
196 results
Advancing health equity through action in antimicrobial stewardship and healthcare epidemiology
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 4 / April 2024
- Published online by Cambridge University Press:
- 14 February 2024, pp. 412-419
- Print publication:
- April 2024
-
- Article
-
- You have access
- HTML
- Export citation
Impact of primary care triage using the Head and Neck Cancer Risk Calculator version 2 on tertiary head and neck services in the post-coronavirus disease 2019 period
-
- Journal:
- The Journal of Laryngology & Otology , First View
- Published online by Cambridge University Press:
- 22 January 2024, pp. 1-6
-
- Article
- Export citation
Variations in implementation of antimicrobial stewardship via telehealth at select Veterans Affairs medical centers
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s38
-
- Article
-
- You have access
- Open access
- Export citation
Susceptibility results discrepancy analysis between NHSN antimicrobial resistance (AR) Option and NEDSS Base System in Tennessee, July 2020–December 2021
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s104
-
- Article
-
- You have access
- Open access
- Export citation
Using telehealth to support antimicrobial stewardship at four rural VA medical centers: Interim analysis
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s110
-
- Article
-
- You have access
- Open access
- Export citation
-
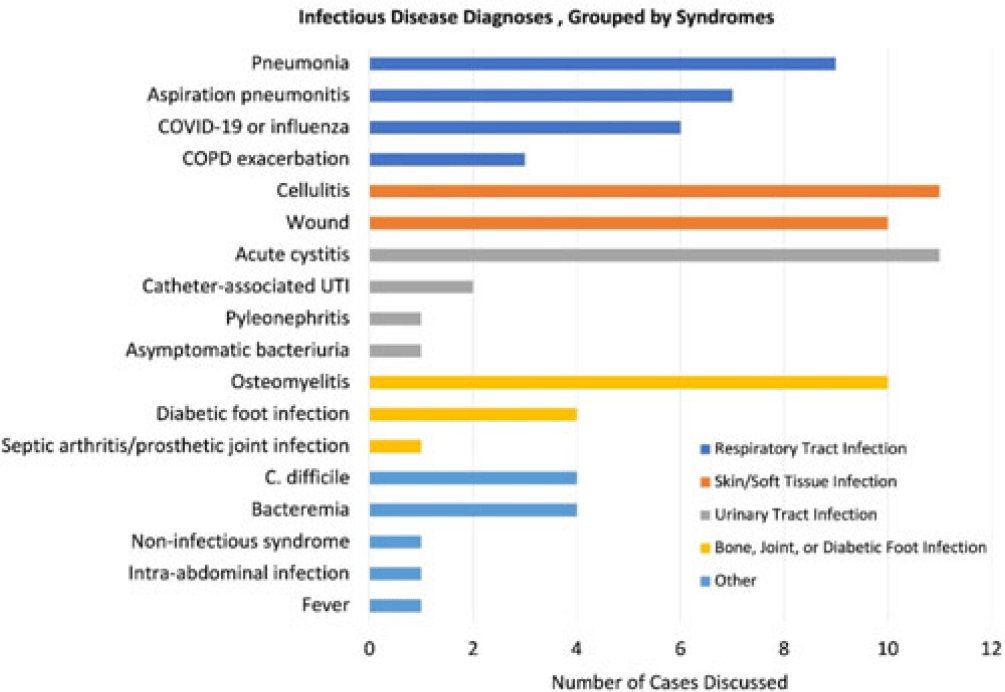
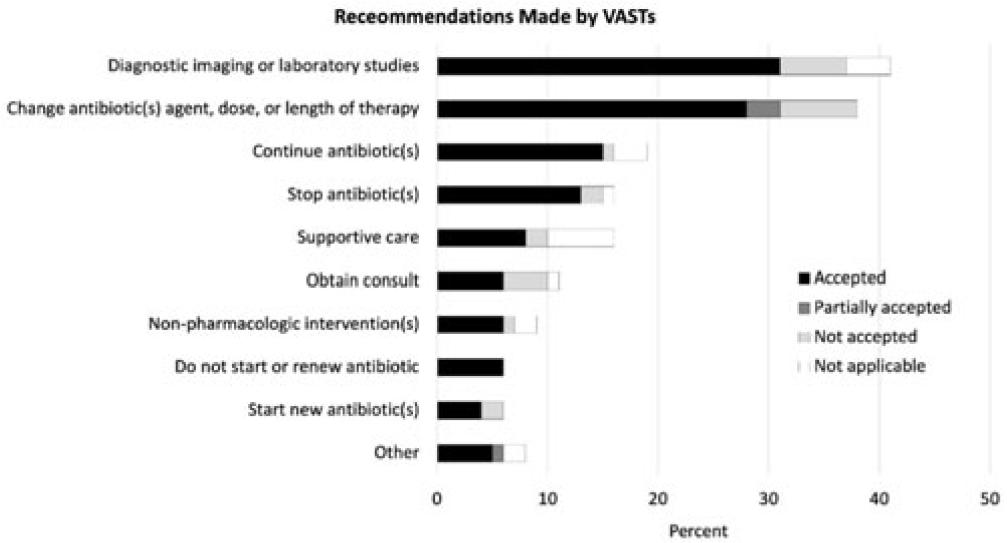
Background: Healthcare settings without access to infectious diseases experts may struggle to implement effective antibiotic stewardship programs. We previously described a successful pilot project using the Veterans Affairs (VA) telehealth system to form a Videoconference Antimicrobial Stewardship Team (VAST) that connected multidisciplinary teams from rural VA medical centers (VAMCs) with infectious diseases experts at geographically distant locations. VASTs discussed patients from the rural VAMC, with the overarching goal of supporting antibiotic stewardship. This project is currently