
135 results
4 Evaluating Plasma GFAP for the Detection of Alzheimer’s Disease Dementia
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 408-409
-
- Article
-
- You have access
- Export citation
6 Association Between American Football Play and Parkinson's Disease: Analysis of the Fox Insight Data Set
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 415-416
-
- Article
-
- You have access
- Export citation
64 Neuroimaging Evidence of Neurodegenerative Disease in Former Professional American Football Players Who “Fail” Validity Testing: A Case Series
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 574-575
-
- Article
-
- You have access
- Export citation
5 Antemortem Plasma GFAP Predicts Alzheimer’s Disease Neuropathological Changes
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 409-410
-
- Article
-
- You have access
- Export citation
Participation in the Georgia Food for Health programme and CVD risk factors: a longitudinal observational study
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 11 / November 2023
- Published online by Cambridge University Press:
- 07 August 2023, pp. 2470-2479
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The use of a Subjective wellbeing scale as predictor of adherence to neuroleptic treatment to determine poor prognostic factor in African population with Schizophrenia
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S156
-
- Article
-
- You have access
- Open access
- Export citation
Random variation drives a critical bias in the comparison of healthcare-associated infections
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 9 / September 2023
- Published online by Cambridge University Press:
- 10 March 2023, pp. 1396-1402
- Print publication:
- September 2023
-
- Article
- Export citation
The thalamus and its subregions – a gateway to obsessive-compulsive disorder
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, pp. S77-S78
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Higher thalamic volume has been found in children with obsessive-compulsive disorder (OCD) and children with clinical-level symptoms within the general population (Boedhoe et al. 2017, Weeland et al. 2021a). Functionally distinct thalamic nuclei are an integral part of OCD-relevant brain circuitry.
ObjectivesWe aimed to study the thalamic nuclei volume in relation to subclinical and clinical OCD across different age ranges. Understanding the role of thalamic nuclei and their associated circuits in pediatric OCD could lead towards treatment strategies specifically targeting these circuits.
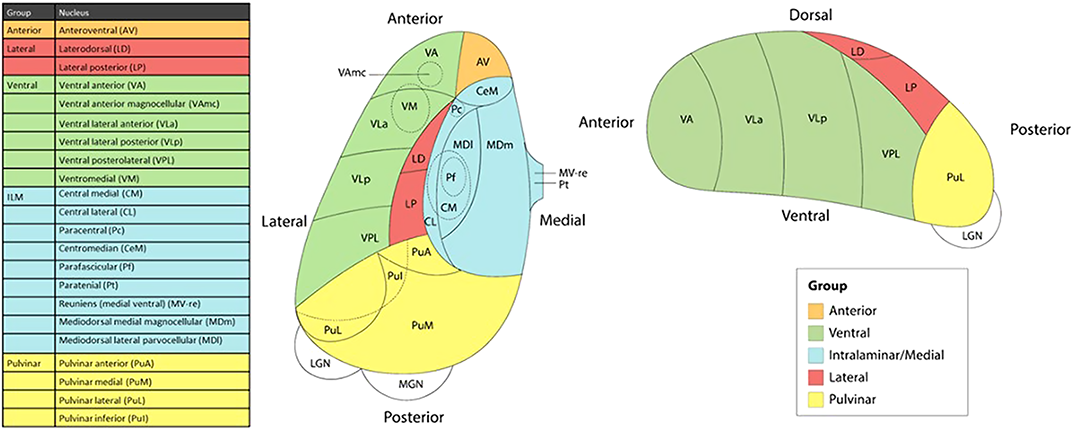
MethodsWe studied the relationship between thalamic nuclei and obsessive-compulsive symptoms (OCS) in a large sample of school-aged children from the Generation R Study (N = 2500) (Weeland et al. 2021b). Using the data from the ENIGMA-OCD working group we conducted mega-analyses to study thalamic subregional volume in OCD across the lifespan in 2,649 OCD patients and 2,774 healthy controls across 29 sites (Weeland et al. 2021c). Thalamic nuclei were grouped into five subregions: anterior, ventral, intralaminar/medial, lateral and pulvinar (Figure 1).
