
214 results
469 Diverse Role of blaCTX-M and Porins in Mediating Ertapenem Resistance Among Carbapenem Resistant Enterobacterales
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue s1 / April 2024
- Published online by Cambridge University Press:
- 03 April 2024, p. 138
-
- Article
-
- You have access
- Open access
- Export citation
3 - What If There Is No Legislator?
-
-
- Book:
- The Cambridge Companion to Rousseau's <i>Social Contract</i>
- Published online:
- 28 March 2024
- Print publication:
- 22 February 2024, pp 40-63
-
- Chapter
- Export citation
Research agenda for antibiotic stewardship within the Veterans’ Health Administration, 2024–2028
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 02 February 2024, pp. 1-7
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
6 Improved verbal fluency following unilateral right hemisphere subthalamic nucleus deep brain stimulation for Parkinson’s disease: Is implant hemisphere a modifiable risk factor for cognitive decline?
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 112-113
-
- Article
-
- You have access
- Export citation
The N3C governance ecosystem: A model socio-technical partnership for the future of collaborative analytics at scale
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 14 November 2023, e252
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Partula tree snail conservation back on track
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Radiofrequency ice dielectric measurements at Summit Station, Greenland
-
- Journal:
- Journal of Glaciology , First View
- Published online by Cambridge University Press:
- 09 October 2023, pp. 1-12
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
We recently reported on the radio-frequency attenuation length of cold polar ice at Summit Station, Greenland, based on bi-static radar measurements of radio-frequency bedrock echo strengths taken during the summer of 2021. Those data also allow studies of (a) the relative contributions of coherent (such as discrete internal conducting layers with sub-centimeter transverse scale) vs incoherent (e.g. bulk volumetric) scattering, (b) the magnitude of internal layer reflection coefficients, (c) limits on signal propagation velocity asymmetries (‘birefringence’) and (d) limits on signal dispersion in-ice over a bandwidth of ~100 MHz. We find that (1) attenuation lengths approach 1 km in our band, (2) after averaging 10 000 echo triggers, reflected signals observable over the thermal floor (to depths of ~1500 m) are consistent with being entirely coherent, (3) internal layer reflectivities are ≈–60$\to$
 –70 dB, (4) birefringent effects for vertically propagating signals are smaller by an order of magnitude relative to South Pole and (5) within our experimental limits, glacial ice is non-dispersive over the frequency band relevant for neutrino detection experiments.
–70 dB, (4) birefringent effects for vertically propagating signals are smaller by an order of magnitude relative to South Pole and (5) within our experimental limits, glacial ice is non-dispersive over the frequency band relevant for neutrino detection experiments.

Chapter 11 - The Need to Belong
- from Part III - QAnon and Society
-
-
- Book:
- The Social Science of QAnon
- Published online:
- 14 September 2023
- Print publication:
- 28 September 2023, pp 176-192
-
- Chapter
- Export citation
“The Wild West:” Nurse Experiences of Responding to the 2017 Las Vegas Mass Shooting
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 17 / 2023
- Published online by Cambridge University Press:
- 18 September 2023, e492
-
- Article
- Export citation
Moral Individualism in Modern Politics: A New Measure Inspired by Political Theory
-
- Journal:
- Perspectives on Politics / Volume 21 / Issue 4 / December 2023
- Published online by Cambridge University Press:
- 14 June 2023, pp. 1376-1398
- Print publication:
- December 2023
-
- Article
- Export citation
361 WDR5 represents a therapeutically exploitable target for cancer stem cells in glioblastoma
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue s1 / April 2023
- Published online by Cambridge University Press:
- 24 April 2023, p. 107
-
- Article
-
- You have access
- Open access
- Export citation
KAMIL CYPRIAN CHODA, MAURITS STERK DE LEEUW and FABIAN SCHULZ (EDS), GAINING AND LOSING IMPERIAL POWER IN LATE ANTIQUITY: REPRESENTATION AND REALITY (Impact of Empire 36). Leiden and Boston: Brill, 2019. Pp. xi + 255. isbn 9789004407695. €119.00/$144.00. - MARÍA PILAR GARCÍA RUIZ and ALBERTO J. QUIROGA PUERTAS (EDS), EMPERORS AND EMPERORSHIP IN LATE ANTIQUITY: IMAGES AND NARRATIVES (Impact of Empire 40). Leiden and Boston: Brill, 2021. Pp. xii + 248, illus. isbn 9789004446908. €105.00/$127.00.
