
11 results
A comparison between two rTMS protocols as augmentation strategies in patients with treatment-resistant depression
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S114-S115
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Repetitive transcranial magnetic stimulation (rTMS) is an evidence-based treatment and rTMS protocols have been included in international guidelines for patients with treatment-resistant depression (TRD). The daily administration of standard rTMS protocols, typically over several weeks, could be a limiting factor (e.g., time off from work, commuting issues). To intensify the antidepressant response and to reduce the number of stimulation days, it has been proposed that increasing the number of rTMS sessions performed per day could be more effective and help to reduce the burden for patients and clinicians. Although there is much interest in accelerated TMS protocols, little is known about their efficacy and tolerability, and the literature on the topic is still scarce.
ObjectivesTo compare the efficacy and tolerability of two rTMS protocols (standard vs. accelerated) as augmentative strategies in patients with TRD.
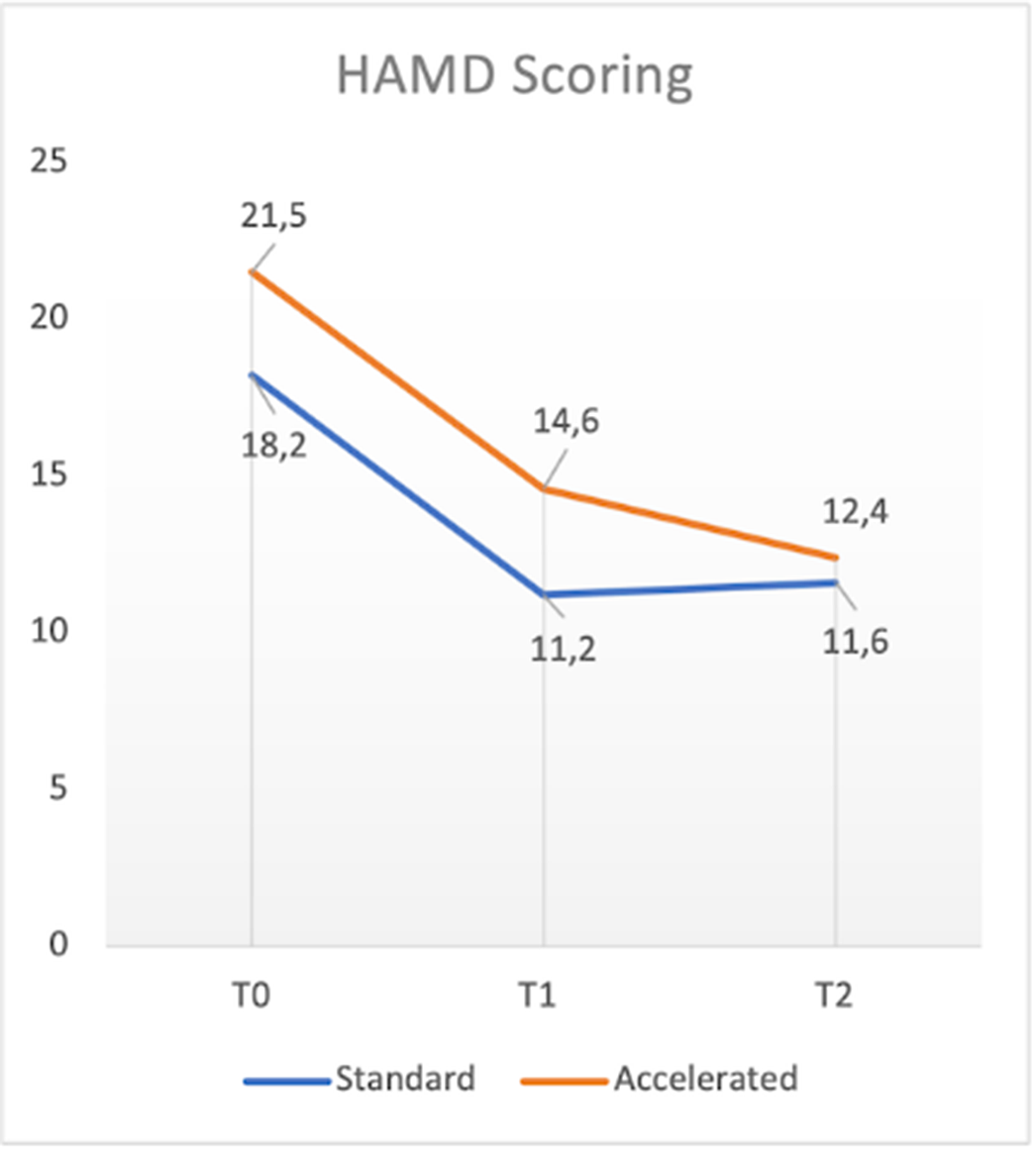
MethodsIn the present ongoing, open-label, trial 14 patients meeting DSM-5 criteria for major depressive episode (either unipolar or bipolar), classified as partial responders or non-responders to adequate pharmacological treatment, were randomized to receive either standard (one session per day, five days a week, for four weeks; n= 7) or accelerated (two sessions per day, five days a week, for two weeks; n=6) rTMS treatment protocols. In both cases, rTMS was performed on the left dorsolateral prefrontal cortex, high frequency (10 Hz) at 120% of the motor threshold, 3000 pulses per sessions. Primary outcome measures included HAM-D, MADRS, and CGI-S scores at baseline (T0), at the end of rTMS treatment (T1), and after 1 month (T2), as well as tolerability based on adverse effects. Paired Samples t-Test for continuous variables was used to compare psychometric scales at each timepoint, while t-Test was used to compare differences between the two groups.