ongoing. Here, we describe preliminary outcomes describing the cases discussed, recommendations made, and acceptance of those recommendations among 4 VASTs. Methods: Cases discussed at any of the 4 participating intervention sites were independently reviewed by study staff, noting the infectious disease diagnoses, recommendations made by infectious diseases experts and, when applicable, acceptance of those recommendations at the rural VAMC within 1 week. Discrepancies between independent reviewers were discussed and, when consensus could not be reached, discrepancies were discussed with an infectious diseases clinician. Results: The VASTs serving 4 different rural VAMCs discussed 96 cases involving 92 patients. Overall, infection of the respiratory tract was the most common syndrome discussed by VASTs (Fig. 1). The most common specific diagnoses among discussed cases were cellulitis (n = 11), acute cystitis (n = 11), wounds (n = 11), and osteomyelitis (n = 10). Of 172 recommendations, 41 (24%) related to diagnostic imaging or laboratory results and 38 (22%) were to change the antibiotic agent, dose, or duration (Fig. 2). Of the 151 recommendations that could be assessed via chart review, 122 (81%) were accepted within 1 week. Conclusions: These findings indicate successful implementation of telehealth to connect clinicians at rural VAMCs with an offsite infectious diseases expert. The cases represented an array of common infectious syndromes. The most frequent recommendations pertained to getting additional diagnostic information and to adjusting, but not stopping, antibiotic therapy. These results suggest that many of the cases discussed warrant antibiotics and that VASTs may use the results of diagnostic studies to tailor that therapy. The high rate of acceptance suggests that the VASTs are affecting patient care. Future work will describe VAST implementation at 4 additional VAMCs, and we will assess whether using telehealth to disseminate infectious diseases expertise to rural VAMCs supports changes in antibiotic use that align with principles of antimicrobial stewardship.
