
135 results
Understanding the role of antibiotic-associated adverse events in influencing antibiotic decision-making
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 30 January 2024, e13
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Understanding clinician perspectives on antibiotic associated adverse events to inform feedback
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s35-s36
-
- Article
-
- You have access
- Open access
- Export citation
-
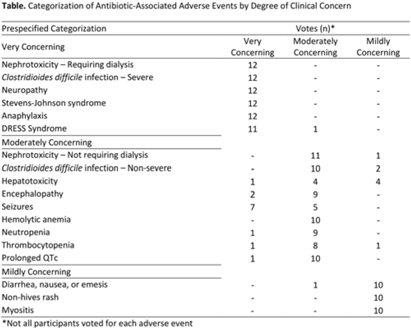
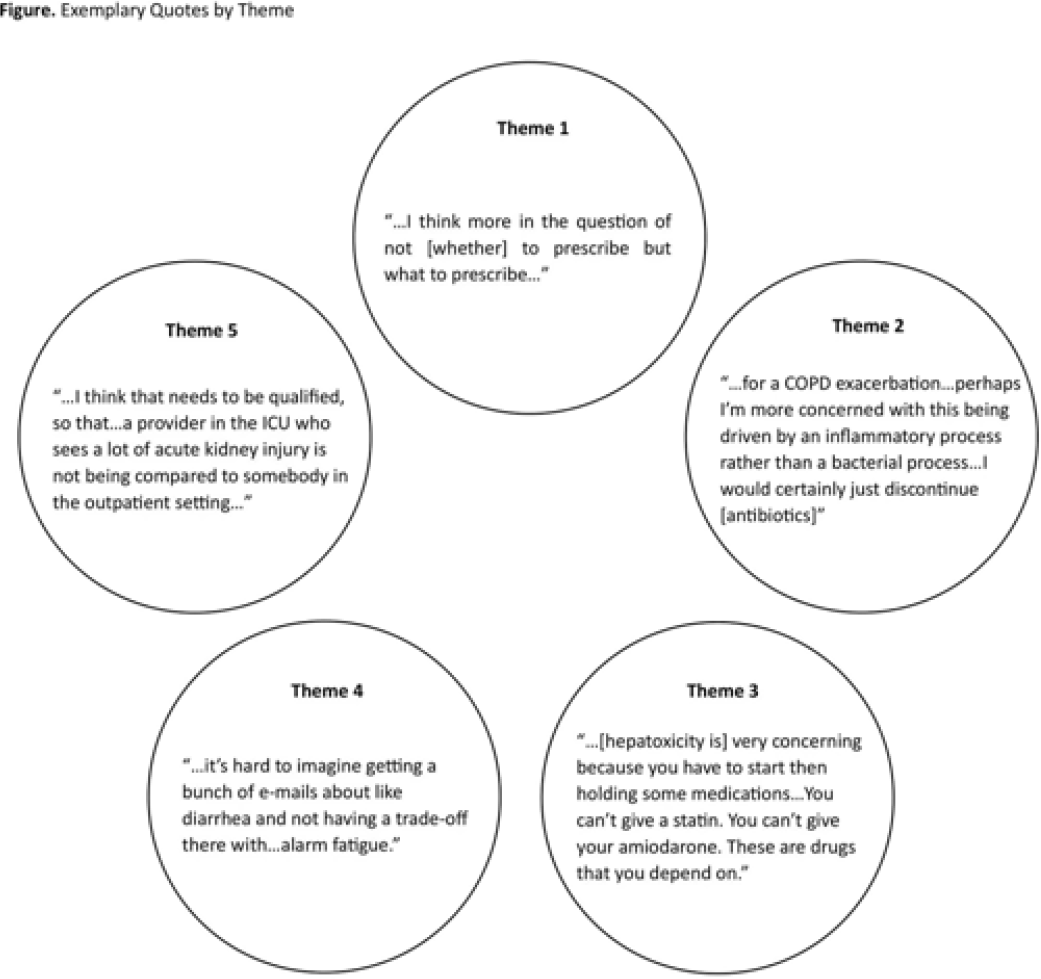
Background: Feedback regarding antibiotic-associated adverse events (ABX-AEs) may assist clinicians with antibiotic decision making. We sought to understand how clinicians account for ABX-AEs when prescribing and their preferences for ABX-AE feedback. Methods: We conducted 1-hour virtual focus groups with 3–5 physicians or advance practice practitioners (APPs) per session at Johns Hopkins Hospital. Participants discussed the role of ABX-AEs in antibiotic decision making and feedback preferences. Participants evaluated prespecified categorization (mildly, moderately, or very concerning) of several ABX-AEs. Focus groups were recorded and transcribed. Transcripts were coded inductively by 2 independent reviewers; discrepancies were resolved by consensus. Codes were used to conduct thematic analysis. Results: Overall, 3 focus groups were conducted with 12 participants: 41.6% were house staff, 16.7% were attending physicians, and 41.6% were APPs. Most were female (91.6%) and were white (41.7%) or Asian (41.7%). Clinicians generally agreed with the prespecified categorizations of ABX-AEs based on degree of clinical concern (Table). We identified 5 themes: (1) The risk of ABX-AE is considered during initial prescribing but influences agent selection more than the decision to prescribe antibiotics. (2) The occurrence of an ABX-AE leads to assessment of need for continued antibiotic therapy. (3) The impact of an ABX-AE on other management decisions is as important as the direct harm of the ABX-AE when assessing severity. (4) Feedback must be curated to prevent clinicians from being overwhelmed with data. (5) Clinicians will be more receptive to feedback regarding ABX-AEs if feedback is contextualized (Fig.). Conclusions: The themes identified and assessment of ABX-AEs of greatest clinical concern may help inform the development of effective ABX-AE feedback methods to improve antibiotic safety.
