
136 results
Importance, motivation and confidence of eating healthily whilst at university and barriers UK students face to eating well at university
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE5 / 2023
- Published online by Cambridge University Press:
- 08 January 2024, E347
-
- Article
-
- You have access
- HTML
- Export citation
Extensive dickitization of the permo-triassic fluvial sandstones from the eastern Iberian Range, Spain
-
- Journal:
- Clays and Clay Minerals / Volume 55 / Issue 5 / October 2007
- Published online by Cambridge University Press:
- 01 January 2024, pp. 481-490
-
- Article
- Export citation
Guide to assembling a successful K99/R00 application
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 29 September 2023, e215
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Dementia as a presentation of motor neurone disease: a case report
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S753
-
- Article
-
- You have access
- Open access
- Export citation
Cyclothymia, bipolar disorder and multiple sclerosis: A case report
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S703-S704
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
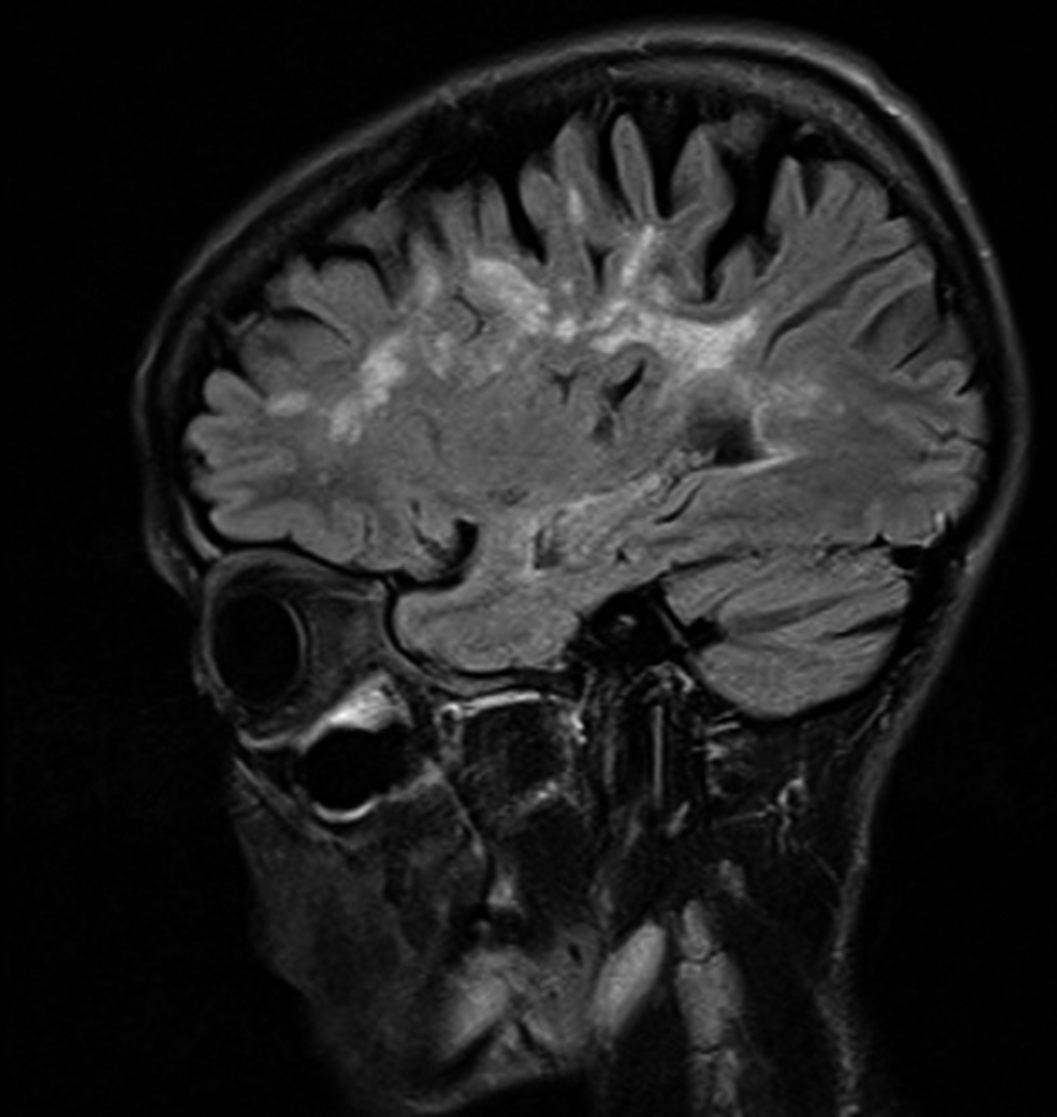
