
518 results
Concurrent transmission of multiple carbapenemases in a long-term acute-care hospital
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 3 / March 2024
- Published online by Cambridge University Press:
- 10 January 2024, pp. 292-301
- Print publication:
- March 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
6 Pulse Pressure and APOE ε4 Dose Interact to Affect Cerebral Blood Flow in Older Adults Without Dementia
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 107-108
-
- Article
-
- You have access
- Export citation
17 Education Moderates the Association Between Hippocampal CBF and Memory in Women but Not Men
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 227-228
-
- Article
-
- You have access
- Export citation
Ten New Insights in Climate Science 2023/2024
-
- Journal:
- Global Sustainability / Accepted manuscript
- Published online by Cambridge University Press:
- 01 December 2023, pp. 1-58
-
- Article
-
- You have access
- Open access
- Export citation
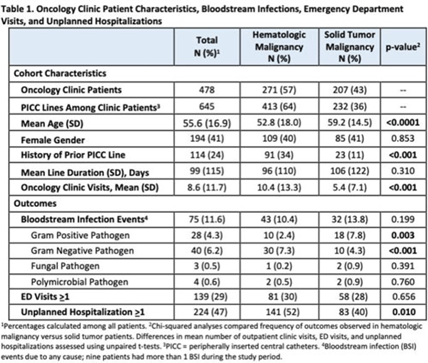
Bloodstream infection burden among cancer clinic patients with PICC Lines: A prospective, observational study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s49
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Oncology patients are at high risk for bloodstream infection (BSI) due to immunosuppression and frequent use of central venous catheters. Surveillance in this population is largely relegated to inpatient settings and limited data are available describing community burden. We evaluated rates of BSI, clinic or emergency department (ED) visits, and hospitalizations in a large cohort of oncology outpatients with peripherally inserted central catheters (PICCs). Methods: In this prospective, observational study, we followed a convenience sample of adults (age>18) with PICCs at a large academic outpatient oncology clinic for 35 months between July 2015 and November 2018. We assessed demographics, malignancy type, PICC insertion and removal dates, history of prior PICC, and line duration. Outcomes included BSI events (defined as >1 positive blood cultures or >2 positive blood cultures if coagulase-negative Staphylococcus), ED visits (without hospitalization), and unplanned hospitalizations (excluding scheduled chemotherapy hospitalizations). We used χ2 analyses to compare the frequency of categorical outcomes, and we used unpaired t tests to assess differences in means of continuous variable in hematologic versus solid-tumor malignancy patients. We used generalized linear mixed-effects models to assess differences in BSI (clustered by patient) separately for gram-positive and gram-negative BSI outcomes. Results: Among 478 patients with 658 unique PICC lines and 64,190 line days, 271 patients (413 lines) had hematologic malignancy and 207 patients (232 lines) had solid-tumor malignancy. Cohort characteristics and outcomes stratified by malignancy type are shown in Table 1. Compared to those with hematologic malignancy, solid-tumor patients were older, had 47% fewer clinic visits, and had 32% lower frequency of prior PICC lines. Overall, there were 75 BSI events (12%; 1.2 per 1,000 catheter days). We detected no significant difference in BSI rates when comparing solid-tumor versus hematologic malignancies (P = 0.20); BSIs with gram-positive pathogen were 69% higher in patients with solid tumors. Gram-negative BSIs were 41% higher in patients with hematologic malignancy. Solid-tumor malignancy was associated with 4.5-fold higher odds of developing BSI with gram-positive pathogen (OR, 4.48; 95% CI, 1.60–12.60; P = .005) compared to those with hematologic malignancy, after adjusting for age, sex, history of prior PICC, and line duration. Differences in gram-negative BSI were not significant on multivariate analysis. Conclusions: The burden of all-cause BSIs in cancer clinic adults with PICC lines was 12% or 1.2 per 1,000 catheter days, as high as nationally reported inpatient BSI rates. Higher risk of gram-positive BSIs in solid-tumor patients suggests the need for targeted infection prevention activities in this population, such as improvements in central-line monitoring, outpatient care, and maintenance of lines and/or dressings, as well as chlorhexidine bathing to reduce skin bioburden.