 Results
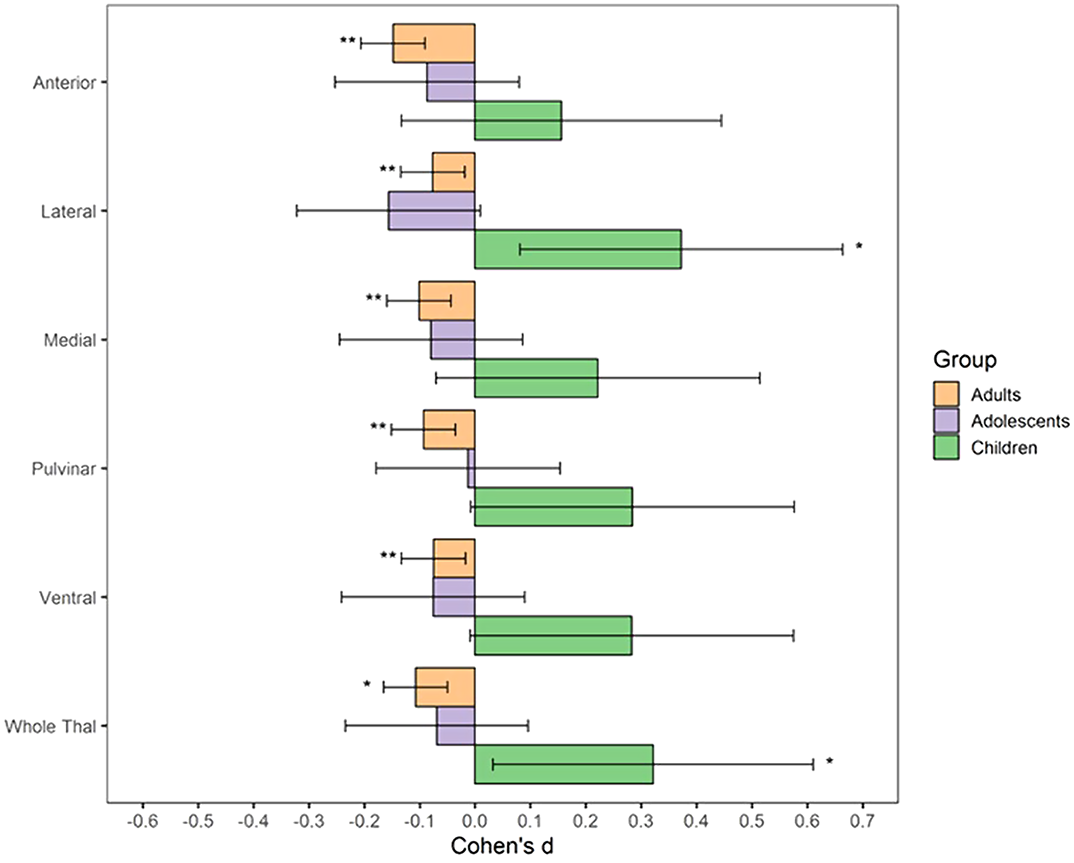
ResultsBoth children with subclinical and clinical OCD compared with controls show increased volume across multiple thalamic subregions. Adult OCD patients have decreased volume across all subregions (Figure 2), which was mostly driven by medicated and adult-onset patients.
 Conclusions
ConclusionsOur results suggests that OCD-related thalamic volume differences are global and not driven by particular subregions and that the direction of effects are driven by both age and medication status.
DisclosureNo significant relationships.


Risk of bacterial bloodstream infection does not vary by central-line type during neutropenic periods in pediatric acute myeloid leukemia
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 2 / February 2023
- Published online by Cambridge University Press:
- 25 April 2022, pp. 222-229
- Print publication:
- February 2023
-
- Article
- Export citation
Pain perception and physiological correlates in body-focused repetitive behavior disorders
-
- Journal:
- CNS Spectrums / Volume 28 / Issue 2 / April 2023
- Published online by Cambridge University Press:
- 22 March 2022, pp. 197-204
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Childhood adversities and mental disorders in first-year college students: results from the World Mental Health International College Student Initiative
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 7 / May 2023
- Published online by Cambridge University Press:
- 11 January 2022, pp. 2963-2973
-
- Article
- Export citation
Effects of prior deployments and perceived resilience on anger trajectories of combat-deployed soldiers
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 5 / April 2023
- Published online by Cambridge University Press:
- 22 November 2021, pp. 2031-2040
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Neurobiology of subtypes of trichotillomania and skin picking disorder
-
- Journal:
- CNS Spectrums / Volume 28 / Issue 1 / February 2023
- Published online by Cambridge University Press:
- 03 November 2021, pp. 98-103
-
- Article
- Export citation
Antidepressant use in low- middle- and high-income countries: a World Mental Health Surveys report
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 4 / March 2023
- Published online by Cambridge University Press:
- 23 September 2021, pp. 1583-1591
-
- Article
- Export citation
Direct maxillary irrigation therapy in non-operated chronic sinusitis: a prospective randomised controlled trial
-
- Journal:
- The Journal of Laryngology & Otology / Volume 136 / Issue 3 / March 2022
- Published online by Cambridge University Press:
- 01 September 2021, pp. 229-236
- Print publication:
- March 2022
-
- Article
- Export citation
Non-suicidal self-injury among first-year college students and its association with mental disorders: results from the World Mental Health International College Student (WMH-ICS) initiative
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 3 / February 2023
- Published online by Cambridge University Press:
- 18 June 2021, pp. 875-886
-
- Article
- Export citation
The prevalence of mental health problems in sub-Saharan adolescents living with HIV: a systematic review
-
- Journal:
- Global Mental Health / Volume 7 / 2020
- Published online by Cambridge University Press:
- 26 October 2020, e29
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Comorbidity within mental disorders: a comprehensive analysis based on 145 990 survey respondents from 27 countries
-
- Journal:
- Epidemiology and Psychiatric Sciences / Volume 29 / 2020
- Published online by Cambridge University Press:
- 12 August 2020, e153
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Intermittent explosive disorder subtypes in the general population: association with comorbidity, impairment and suicidality
-
- Journal:
- Epidemiology and Psychiatric Sciences / Volume 29 / 2020
- Published online by Cambridge University Press:
- 23 June 2020, e138
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Unit cohesion during deployment and post-deployment mental health: is cohesion an individual- or unit-level buffer for combat-exposed soldiers?
-
- Journal:
- Psychological Medicine / Volume 52 / Issue 1 / January 2022
- Published online by Cambridge University Press:
- 10 June 2020, pp. 121-131
-
- Article
- Export citation