-
- Journal:
- The Journal of Roman Studies / Volume 112 / November 2022
- Published online by Cambridge University Press:
- 25 October 2022, pp. 336-338
- Print publication:
- November 2022
-
- Article
- Export citation
Understanding Turkey Management in the Mimbres Valley of Southwestern New Mexico Using Ancient Mitochondrial DNA and Stable Isotopes
-
- Journal:
- American Antiquity / Volume 88 / Issue 1 / January 2023
- Published online by Cambridge University Press:
- 21 October 2022, pp. 41-61
- Print publication:
- January 2023
-
- Article
- Export citation
Chapter 8 - Substance Misuse and Addiction
-
-
- Book:
- Spirituality and Psychiatry
- Published online:
- 07 October 2022
- Print publication:
- 20 October 2022, pp 158-179
-
- Chapter
- Export citation
Implementation and outcomes of a clinician-directed intervention to improve antibiotic prescribing for acute respiratory tract infections within the Veterans’ Affairs Healthcare System
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 5 / May 2023
- Published online by Cambridge University Press:
- 15 August 2022, pp. 746-754
- Print publication:
- May 2023
-
- Article
- Export citation
KAMIL CYPRIAN CHODA, MAURITS STERK DE LEEUW and FABIAN SCHULZ (EDS), GAINING AND LOSING IMPERIAL POWER IN LATE ANTIQUITY: REPRESENTATION AND REALITY (Impact of Empire 36). Leiden and Boston: Brill, 2019. Pp. xi + 255. isbn 9789004407695. €119.00/$144.00. - MARÍA PILAR GARCÍA RUIZ and ALBERTO J. QUIROGA PUERTAS (EDS), EMPERORS AND EMPERORSHIP IN LATE ANTIQUITY: IMAGES AND NARRATIVES (Impact of Empire 40). Leiden and Boston: Brill, 2021. Pp. xii + 248, illus. isbn 9789004446908. €105.00/$127.00.
-
- Journal:
- The Journal of Roman Studies , First View
- Published online by Cambridge University Press:
- 11 July 2022, pp. 1-3
-
- Article
- Export citation
Practice Variation between Salaried and Fee-for-Service Surgeons for Lumbar Surgery
-
- Journal:
- Canadian Journal of Neurological Sciences / Volume 50 / Issue 4 / July 2023
- Published online by Cambridge University Press:
- 16 June 2022, pp. 604-611
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Ensuring a safe(r) harbor: Excising personally identifiable information from structured electronic health record data
-
- Journal:
- Journal of Clinical and Translational Science / Volume 6 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 09 December 2021, e10
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Efficacy and Safety of Investigational Microbiome Drug SER-109 for Treatment of Recurrent Clostridioides difficile Infection
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s5
-
- Article
-
- You have access
- Open access
- Export citation
-
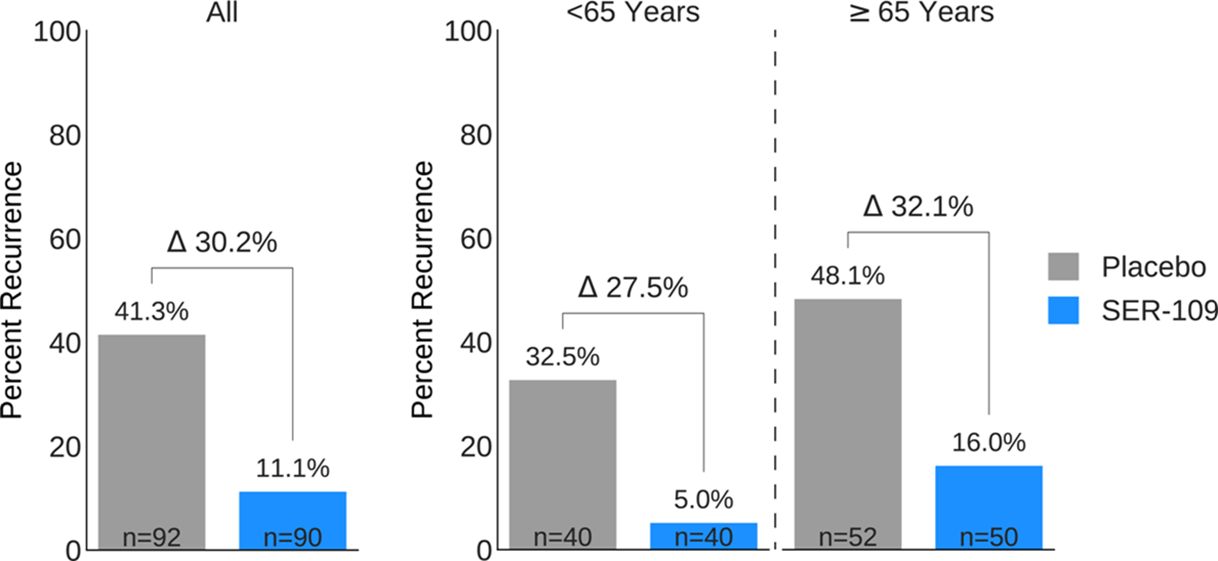
