
222 results
Research agenda for transmission prevention within the Veterans Health Administration, 2024–2028
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 11 April 2024, pp. 1-10
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
59 Objectively-Measured Performance on Tests of Episodic Memory and Executive Function in Autopsy-Confirmed Chronic Traumatic Encephalopathy
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 264-265
-
- Article
-
- You have access
- Export citation
Strengthening self-regulation and reducing poverty to prevent adolescent depression and anxiety: Rationale, approach and methods of the ALIVE interdisciplinary research collaboration in Colombia, Nepal and South Africa
- Part of
-
- Journal:
- Epidemiology and Psychiatric Sciences / Volume 32 / 2023
- Published online by Cambridge University Press:
- 13 December 2023, e69
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Treatment effectiveness of antibiotic therapy in Veterans with multidrug-resistant Acinetobacter spp. bacteremia
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 12 December 2023, e230
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Investigating the association between characteristics of local crisis care systems and service use in an English national survey – CORRIGENDUM
-
- Journal:
- BJPsych Open / Volume 10 / Issue 1 / January 2024
- Published online by Cambridge University Press:
- 06 December 2023, e6
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Investigating the association between characteristics of local crisis care systems and service use in an English national survey
-
- Journal:
- BJPsych Open / Volume 9 / Issue 6 / November 2023
- Published online by Cambridge University Press:
- 03 November 2023, e209
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Lessons from leadership transition of an AMR telementoring program to sustain laboratory capacity building in Ethiopia
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s123
-
- Article
-
- You have access
- Open access
- Export citation
Active surveillance and contact precautions for preventing MRSA healthcare-associated infections during the COVID-19 pandemic
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s117-s118
-
- Article
-
- You have access
- Open access
- Export citation
-
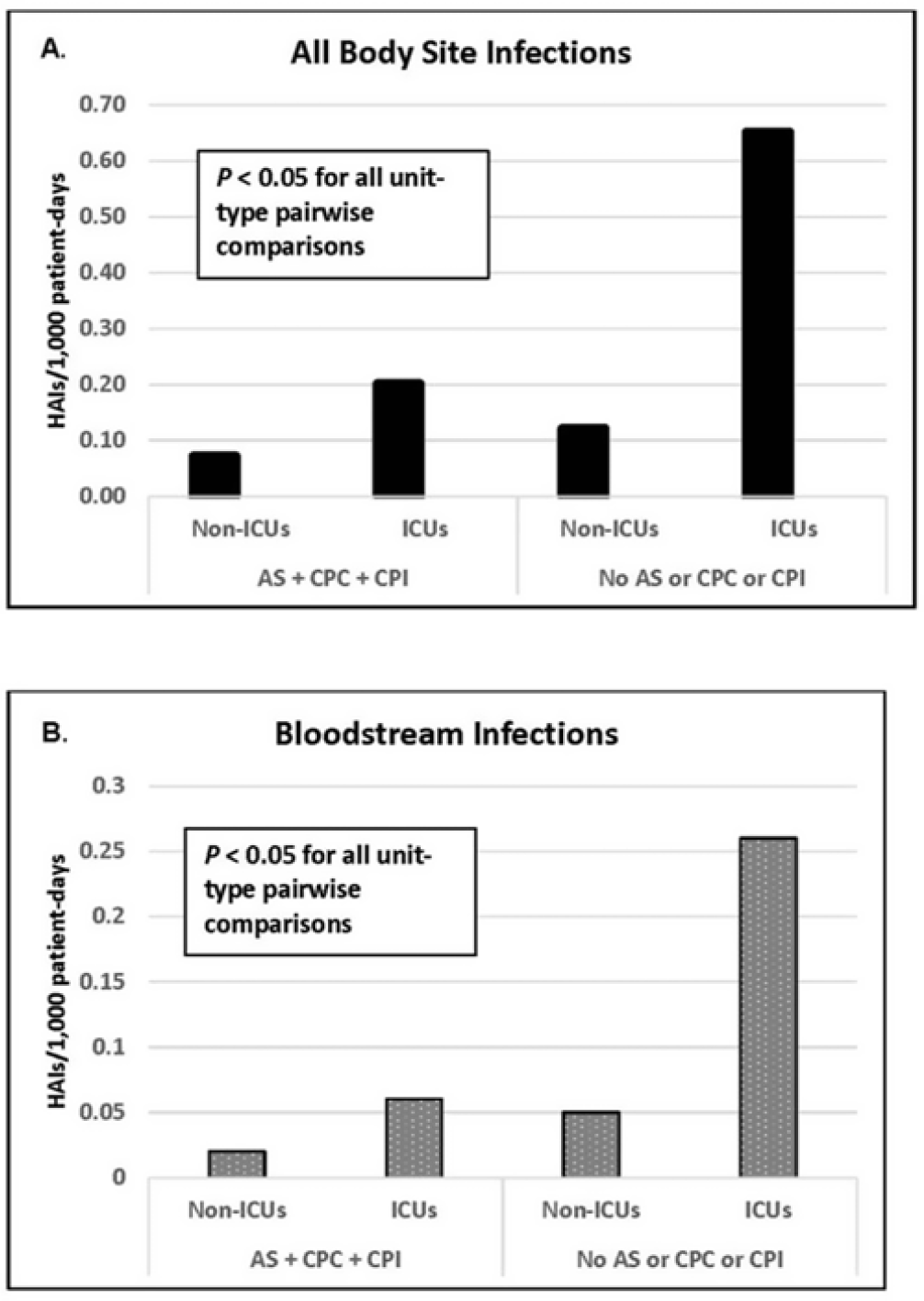
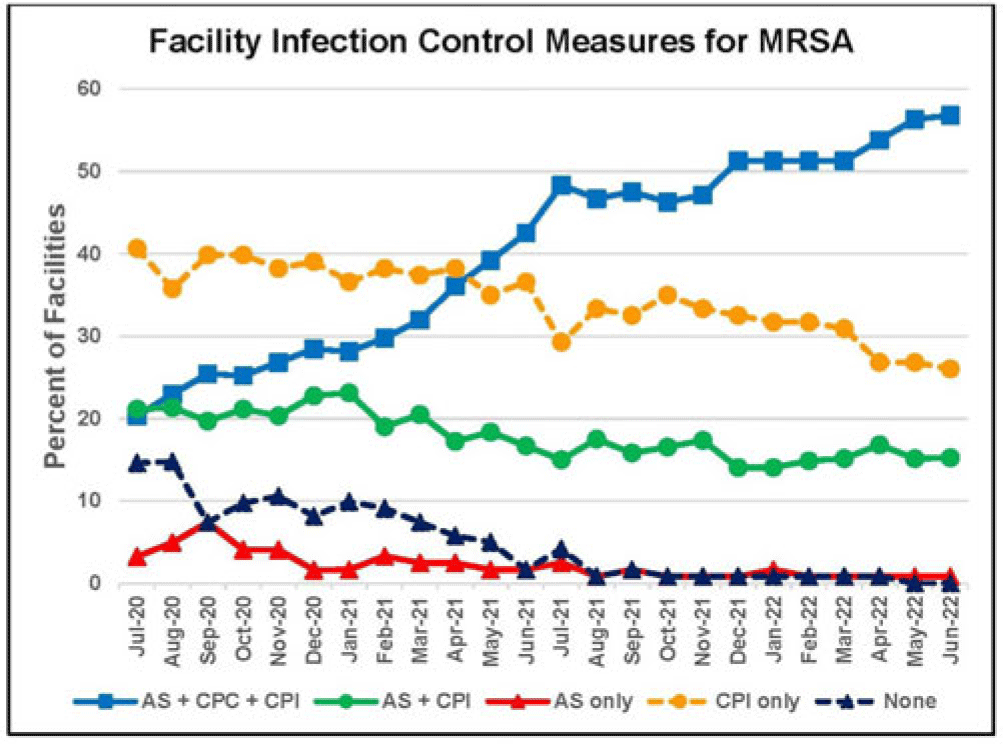
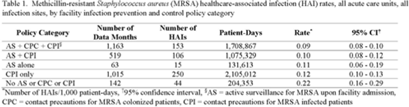
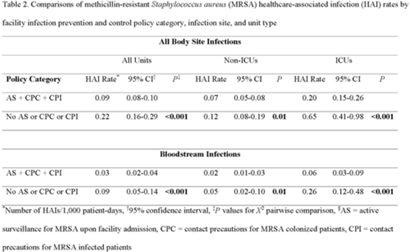
