
22 results
Factors influencing healthcare personnel decision making to work with respiratory symptoms during the COVID-19 pandemic
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s57-s58
-
- Article
-
- You have access
- Open access
- Export citation
-
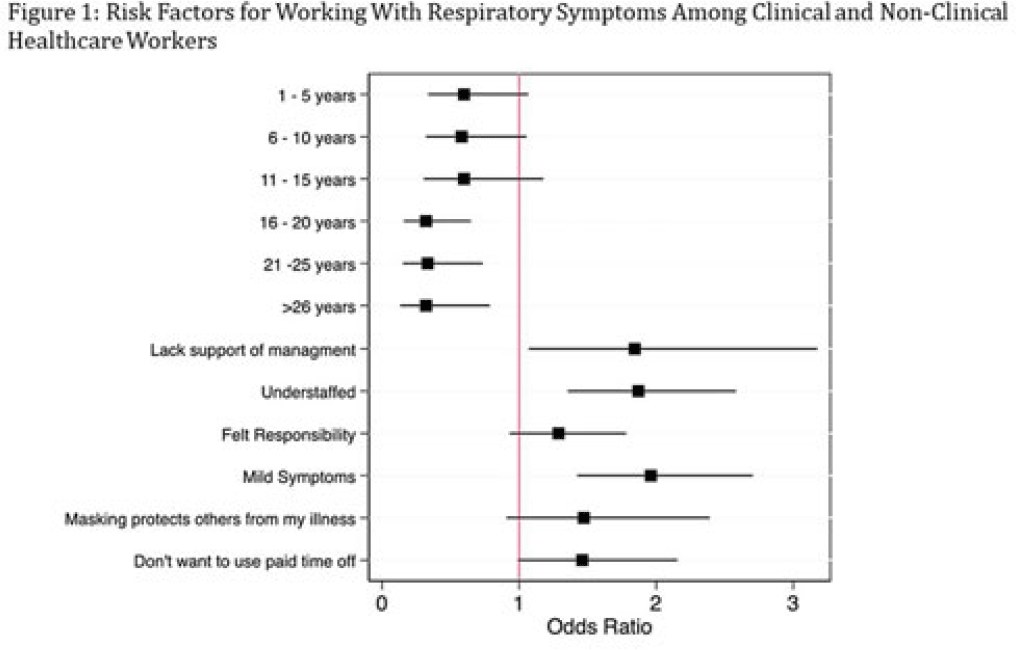
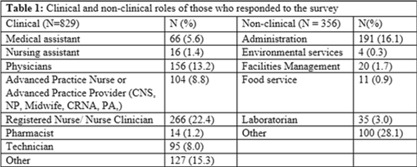
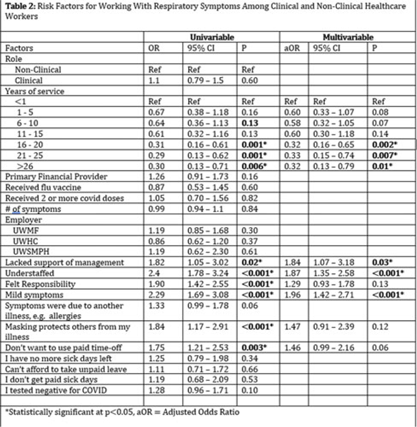
Background: Amid the COVID-19 pandemic, healthcare systems were stretched thin, with staffing shortages posing substantial challenges. Limiting spread of COVID-19 among healthcare professionals (HCP) is paramount to preventing exacerbation of such shortages, but strategies are highly dependent on HCP self-screening for symptoms and isolating when present. We examined HCP perceptions of barriers and factors that facilitate staying home when experiencing respiratory symptoms. Methods: At an academic tertiary-care referral center, in inpatient and ambulatory settings, we conducted an anonymous electronic survey between March 11, 2022, and April 12, 2022. Using logistic regression analysis, we analyzed predictors of employees reporting to work with respiratory symptoms using STATA and SAS software. Results: In total, 1,185 individuals including 829 clinical staff and 356 nonclinical staff responded to the survey. When excluding participants who reported working “remotely” (N = 381) and those who reported being unsure of whether they had worked with symptoms (N = 14), the prevalence of working with respiratory symptoms was 63%. There was no significant difference between clinical and nonclinical staff (OR, 1.1; 95% CI, 0.8–1.5; P = .60). Increasing number of years of service was protective against working with symptoms, achieving statistically significance in multivariable analysis after 16 years. Compared to those having worked <1 year, the odds ratios of working with symptoms were 0.32 (95% CI, 0.16–0.65; P = .002), 0.33 (95% CI, 0.15–0.74; P = .007), and 0.32 (95% CI, 0.13–0.79; P = .007) for those working 16–20 years, 21–25 years, and ≥26 years, respectively. More than half of HCP who worked with symptoms identified being understaffed (56.9%), having mild symptoms (55.3%), and sense of responsibility (55.1%) as reasons to work with respiratory symptoms. The following barriers, or reasons to work with symptoms, were more commonly identified as significant by those who worked with symptoms compared to those who did not: being understaffed (OR, 1.87; 95% CI, 1.35–2.58; P ≤ .001), having mild symptoms (OR, 1.96; 95% CI, 1.42–2.71; P < .001), and lack of support from management (OR, 1.84; 95% CI, 1.07–3.18; P = .03). Conclusions: Working with respiratory symptoms is prevalent in clinical and nonclinical HCP. Those with fewer years of work experience appear to be more susceptible to misconceptions and pressures to work despite respiratory symptoms. Messaging should stress support from leadership and the significance of even mild respiratory symptoms and should emphasize responsibility to patients and colleagues to stay home with respiratory symptoms. Strategies to ensure adequate staffing and sick leave may also be high yield.
