
336 results
Maternal pea fiber supplementation to a high calorie diet in obese pregnancies protects male offspring from metabolic dysfunction in adulthood
-
- Journal:
- Journal of Developmental Origins of Health and Disease / Volume 14 / Issue 6 / December 2023
- Published online by Cambridge University Press:
- 18 January 2024, pp. 711-718
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Overview of climate disclosures
-
- Journal:
- British Actuarial Journal / Volume 28 / 2023
- Published online by Cambridge University Press:
- 03 January 2024, e13
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
3 Stricker Learning Span criterion validity: remote self-administration of a computer adaptive word list memory test shows similar ability to differentiate PET-defined biomarker groups as in-person Rey Auditory Verbal Learning Test performance in cognitively unimpaired individuals on the Alzheimer’s continuum
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 407-408
-
- Article
-
- You have access
- Export citation
Persistent colonization of Candida auris among inpatients rescreened as part of a weekly surveillance program
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 13 December 2023, pp. 1-4
-
- Article
- Export citation
Beta-lactam comprehensive allergy management program in a community medical center
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 27 October 2023, e189
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Operational impact of decreased turnaround times for Candida auris screening tests in a tertiary academic medical center
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 18 October 2023, e176
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Introduction to A Compendium of Strategies to Prevent Healthcare-Associated Infections In Acute-Care Hospitals: 2022 Updates
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 10 / October 2023
- Published online by Cambridge University Press:
- 19 October 2023, pp. 1533-1539
- Print publication:
- October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Executive Summary: A Compendium of Strategies to Prevent Healthcare-Associated Infections in Acute-Care Hospitals: 2022 Updates
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 10 / October 2023
- Published online by Cambridge University Press:
- 22 August 2023, pp. 1540-1554
- Print publication:
- October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Strategies to prevent catheter-associated urinary tract infections in acute-care hospitals: 2022 Update
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 8 / August 2023
- Published online by Cambridge University Press:
- 25 August 2023, pp. 1209-1231
- Print publication:
- August 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A real-world data analysis of Clinical Global Impression-Severity (CGI-S) as a transdiagnostic predictor of psychiatric hospitalisation
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S619-S620
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Preventing psychiatric admissions holds benefits for patients as well as healthcare systems. The Clinical Global Impression-Severity (CGI-S) scale is a 7-point measurement of symptom severity, independent of diagnosis, which has shown capability of predicting risk of hospitalisation in schizophrenia. Due to its routine use in clinical practice and ease of administration, it may have potential as a transdiagnostic predictor of hospitalisation.
ObjectivesTo investigate whether early trajectories of CGI-S scores predict risk of hospitalisation over a 6 month-follow-up period.
MethodsA retrospective cohort study was conducted, analysing Electronic Health Record (EHR) data from the NeuroBlu Database (Patel et al. BMJ Open 2022;12:e057227). Patients were included if they had a psychiatric diagnosis and at least 5 recorded CGI-S scores within a 2-month period, defined as the ‘index’ period. The relationship between early CGI-S trajectories and risk of hospitalisation was investigated using Cox regression. The analysis was adjusted for age, gender, race, number of years in education, and psychiatric diagnosis. Early CGI-S trajectories were estimated as clinical severity (defined as the mean CGI-S score during the index period) and clinical instability (defined as a generalised Root Mean Squared Subsequent Differences of all CGI-S scores recorded during the index period). The primary outcome was time to psychiatric hospitalisation up to 6 months following the index period. Patients who had been hospitalised before or within the index period were excluded.
ResultsA total of 36,914 patients were included (mean [SD] age: 29.7 [17.5] years; 57.3% female). Clinical instability (hazard ratio: 1.09, 95% CI 1.07-1.10, p<0.001) and severity (hazard ratio: 1.11, 95% CI 1.09-1.12, p<0.001) independently predicted risk of hospitalisation. These associations were consistent across all psychiatric diagnoses. Patients in the top 50% of severity and/or instability were at a 45% increased risk of hospitalisation compared to those in the bottom 50% (Figure 1).
