
702 results
D.1 Efficacy, safety, and tolerability of subcutaneous efgartigimod in chronic inflammatory demyelinating polyneuropathy: results from the ADHERE trial
-
- Journal:
- Canadian Journal of Neurological Sciences / Volume 51 / Issue s1 / June 2024
- Published online by Cambridge University Press:
- 24 May 2024, pp. S8-S9
-
- Article
-
- You have access
- Export citation
B.6 Long-term risk of subsequent stroke after transient ischemic attack or minor stroke: a systematic review and meta-analysis
-
- Journal:
- Canadian Journal of Neurological Sciences / Volume 51 / Issue s1 / June 2024
- Published online by Cambridge University Press:
- 24 May 2024, p. S6
-
- Article
-
- You have access
- Export citation
Head and Neck Cancer: United Kingdom National Multidisciplinary Guidelines, Sixth Edition
-
- Journal:
- The Journal of Laryngology & Otology / Volume 138 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 14 March 2024, pp. S1-S224
- Print publication:
- April 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Efficacy and safety of transcranial magnetic stimulation on cognition in mild cognitive impairment, Alzheimer’s disease, Alzheimer’s disease-related dementias, and other cognitive disorders: a systematic review and meta-analysis
-
- Journal:
- International Psychogeriatrics , First View
- Published online by Cambridge University Press:
- 08 February 2024, pp. 1-49
-
- Article
- Export citation
4 Evaluating Plasma GFAP for the Detection of Alzheimer’s Disease Dementia
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 408-409
-
- Article
-
- You have access
- Export citation
4 Risk Factor and Biomarker Correlates of FLAIR White Matter Hyperintensities in Former American Football Players
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 608-610
-
- Article
-
- You have access
- Export citation
2 Higher White Matter Hyperintensity Load Adversely Affects Pre-Post Proximal Cognitive Training Performance in Healthy Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 671-672
-
- Article
-
- You have access
- Export citation
5 Antemortem Plasma GFAP Predicts Alzheimer’s Disease Neuropathological Changes
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 409-410
-
- Article
-
- You have access
- Export citation
9 Connecting memory and functional brain networks in older adults: a resting state fMRI study
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 527-528
-
- Article
-
- You have access
- Export citation
The Mopra Southern Galactic Plane CO Survey – data release 4– complete survey
-
- Journal:
- Publications of the Astronomical Society of Australia / Volume 40 / 2023
- Published online by Cambridge University Press:
- 22 August 2023, e047
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
We present observations of the Mopra carbon monoxide (CO) survey of the Southern Galactic Plane, covering Galactic longitudes spanning
 $l = 250^{\circ}$ (
$l = 250^{\circ}$ ( $-110^{\circ}$) to
$-110^{\circ}$) to  $l = 355^{\circ}$ (
$l = 355^{\circ}$ ( $-5^{\circ}$), with a latitudinal coverage of at least
$-5^{\circ}$), with a latitudinal coverage of at least  $|b|<1^\circ$, totalling an area of
$|b|<1^\circ$, totalling an area of  $>$210 deg
$>$210 deg $^{2}$. These data have been taken at 0.6 arcmin spatial resolution and 0.1 km s
$^{2}$. These data have been taken at 0.6 arcmin spatial resolution and 0.1 km s $^{-1}$ spectral resolution, providing an unprecedented view of the molecular gas clouds of the Southern Galactic Plane in the 109–115 GHz
$^{-1}$ spectral resolution, providing an unprecedented view of the molecular gas clouds of the Southern Galactic Plane in the 109–115 GHz  $J = 1-0$ transitions of
$J = 1-0$ transitions of  $^{12}$CO,
$^{12}$CO,  $^{13}$CO, C
$^{13}$CO, C $^{18}$O, and C
$^{18}$O, and C $^{17}$O.
$^{17}$O.













Agricultural Research Service Weed Science Research: Past, Present, and Future
-
- Journal:
- Weed Science / Volume 71 / Issue 4 / July 2023
- Published online by Cambridge University Press:
- 16 August 2023, pp. 312-327
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Translation and validation of Greek version of the Pandemic Grief Scale
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S474
-
- Article
-
- You have access
- Open access
- Export citation
The Role of Social Defeat in Neurological differences in Psychotic Patients
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S183
-
- Article
-
- You have access
- Open access
- Export citation
Prevalence of mental health effects among healthcare professionals during the COVID-19 pandemic
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S543-S544
-
- Article
-
- You have access
- Open access
- Export citation
Antiviral and Anti-Inflammatory Activities of Fluoxetine in a SARS-CoV-2 Infection Mouse Model
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S119-S120
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
The coronavirus disease 2019 (COVID-19) pandemic continues to cause significant morbidity and mortality worldwide. Since a large portion of the world’s population is currently unvaccinated or incompletely vaccinated and has limited access to approved treatments against COVID-19, there is an urgent need to continue research on treatment options, especially those at low cost and which are immediately available to patients, particularly in low- and middle-income countries. Prior in vitro and observational studies have shown that fluoxetine, possibly through its inhibitory effect on the acid sphingomyelinase/ceramide system, could be a promising antiviral and anti-inflammatory treatment against COVID-19.
