
200 results
546 Using Contingency Management to Understand the Cardiovascular, Immune and Psychosocial Benefits of Reduced Cocaine Use: A Protocol for a Randomized Controlled Trial
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue s1 / April 2024
- Published online by Cambridge University Press:
- 03 April 2024, p. 163
-
- Article
-
- You have access
- Open access
- Export citation
Population and hospital-level COVID-19 measures are associated with increased risk of hospital-onset COVID-19
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 18 March 2024, pp. 1-3
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The prevalence of gram-negative bacteria with difficult-to-treat resistance and utilization of novel β-lactam antibiotics in the southeastern United States
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 18 March 2024, e35
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Implementation of contact precautions for multidrug-resistant organisms in the post–COVID-19 pandemic era: An updated national Emerging Infections Network (EIN) survey
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 14 February 2024, pp. 1-6
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Simultaneous submission of seven CTSA proposals: UM1, K12, R25, T32-predoctoral, T32-postdoctoral, and RC2: strategies, evaluation, and lessons learned
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 25 January 2024, e33
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A severe acute respiratory coronavirus virus 2 (SARS-CoV-2) nosocomial cluster with inter-facility spread: Lessons learned
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 5 / May 2024
- Published online by Cambridge University Press:
- 04 January 2024, pp. 635-643
- Print publication:
- May 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
78 Examining the Association Between a Patient's Diagnosis and Occurrence of The First Error on Trails B
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, p. 280
-
- Article
-
- You have access
- Export citation
Use of contact precautions for multidrug-resistant organisms and the impact of the COVID-19 pandemic: An Emerging Infections Network (EIN) survey
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s102-s103
-
- Article
-
- You have access
- Open access
- Export citation
-
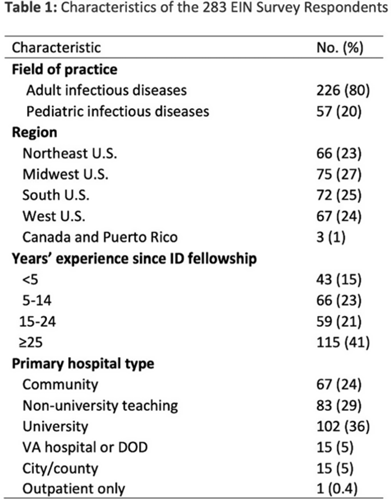
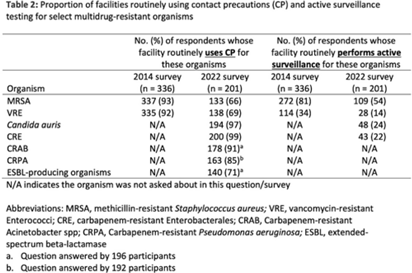
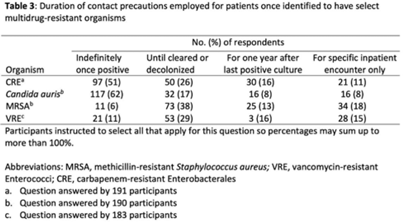
Background: The CDC recommends routine use of contact precautions for patients infected or colonized with multidrug-resistant organisms (MDROs). There is variability in implementation of and adherence to this recommendation, which we hypothesized may have been exacerbated by the COVID-19 pandemic. Methods: In September 2022, we emailed an 8-question survey to Emerging Infections Network (EIN) physician members with infection prevention and hospital epidemiology responsibilities. The survey asked about the respondent’s primary hospital’s recommendations on transmission-based precautions, adjunctive measures to reduce MDRO transmission, and changes that occurred during the COVID-19 pandemic. We sent 2 reminder emails over a 1-month period. We used descriptive statistics to summarize the data and to compare results to a similar EIN survey (n = 336) administered in 2014 (Russell D, et al. doi:10.1017/ice.2015.246). Results: Of 708 EIN members, 283 (40%) responded to the survey, and 201 were involved in infection prevention. Most respondents were adult infectious diseases physicians (n = 228, 80%) with at least 15 years of experience (n = 174, 63%). Respondents were well distributed among community, academic, and nonuniversity teaching facilities (Table 1). Most respondents reported that their facility routinely used CP for methicillin-resistant Staphylococcus aureus (MRSA, 66%) and vancomycin-resistant Enterococcus (VRE, 69%), compared to 93% and 92% respectively, in the 2014 survey. Nearly all (>90%) reported using contact precautions for Candida auris, carbapenem-resistant Enterobacterales (CRE), and carbapenem-resistant Acinetobacter spp, but there was variability in the use of contact precautions for carbapenem-resistant Pseudomonas aeruginosa and extended-spectrum β-lactamase–producing gram-negative organisms. In 2014, 81% reported that their hospital performed active surveillance testing for MRSA, and in 2022 this rate fell to 54% (Table 2). The duration of contact precautions varied by MDRO (Table 3). Compared to 2014, in 2022 facilities were less likely to use contact precautions indefinitely for MRSA (18% vs 6%) and VRE (31% vs 11%). Also, 180 facilities (90%) performed chlorhexidine bathing in at least some inpatients and 106 facilities (53%) used ultraviolet light or hydrogen peroxide vapor disinfection at discharge in some rooms. Furthermore, 89 facilities (44%) reported institutional changes to contact precautions policies after the start of the COVID-19 pandemic that remain in place. Conclusions: Use of contact precautions for patients with MDROs is heterogenous, and policies vary based on the organism. Although most hospitals still routinely use contact precautions for MRSA and VRE, this practice has declined substantially since 2014. Changes in contact-precaution policies may have been influenced by the COVID-19 pandemic, and more specifically, contemporary public health guidance is needed to define who requires contact precautions and for what duration.