Background: Statistically significant decreases in methicillin-resistant Staphylococcus aureus (MRSA) healthcare-associated infections (HAIs) occurred in Veterans Health Administration (VA) facilities from 2007 to 2019 using active surveillance for facility admissions and contact precautions for patients colonized (CPC) or infected (CPI) with MRSA, but the value of these interventions is controversial. Objective: To determine the impact of active surveillance, CPC, and CPI on prevention MRSA HAIs, we conducted a prospective cohort study between July 2020 and June 2022 in all 123 acute-care VA medical facilities. In April 2020, all facilities were given the option to suspend any combination of active surveillance, CPC, or CPI to free up laboratory resources for COVID-19 testing and conserve personal protective equipment. We measured MRSA HAIs (cases per 1,000 patient days) in intensive care units (ICUs) and non-ICUs by the infection control policy. Results: During the analysis period, there were 917,591 admissions, 5,225,174 patient days, and 568 MRSA HAIs. Only 20% of facilities continued all 3 MRSA infection control measures in July 2020, but this rate increased to 57% by June 2022. The MRSA HAI rate for all infection sites in non-ICUs was 0.07 (95% CI, 0.05–0.08) for facilities practicing active surveillance plus CPC plus CPI compared to 0.12 (95% CI, 0.08–0.19; P = .01) for those not practicing any of these strategies, and in ICUs the MRSA HAI rates were 0.20 (95% CI, 0.15–0.26) and 0.65 (95% CI, 0.41–0.98; P < .001) for the respective policies. Similar differences were seen when the analyses were restricted to MRSA bloodstream HAIs. Accounting for monthly COVID-19 admissions to facilities over the analysis period using a negative binomial regression model did not change the relationships between facility policy and MRSA HAI rates in the ICUs or non-ICUs. There was no statistically significant difference in monthly facility urinary catheter-associated infection rates, a nonequivalent dependent variable, in the categories during the analysis period in either ICUs or non-ICUs. Conclusions: In Veterans Affairs medical centers, there were fewer MRSA HAIs when facilities practiced active surveillance and contact precautions for colonized or infected patients during the COVID-19 pandemic. The effect was greater in ICUs than non-ICUs.
Disclosures: None




Increasing Registration for a VA Multidrug-Resistant Organism Alert Tool
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s124-s125
-
- Article
-
- You have access
- Open access
- Export citation
-
Objectives: To address the importation of multi-drug-resistant organisms (MDROs) when a colonized or infected patient is transferred from another VA facility, the Veterans Health Administration (VHA) launched the Inpatient Pathogen Tracker (IPT) in 2020. IPT tracks MDRO-infected/colonized patients and alerts MDRO Program Coordinators (MPCs) and Infection Preventionists (IPs) when such patients are admitted to their facility to facilitate rapid identification and isolation of