We present the case of a 49-year-old woman who was diagnosed with multiple sclerosis at the age of 19 and suffers from an affective disorder that has been evolving for years. This condition, for which she has been followed by psychiatry and psychology for more than ten years, consists of alternating periods of hypomania lasting weeks and phases in which frank depressive symptomatology predominates, with no phases of euthymia in between and with a predominance of severe deterioration of her functionality at both poles.
Objectives(1) We will review the term cyclothymia and explore the concept of “cyclothymic temperament” advocated by some authors, in order to be able to understand the dimension of the present case and reformulate its approach.
(2) The relationship between multiple sclerosis and bipolar spectrum disorders will be covered, reviewing the current knowledge in this regard and relating it to the patient’s symptomatology.
MethodsA review of the patient’s clinical history will be carried out, taking into account her life history, the complementary tests performed as well as the multiple therapeutic approaches tried over the last few years.
Likewise, a bibliographic review of the available scientific literature will be carried out in relation to the diagnosis of cyclothymia or bipolar disorder type II, the controversial term “cyclothymic temperament”, and the relationship that these diagnoses have with the diagnosis of Multiple Sclerosis.
Results(1) Our patient could fit into what many authors define as a cyclothymic temperament, fulfilling, in certain episodes, the criteria that the manuals propose for bipolar disorder type II.
(2) 2.1 The prevalence of bipolar affective disorder in MS is approximately twice as high as in the general population (rates of 0.3-2.4%). 2.2 Patients with MS have higher scores in cyclothymic and hyperthymic temperament than the control group. 2.3 Certain drugs generally used in BD also seem to have a beneficial effect on MS.
Image:
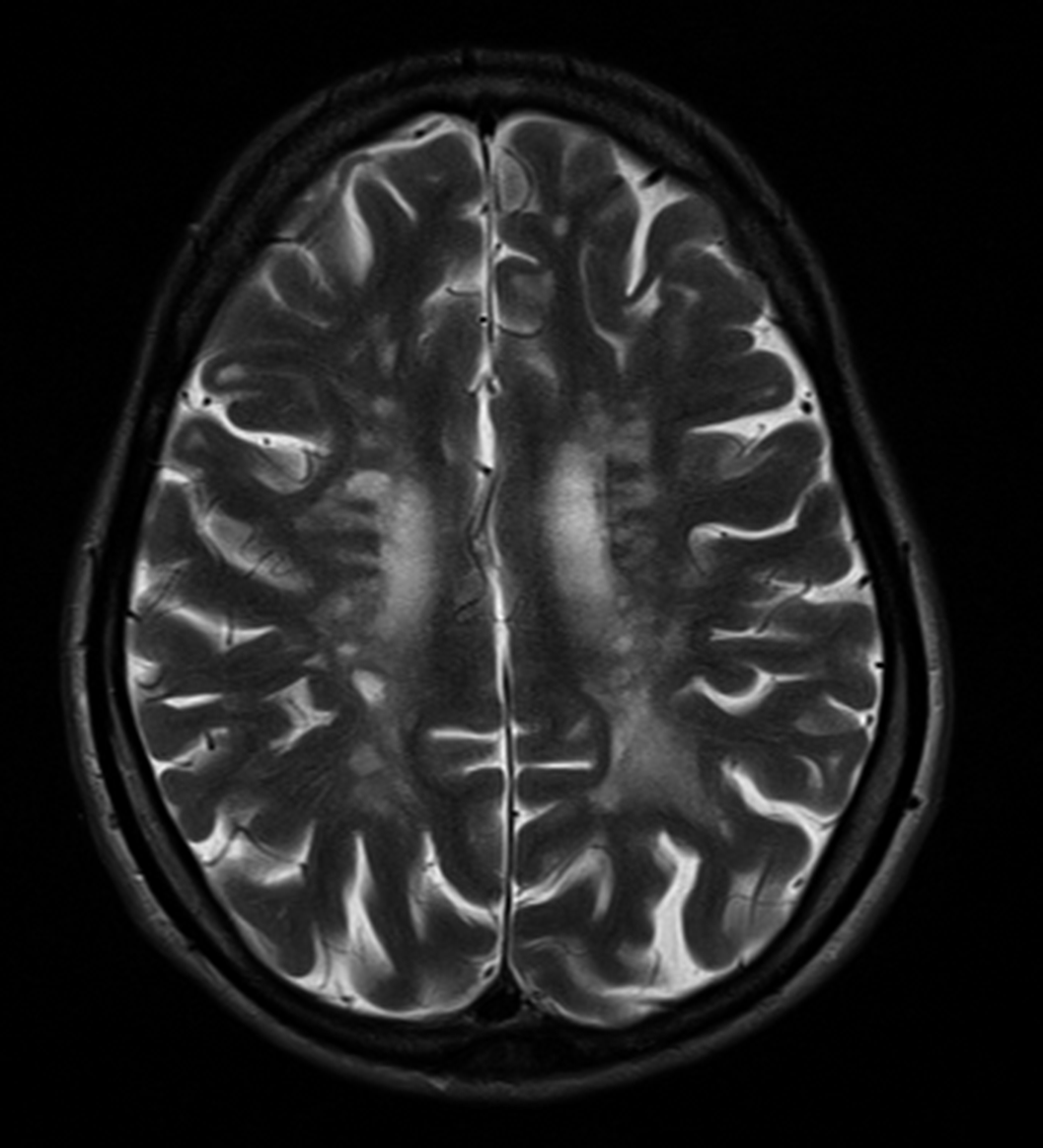
Image 2:
 Conclusions
ConclusionsThe reformulation of the concept of cyclothymia would allow us to recognize in our patient a basic temperament of long evolution that would be the substrate on which different factors have subsequently influenced, such as antidepressant drugs or multiple sclerosis. In addition, it is necessary to know the association between BD and MS, in order to be able to offer an adequate treatment, contemplating some pharmacological options such as Lithium or some Atypical Antipsychotics, given the beneficial effect both for the affective disorder and for the neurological process.