Image:
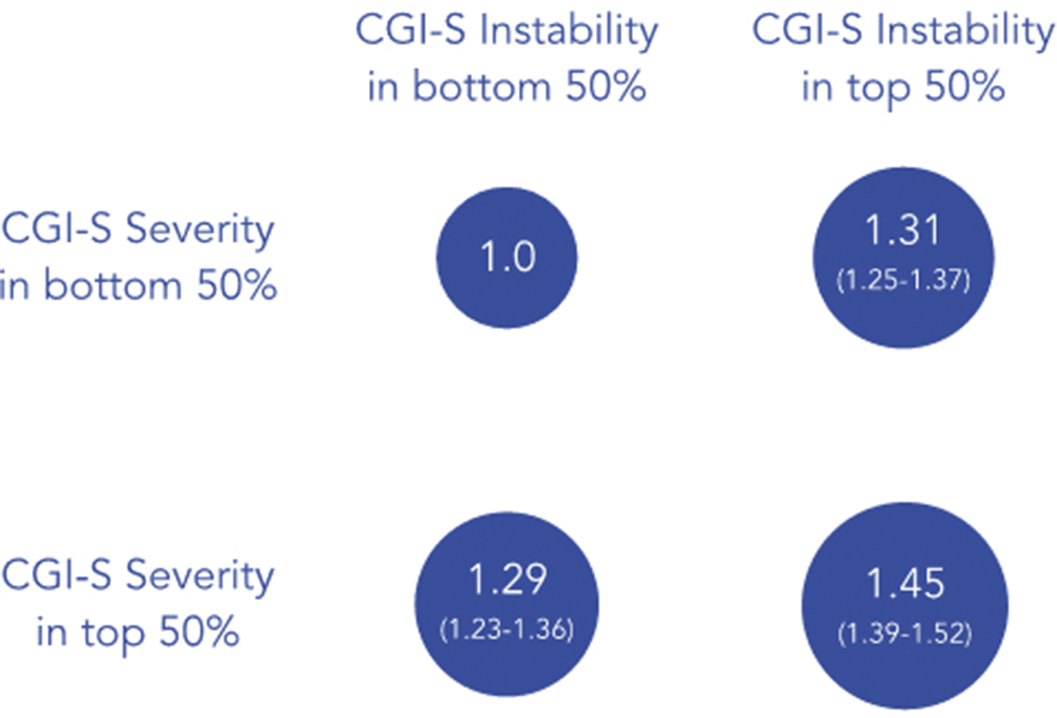 Conclusions
ConclusionsEarly CGI-S trajectories reflecting clinical severity and instability independently predict risk of hospitalisation across diagnoses. This risk was compounded when instability and severity were present together. These results have translation potential in predicting individuals who are at high risk of hospitalisation and could benefit from preventative strategies to mitigate this risk.
Disclosure of InterestE. Palmer Employee of: Holmusk, M. Taquet Consultant of: Holmusk, K. Griffiths Employee of: Holmusk, S. Ker Employee of: Holmusk, C. Liman Employee of: Holmusk, S. N. Wee Employee of: Holmusk, S. Kollins Employee of: Holmusk, R. Patel Grant / Research support from: National Institute of Health Research (NIHR301690); Medical Research Council (MR/S003118/1); Academy of Medical Sciences (SGL015/1020); Janssen, Employee of: Holmusk

Stricker Learning Span criterion validity: a remote self-administered multi-device compatible digital word list memory measure shows similar ability to differentiate amyloid and tau PET-defined biomarker groups as in-person Auditory Verbal Learning Test
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 30 / Issue 2 / February 2024
- Published online by Cambridge University Press:
- 30 June 2023, pp. 138-151
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Penicillin allergy evaluation in hospitalized patients with hematologic malignancy
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 16 May 2023, e92
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Interpreting politically-charged numerical information: The influence of numeracy and problem difficulty on response accuracy
-
- Journal:
- Judgment and Decision Making / Volume 15 / Issue 2 / March 2020
- Published online by Cambridge University Press:
- 01 January 2023, pp. 203-213
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The $5 Billion Hop: Glatiramer Acetate and the US Patent System
-
- Journal:
- Journal of Law, Medicine & Ethics / Volume 50 / Issue 4 / Winter 2022
- Published online by Cambridge University Press:
- 08 March 2023, pp. 852-856
- Print publication:
- Winter 2022
-
- Article
- Export citation
Comparison of treatment modalities for single-sided deafness in paediatric patients
-
- Journal:
- The Journal of Laryngology & Otology / Volume 137 / Issue 7 / July 2023