ObjectivesThe aim of this sudy was to test the potential antiviral and anti-inflammatory activities of fluoxetine against SARS-CoV-2 in a K18-hACE2 mouse model of infection, and against several variants of concern in vitro, and test the hypothesis of the implication of ceramides and/or their derivatives hexosylceramides.
MethodsWe evaluated the potential antiviral and anti-inflammatory activities of fluoxetine in a K18-hACE2 mouse model of SARS-CoV-2 infection, and against variants of concern in vitro, i.e., SARS-CoV-2 ancestral strain, Alpha B.1.1.7, Gamma P1, Delta B1.617 and Omicron BA.5.
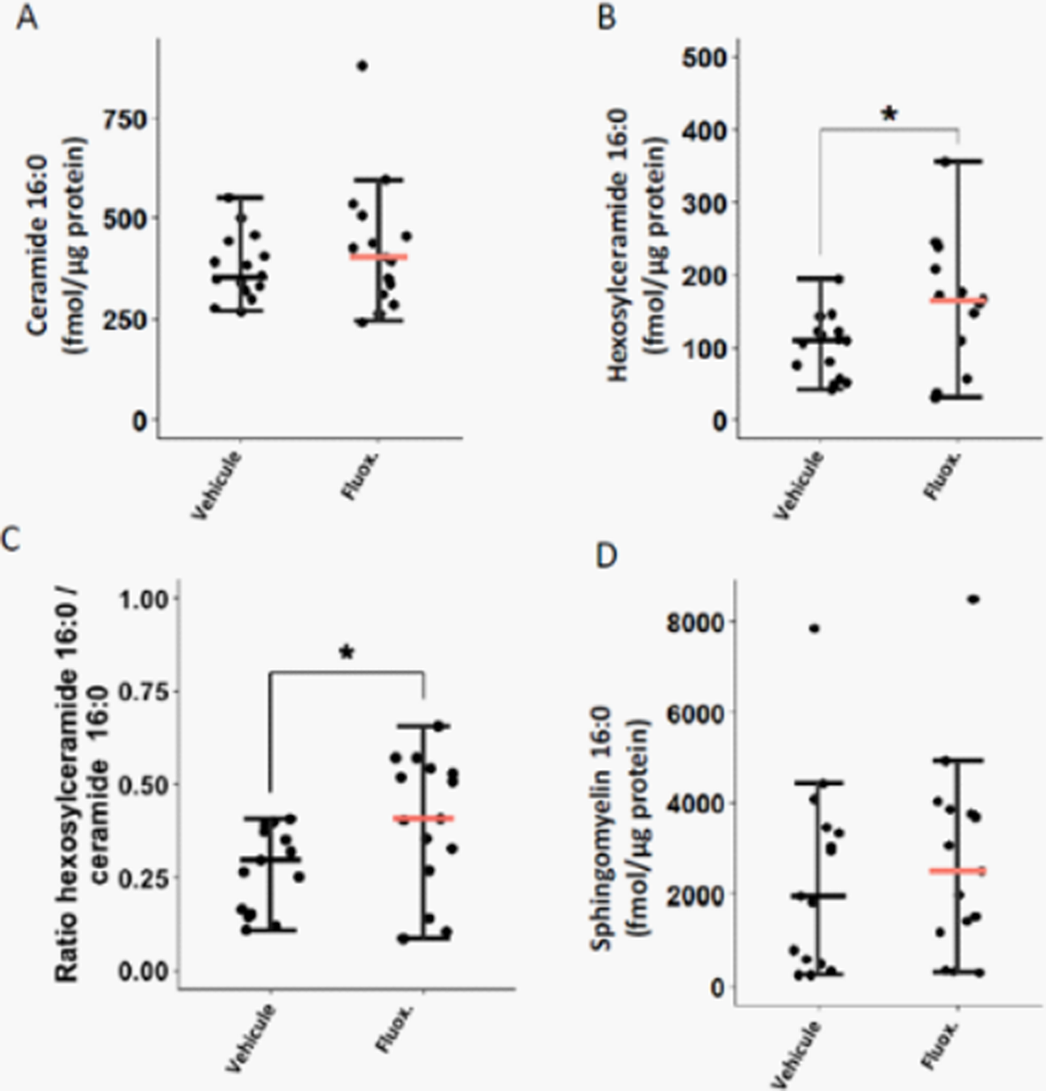
ResultsFluoxetine, administrated after SARS-CoV-2 infection, significantly reduced lung tissue viral titres (Figure 1) and expression of several inflammatory markers (i.e., IL-6, TNFα, CCL2 and CXCL10) (Figure 2). It also inhibited the replication of all variants of concern in vitro. A modulation of the ceramide system in the lung tissues, as reflected by the increase in the ratio HexCer 16:0/Cer 16:0 in fluoxetine-treated mice, may contribute to explain these effects (Figure 3).