Disclosure of InterestNone Declared


Blue justice: A review of emerging scholarship and resistance movements
-
- Journal:
- Cambridge Prisms: Coastal Futures / Volume 1 / 2023
- Published online by Cambridge University Press:
- 26 January 2023, e15
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Biomarkers of sepsis in pigs, horses and cattle: from acute phase proteins to procalcitonin
-
- Journal:
- Animal Health Research Reviews / Volume 23 / Issue 1 / June 2022
- Published online by Cambridge University Press:
- 07 July 2022, pp. 82-99
-
- Article
- Export citation
Validating a risk assessment tool in United Kingdom and Irish paediatric cardiac catheterisation practice
- Part of
-
- Journal:
- Cardiology in the Young / Volume 32 / Issue 9 / September 2022
- Published online by Cambridge University Press:
- 14 October 2021, pp. 1407-1414
-
- Article
- Export citation
Impacts of social distancing during the covid19 pandemic on the development of children with autism in Brazil
-
- Journal:
- European Psychiatry / Volume 64 / Issue S1 / April 2021
- Published online by Cambridge University Press:
- 13 August 2021, pp. S262-S263
-
- Article
-
- You have access
- Open access
- Export citation
Glucagon-like peptide-1 receptor agonists in patients treated with antipsychotics
-
- Journal:
- European Psychiatry / Volume 64 / Issue S1 / April 2021
- Published online by Cambridge University Press:
- 13 August 2021, p. S775
-
- Article
-
- You have access
- Open access
- Export citation
Creating enriched training sets of eligible studies for large systematic reviews: the utility of PubMed's Best Match algorithm
- Part of
-
- Journal:
- International Journal of Technology Assessment in Health Care / Volume 37 / Issue 1 / 2021
- Published online by Cambridge University Press:
- 18 December 2020, e7
-
- Article
- Export citation
Clinical Factors as Predictors on Functional Impairment in Bipolar Disorder
-
- Journal:
- European Psychiatry / Volume 24 / Issue S1 / January 2009
- Published online by Cambridge University Press:
- 16 April 2020, 24-E603
-
- Article
-
- You have access
- Export citation
P0157 - Why clinicians maintain antidepressants in some patients with acute mania? Hints from a large, observational study (EMBLEM)
-
- Journal:
- European Psychiatry / Volume 23 / Issue S2 / April 2008
- Published online by Cambridge University Press:
- 16 April 2020, p. S238
-
- Article
-
- You have access
- Export citation
Functioning in patients with recently diagnosed vs. chronic schizophrenia treated with paliperidone ER
-
- Journal:
- European Psychiatry / Volume 26 / Issue S2 / March 2011
- Published online by Cambridge University Press:
- 16 April 2020, p. 1285
-
- Article
-
- You have access
- Export citation
Tolerability and treatment response in patients with recently diagnosed vs. chronic schizophrenia treated with paliperidone ER
-
- Journal:
- European Psychiatry / Volume 26 / Issue S2 / March 2011
- Published online by Cambridge University Press:
- 16 April 2020, p. 1503
-
- Article
-
- You have access
- Export citation
P0179 - Prospective, multicenter, open-label, observational study of sexual function in patients beginning aripiprazole treatment
-
- Journal:
- European Psychiatry / Volume 23 / Issue S2 / April 2008
- Published online by Cambridge University Press:
- 16 April 2020, pp. S133-S134
-
- Article
-
- You have access
- Export citation
Tolerability and treatment response in patients with recently diagnosed vs. chronic schizophrenia treated with paliperidone ER
-
- Journal:
- European Psychiatry / Volume 26 / Issue S2 / March 2011
- Published online by Cambridge University Press:
- 16 April 2020, p. 1502
-
- Article
-
- You have access
- Export citation
EPA-1549 - A Randomized, Active-controlled Rater-blinded 2-year Study of Paliperidone Palmitate Versus Investigators’ Choice of Oral Antipsychotic Monotherapy in Patients with Schizophrenia (prosipal)
-
- Journal:
- European Psychiatry / Volume 29 / Issue S1 / 2014
- Published online by Cambridge University Press:
- 15 April 2020, p. 1
-
- Article
-
- You have access
- Export citation
EPA-0330 – Ilex Paraguariensis use and Affective Symptoms: ¿is There an Association?
-
- Journal:
- European Psychiatry / Volume 29 / Issue S1 / 2014
- Published online by Cambridge University Press:
- 15 April 2020, p. 1
-
- Article
-
- You have access
- Export citation
P-201 - Effectiveness of Quetiapine xr Vs. Sertraline in Acute Bipolar Depression as Add-on Therapy to Previous Mood Stabilizer Treatment: a Pilot Study
-
- Journal:
- European Psychiatry / Volume 27 / Issue S1 / 2012
- Published online by Cambridge University Press:
- 15 April 2020, p. 1
-
- Article
-
- You have access
- Export citation