ResultsWith respect to total sample, in terms of primary outcome measures a significant reduction of HAM-D, MADRS and CGI-S total scores between T0 and T1 (t: 3.01, p<0.05; t: 1.692, p<0.5; t:3.207, p<0.05 respectively), T1 and T2 (t: 3.264, p<0.05: t:2.669, p<0.05; t:.085, p=0.437 respectively) and T0 and T2 (t:5.669, p<0.05; t=4.711, p<0.05; t:2.551, p<0.05 respectively) was found. No significant differences in terms of efficacy were found between the two groups. One patient dropped-out for reasons not related to rTMS treatment. Mild and transient headache during the stimulation was the only side effect reported (4 patients).
Image:
 Conclusions
ConclusionsConsistently with previous literature studies, our preliminary results supported the evidence of comparable efficacy and tolerability between accelerated and standard rTMS protocols. In the future, larger, blinded, and controlled trials might support these conclusions and further address treatment parameters of novel accelerated rTMS protocols.
Disclosure of InterestNone Declared

Criminal behaviors and substance abuse in psychiatric patients
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S536-S537
-
- Article
-
- You have access
- Open access
- Export citation
Clinical relevance of Paliperidone Palmitate three-month intramuscular injection formulation: an Italian Real-World, Retrospective, one-year Mirror Image Study
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S346
-
- Article
-
- You have access
- Open access
- Export citation
Incidence and predictive factors of non adherence to therapy in young adults attending a psycho social center in Milan: a retrospective observational “Real world” study
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S691
-
- Article
-
- You have access
- Open access
- Export citation
Chapter 14 - Alagille Syndrome
- from Section II - Cholestatic Liver Disease
-
-
- Book:
- Liver Disease in Children
- Published online:
- 19 January 2021
- Print publication:
- 18 March 2021, pp 222-241
-
- Chapter
- Export citation
Effect of dietary lipids on circulating adiponectin: a systematic review with meta-analysis of randomised controlled trials
-
- Journal:
- British Journal of Nutrition / Volume 112 / Issue 8 / 28 October 2014
- Published online by Cambridge University Press:
- 05 September 2014, pp. 1235-1250
- Print publication:
- 28 October 2014
-
- Article
-
- You have access
- HTML
- Export citation
Chapter 14 - Alagille syndrome
- from Section II - Cholestatic liver disease
-
-
- Book:
- Liver Disease in Children
- Published online:
- 05 March 2014
- Print publication:
- 20 February 2014, pp 216-233
-
- Chapter
- Export citation
Optimal distribution of traffic flows in emergency cases
-
- Journal:
- European Journal of Applied Mathematics / Volume 23 / Issue 4 / August 2012
- Published online by Cambridge University Press:
- 12 April 2012, pp. 515-535
-
- Article
- Export citation
3 - Hybrid automata
- from Part I - Theory
-
-
- Book:
- Handbook of Hybrid Systems Control
- Published online:
- 21 February 2011
- Print publication:
- 15 October 2009, pp 57-86
-
- Chapter
- Export citation
15 - Alagille Syndrome
- from SECTION II - CHOLESTATIC LIVER DISEASES
-
-
- Book:
- Liver Disease in Children
- Published online:
- 18 December 2009
- Print publication:
- 07 May 2007, pp 326-345
-
- Chapter
- Export citation
Infinite time regular synthesis
-
- Journal:
- ESAIM: Control, Optimisation and Calculus of Variations / Volume 3 / 1998
- Published online by Cambridge University Press:
- 15 August 2002, pp. 381-405
- Print publication:
- 1998
-
- Article
- Export citation