Disclosures: None

Kilowatt-class high-energy frequency conversion to 95 J at 10 Hz at 515 nm
- Part of
-
- Journal:
- High Power Laser Science and Engineering / Volume 11 / 2023
- Published online by Cambridge University Press:
- 27 July 2023, e65
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Point of care assay for blood aripiprazole concentrations: development, validation and utility
-
- Journal:
- The British Journal of Psychiatry / Volume 223 / Issue 2 / August 2023
- Published online by Cambridge University Press:
- 31 May 2023, pp. 389-393
- Print publication:
- August 2023
-
- Article
- Export citation
Within-person pathways among maternal depressive symptoms and offspring internalizing problems from early childhood through adolescence
-
- Journal:
- Development and Psychopathology , First View
- Published online by Cambridge University Press:
- 15 May 2023, pp. 1-9
-
- Article
- Export citation
153 Adapting Motivational Interviewing for Vaccine Hesitancy in Underserved Communities
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue s1 / April 2023
- Published online by Cambridge University Press:
- 24 April 2023, p. 47
-
- Article
-
- You have access
- Open access
- Export citation
Traditional definition of healthcare-associated influenza underestimates cases associated with other healthcare exposures in a population-based surveillance system
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 11 / November 2023
- Published online by Cambridge University Press:
- 19 April 2023, pp. 1816-1822
- Print publication:
- November 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Transporting monovalent rotavirus vaccine efficacy estimates to an external target population: a secondary analysis of data from a randomised controlled trial in Malawi
-
- Journal:
- Epidemiology & Infection / Volume 151 / 2023
- Published online by Cambridge University Press:
- 27 February 2023, e49
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
PP57 Collaborating In Times Of COVID: The Launch Of The National Wales COVID-19 Evidence Centre
-
- Journal:
- International Journal of Technology Assessment in Health Care / Volume 38 / Issue S1 / December 2022
- Published online by Cambridge University Press:
- 23 December 2022, p. S59
-
- Article
-
- You have access
- Export citation
PP150 The Role Of Expert Consensus In UK Guidance: Patient Selection For Hydrogel Spacer Use During Prostate Cancer Radiotherapy
-
- Journal:
- International Journal of Technology Assessment in Health Care / Volume 38 / Issue S1 / December 2022
- Published online by Cambridge University Press:
- 23 December 2022, pp. S88-S89
-
- Article
-
- You have access
- Export citation
Response of quizalofop-resistant rice to sequential quizalofop applications under differential environmental conditions
-
- Journal:
- Weed Technology / Volume 36 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 15 December 2022, pp. 789-799
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Using a multicultural and multilingual awareness-raising strategy to enhance enrollment of racially underrepresented minoritized communities – the PassITON trial
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 07 December 2022, e9
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Prescribing for different antibiotic classes across age groups in the Kaiser Permanente Northern California population in association with influenza incidence, 2010–2018
-
- Journal:
- Epidemiology & Infection / Volume 150 / 2022
- Published online by Cambridge University Press:
- 26 October 2022, e180
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Quizalofop-resistant rice response to quizalofop when exposed to low rates of glyphosate and imazethapyr
-
- Journal:
- Weed Technology / Volume 36 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 20 September 2022, pp. 800-807
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Cognitive dispersion is elevated in amyloid-positive older adults and associated with regional hypoperfusion
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue 7 / August 2023
- Published online by Cambridge University Press:
- 12 September 2022, pp. 621-631
-
- Article
- Export citation
Quantitative and Qualitative Correlation of CL and X-ray Signals in Cr-bearing Jade from Chichén-Itzá Archaeological Zone, Mexico
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 656-660
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Benzobicyclon for weedy rice control in quizalofop- and imidazolinone-resistant rice systems
-
- Journal:
- Weed Technology / Volume 36 / Issue 4 / August 2022
- Published online by Cambridge University Press:
- 27 June 2022, pp. 497-505
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