- Published online by Cambridge University Press:
- 16 November 2022, pp. 725-731
- Print publication:
- July 2023
-
- Article
- Export citation
Management of routine postoperative pain for children undergoing cardiac surgery: a Paediatric Acute Care Cardiology Collaborative Clinical Practice Guideline
-
- Journal:
- Cardiology in the Young / Volume 32 / Issue 12 / December 2022
- Published online by Cambridge University Press:
- 16 November 2022, pp. 1881-1893
-
- Article
- Export citation
Inpatient antibiotic prescribing patterns using the World Health Organization (WHO) Access Watch and Reserve (AWaRe) classification in Okinawa, Japan: A point-prevalence survey
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 14 September 2022, e155
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Factors Affecting School Performance in the Adolescents of USA- Youth Risk Behavior Surveillance System
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S226
-
- Article
-
- You have access
- Open access
- Export citation
Electronic smart-hub based intervention during COVID-19 in a rural Psychiatry of Old Age service in North-West Ireland
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S654
-
- Article
-
- You have access
- Open access
- Export citation
NeuroBlu: a natural language processing (NLP) electronic health record (EHR) data analytic tool to generate real-world evidence in mental healthcare
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, pp. S99-S100
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
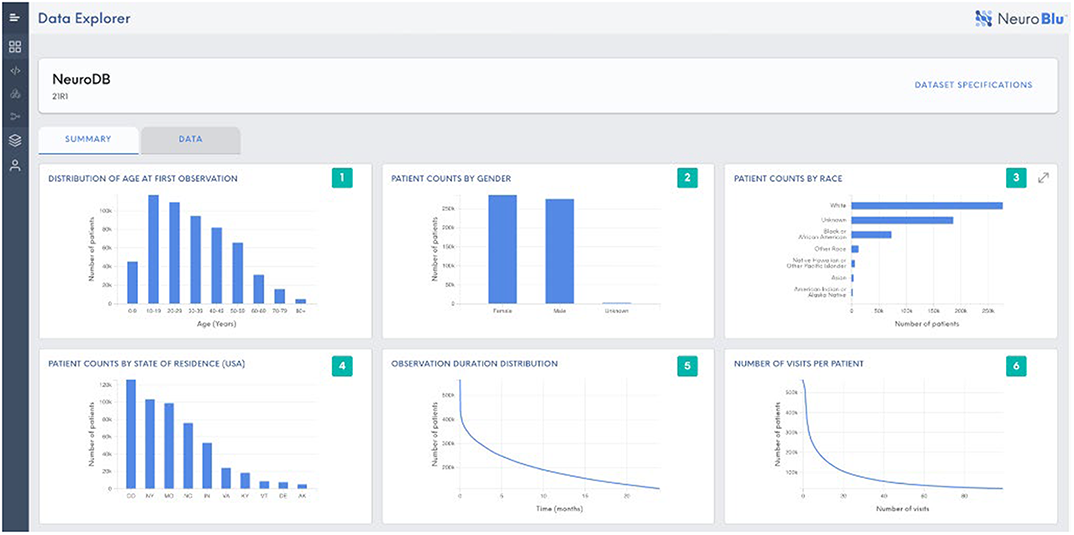
EHRs contain a rich source of real-world data that can support evidence generation to better understand mental disorders and improve treatment outcomes. However, EHR datasets are complex and include unstructured free text data that are time consuming to manually review and analyse. We present NeuroBlu, a secure, cloud-based analytic tool that includes bespoke NLP software to enable users to analyse large volumes of EHR data to generate real-world evidence in mental healthcare.
 Objectives
Objectives(i) To assemble a large mental health EHR dataset in a secure, cloud-based environment.
(ii) To apply NLP software to extract data on clinical features as part of the Mental State Examination (MSE).
(iii) To analyse the distribution of NLP-derived MSE features by psychiatric diagnosis.
