
173 results
A causal roadmap for generating high-quality real-world evidence
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 22 September 2023, e212
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A new era for the negative symptoms of schizophrenia
-
- Journal:
- The British Journal of Psychiatry / Volume 223 / Issue 1 / July 2023
- Published online by Cambridge University Press:
- 10 July 2023, pp. 269-270
- Print publication:
- July 2023
-
- Article
-
- You have access
- HTML
- Export citation
Socioeconomic differences in antibiotic use for common infections in pediatric urgent-care centers—A quasi-experimental study
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 29 June 2023, pp. 2009-2016
- Print publication:
- December 2023
-
- Article
-
- You have access
- HTML
- Export citation
Appropriateness of antibiotic prescribing varies by clinical services at United States children’s hospitals
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 11 / November 2023
- Published online by Cambridge University Press:
- 12 April 2023, pp. 1711-1717
- Print publication:
- November 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
In defense of the personal/impersonal distinction in moral psychology research: Cross-cultural validation of the dual process model of moral judgment
-
- Journal:
- Judgment and Decision Making / Volume 6 / Issue 3 / April 2011
- Published online by Cambridge University Press:
- 01 January 2023, pp. 186-195
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Tricuspid atresia and common arterial trunk: a rare form of CHD
-
- Journal:
- Cardiology in the Young / Volume 33 / Issue 7 / July 2023
- Published online by Cambridge University Press:
- 06 December 2022, pp. 1192-1195
-
- Article
- Export citation
Characteristics of antifungal utilization for hospitalized children in the United States
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 02 December 2022, e190
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Novel expansion of a well-established antimicrobial stewardship program: Enhancing program efficiency and reach
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 30 August 2022, pp. 869-874
- Print publication:
- June 2023
-
- Article
- Export citation
Large-Format Direct Detection Camera for Cryo-EM at 100 keV
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 1172-1173
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Variation in ampicillin dosing for lower respiratory tract infections and neonatal bacterial infections in US children’s hospitals
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 23 May 2022, e85
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The utility of a structured, interactive cardiac anatomy teaching session for resident education
-
- Journal:
- Cardiology in the Young / Volume 33 / Issue 2 / February 2023
- Published online by Cambridge University Press:
- 22 April 2022, pp. 208-212
-
- Article
- Export citation
Reptamsassia n. gen. (Amsassiaceae n. fam.; calcareous algae) from the Lower Ordovician (Floian) of western Newfoundland, and the earliest symbiotic intergrowth of modular species
-
- Journal:
- Journal of Paleontology / Volume 96 / Issue 3 / May 2022
- Published online by Cambridge University Press:
- 28 January 2022, pp. 715-728
-
- Article
- Export citation
Hippocampal volume and volume asymmetry prospectively predict PTSD symptom emergence among Iraq-deployed soldiers
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 5 / April 2023
- Published online by Cambridge University Press:
- 22 November 2021, pp. 1906-1913
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Outpatient antimicrobial stewardship programs in pediatric institutions in 2020: Status, needs, barriers
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 10 / October 2022
- Published online by Cambridge University Press:
- 22 October 2021, pp. 1396-1402
- Print publication:
- October 2022
-
- Article
- Export citation
Amsassia (calcareous alga) from the Lower Ordovician (Tremadocian) of western Newfoundland, and the biologic affinity and geologic history of the genus
-
- Journal:
- Journal of Paleontology / Volume 96 / Issue 1 / January 2022
- Published online by Cambridge University Press:
- 21 September 2021, pp. 1-18
-
- Article
- Export citation
Alpha-blockade during congenital heart surgery admissions: analysis from national database
- Part of
-
- Journal:
- Cardiology in the Young / Volume 32 / Issue 7 / July 2022
- Published online by Cambridge University Press:
- 17 September 2021, pp. 1136-1142
-
- Article
- Export citation
Revealing the Relation between Star Formation Activity of Jellyfish Galaxies and Ram Pressure Stripping
-
- Journal:
- Proceedings of the International Astronomical Union / Volume 17 / Issue S373 / August 2021
- Published online by Cambridge University Press:
- 09 June 2023, pp. 132-135
- Print publication:
- August 2021
-
- Article
- Export citation
Promoting Antimicrobial Stewardship Education Among Pediatricians Through a Maintenance of Certification Part 4 Quality Impro
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s29
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: The rise of antimicrobial resistance has made it critical for clinicians to understand antimicrobial stewardship principles. We sought to determine whether the opportunity to participate in an American Board of Pediatrics Maintenance of Certification Part 4 (MOC4) quality improvement (QI) project would engage pediatricians and improve their knowledge about antimicrobial stewardship. Methods: In August 2019, a new clinical algorithm for acute appendicitis, spearheaded by the antimicrobial stewardship program (ASP), was implemented at UCSF Benioff Children’s Hospital Oakland to standardize care and optimize antimicrobial use. Medical staff were invited to participate in a QI project evaluating the impact of this algorithm. Data were collected for the 2 quarters preceding implementation (baseline), for the quarter of implementation (transition period), and for the quarter after implementation. Participants were offered MOC4 credit for reviewing these 3 cycles of data and associated materials highlighting information about antimicrobial stewardship. An initial survey was given to participants to assess their baseline knowledge via 4 questions about antimicrobial use in surgical patients (Table 1). At the conclusion of the QI project, another survey was conducted to reassess participant knowledge and to evaluate overall satisfaction with the project. Results: In total, 150 clinicians completed the initial survey. Of these, 44% were general pediatricians and 56% were pediatric subspecialists. Based on years out of training, their levels of experience varied: >20 years in 24%, 11–20 years in 32.7%, 0–10 years in 34.7%, and currently in training in 8.7%. Of the 150 initial participants, 133 (89%) completed the QI project and the second survey. Between surveys, there was significant improvement in knowledge about the appropriate timing and duration of surgical antibiotic prophylaxis (Table 1). Moreover, 88% of participants responded that the QI project was extremely effective in helping them learn about antimicrobial stewardship principles and about ASP interventions. Conclusions: Participation in this MOC4 QI project resulted in significant improvement in knowledge about antimicrobial use in surgical patients, and the activity was perceived as a highly effective way to learn about antimicrobial stewardship. QI projects that leverage MOC4 credit can be a powerful tool for engaging pediatricians and disseminating education about antimicrobial stewardship.
Funding: No
Disclosures: None
Table 1. 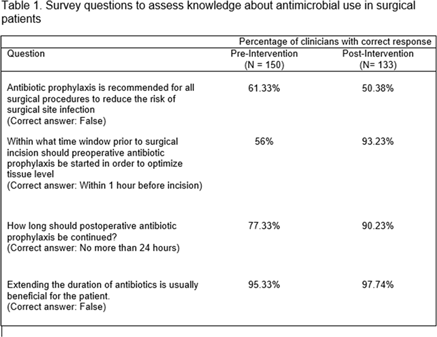

Quality Indicators for Older Persons’ Transitions in Care: A Systematic Review and Delphi Process
-
- Journal:
- Canadian Journal on Aging / La Revue canadienne du vieillissement / Volume 41 / Issue 1 / March 2022
- Published online by Cambridge University Press:
- 03 June 2021, pp. 40-54
-
- Article
-
- You have access
- HTML
- Export citation
39901 Breaking down silos to synergize clinical trial development and initiation: The Clinical Research Support Center, University of Minnesota
-
- Journal:
- Journal of Clinical and Translational Science / Volume 5 / Issue s1 / March 2021
- Published online by Cambridge University Press:
- 30 March 2021, pp. 108-109
-
- Article
-
- You have access
- Open access
- Export citation