Disclosures: None


Determining trends of respiratory tract infections in a long-term care facility pilot surveillance project
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s24
-
- Article
-
- You have access
- Open access
- Export citation
Increasing Registration for a VA Multidrug-Resistant Organism Alert Tool
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s124-s125
-
- Article
-
- You have access
- Open access
- Export citation
-
Objectives: To address the importation of multi-drug-resistant organisms (MDROs) when a colonized or infected patient is transferred from another VA facility, the Veterans Health Administration (VHA) launched the Inpatient Pathogen Tracker (IPT) in 2020. IPT tracks MDRO-infected/colonized patients and alerts MDRO Program Coordinators (MPCs) and Infection Preventionists (IPs) when such patients are admitted to their facility to facilitate rapid identification and isolation of infected/colonized patients. IPT usage has been low during initial rollout (32.5%). The VHA and the CARRIAGE QUERI Program developed targeted implementation strategies to increase utilization of IPT’s second iteration, VA Bug Alert (VABA). Methods: Familiarity with IPT was assessed via pre-education survey (3/2022). All sites received standard VABA implementation including: 1) adaptation of VABA features based on end-user feedback (completed 4/2022), 2) development and delivery of an educational module regarding the revised tool (completed 4/2022), and 3) internal facilitation from the VHA MDRO Program Office (ongoing) (see Figure for all key timepoints). Intent to register for VABA was assessed via post-education survey (4-5/2022). Sites (125 eligible) not registered for VABA by 6/1/2022 were randomly assigned to receive one of two conditions from 6/2022–8/2022: continued standard implementation alone or enhanced implementation. Enhanced implementation added the following to standard implementation: 1) audit and feedback reports and 2) external facilitation, including interviews and education about VABA. We compared the number of sites with ≥1 MPC/IP registered for VABA to-date between implementation conditions. Results: Pre-education survey. 168 MPC/IPs across 117 sites responded (94% of eligible sites). Among respondents, 25% had used IPT, 35.1% were familiar with but had not used IPT, and 39.9% were unfamiliar with IPT. Post-education survey. 93 MPC/IPs across 80 sites responded (59% of eligible sites). Of these, 81.7% said they planned to register for VABA, 4.3% said they would not register, and 14.0% said they were unsure. Post-6/1/2022 Registrations. By 6/1/2022, 71% of sites had ≥1 registered VABA user. Of the 28 unregistered sites eligible for enhanced implementation, thirteen were assigned to receive enhanced implementation, and fifteen were assigned to receive continued standard implementation. Eight sites in the enhanced implementation condition (61.5%) registered for VABA. Seven standard-implementation-only sites (46.7%) registered. The number of registered sites did not significantly differ by implementation condition (Fisher’s exact p=0.476). Conclusions: Standard and enhanced implementation were equally effective at encouraging VABA registration, suggesting that allocating resources to enhanced implementation may not be necessary.
Disclosures: None.


Dense pasts: settlement archaeology after Fox's The archaeology of the Cambridge region (1923)
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Volatility, Realignment, and Electoral Shocks: Brexit and the UK General Election of 2019
-
- Journal:
- PS: Political Science & Politics / Volume 56 / Issue 4 / October 2023
- Published online by Cambridge University Press:
- 10 August 2023, pp. 537-545
- Print publication:
- October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Incidence and risk factors for clinically confirmed secondary bacterial infections in patients hospitalized for coronavirus disease 2019 (COVID-19)
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 10 / October 2023
- Published online by Cambridge University Press:
- 15 May 2023, pp. 1650-1656
- Print publication:
- October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
No effects of synchronicity in online social dilemma experiments: A registered report
-
- Journal:
- Judgment and Decision Making / Volume 16 / Issue 4 / July 2021
- Published online by Cambridge University Press:
- 01 January 2023, pp. 823-843
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Chapter 5 - Financing Health Care
- from Section 1 - Analyzing Health Systems: Concepts, Components, Performance
-
-
- Book:
- Making Health Systems Work in Low and Middle Income Countries
- Published online:
- 08 December 2022
- Print publication:
- 29 December 2022, pp 67-82
-
- Chapter
- Export citation
The Evolutionary Map of the Universe Pilot Survey – ADDENDUM
-
- Journal:
- Publications of the Astronomical Society of Australia / Volume 39 / 2022
- Published online by Cambridge University Press:
- 02 November 2022, e055
-
- Article
- Export citation
Examining the Scope of Nuclear Weapons-Related Activities Covered under the Environmental Remediation Obligation of the Treaty on the Prohibition of Nuclear Weapons
-
- Journal:
- Asian Journal of International Law / Volume 13 / Issue 2 / July 2023
- Published online by Cambridge University Press:
- 22 September 2022, pp. 365-390
- Print publication:
- July 2023
-
- Article
- Export citation
A Three-Dimensional Reconstruction Algorithm for Scanning Transmission Electron Microscopy Data from a Single Sample Orientation
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue 5 / October 2022
- Published online by Cambridge University Press:
- 24 June 2022, pp. 1632-1640
- Print publication:
- October 2022
-
- Article
- Export citation
-
Increasing interest in three-dimensional nanostructures adds impetus to electron microscopy techniques capable of imaging at or below the nanoscale in three dimensions. We present a reconstruction algorithm that takes as input a focal series of four-dimensional scanning transmission electron microscopy (4D-STEM) data. We apply the approach to a lead iridate, Pb
 $_2$Ir
$_2$Ir $_2$O
$_2$O $_7$, and yttrium-stabilized zirconia, Y
$_7$, and yttrium-stabilized zirconia, Y $_{0.095}$Zr
$_{0.095}$Zr $_{0.905}$O
$_{0.905}$O $_2$, heterostructure from data acquired with the specimen in a single plan-view orientation, with the epitaxial layers stacked along the beam direction. We demonstrate that Pb–Ir atomic columns are visible in the uppermost layers of the reconstructed volume. We compare this approach to the alternative techniques of depth sectioning using differential phase contrast scanning transmission electron microscopy (DPC-STEM) and multislice ptychographic reconstruction.