infected/colonized patients. IPT usage has been low during initial rollout (32.5%). The VHA and the CARRIAGE QUERI Program developed targeted implementation strategies to increase utilization of IPT’s second iteration, VA Bug Alert (VABA). Methods: Familiarity with IPT was assessed via pre-education survey (3/2022). All sites received standard VABA implementation including: 1) adaptation of VABA features based on end-user feedback (completed 4/2022), 2) development and delivery of an educational module regarding the revised tool (completed 4/2022), and 3) internal facilitation from the VHA MDRO Program Office (ongoing) (see Figure for all key timepoints). Intent to register for VABA was assessed via post-education survey (4-5/2022). Sites (125 eligible) not registered for VABA by 6/1/2022 were randomly assigned to receive one of two conditions from 6/2022–8/2022: continued standard implementation alone or enhanced implementation. Enhanced implementation added the following to standard implementation: 1) audit and feedback reports and 2) external facilitation, including interviews and education about VABA. We compared the number of sites with ≥1 MPC/IP registered for VABA to-date between implementation conditions. Results: Pre-education survey. 168 MPC/IPs across 117 sites responded (94% of eligible sites). Among respondents, 25% had used IPT, 35.1% were familiar with but had not used IPT, and 39.9% were unfamiliar with IPT. Post-education survey. 93 MPC/IPs across 80 sites responded (59% of eligible sites). Of these, 81.7% said they planned to register for VABA, 4.3% said they would not register, and 14.0% said they were unsure. Post-6/1/2022 Registrations. By 6/1/2022, 71% of sites had ≥1 registered VABA user. Of the 28 unregistered sites eligible for enhanced implementation, thirteen were assigned to receive enhanced implementation, and fifteen were assigned to receive continued standard implementation. Eight sites in the enhanced implementation condition (61.5%) registered for VABA. Seven standard-implementation-only sites (46.7%) registered. The number of registered sites did not significantly differ by implementation condition (Fisher’s exact p=0.476). Conclusions: Standard and enhanced implementation were equally effective at encouraging VABA registration, suggesting that allocating resources to enhanced implementation may not be necessary.
Disclosures: None.


Lessons from an evaluation of an antimicrobial resistance laboratory capacity telementoring program in Ethiopia and Kenya
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s123
-
- Article
-
- You have access
- Open access
- Export citation
The development and validation of the Discrimination and Stigma Scale Ultra Short for People Living with Dementia (DISCUS-Dementia)