Image:
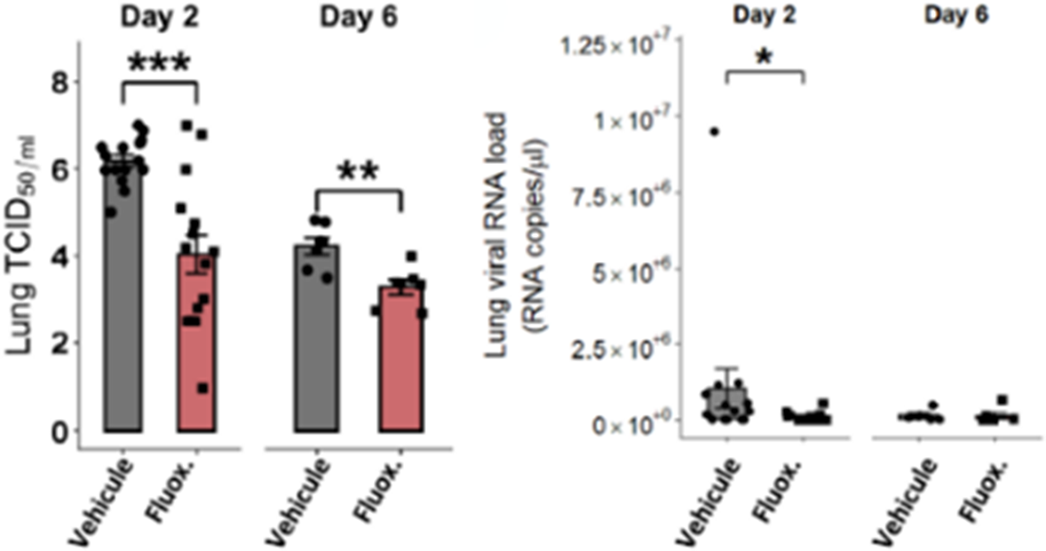
Image 2:
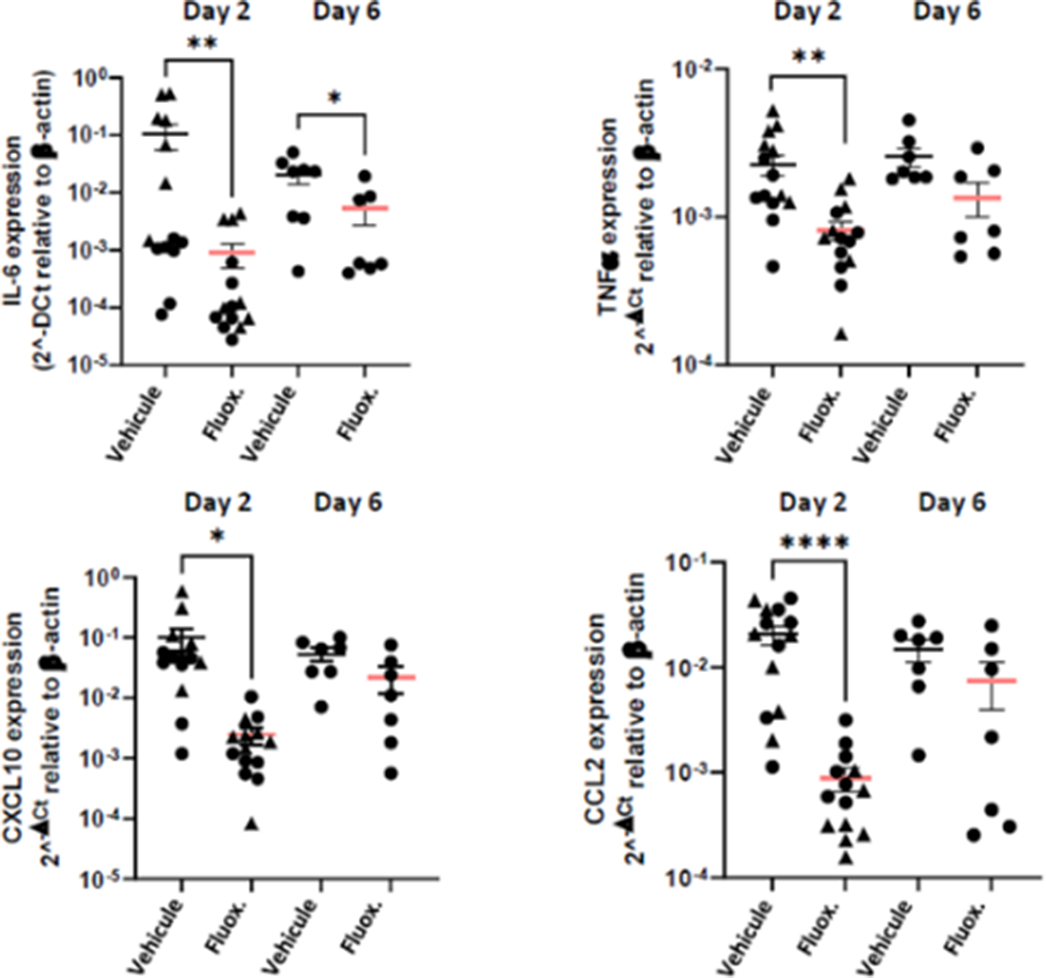
Image 3:
 Conclusions
ConclusionsOur findings demonstrate the antiviral and anti-inflammatory properties of fluoxetine in a K18-hACE2 mouse model of SARS-CoV-2 infection, and its in vitro antiviral activity against variants of concern, establishing fluoxetine as a very promising candidate for the prevention and treatment of SARS-CoV-2 infection and disease pathogenesis.