$_2$, heterostructure from data acquired with the specimen in a single plan-view orientation, with the epitaxial layers stacked along the beam direction. We demonstrate that Pb–Ir atomic columns are visible in the uppermost layers of the reconstructed volume. We compare this approach to the alternative techniques of depth sectioning using differential phase contrast scanning transmission electron microscopy (DPC-STEM) and multislice ptychographic reconstruction.






Increased carbapenemase testing following implementation of national VA guidelines for carbapenem-resistant Enterobacterales (CRE)
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 02 June 2022, e88
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Susceptibility results discrepancy analysis between NHSN Antibiotic Resistance (AR) Option and laboratory instrument data
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s66
-
- Article
-
- You have access
- Open access
- Export citation
Effect of the COVID-19 pandemic on Tennessee hospital antibiotic use
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s20
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: On March 5, 2020, the Tennessee Department of Health (TDH) announced the first case of COVID-19 in the state. Since then, hospitals have been overwhelmed by the spike in respiratory infections. Several studies have attempted to describe the impact of the pandemic on antibiotic prescriptions. The NHSN Antimicrobial Use Option offers a platform for hospitals to report their antibiotic usage. The TDH has established access to hospital antibiotic usage data statewide through an existing NHSN user group. We compared the change in the volume of inpatient antibiotic prescriptions before and during the pandemic. Methods: An ecological study was conducted from January 2019 to December 2021. Aggregated facility-level data from the NHSN Antimicrobial Use Option were used to describe antibacterial use among Tennessee hospitals. Data from facilities that had reported at least 1 month of data during the study period were included in this study. The antimicrobial use rate was calculated by dividing the antimicrobial days of therapy (DOT) by the number of 1,000 days present. Overall antimicrobial use rates as well as specific antimicrobial use rates for azithromycin, ceftriaxone, and piperacillin–tazobactam were compared across years. Results: In total, 55 hospitals reported at least 1 month of data into the NHSN Antimicrobial Use Option during the study period. These hospitals had a median bed size of 140 (range, 12–689). Conclusions: We observed a modest increase in overall antibiotic use during the COVID-19 pandemic in Tennessee facilities. This trend appeared to be primarily attributed to agents used for community-acquired respiratory infections, such as azithromycin and ceftriaxone, earlier in the pandemic. However, both of these agents have fallen to prepandemic use levels during 2021. The fact that overall use increased in 2021 suggests that other agents not analyzed may have contributed to this effect. Further analysis may help determine which agents are responsible for this increase in 2021.
Funding: None
Disclosures: None


Determining the effect of COVID-19 on antibiotic use in long-term care facilities across Tennessee
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s21-s22
-
- Article
-
- You have access
- Open access
- Export citation
Effects of antibiotic suppression on three healthcare systems’ National Healthcare Safety Network Antibiotic Resistance Option data
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue 1 / 2021
- Published online by Cambridge University Press:
- 10 November 2021, e47
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