Disclosures: None



Hospital-onset COVID-19: Associations with population- and hospital-level measures to guide infection prevention efforts
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s7
-
- Article
-
- You have access
- Open access
- Export citation
-
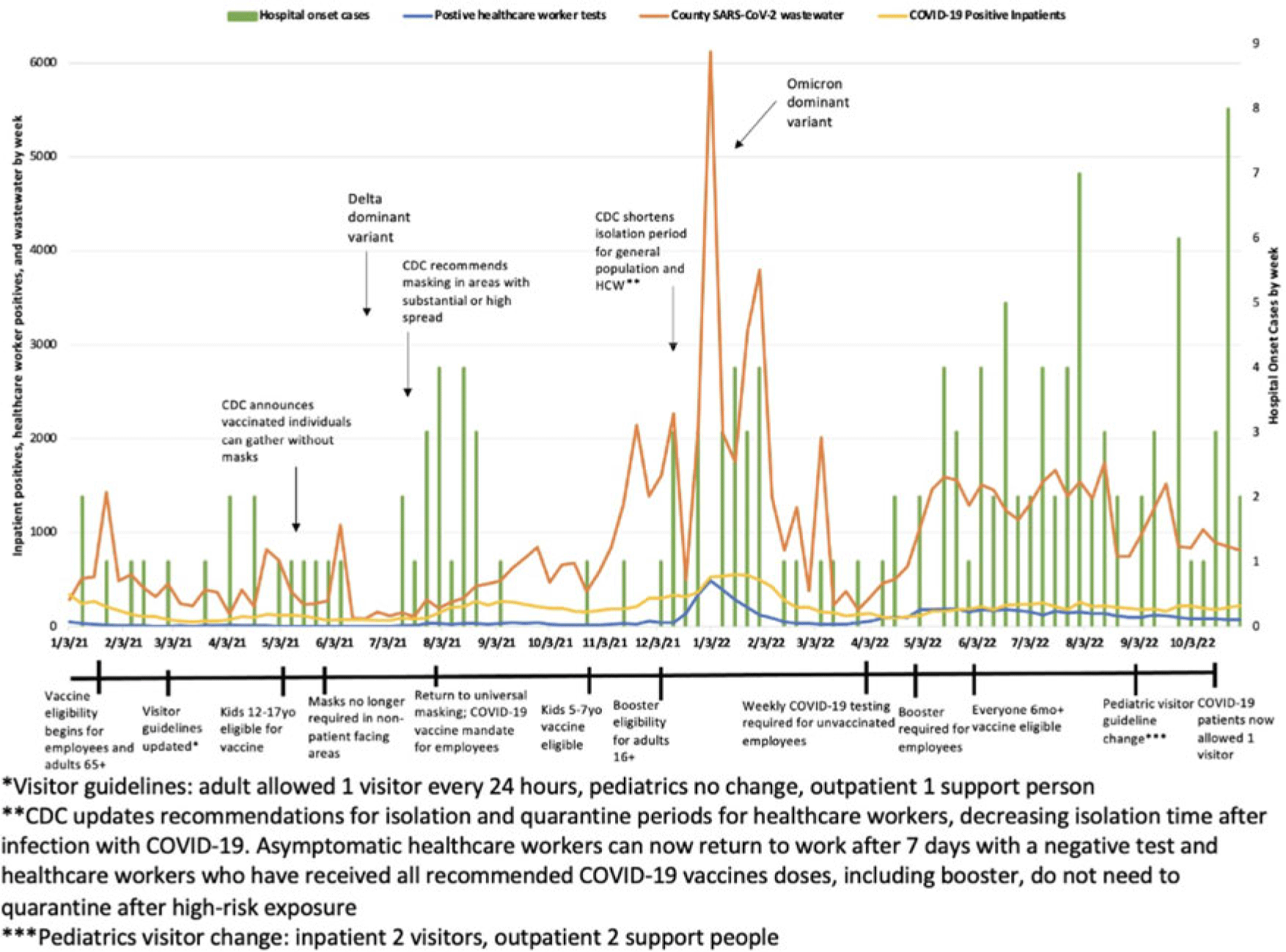
Objective: To characterize hospital-onset COVID-19 cases and to investigate the associations between these rates and population and hospital-level rates including trends in healthcare worker infections (HCW), community cases, and COVID-19 wastewater data. Design: Retrospective cohort study from January 1, 2021, to November 23, 2022. Setting: This study was conducted at a 589-bed urban Midwestern tertiary-care hospital system. Participants and interventions: The infection prevention team reviewed the electronic medical records (EMR) of patients who were admitted for >48 hours and subsequently tested positive for SARS-CoV-2 to determine whether COVID-19 was likely to be hospital-onset illness. Each case was further categorized as definite, probable, or possible based on viral sequencing, caregiver tracing analysis, symptoms, and cycle threshold values. Patients were excluded if there was a known exposure prior to admission. Clinical data including vaccination status were collected from the EMR. HCW case data were collected via our institution’s employee health services. Community cases and wastewater data were collected via the Wisconsin Department of Health Services database. Additionally, we evaluated the timing of changes in infection prevention guidance such as visitor restrictions. Results: In total, 156 patients met criteria for hospital-onset COVID-19. Overall, 6% of cases were categorized as definite, 24% were probable, and 70% were possible hospital-onset illness. Most patients were tested prior to a procedure (31%), for new symptoms (30%), and for discharge planning (30%). Also, 53% were symptomatic and 41% received treatment for their COVID-19. Overall, 38% of patients were immunocompromised and 27% were unvaccinated. Overall, 12% of patients died within 1 month of their positive SARS-CoV-2 test, and 11% required ICU admission during their hospital stay. Hospital-onset COVID-19 increased in fall of 2022. Specifically, October 2022 had 16 cases, whereas fall of 2021 (September–November) only had 3 cases total. Finally, similar peaks were observed in total cases by week between healthcare workers, county cases, and COVID-19 wastewater levels. These peaks correspond with the SARS-CoV-2 delta and omicron variant surges, respectively. Conclusions: Hospital-onset cases followed similar trends as population and hospital-level data throughout the study period. However, hospital-onset rate did not correlate as strongly in the second half of 2022 when cases were disproportionately high. Given that hospital-onset cases can result in significant morbidity, continued enhanced infection prevention efforts and low threshold for testing are warranted in the inpatient environment.
Disclosure: None

Agricultural Research Service Weed Science Research: Past, Present, and Future
-
- Journal:
- Weed Science / Volume 71 / Issue 4 / July 2023
- Published online by Cambridge University Press:
