
1529 results
Lockean Liberalism in International Relations
-
- Published online:
- 13 March 2024
- Print publication:
- 04 April 2024
-
- Element
- Export citation
Provider-ordered viral testing and antibiotic administration practices among children with acute respiratory infections across healthcare settings in Nashville, Tennessee
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 06 March 2024, e29
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Development of a mentor training curriculum to support LGBTQIA+ health professionals
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 15 February 2024, e44
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The Impact of the Size of Bribes on Criminal Sanctions: An Integrated Philosophical and Economic Analysis
-
- Journal:
- Canadian Journal of Law & Jurisprudence / Volume 37 / Issue 1 / February 2024
- Published online by Cambridge University Press:
- 17 April 2024, pp. 31-46
- Print publication:
- February 2024
-
- Article
- Export citation
Chapter 2 - Point-of-Care Ultrasound for Obstetrics: Basics and Introductory Chapter
-
-
- Book:
- Obstetric Anesthesia and Uncommon Disorders
- Published online:
- 26 January 2024
- Print publication:
- 01 February 2024, pp 6-13
-
- Chapter
- Export citation
On the scaling and critical layer in a turbulent boundary layer over a compliant surface
-
- Journal:
- Journal of Fluid Mechanics / Volume 980 / 10 February 2024
- Published online by Cambridge University Press:
- 31 January 2024, R2
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Impact of oral vancomycin treatment duration on rate of Clostridioides difficile recurrence in patients requiring concurrent systemic antibiotics
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 30 January 2024, pp. 1-9
-
- Article
- Export citation
Influence of Cations on Aggregation Rates in Mg-Montmorillonite
-
- Journal:
- Clays and Clay Minerals / Volume 61 / Issue 1 / February 2013
- Published online by Cambridge University Press:
- 01 January 2024, pp. 1-10
-
- Article
- Export citation
Bacteria-clay interaction: Structural changes in smectite induced during biofilm formation
-
- Journal:
- Clays and Clay Minerals / Volume 57 / Issue 2 / April 2009
- Published online by Cambridge University Press:
- 01 January 2024, pp. 205-212
-
- Article
- Export citation
Granular dilatancy and non-local fluidity of partially molten rock
-
- Journal:
- Journal of Fluid Mechanics / Volume 978 / 10 January 2024
