While unobscured and radio-quiet active galactic nuclei are regularly being found at redshifts
 $z > 6$
, their obscured and radio-loud counterparts remain elusive. We build upon our successful pilot study, presenting a new sample of low-frequency-selected candidate high-redshift radio galaxies (HzRGs) over a sky area 20 times larger. We have refined our selection technique, in which we select sources with curved radio spectra between 72–231 MHz from the GaLactic and Extragalactic All-sky Murchison Widefield Array (GLEAM) survey. In combination with the requirements that our GLEAM-selected HzRG candidates have compact radio morphologies and be undetected in near-infrared
$z > 6$
, their obscured and radio-loud counterparts remain elusive. We build upon our successful pilot study, presenting a new sample of low-frequency-selected candidate high-redshift radio galaxies (HzRGs) over a sky area 20 times larger. We have refined our selection technique, in which we select sources with curved radio spectra between 72–231 MHz from the GaLactic and Extragalactic All-sky Murchison Widefield Array (GLEAM) survey. In combination with the requirements that our GLEAM-selected HzRG candidates have compact radio morphologies and be undetected in near-infrared
 $K_{\rm s}$
-band imaging from the Visible and Infrared Survey Telescope for Astronomy Kilo-degree Infrared Galaxy (VIKING) survey, we find 51 new candidate HzRGs over a sky area of approximately
$K_{\rm s}$
-band imaging from the Visible and Infrared Survey Telescope for Astronomy Kilo-degree Infrared Galaxy (VIKING) survey, we find 51 new candidate HzRGs over a sky area of approximately
 $1200\ \mathrm{deg}^2$
. Our sample also includes two sources from the pilot study: the second-most distant radio galaxy currently known, at
$1200\ \mathrm{deg}^2$
. Our sample also includes two sources from the pilot study: the second-most distant radio galaxy currently known, at
 $z=5.55$
, with another source potentially at
$z=5.55$
, with another source potentially at
 $z \sim 8$
. We present our refined selection technique and analyse the properties of the sample. We model the broadband radio spectra between 74 MHz and 9 GHz by supplementing the GLEAM data with both publicly available data and new observations from the Australia Telescope Compact Array at 5.5 and 9 GHz. In addition, deep
$z \sim 8$
. We present our refined selection technique and analyse the properties of the sample. We model the broadband radio spectra between 74 MHz and 9 GHz by supplementing the GLEAM data with both publicly available data and new observations from the Australia Telescope Compact Array at 5.5 and 9 GHz. In addition, deep
 $K_{\rm s}$
-band imaging from the High-Acuity Widefield K-band Imager (HAWK-I) on the Very Large Telescope and from the Southern Herschel Astrophysical Terahertz Large Area Survey Regions
$K_{\rm s}$
-band imaging from the High-Acuity Widefield K-band Imager (HAWK-I) on the Very Large Telescope and from the Southern Herschel Astrophysical Terahertz Large Area Survey Regions
 $K_{\rm s}$
-band Survey (SHARKS) is presented for five sources. We discuss the prospects of finding very distant radio galaxies in our sample, potentially within the epoch of reionisation at
$K_{\rm s}$
-band Survey (SHARKS) is presented for five sources. We discuss the prospects of finding very distant radio galaxies in our sample, potentially within the epoch of reionisation at
 $z \gtrsim 6.5$
.
$z \gtrsim 6.5$
.
Attention-deficit/hyperactivity disorder (ADHD) is a psychiatric condition in which children suffer from inattentiveness, hyperactivity, and or impulsivity. ADHD patients frequently present comorbid psychiatric disorders: in adults, the most common are depression, substance-related disorders, anxiety, and eating disorders. Children and adolescents present conduct disorders, learning disorders, anxiety and depression. Since ADHD and its psychiatric comorbidities share similarities, a partial overlap of their pathophysiological mechanisms has been suggested. ADHD, can be treated with lisdexamfetamine (LDX), a prodrug indicated by the FDA as treatment for binge eating disorder (BED) and ADHD.
To evaluate, through a systems biology-based in silico method, the efficacy of LDX as first-line ADHD treatment to improve ADHD psychiatric comorbidities. Furthermore, we explored the molecular mechanisms behind LDX’s action.
We used the systems biology- and artificial intelligence-based Therapeutic Performance Mapping System (TPMS) technology to characterise and model ADHD comorbidities. Artificial neural networks (ANNs) algorithms were used to identify specific relationships between protein sets. Finally, we modelled the mechanisms of LDX for the most relevant comorbidities by using sampling methods and comorbidity-specific virtual patients in each case.
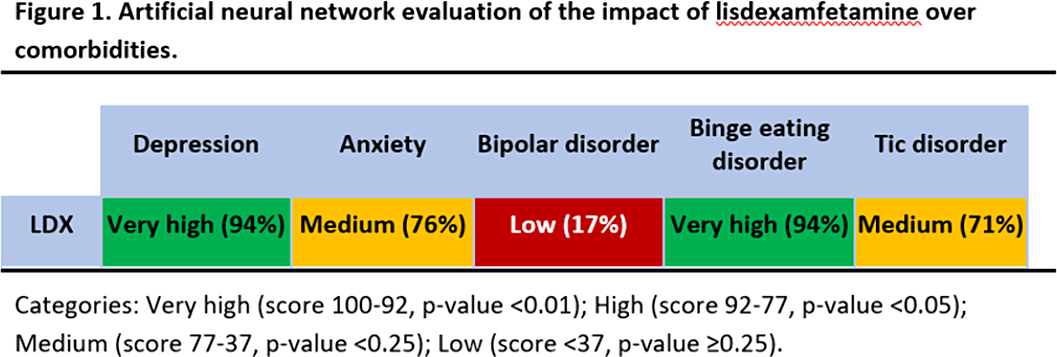
This study predicts a strong relationship between LDX’s targets and proteins involved in BED and depression (Fig 1). Our results could be explained not only by LDX role in neurotransmitter regulation, but also by modulation of neuroplasticity (BDNF/NTRK2, GSK3), neuroinflammation (interleukins, inflammasome), oxidative stress (NOS2, SOD), and the hypothalamic-pituitary-adrenal (HPA) axis (CRH, CRHR1).
These findings could be used in pre-clinical and clinical future investigations to assess optimal treatment for ADHD patients with psychiatric comorbidities.
JRGC: speaker for Takeda and Shire, research funding from Shire and Lumbeck, collaborations with Laboratoires Servier JQ: speaker or scientific advisor for Takeda, Janssen, Rubio. Investigation funding: Instituto de Salud Carlos III. PR, CM, TPR: full-ti