Disclosure of InterestNone Declared



Changing trends of suicide mortality from 2011 to 2019: an analysis of 38 European Countries
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S85-S86
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Suicide is a serious public health problem since it accounts for nearly 900,000 deaths each year worldwide. Globally in 2019, 10.7 persons out of 100,000 died by suicide. Psychiatric disorders are related to an overwhelming proportion of these cases. In the last years, several specific interventions and action plans for suicide prevention have been implemented in a number of European countries.
ObjectivesOur aim was to analyze recent epidemiologic trends of suicide mortality rates in Europe.
MethodsAnnual national statistics of suicide mortality rates derived from Eurostat public databases from 2011 to 2019 were analyzed for 38 European countries. The suicide mortality rate was estimated per year/100,000 population. Linear regression models were used to study temporal trends of suicidal mortality. Analyses were performed using RStudio.
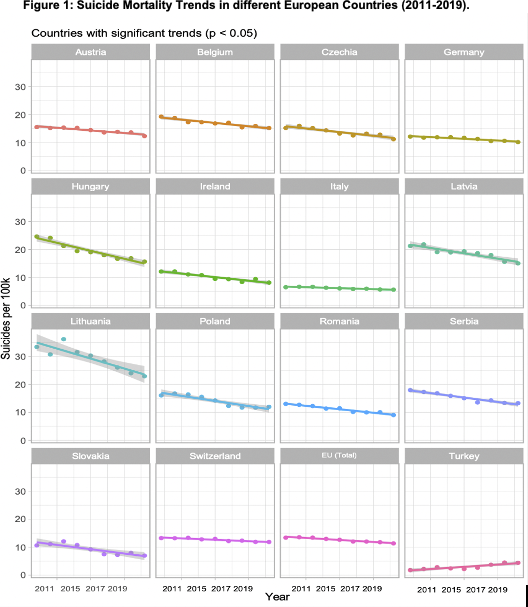
ResultsAvailable data show a statistically significant reduction in suicide mortality rates from 2011 to 2019 in 15 European countries, and a significant increase for Turkey (ES=0.32, SD=0.06, p=0.037) (Fig 1). The greatest significant decrease was reported in Lithuania (ES=-1.42, SD=0.02, p=0.02), followed by Hungary (ES=-1.13, SD=0.11, p=0.0007), Latvia (ES=-0.76, SD=0.11, p=0.007), and Poland (ES=-0.73, SD=0.10, p=0.001). Italy reported the lowest significant reduction in suicide mortality rates (ES=-0.13, SD=0.018, p=0.003). The remaining 16 countries showed no significant changes in suicide mortality trends.
Image:
 Conclusions
ConclusionsIn the last years, Europe registered an overall reduction in reported suicide rates. However, more recent data (i.e., suicide rates after COVID-19 pandemic, age and sex-related effect on suicide rates) should be analyzed and used to implement future recommendations. Current and future suicide prevention strategies aim to contribute to a greater reduction of suicide rates in the different European countries.
Disclosure of InterestNone Declared

Characteristics of Adults Hospitalized for a Major Depressive Disorder: Results from the Multicenter OASIS-D Study
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S346-S347
-
- Article
-
- You have access
- Open access
- Export citation
Antidepressant Use and Its Association with 28-Day Mortality in Inpatients with SARS-CoV-2: Support for the FIASMA Model against COVID-19
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S118-S119
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
To reduce Coronavirus Disease 2019 (COVID-19)-related mortality and morbidity, widely available oral COVID-19 treatments are urgently needed. Certain antidepressants, such as fluvoxamine or fluoxetine, may be beneficial against COVID-19.