- Published online by Cambridge University Press:
- 27 December 2023, A7
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
14 Changes in Service Delivery Models for Children with Neurodevelopmental Disorders During the Covid-19 Pandemic
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 623-624
-
- Article
-
- You have access
- Export citation
90 School-based Implementation of Educational and Neurocognitive Interventions in Children with Neurodevelopmental Disorders.
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 190-191
-
- Article
-
- You have access
- Export citation
22 - Pictorial Irony and Sarcasm
- from Part VI - Irony in Expressive, Nonlinguistic Media
-
-
- Book:
- The Cambridge Handbook of Irony and Thought
- Published online:
- 20 December 2023
- Print publication:
- 07 December 2023, pp 402-425
-
- Chapter
- Export citation
Wave statistics and energy dissipation of shallow-water breaking waves in a tank with a level bottom
-
- Journal:
- Journal of Fluid Mechanics / Volume 975 / 25 November 2023
- Published online by Cambridge University Press:
- 16 November 2023, A25
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
The present study focuses on two-dimensional direct numerical simulations of shallow-water breaking waves, specifically those generated by a wave plate at constant water depths. The primary objective is to quantitatively analyse the dynamics, kinematics and energy dissipation associated with wave breaking. The numerical results exhibit good agreement with experimental data in terms of free-surface profiles during wave breaking. A parametric study was conducted to examine the influence of various wave properties and initial conditions on breaking characteristics. According to research on the Bond number (
 $Bo$, the ratio of gravitational to surface tension forces), an increased surface tension leads to the formation of more prominent parasitic capillaries at the forwards face of the wave profile and a thicker plunging jet, which causes a delayed breaking time and is tightly correlated with the main cavity size. A close relationship between wave statistics and the initial conditions of the wave plate is discovered, allowing for the classification of breaker types based on the ratio of wave height to water depth,