Disclosures: None


Extension event attendance increases adoption of weed management practices by sports field managers
-
- Journal:
- Weed Technology / Volume 37 / Issue 5 / October 2023
- Published online by Cambridge University Press:
- 20 September 2023, pp. 578-587
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Virtuous opinion change in structured groups
-
- Journal:
- Judgment and Decision Making / Volume 18 / 2023
- Published online by Cambridge University Press:
- 03 August 2023, e25
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Service Evaluation Exploring the Use of Standardised Assessment Tools to Assess Non-Cognitive Symptoms of Dementia
-
- Journal:
- BJPsych Open / Volume 8 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 20 June 2022, p. S144
-
- Article
-
- You have access
- Open access
- Export citation
A community–university run conference as a catalyst for addressing health disparities in an urban community
-
- Journal:
- Journal of Clinical and Translational Science / Volume 6 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 06 May 2022, e67
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Neuropsychological Impairments and Their Cognitive Architecture in Mild Cognitive Impairment (MCI) with Lewy Bodies and MCI-Alzheimer’s Disease
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 28 / Issue 9 / October 2022
- Published online by Cambridge University Press:
- 20 October 2021, pp. 963-973
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Empathic communication in dignity therapy: Feasibility of measurement and descriptive findings
-
- Journal:
- Palliative & Supportive Care / Volume 20 / Issue 3 / June 2022
- Published online by Cambridge University Press:
- 19 October 2021, pp. 321-327
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Advances in Momentum Resolved EELS
-
- Journal:
- Microscopy and Microanalysis / Volume 27 / Issue S1 / August 2021
- Published online by Cambridge University Press:
- 30 July 2021, pp. 136-138
- Print publication:
- August 2021
-
- Article
-
- You have access
- Export citation
Integrating primary care and public health to enhance response to a pandemic
-
- Journal:
- Primary Health Care Research & Development / Volume 22 / 2021
- Published online by Cambridge University Press:
- 10 June 2021, e27
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Hospital-acquired infections among adult patients admitted for coronavirus disease 2019 (COVID-19)
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 8 / August 2022
- Published online by Cambridge University Press:
- 13 April 2021, pp. 1054-1057
- Print publication:
- August 2022
-
- Article
- Export citation
N95 filtering face piece respirators remain effective after extensive reuse during the coronavirus disease 2019 (COVID-19) pandemic
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 42 / Issue 7 / July 2021
- Published online by Cambridge University Press:
- 19 February 2021, pp. 896-899
- Print publication:
- July 2021
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Accuracy of dopaminergic imaging as a biomarker for mild cognitive impairment with Lewy bodies
-
- Journal:
- The British Journal of Psychiatry / Volume 218 / Issue 5 / May 2021
- Published online by Cambridge University Press:
- 23 December 2020, pp. 276-282
- Print publication:
- May 2021
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Ultra-high Energy Resolution EELS
-
- Journal:
- Microscopy and Microanalysis / Volume 26 / Issue S2 / August 2020
- Published online by Cambridge University Press:
- 30 July 2020, pp. 1804-1805
- Print publication:
- August 2020
-
- Article
-
- You have access
- Export citation
Implementation of the Navajo fruit and vegetable prescription programme to improve access to healthy foods in a rural food desert
-
- Journal:
- Public Health Nutrition / Volume 23 / Issue 12 / August 2020
- Published online by Cambridge University Press:
- 13 May 2020, pp. 2199-2210
-
- Article
-
- You have access
- HTML
- Export citation
Evidence for causal effects of lifetime smoking on risk for depression and schizophrenia: a Mendelian randomisation study
-
- Journal:
- Psychological Medicine / Volume 50 / Issue 14 / October 2020
- Published online by Cambridge University Press:
- 06 November 2019, pp. 2435-2443
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Chemical, Biological, Radiological, Nuclear, and Explosive (CBRNE) Science and the CBRNE Science Medical Operations Science Support Expert (CMOSSE)
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 13 / Issue 5-6 / December 2019
- Published online by Cambridge University Press:
- 17 June 2019, pp. 995-1010
-
- Article
- Export citation
8 - Melodramatic Acting
- from II - Melodramatic Technique
-
-
- Book:
- The Cambridge Companion to English Melodrama
- Published online:
- 06 October 2018
- Print publication:
- 04 October 2018, pp 112-125
-
- Chapter
- Export citation
Prehospital Airway Management Examined at Two Pediatric Emergency Centers
-
- Journal:
- Prehospital and Disaster Medicine / Volume 33 / Issue 5 / October 2018
- Published online by Cambridge University Press:
- 31 October 2018, pp. 532-538
- Print publication:
- October 2018
-
- Article
- Export citation
Diagnostic accuracy of dopaminergic imaging in prodromal dementia with Lewy bodies
-
- Journal:
- Psychological Medicine / Volume 49 / Issue 3 / February 2019
- Published online by Cambridge University Press:
- 25 April 2018, pp. 396-402
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