ObjectivesThe main objective was two-fold: (i) to test the hypothesis that the prevalence of antidepressant use in patients hospitalized with COVID-19 would be lower than in patients with similar characteristics hospitalized without COVID-19, and (ii) to examine, among patients hospitalized with COVID-19, whether antidepressant use is associated with reduced 28-day mortality. Our secondary aim was to examine whether this potential association could only concern specific antidepressant classes or molecules, is dose-dependent, and/or only observed beyond a certain dose threshold.
MethodsWe included 388,945 adult inpatients who tested positive for SARS-CoV-2 at 36 AP–HP (Assistance Publique–Hôpitaux de Paris) hospitals from 2 May 2020 to 2 November 2021. We compared the prevalence of antidepressant use at admission in a 1:1 ratio matched analytic sample with and without COVID-19 (N = 82,586), and assessed its association with 28-day all-cause mortality in a 1:1 ratio matched analytic sample of COVID-19 inpatients with and without antidepressant use at admission (N = 1482) (Figure 1).
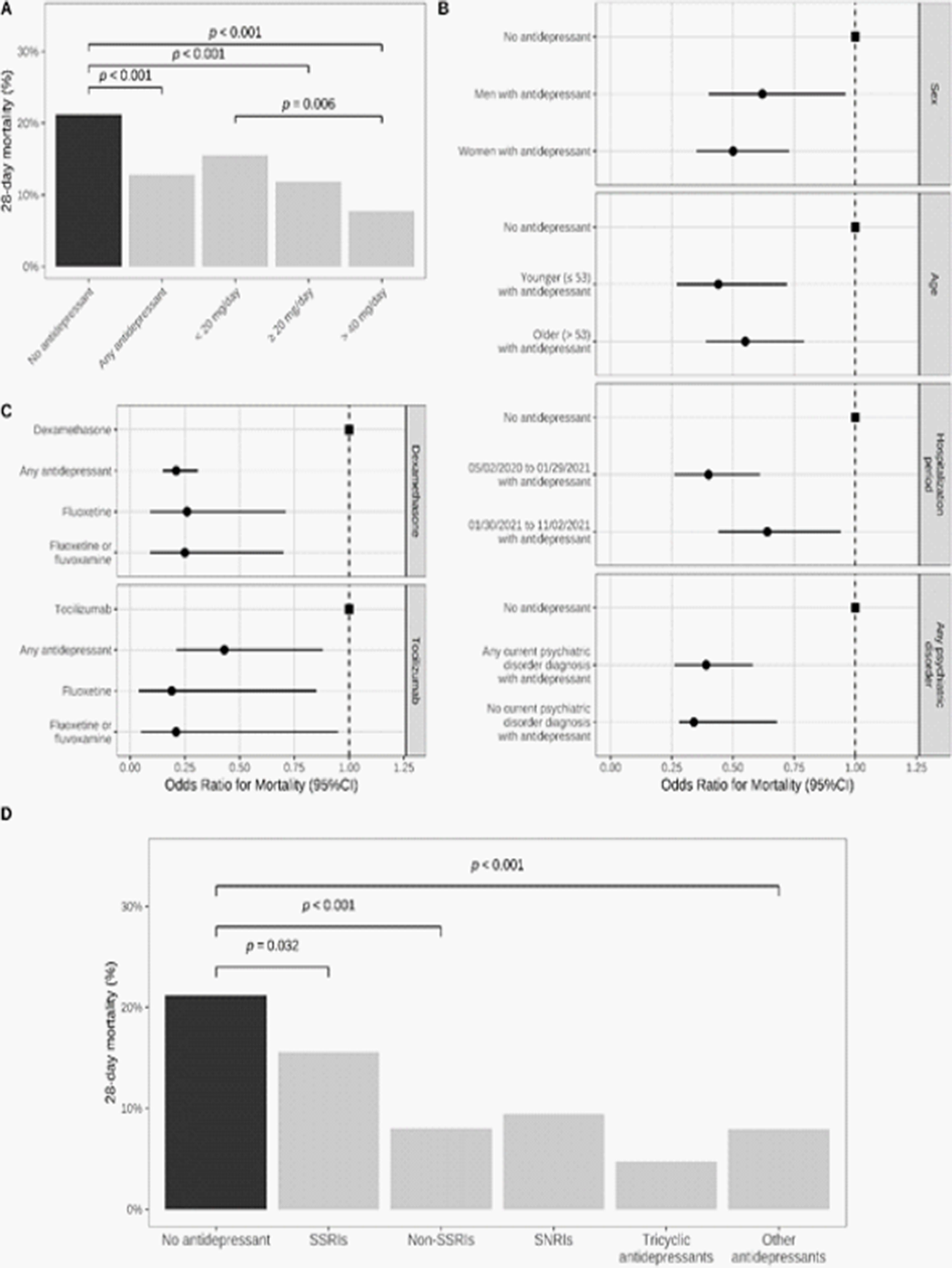
ResultsAntidepressant use was significantly less prevalent in inpatients with COVID-19 than in a matched control group of inpatients without COVID-19 (1.9% versus 4.8%; Odds Ratio (OR) = 0.38; 95%CI = 0.35–0.41, p < 0.001) (Figure 2). Antidepressant use was significantly associated with reduced 28-day mortality among COVID-19 inpatients (12.8% versus 21.2%; OR = 0.55; 95%CI = 0.41–0.72, p < 0.001), particularly at daily doses of at least 40 mg fluoxetine equivalents (Figure 3). Antidepressants with high FIASMA (Functional Inhibitors of Acid Sphingomyelinase) activity seem to drive both associations.