$Bo$, the ratio of gravitational to surface tension forces), an increased surface tension leads to the formation of more prominent parasitic capillaries at the forwards face of the wave profile and a thicker plunging jet, which causes a delayed breaking time and is tightly correlated with the main cavity size. A close relationship between wave statistics and the initial conditions of the wave plate is discovered, allowing for the classification of breaker types based on the ratio of wave height to water depth,  $H/d$. Moreover, an analysis based on inertial scaling arguments reveals that the energy dissipation rate due to breaking can be linked to the local geometry of the breaking crest
$H/d$. Moreover, an analysis based on inertial scaling arguments reveals that the energy dissipation rate due to breaking can be linked to the local geometry of the breaking crest  $H_b/d$, and exhibits a threshold behaviour, where the energy dissipation approaches zero at a critical value of
$H_b/d$, and exhibits a threshold behaviour, where the energy dissipation approaches zero at a critical value of  $H_b/d$. An empirical scaling of the breaking parameter is proposed as
$H_b/d$. An empirical scaling of the breaking parameter is proposed as  $b = a(H_b/d - \chi _0)^n$, where
$b = a(H_b/d - \chi _0)^n$, where  $\chi _0 = 0.65$ represents the breaking threshold and
$\chi _0 = 0.65$ represents the breaking threshold and  $n = 1.5$ is a power law determined through the best fit to the numerical results.
$n = 1.5$ is a power law determined through the best fit to the numerical results.







Remembrance of Things Past
-
-
- Book:
- International Survey of Family Law 2023
- Published by:
- Intersentia
- Published online:
- 03 April 2024
- Print publication:
- 31 October 2023, pp 33-36
-
- Chapter
- Export citation
Analysis of high-speed drop impact onto deep liquid pool
-
- Journal:
- Journal of Fluid Mechanics / Volume 972 / 10 October 2023
- Published online by Cambridge University Press:
- 04 October 2023, A31
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Congruence between International Classification of Disease, Tenth Revision (ICD-10) code and written documentation for outpatient encounters with antibiotic prescriptions
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s39
-
- Article
-
- You have access
- Open access
- Export citation
Impact of COVID-19 on healthcare-associated infections in Canadian acute-care hospitals: Interrupted time series (2018–2021)
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s112-s113
-
- Article
-
- You have access
- Open access
- Export citation
-
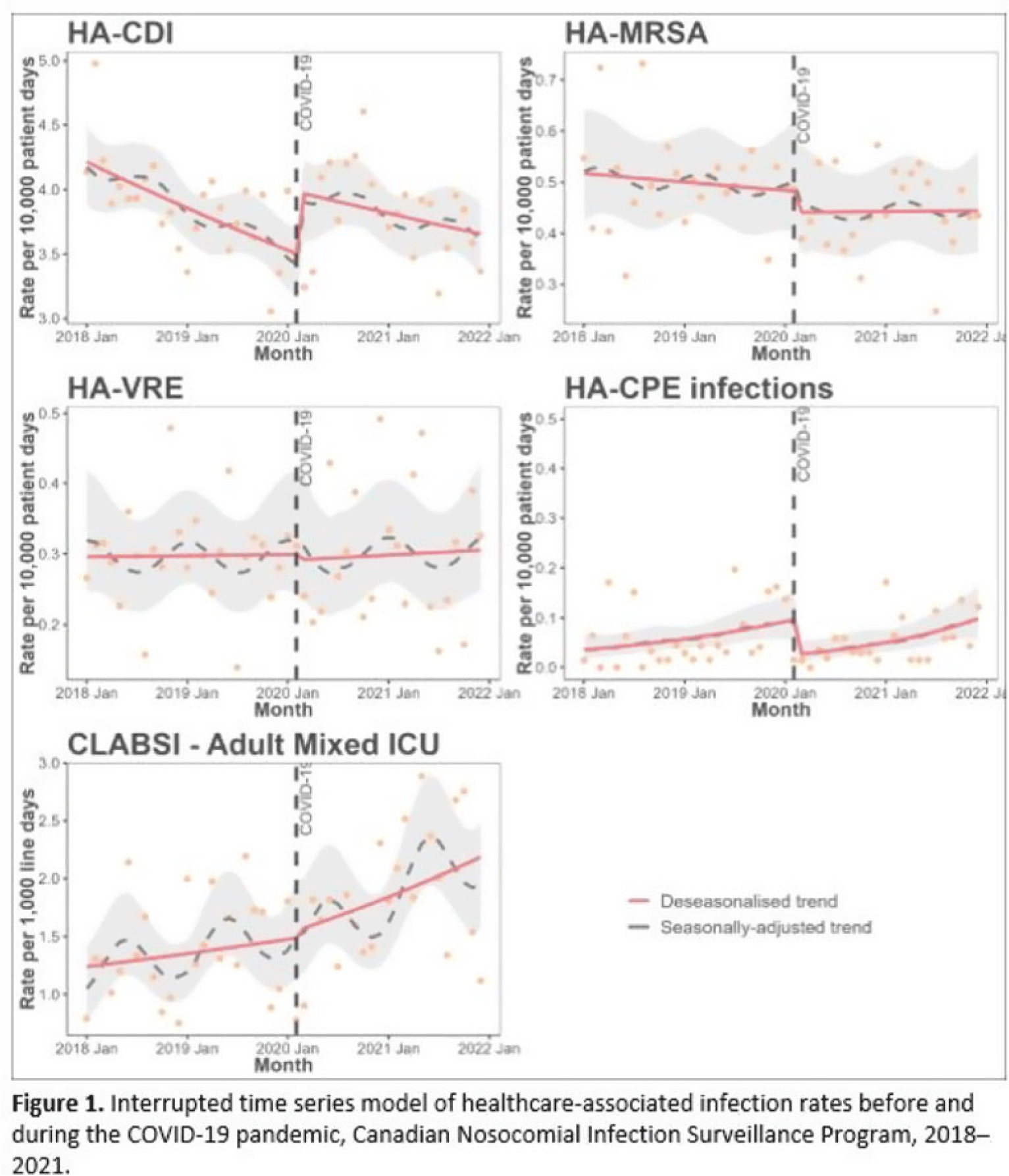
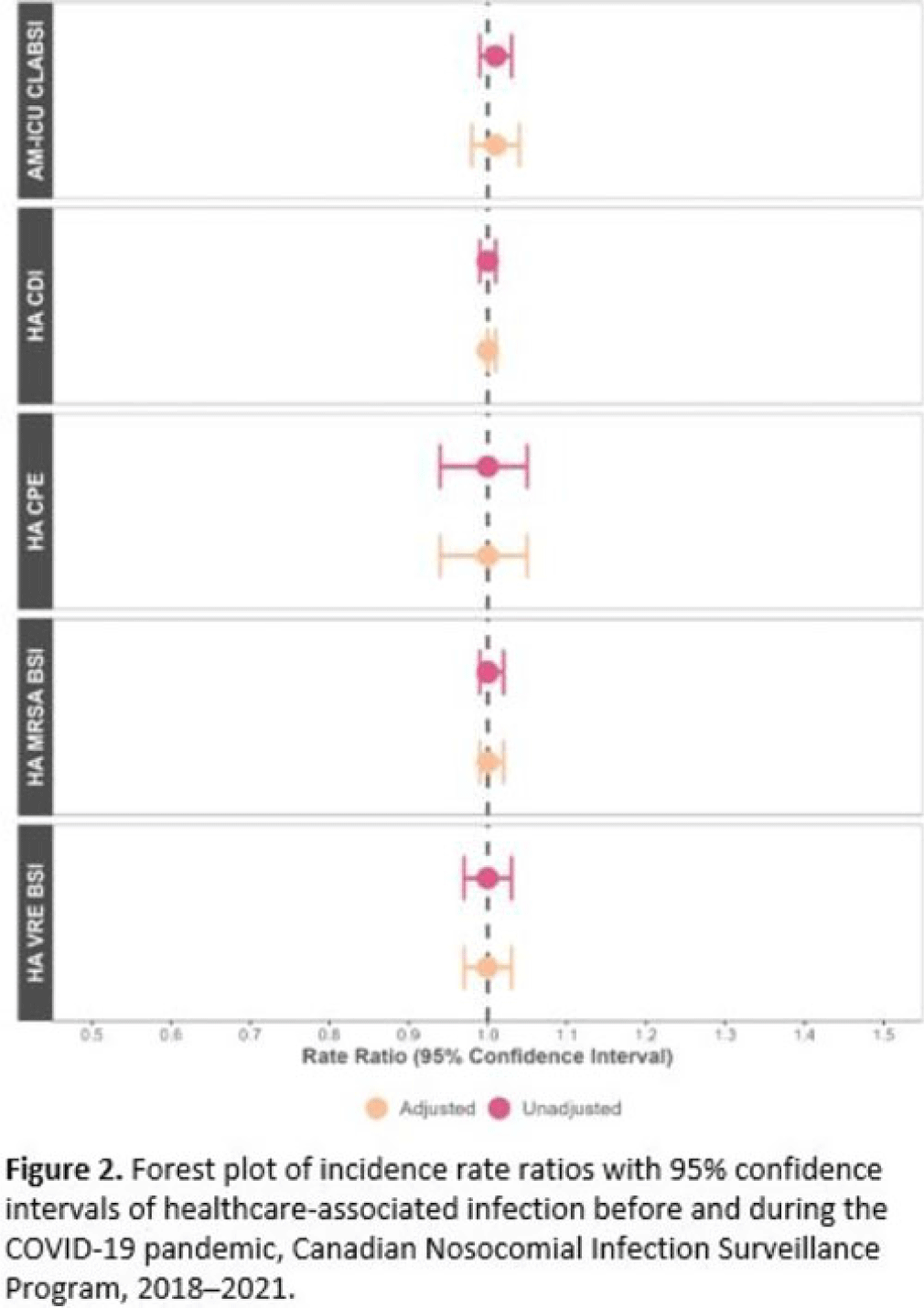