- 16 August 2023, pp. 312-327
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Psychological interventions for cancer-related post-traumatic stress disorder: narrative review
-
- Journal:
- BJPsych Bulletin / Volume 48 / Issue 2 / April 2024
- Published online by Cambridge University Press:
- 08 June 2023, pp. 100-109
- Print publication:
- April 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Risk factors for long coronavirus disease 2019 (long COVID) among healthcare personnel, Brazil, 2020–2022
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 05 June 2023, pp. 1972-1978
- Print publication:
- December 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Cannabis use as a potential mediator between childhood adversity and first-episode psychosis: results from the EU-GEI case–control study
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 15 / November 2023
- Published online by Cambridge University Press:
- 04 May 2023, pp. 7375-7384
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The association between reasons for first using cannabis, later pattern of use, and risk of first-episode psychosis: the EU-GEI case–control study
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 15 / November 2023
- Published online by Cambridge University Press:
- 02 May 2023, pp. 7418-7427
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Detection of severe acute respiratory coronavirus virus 2 (SARS-CoV-2) in the air near patients using noninvasive respiratory support devices
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 5 / May 2023
- Published online by Cambridge University Press:
- 15 March 2023, pp. 843-845
- Print publication:
- May 2023
-
- Article
- Export citation
Infection prevention and antibiotic stewardship program needs and practices in 2021: A survey of the Society for Healthcare Epidemiology of America Research Network
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 14 March 2023, pp. 948-950
- Print publication:
- June 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Success stories cause false beliefs about success
-
- Journal:
- Judgment and Decision Making / Volume 16 / Issue 6 / November 2021
- Published online by Cambridge University Press:
- 01 January 2023, pp. 1439-1463
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Belief bias and representation in assessing the Bayesian rationality of others
-
- Journal:
- Judgment and Decision Making / Volume 14 / Issue 1 / January 2019
- Published online by Cambridge University Press:
- 01 January 2023, pp. 1-10
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Chapter 16 - Interprofessional Education in Mental Health Services
- from Section 4 - Bridging the Gaps: Foundation Years and Interprofessional Education
-
-
- Book:
- Clinical Topics in Teaching Psychiatry
- Published online:
- 24 November 2022
- Print publication:
- 08 December 2022, pp 187-198
-
- Chapter
- Export citation
Child maltreatment, migration and risk of first-episode psychosis: results from the multinational EU-GEI study
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 13 / October 2023
- Published online by Cambridge University Press:
- 28 October 2022, pp. 6150-6160
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