Image:
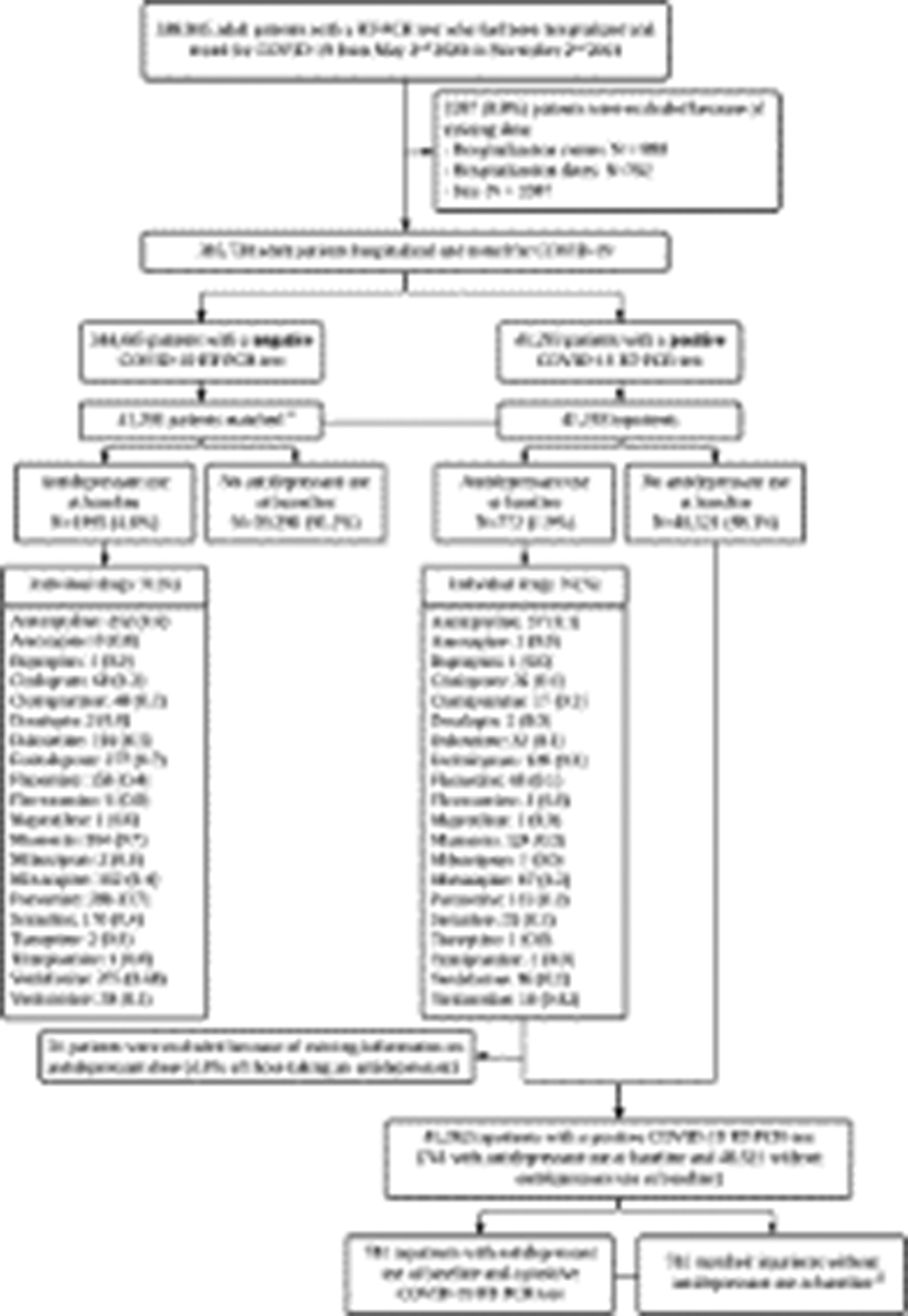
Image 2:
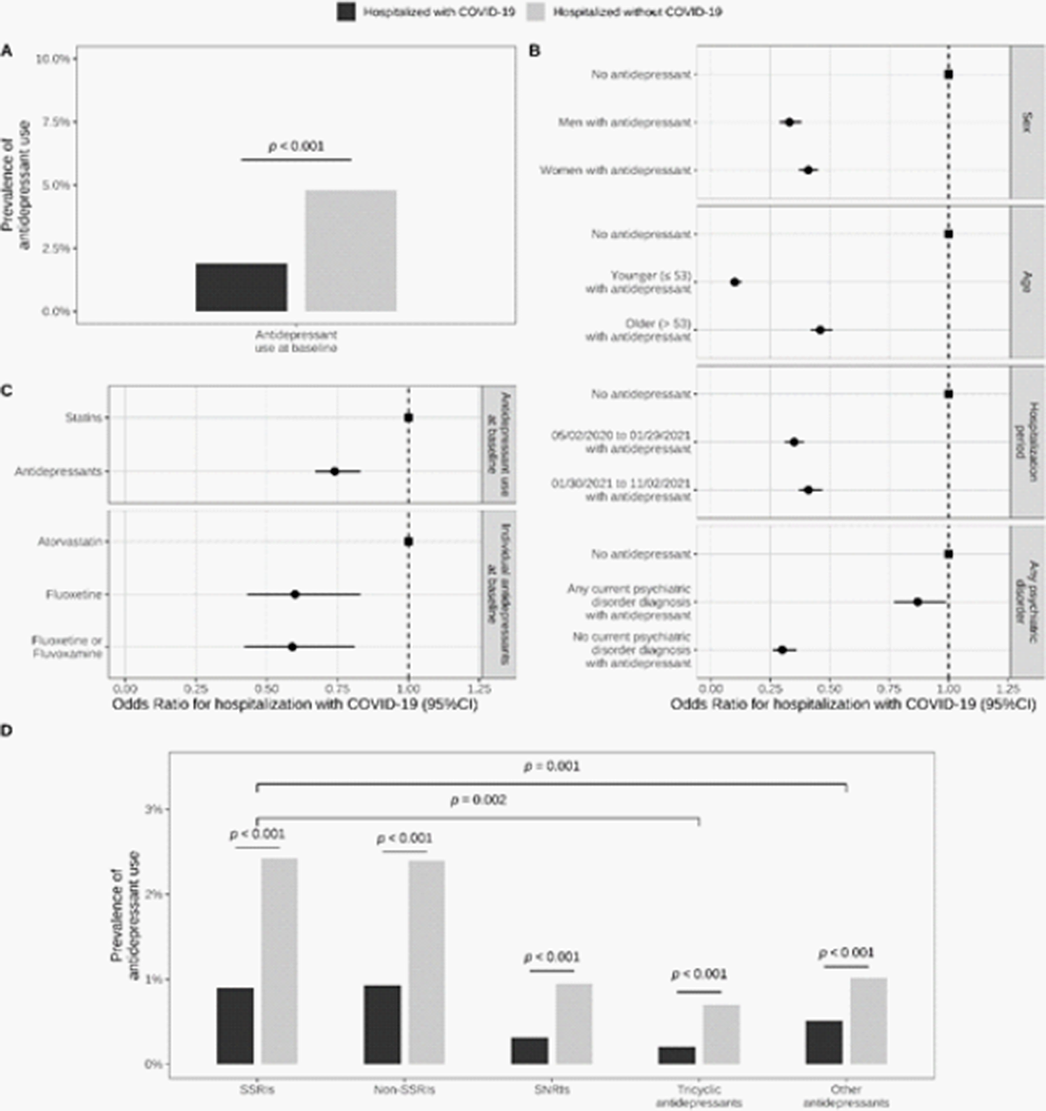
Image 3:
 Conclusions
ConclusionsAntidepressant use is associated with a reduced likelihood of hospitalization in patients infected with SARS-CoV-2 and with a reduced risk of death in patients hospitalized with COVID-19. These associations were stronger for molecules with high FIASMA activity. These findings posit that prospective interventional studies of antidepressants with the highest FIASMA activity may be appropriate to help identify variant-agnostic, affordable, and scalable interventions for outpatient and inpatient therapy of COVID-19.
Disclosure of InterestNone Declared



A real-world data analysis of Clinical Global Impression-Severity (CGI-S) as a transdiagnostic predictor of psychiatric hospitalisation
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S619-S620
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Preventing psychiatric admissions holds benefits for patients as well as healthcare systems. The Clinical Global Impression-Severity (CGI-S) scale is a 7-point measurement of symptom severity, independent of diagnosis, which has shown capability of predicting risk of hospitalisation in schizophrenia. Due to its routine use in clinical practice and ease of administration, it may have potential as a transdiagnostic predictor of hospitalisation.
ObjectivesTo investigate whether early trajectories of CGI-S scores predict risk of hospitalisation over a 6 month-follow-up period.