Background: Data regarding the effects of the SARS-COV-2 (COVID-19) pandemic on healthcare-associated infections (HAIs) in Canadian acute-care hospitals are limited. We examined the impact of the COVID-19 pandemic on HAIs and antimicrobial resistant organisms in hospitals participating in the Canadian Nosocomial Infection Surveillance Program. Methods: We analyzed 13,406 HAIs including adult mixed intensive care unit (ICU) central-line–associated bloodstream infections (CLABSIs), and healthcare-associated (HA) Clostridioides difficile infection (CDI), methicillin-resistant Staphylococcus aureus (MRSA) bloodstream infections (BSI), vancomycin-resistant Enterococcus (VRE) BSI, and carbapenemase-producing Enterobacterales (CPE) infections collected using standardized case definitions and questionnaires from 29–64 hospitals participating in the Canadian Nosocomial Infection Surveillance Program (CNISP) from January 2018 to December 2021. We used a generalized linear mixed model with quasi-Poisson distribution to assess step and slope changes in monthly HAI rates between the pre–COVID-19 pandemic period (January 1, 2018–February 29, 2020; 26 time points) and the COVID-19 pandemic period (March 1, 2020–December 31, 2021; 22 time points). Results were reported as incidence rate ratios (IRRs) with 95% confidence intervals (CIs) and adjusted for seasonality, hospital clustering, and hospital characteristics of interest. Results: In the CNISP network, 7,352 (55%) HAIs were reported in the prepandemic period and 6,054 (45%) in the pandemic period. Median age was significantly younger during the pandemic period compared to the prepandemic period among patients with HA-CDI, HA-MRSA BSI, and adult mixed ICU CLABSIs, and more than half of cases among all reported HAIs were male (range, 52%–65%). The 30-day all-cause in-hospital mortality rate did not significantly change between the prepandemic and pandemic periods for all reported HAIs and was highest among HA-VRE BSIs (34%). Modeling results indicated that the COVID-19 pandemic was associated with an immediate increase in HA-CDI and adult mixed ICU CLABSI rates whereas HA-MRSA BSI, HA-CPE and HA-VRE BSI rates immediately decreased. However, pandemic status did not have a statistically significant lasting impact on monthly rate trends for all reported HAIs after adjusting for seasonality, clustering, and hospital covariates (Fig. 1 and 2). Adjusted IRRs for all HAIs ranged from 1.00 to 1.01 (95% CI, 0.94–0.99 to 1.01–1.05).