Disclosures: None



Patterns, predictors, and patient-reported reasons for antidepressant discontinuation in the WHO World Mental Health Surveys
-
- Journal:
- Psychological Medicine / Volume 54 / Issue 1 / January 2024
- Published online by Cambridge University Press:
- 14 September 2023, pp. 67-78
-
- Article
- Export citation
Evaluation of an experiential training program in patient-centered outcomes and comparative effectiveness research for diverse researcher communities and health care organizations
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 15 March 2023, e81
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Antidepressant use and risk of adverse outcomes: population-based cohort study
-
- Journal:
- BJPsych Open / Volume 8 / Issue 5 / September 2022
- Published online by Cambridge University Press:
- 13 September 2022, e164
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Antidepressant use in low- middle- and high-income countries: a World Mental Health Surveys report
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 4 / March 2023
- Published online by Cambridge University Press:
- 23 September 2021, pp. 1583-1591
-
- Article
- Export citation
Dissecting the heterogeneity of posttraumatic stress disorder: differences in polygenic risk, stress exposures, and course of PTSD subtypes
-
- Journal:
- Psychological Medicine / Volume 52 / Issue 15 / November 2022
- Published online by Cambridge University Press:
- 05 May 2021, pp. 3646-3654
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Toward measuring effective treatment coverage: critical bottlenecks in quality- and user-adjusted coverage for major depressive disorder
-
- Journal:
- Psychological Medicine / Volume 52 / Issue 10 / July 2022
- Published online by Cambridge University Press:
- 20 October 2020, pp. 1948-1958
-
- Article
- Export citation
Like a Bat Out of…. the Hospital? Development of a Bat Capture and Testing Protocol Prompted by Two Nosocomial Encounters
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, p. s314
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
1 - Neuroimaging in Personality Disorders
- from Part I - Etiology
-
-
- Book:
- The Cambridge Handbook of Personality Disorders
- Published online:
- 24 February 2020
- Print publication:
- 07 May 2020, pp 3-19
-
- Chapter
- Export citation
1c - Illustrating the Value of Neuroimaging Studies Using the Example of Affect Regulation: Author Rejoinder to Commentaries on Neuroimaging in Personality Disorders
- from Part I - Etiology
-
-
- Book:
- The Cambridge Handbook of Personality Disorders
- Published online:
- 24 February 2020
- Print publication:
- 07 May 2020, pp 27-28
-
- Chapter
- Export citation
Patterns of care and dropout rates from outpatient mental healthcare in low-, middle- and high-income countries from the World Health Organization's World Mental Health Survey Initiative
-
- Journal:
- Psychological Medicine / Volume 51 / Issue 12 / September 2021
- Published online by Cambridge University Press:
- 28 April 2020, pp. 2104-2116
-
- Article
- Export citation
A low-fidelity, high-functionality, inexpensive ultrasound-guided nerve block model
-
- Journal:
- Canadian Journal of Emergency Medicine / Volume 19 / Issue 1 / January 2017
- Published online by Cambridge University Press:
- 01 August 2016, pp. 58-60
- Print publication:
- January 2017
-
- Article
-
- You have access
- HTML
- Export citation
Divorcing the puzzles: When group identities foster in-group cooperation
-
- Journal:
- Behavioral and Brain Sciences / Volume 39 / 2016
- Published online by Cambridge University Press:
- 07 March 2016, e23
-
- Article
- Export citation
The US National Comorbidity Survey: overview and future directions
-
- Journal:
- Epidemiologia e Psichiatria Sociale / Volume 6 / Issue 1 / April 1997
- Published online by Cambridge University Press:
- 11 October 2011, pp. 4-16
-
- Article
-
- You have access
- Export citation
Contributors
-
-
- Book:
- The Cambridge Dictionary of Christianity
- Published online:
- 05 August 2012
- Print publication:
- 20 September 2010, pp xi-xliv
-
- Chapter
- Export citation
Who Supports Health Reform?
-
- Journal:
- PS: Political Science & Politics / Volume 43 / Issue 1 / January 2010
- Published online by Cambridge University Press:
- 15 January 2010, pp. 1-6
- Print publication:
- January 2010
-
- Article
- Export citation
Contributors
-
-
- Book:
- A Handbook for the Study of Mental Health
- Published online:
- 05 June 2012
- Print publication:
- 16 November 2009, pp xi-xiv
-
- Chapter
- Export citation
Surface Coatings Based on Polysilsesquioxanes: Grafting-from Approach Starting from Organic Polymers
-
- Journal:
- MRS Online Proceedings Library Archive / Volume 1190 / 2009
- Published online by Cambridge University Press:
- 31 January 2011, 1190-NN10-02
- Print publication:
- 2009
-
- Article
- Export citation
5 - The Effects of the U.S. Malpractice System on the Cost and Quality of Care
-
-
- Book:
- Medical Malpractice and the U.S. Health Care System
- Published online:
- 10 December 2009
- Print publication:
- 12 June 2006, pp 84-92
-
- Chapter
- Export citation
A posteriori error control for the Allen–Cahn problem: circumventing Gronwall's inequality
-
- Journal:
- ESAIM: Mathematical Modelling and Numerical Analysis / Volume 38 / Issue 1 / January 2004
- Published online by Cambridge University Press:
- 15 February 2004, pp. 129-142
- Print publication:
- January 2004
-
- Article
- Export citation