MethodsA retrospective cohort study was conducted, analysing Electronic Health Record (EHR) data from the NeuroBlu Database (Patel et al. BMJ Open 2022;12:e057227). Patients were included if they had a psychiatric diagnosis and at least 5 recorded CGI-S scores within a 2-month period, defined as the ‘index’ period. The relationship between early CGI-S trajectories and risk of hospitalisation was investigated using Cox regression. The analysis was adjusted for age, gender, race, number of years in education, and psychiatric diagnosis. Early CGI-S trajectories were estimated as clinical severity (defined as the mean CGI-S score during the index period) and clinical instability (defined as a generalised Root Mean Squared Subsequent Differences of all CGI-S scores recorded during the index period). The primary outcome was time to psychiatric hospitalisation up to 6 months following the index period. Patients who had been hospitalised before or within the index period were excluded.
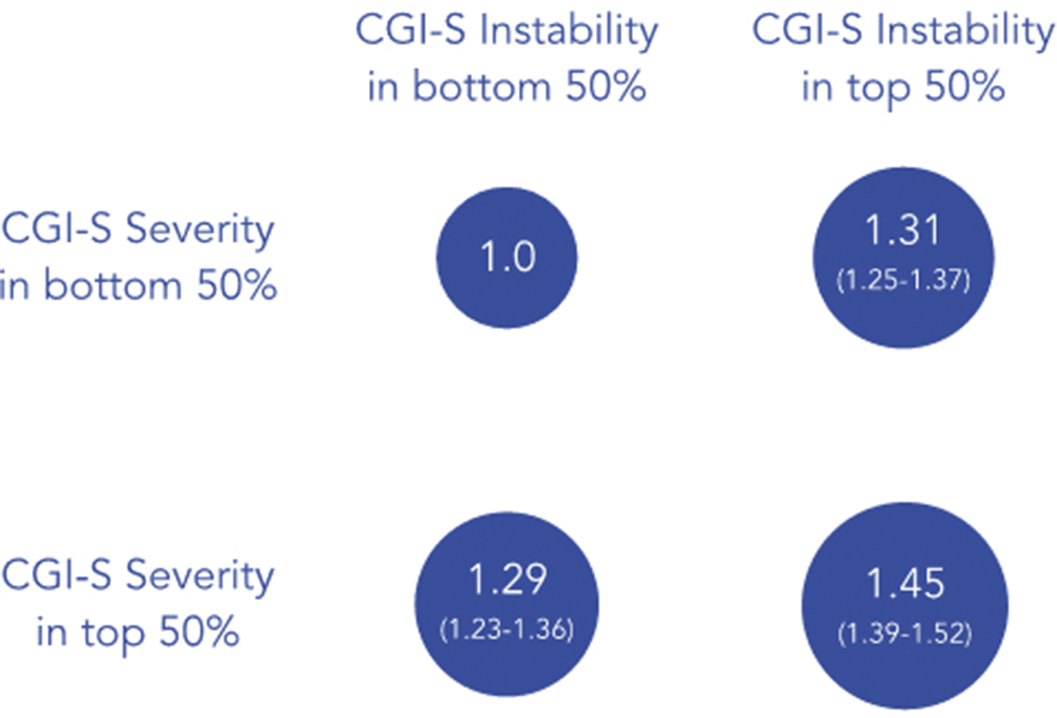
ResultsA total of 36,914 patients were included (mean [SD] age: 29.7 [17.5] years; 57.3% female). Clinical instability (hazard ratio: 1.09, 95% CI 1.07-1.10, p<0.001) and severity (hazard ratio: 1.11, 95% CI 1.09-1.12, p<0.001) independently predicted risk of hospitalisation. These associations were consistent across all psychiatric diagnoses. Patients in the top 50% of severity and/or instability were at a 45% increased risk of hospitalisation compared to those in the bottom 50% (Figure 1).
Image:
 Conclusions
ConclusionsEarly CGI-S trajectories reflecting clinical severity and instability independently predict risk of hospitalisation across diagnoses. This risk was compounded when instability and severity were present together. These results have translation potential in predicting individuals who are at high risk of hospitalisation and could benefit from preventative strategies to mitigate this risk.
Disclosure of InterestE. Palmer Employee of: Holmusk, M. Taquet Consultant of: Holmusk, K. Griffiths Employee of: Holmusk, S. Ker Employee of: Holmusk, C. Liman Employee of: Holmusk, S. N. Wee Employee of: Holmusk, S. Kollins Employee of: Holmusk, R. Patel Grant / Research support from: National Institute of Health Research (NIHR301690); Medical Research Council (MR/S003118/1); Academy of Medical Sciences (SGL015/1020); Janssen, Employee of: Holmusk

Exploring Decision-Making Strategies in the IOWA Gambling Task and Rat Gambling Task
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S106-S107
-
- Article
-
- You have access
- Open access
- Export citation