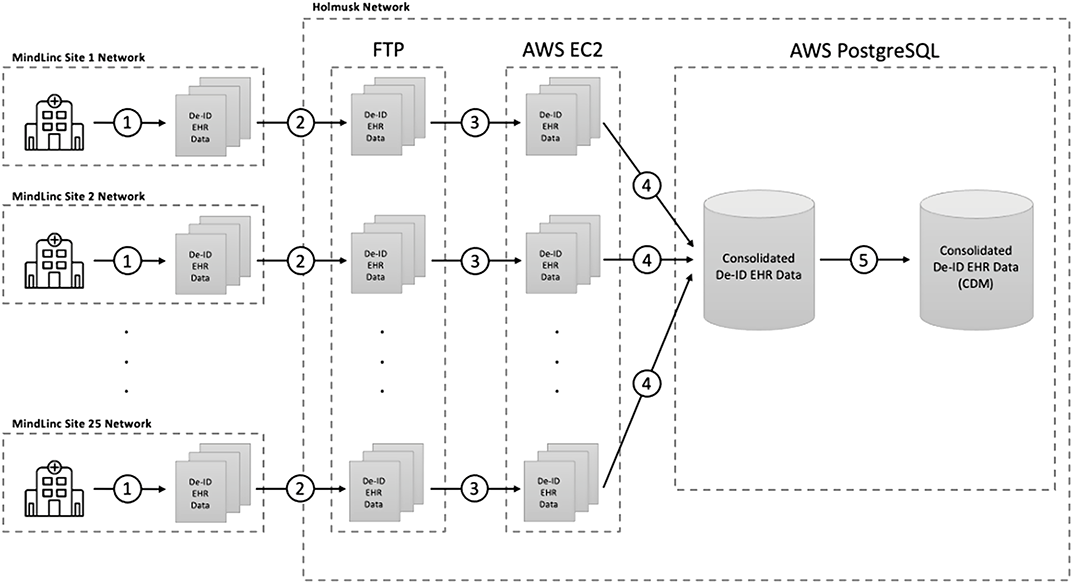
MethodsEHR data from 25 U.S. mental healthcare providers were de-identified and transformed into a common data model. NLP models were developed to extract 241 MSE features using a deep learning, long short-term memory (LSTM) approach. The NeuroBlu tool (https://www.neuroblu.ai/) was used to analyse the associations of MSE features in 543,849 patients.
 Results
ResultsThe figure below illustrates the percentage of patients in each diagnostic category with at least one recorded MSE feature.
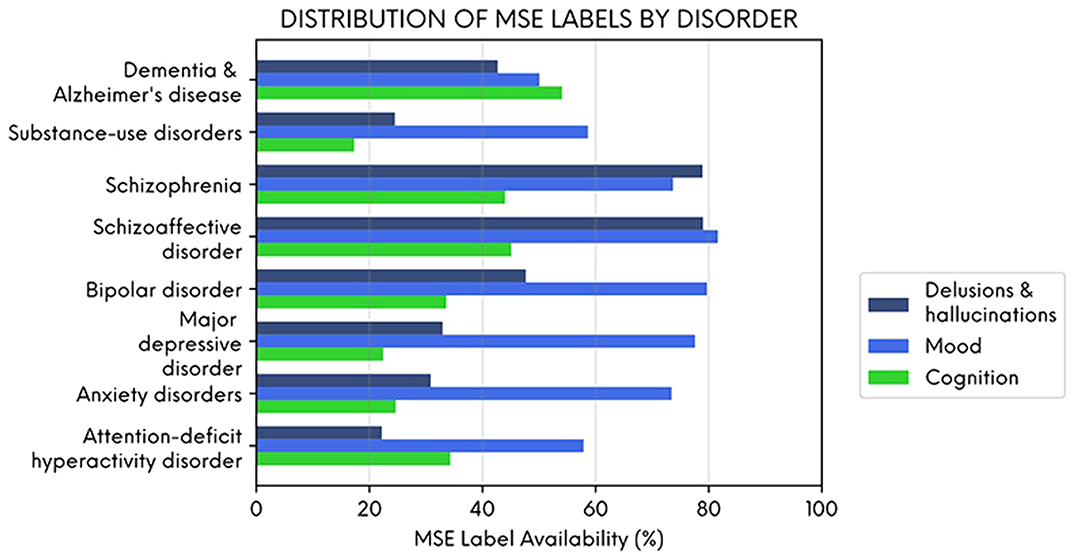 Conclusions
ConclusionsDelusions and hallucinations were more likely to be recorded in people with schizophrenia and schizoaffective disorder, and cognitive features were more likely to be recorded in people with dementia. However, mood symptoms were frequently recorded across all diagnoses illustrating their importance as a transdiagnostic clinical feature. NLP-derived clinical information could enhance the potential of EHR data to generate real-world evidence in mental healthcare.
DisclosureThis study was funded in full by Holmusk.