Background: Antibiotics targeted against Clostridioides difficile bacteria are necessary, but insufficient, to achieve a durable clinical response because they have no effect on C. difficile spores that germinate within a disrupted microbiome. ECOSPOR-III evaluated SER-109, an investigational, biologically derived microbiome therapeutic of purified Firmicute spores for treatment of rCDI. Herein, we present the interim analysis in the ITT population at 8 and 12 weeks. Methods: Adults ≥18 years with rCDI (≥3 episodes in 12 months) were screened at 75 US and CAN sites. CDI was defined as ≥3 unformed stools per day for <48 hours with a positive C. difficile assay. After completion of 10–21 days of vancomycin or fidaxomicin, adults with symptom resolution were randomized 1:1 to SER-109 (4 capsules × 3 days) or matching placebo and stratified by age (≥ or <65 years) and antibiotic received. Primary objectives were safety and efficacy at 8 weeks. Primary efficacy endpoint was rCDI (recurrent toxin+ diarrhea requiring treatment); secondary endpoints included efficacy at 12 weeks after dosing. Results: Overall, 287 participants were screened and 182 were randomized (59.9% female; mean age, 65.5 years). The most common reason for screen failure was a negative C. difficile toxin assay. A significantly lower proportion of SER-109 participants had rCDI after dosing compared to placebo at week 8 (11.1% vs 41.3%, respectively; relative risk [RR], 0.27; 95% confidence interval [CI], 0.15–0.51; p-value <0.001). Efficacy rates were significantly higher with SER-109 vs placebo in both stratified age groups (Figure 1). SER-109 was well-tolerated with a safety profile similar to placebo. The most common treatment-emergent adverse events (TEAEs) were gastrointestinal and were mainly mild to moderate. No serious TEAEs, infections, deaths, or drug discontinuations were deemed related to study drug. Conclusions: SER-109, an oral live microbiome therapeutic, achieved high rates of sustained clinical response with a favorable safety profile. By enriching for Firmicute spores, SER-109 achieves high efficacy while mitigating risk of transmitting infectious agents, beyond donor screening alone. SER-109 represents a major paradigm shift in the clinical management of patients with recurrent CDI. Clinicaltrials.gov Identifier NCT03183128. These data were previously presented as a late breaker at American College of Gastroenterology 2020.
Funding: Seres Therapeutics
Disclosures: None
Figure 1.

Behavioral activation therapy for depression is associated with a reduction in the concentration of circulating quinolinic acid — Erratum
-
- Journal:
- Psychological Medicine / Volume 52 / Issue 13 / October 2022
- Published online by Cambridge University Press:
- 12 July 2021, p. 2846
-
- Article
-
- You have access
- HTML
- Export citation