 Conclusions: Although the COVID-19 pandemic placed a significant burden on the Canadian healthcare system, the immediate impact on monthly rates of HAIs in Canadian acute-care hospitals was not sustained over time. Understanding the epidemiological effects of the COVID-19 pandemic in the context of changing patient populations, and clinical and infection control practices, are essential to inform the continued management and prevention of HAIs in Canadian acute-care settings.
Conclusions: Although the COVID-19 pandemic placed a significant burden on the Canadian healthcare system, the immediate impact on monthly rates of HAIs in Canadian acute-care hospitals was not sustained over time. Understanding the epidemiological effects of the COVID-19 pandemic in the context of changing patient populations, and clinical and infection control practices, are essential to inform the continued management and prevention of HAIs in Canadian acute-care settings.Disclosures: None


Epidemiology of central-line–associated bloodstream infection mortality in Canadian NICUs before and after 2017
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s48
-
- Article
-
- You have access
- Open access
- Export citation
Pain flashbacks: The role of intrusive pain symptoms in posttraumatic chronic pain
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S112
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Findings demonstrate the high comorbidity of posttraumatic stress disorder (PTSD) and chronic pain following exposure to trauma. In exposure to child abuse (CA) in particular, findings imply that CA survivors are at a higher risk of suffering from chronic pain. However, the underlying mechanisms of these processes are yet to be uncovered.
ObjectivesThis study examined a new mechanism pertaining to the potential role of intrusive pain flashbacks for explaining the link between CA, C/PTSD, and chronic pain following interpersonal trauma.
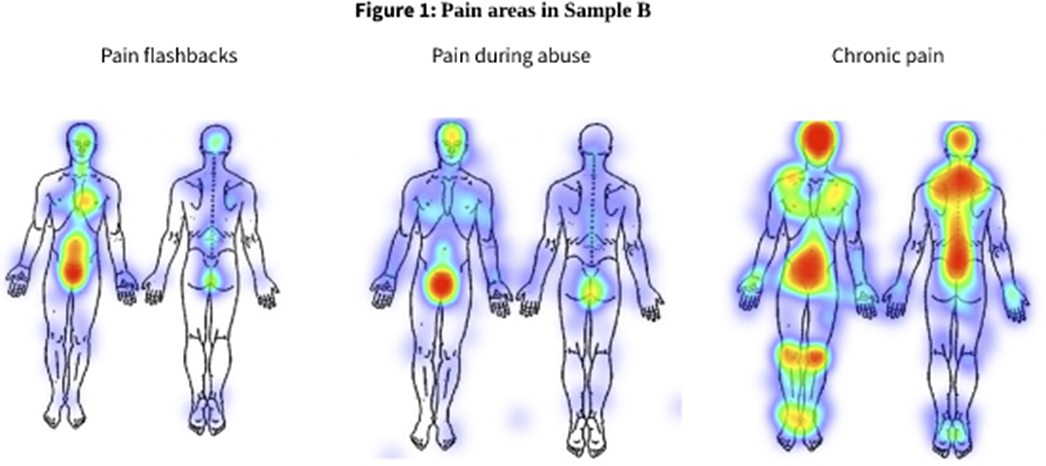
MethodsA community sample of 430 women (Sample A), and a sample of 164 women who were exposed to CA (Sample B) completed questionnaires assessing pain flashbacks, CA, C/PTSD symptoms, the experience of pain during the trauma, and chronic pain.
ResultsThe findings showed that 8.9% of Sample A (N = 36), and 23.1% of Sample B (N = 37) reported experiencing pain flashbacks. In both samples, participants who experienced pain flashbacks reported more severe C/PTSD (p<0.001), compared to participants who experienced flashbacks without pain and those who did not experience pain flashbacks. Participants who experienced pain flashbacks reported more pain during CA (p = 0.001), which corresponded with the pain flashbacks areas (Figure 1). Finally, pain flashbacks were correlated with a higher risk of suffering from chronic pain in Sample B (p=0.002).
Image:
 Conclusions
ConclusionsThe findings of this study reveal that pain flashbacks are associated with more rampant CA and are linked to greater psychopathology. The findings call for further investigation of the role of pain flashbacks in explaining the link between exposure to trauma, C/PTSD and later chronic pain.
Disclosure of InterestNone Declared

