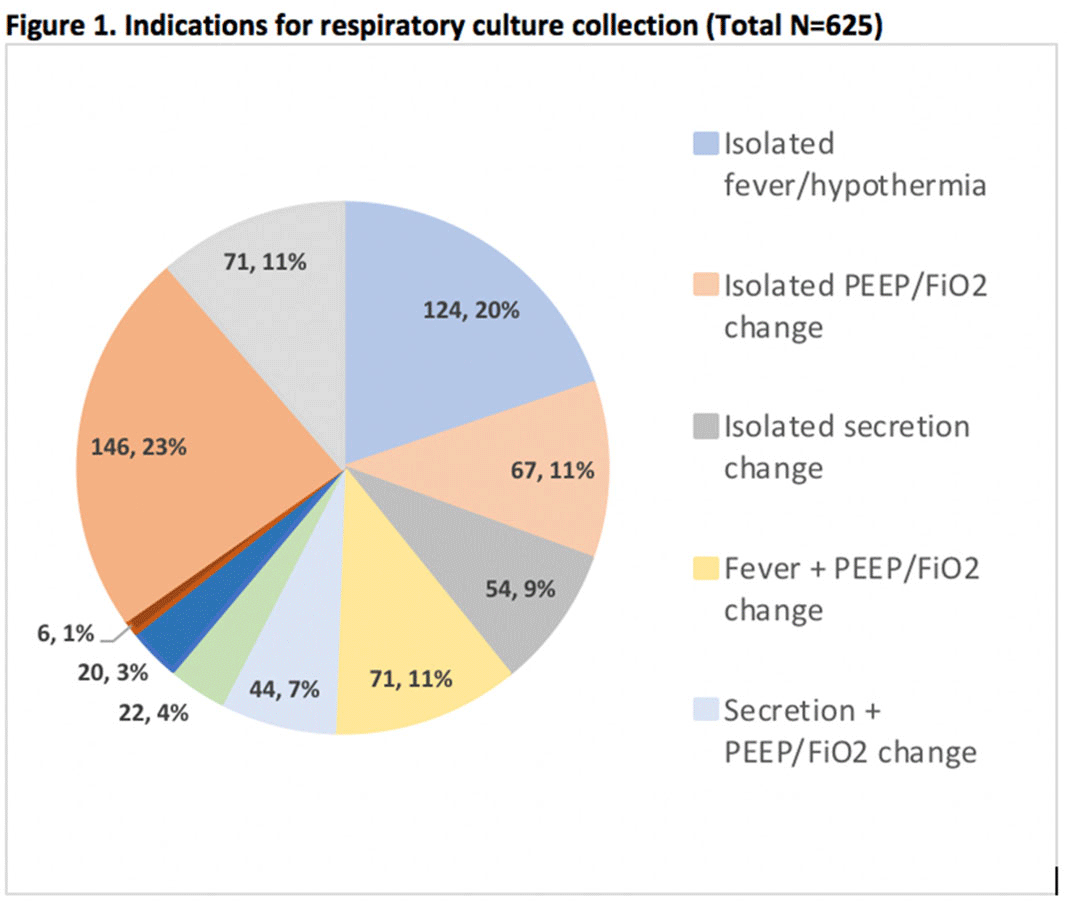
Figure 2.


COVID-19’s Impact on Farmers Market Sales in the Washington, D.C., Area
-
- Journal:
- Journal of Agricultural and Applied Economics / Volume 53 / Issue 1 / February 2021
- Published online by Cambridge University Press:
- 13 January 2021, pp. 94-109
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The Efficacy of Novel Commercial Tourniquet Designs for Extremity Hemorrhage Control: Implications for Spontaneous Responder Every Day Carry
-
- Journal:
- Prehospital and Disaster Medicine / Volume 35 / Issue 3 / June 2020
- Published online by Cambridge University Press:
- 13 April 2020, pp. 276-280
- Print publication:
- June 2020
-
- Article
- Export citation
Efficacy of Novel Commercial Tourniquet Systems in Extremity Hemorrhage Control - An Ultrasound and Generated Force Study
-
- Journal:
- Prehospital and Disaster Medicine / Volume 34 / Issue s1 / May 2019
- Published online by Cambridge University Press:
- 06 May 2019, p. s90
- Print publication:
- May 2019
-
- Article
-
- You have access
- Export citation
An Environmental Scan of Academic Emergency Medicine at the 17 Canadian Medical Schools: Why Does this Matter to Emergency Physicians?
-
- Journal:
- Canadian Journal of Emergency Medicine / Volume 19 / Issue 1 / January 2017
- Published online by Cambridge University Press:
- 21 July 2016, pp. 39-46
- Print publication:
- January 2017
-
- Article
-
- You have access
- HTML
- Export citation
3 - Astrospheres, stellar winds, and the interstellar medium
-
-
- Book:
- Heliophysics: Active Stars, their Astrospheres, and Impacts on Planetary Environments
- Published online:
- 05 March 2016
- Print publication:
- 17 March 2016, pp 56-79
-
- Chapter
- Export citation
CAEP 2014 Academic Symposium: “How to make research succeed in your department: Promoting excellence in Canadian emergency medicine resident research”
-
- Journal:
- Canadian Journal of Emergency Medicine / Volume 17 / Issue 5 / September 2015
- Published online by Cambridge University Press:
- 24 August 2015, pp. 591-599
- Print publication:
- September 2015
-
- Article
-
- You have access
- HTML
- Export citation
Contributors
-
-
- Book:
- The Cambridge Dictionary of Philosophy
- Published online:
- 05 August 2015
- Print publication:
- 27 April 2015, pp ix-xxx
-
- Chapter
- Export citation
Non-targeted lipidomics of CSF and frontal cortex grey and white matter in control, mild cognitive impairment, and Alzheimer’s disease subjects
-
- Journal:
- Acta Neuropsychiatrica / Volume 27 / Issue 5 / October 2015
- Published online by Cambridge University Press:
- 10 April 2015, pp. 270-278
-
- Article
- Export citation