-
- Journal:
- BJPsych Open / Volume 9 / Issue 5 / September 2023
- Published online by Cambridge University Press:
- 31 August 2023, e164
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Birds in Europe 4: the fourth assessment of Species of European Conservation Concern
-
- Journal:
- Bird Conservation International / Volume 33 / 2023
- Published online by Cambridge University Press:
- 30 June 2023, e66
-
- Article
- Export citation
The role of journals in supporting the socially responsible use of conservation technology
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Chapter 5 - Financing Health Care
- from Section 1 - Analyzing Health Systems: Concepts, Components, Performance
-
-
- Book:
- Making Health Systems Work in Low and Middle Income Countries
- Published online:
- 08 December 2022
- Print publication:
- 29 December 2022, pp 67-82
-
- Chapter
- Export citation
Lack of correlation between standardized antimicrobial administration ratios (SAARs) and healthcare-facility–onset Clostridioides difficile infection rates in Veterans Affairs medical facilities
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 01 December 2022, pp. 945-947
- Print publication:
- June 2023
-
- Article
- Export citation
The Evolutionary Map of the Universe Pilot Survey – ADDENDUM
-
- Journal:
- Publications of the Astronomical Society of Australia / Volume 39 / 2022
- Published online by Cambridge University Press:
- 02 November 2022, e055
-
- Article
- Export citation
Diseconomies of Scale in Quantitative and Fundamental Investment Styles
-
- Journal:
- Journal of Financial and Quantitative Analysis / Volume 58 / Issue 6 / September 2023
- Published online by Cambridge University Press:
- 11 July 2022, pp. 2417-2445
- Print publication:
- September 2023
-
- Article
-
- You have access
- Open access
- Export citation
Increased carbapenemase testing following implementation of national VA guidelines for carbapenem-resistant Enterobacterales (CRE)
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 02 June 2022, e88
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Winter Storms and Unplanned School Closure Announcements on Twitter: Comparison Between the States of Massachusetts and Georgia, 2017–2018
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 17 / 2023
- Published online by Cambridge University Press:
- 11 April 2022, e132
-
- Article
- Export citation
Healthcare-associated infections in Veterans Affairs acute-care and long-term healthcare facilities during the coronavirus disease 2019 (COVID-19) pandemic
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 3 / March 2023
- Published online by Cambridge University Press:
- 05 April 2022, pp. 420-426
- Print publication:
- March 2023
-
- Article
- Export citation
