
127 results
98 The Crosstalk between Mitochondrial Dysfunction and Neurodevelopmental Outcomes in Preterm Infants with Pain/Stress in the NICU
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue s1 / April 2024
- Published online by Cambridge University Press:
- 03 April 2024, p. 27
-
- Article
-
- You have access
- Open access
- Export citation
Preventing unnecessary urine cultures at a Veteran’s affairs healthcare system
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 25 March 2024, pp. 1-3
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Estimating minimum dietary diversity for children aged 6–23 months: a comparison of agreement and cost of two recall methods in Cambodia and Zambia
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 22 January 2024, e79
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Inspiring diverse researchers in Virginia: Cultivating research excellence through a career-building program
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 22 January 2024, e27
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Invited Symposium 3: Pediatric Neuropsychology Medical Advances and Life Span Outcomes
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 665-666
-
- Article
-
- You have access
- Export citation
1 Sex Differences in Associations Between APOE ε2 and Longitudinal Cognitive Decline
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 405-406
-
- Article
-
- You have access
- Export citation
3 Does External Locus of Control Moderate the Intergenerational Transmission of Dementia Risk Among Non-Latinx Black and Non-Latinx White Middle-Aged Adults?
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 785-786
-
- Article
-
- You have access
- Export citation
80 The Association between Periodontal Disease and Self-Reported Cognitive and Functional Decline at Age 60 in a Large, Multicultural Cohort Study
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 383-384
-
- Article
-
- You have access
- Export citation
15 Does Subjective Socioeconomic Status Mediate the Relationship Between Objective Socioeconomic Status and Neuropsychological Test Performance Across Race and Ethnicity?
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 430-431
-
- Article
-
- You have access
- Export citation
30 Item response theory and differential item functioning of the AD8: The High School & Beyond Study
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, p. 240
-
- Article
-
- You have access
- Export citation
45 The Impact of Loneliness on Amyloid Burden, Cerebrovascular Disease, Neurodegeneration, and Memory Performance in a Community-Based Sample of Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 455-456
-
- Article
-
- You have access
- Export citation
6 Racial Discrimination and White Matter Integrity Among Black Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 788-789
-
- Article
-
- You have access
- Export citation
81 Occupation Complexity Mediates the Association between Education and Self-Reported Cognitive and Functional Decline in 60-Year-Olds
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 384-385
-
- Article
-
- You have access
- Export citation
4 Associations Between Education, Emotional and Instrumental Support, and Cognitive Function in Black, White, and Latinx Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 88-89
-
- Article
-
- You have access
- Export citation
5 Association of Discrimination to Cognition Among US-Born and Immigrant Latinx
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 89-90
-
- Article
-
- You have access
- Export citation
The Global Dynamics of Inequality (GINI) project: analysing archaeological housing data
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Outcomes after initial heart failure consultation in Fontan patients
-
- Journal:
- Cardiology in the Young , First View
- Published online by Cambridge University Press:
- 28 November 2023, pp. 1-8
-
- Article
- Export citation
Subsurface scientific exploration of extraterrestrial environments (MINAR 5): analogue science, technology and education in the Boulby Mine, UK – CORRIGENDUM
-
- Journal:
- International Journal of Astrobiology / Volume 23 / 2024
- Published online by Cambridge University Press:
- 06 November 2023, e2
-
- Article
-
- You have access
- HTML
- Export citation
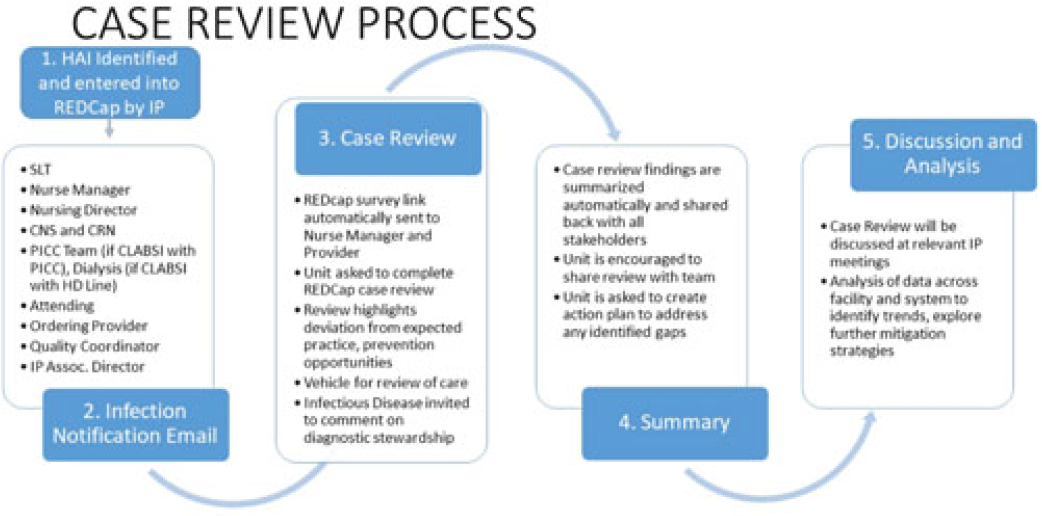
Electrifying the case review process for better speed, reach, and impact
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s95
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Prevention of healthcare-associated infections (HAIs) requires timely feedback to and input from all staff involved in patient care to best identify practice gaps and improvement targets. However, multidisciplinary review of HAI events can be challenging to promptly complete given staffing shortages and the excess administrative burden of emailed and printed forms and disjointed analyses, reporting, and visualization tools. Plagued by a lack of feedback from attending and ordering physicians, difficulty transcribing and analyzing nonstandardized data, and challenges in summarizing and distributing actionable findings, we sought to reduce turnaround time (TAT), improve data collection, and broaden communication of HAI contributing factors and proposed solutions. Methods: A secure web application for electronic data capture and reporting, Research Electronic Data Capture (REDCap), was used; the software application is free to nonprofit organizations. The review process is now initiated by an infection preventionist entering HAI information into an initial survey, which automatically cascades information into 4 subsequent surveys, distributed through automated email links, providing an opportunity for individual responses from the nursing unit, the attending provider, an infectious disease physician, and the ordering provider for the positive test that detected the HAI. Survey questions focus on evaluation of adherence to CDC and SHEA HAI prevention strategies. Reminders are automatically generated and continue to be sent to involved staff until their portion is completed. Survey responses are automatically summarized upon completion of all reviews and are shared with several stakeholders, including hospital leadership, the care team, infection prevention staff, and quality-control partners (Fig.). Discrete qualitative and quantitative data are exported in a standard application-programming interface (API) format for immediate analysis and interpretation. Results: After the review process was launched using new electronic technology, the average TAT and completion rate improved from 23 days and 40% to 7 days and 95%, respectively. Input from ordering and attending physicians, once extremely rare, became frequent. Nuanced insight into causative and preventive factors, previously unachievable, occurred during review of all 38 HAIs reported in December 2022. Reviewers believed that 48% of HAIs reviewed could have been prevented. Conclusions: Applying electronic technology to HAI case review improved completion and timeliness of reviews by both providers and nurses. By sharing data and insights with all stakeholders in real time, the new procedure permitted multidirectional communication between the care teams and increased awareness of patient harm as well as ownership of patient safety. Our process is freely and readily generalizable to any nonprofit healthcare facility.
Disclosures: None

Snack frequency, size, and energy density are associated with diet quality among US adolescents
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 11 / November 2023
- Published online by Cambridge University Press:
- 07 August 2023, pp. 2374-2382
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
