
2044 results
Moderate and Deep Sedation in Clinical Practice
- Coming soon
-
- Expected online publication date:
- December 2024
- Print publication:
- 30 November 2024
-
- Book
- Export citation
Reflecting on Armenians in Ottoman Historiography
-
- Journal:
- Review of Middle East Studies , First View
- Published online by Cambridge University Press:
- 24 September 2024, pp. 1-10
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Social security and retirement around the world: lessons from a long-term collaboration
-
- Journal:
- Journal of Pension Economics & Finance , First View
- Published online by Cambridge University Press:
- 19 September 2024, pp. 1-23
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Temporal decreases in pathogen colonization and infection among hospitalized neonates following routine skin antisepsis with chlorhexidine gluconate: Botswana 2022 – 2023
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s12
-
- Article
-
- You have access
- Open access
- Export citation
-
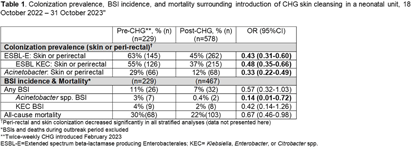
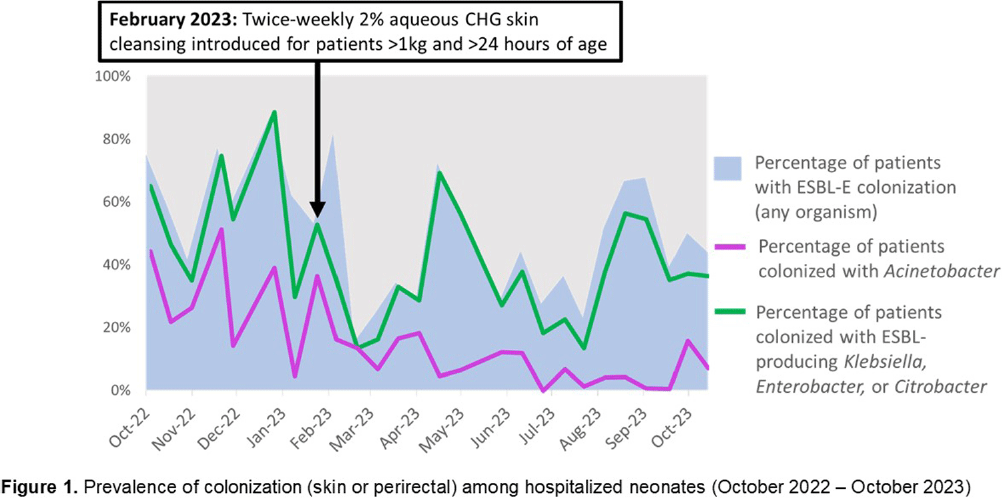
Background: Multidrug-resistant Gram-negative bacteria are a major cause of sepsis among hospitalized neonates globally. Aqueous chlorhexidine gluconate (CHG) skin antisepsis has been shown to be safe for use in infants; however, its sustained effectiveness in preventing Gram-negative pathogen colonization, bloodstream infection (BSI), and mortality is unclear. Methods: We conducted a period prevalence survey, with 26 sampling events over 12 months (18 October 2022 – 31 October 2023) at a 33-bed neonatal unit in a tertiary public hospital in Botswana where ESBL-producing Klebsiella pneumoniae and carbapenem-resistant Acinetobacter baumannii are leading causes of BSI. Perirectal and periumbilical skin swabs were collected every two weeks from all inpatients. Swabs were inoculated onto chromogenic media selective and differential for extended-spectrum beta-lactamase producing Enterobacterales (ESBL-E) and Acinetobacter spp. (CHROMagar™ ESBL, Acinetobacter). Colonization status was determined based on culture growth and colony morphology. Contemporaneous data on all-cause mortality and BSI were abstracted from routine surveillance records. Pre- and post-CHG prevalences were compared using a simple Chi-square test. During the surveillance period, an outbreak of K. pneumoniae linked to contaminated multi-use vials was detected, thus BSIs and deaths during the outbreak period (2 February–6 April, 2023) were excluded. In February 2023, the hospital infection prevention and control (IPC) team introduced twice-weekly whole-body cleansing with commercially available 2% aqueous CHG, performed by caregivers and healthcare workers on neonates >24 hours old and weighing ≥1 kg until discharge. Results: There were significant decreases in ESBL-E and Acinetobacter skin and perirectal colonization following the CHG intervention (Table 1; Figure 1). After the CHG intervention, the incidence of Acinetobacter BSIs declined significantly and there was a trend toward a decline in other BSIs and mortality. No adverse events associated with CHG were reported. Conclusions: Twice-weekly CHG application was temporally associated with significant reductions in neonatal ESBL-E and Actinetobacter skin and perirectal colonization and Acinetobacter BSI. This analysis was limited by a short pre-intervention surveillance period and thus may have been influenced by confounders such as seasonality, and intensified IPC efforts following the outbreak. Analysis of the routine CHG use in other settings and over longer surveillance periods are needed to better understand its effectiveness as an IPC strategy in settings where neonatal sepsis incidence is high. Table 1. Colonization prevalence, BSI incidence, and mortality surrounding introduction of CHG skin cleansing in a neonatal unit, 18 October 2022 – 31 October 2023.


Detecting suicide risk among U.S. servicemembers and veterans: a deep learning approach using social media data
-
- Journal:
- Psychological Medicine , First View
- Published online by Cambridge University Press:
- 09 September 2024, pp. 1-10
-
- Article
-
- You have access
- HTML
- Export citation
Development and initial evaluation of a clinical prediction model for risk of treatment resistance in first-episode psychosis: Schizophrenia Prediction of Resistance to Treatment (SPIRIT)
-
- Journal:
- The British Journal of Psychiatry , FirstView
- Published online by Cambridge University Press:
- 05 August 2024, pp. 1-10
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Ectoparasite and bacterial population genetics and community structure indicate extent of bat movement across an island chain
-
- Journal:
- Parasitology , First View
- Published online by Cambridge University Press:
- 24 May 2024, pp. 1-14
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Interactive visualization tool to understand and monitor health disparities in diabetes care and outcomes
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 17 May 2024, e102
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Diagnostic criteria and core outcome set development for necrotising otitis externa: the COSNOE Delphi consensus study
-
- Journal:
- The Journal of Laryngology & Otology , First View
- Published online by Cambridge University Press:
- 22 April 2024, pp. 1-8
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Laxative use in adults with intellectual disabilities: development of prescribing guidelines
-
- Journal:
- BJPsych Open / Volume 10 / Issue 3 / May 2024
- Published online by Cambridge University Press:
- 18 April 2024, e84
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
VaTEST III: Validation of eight potential super-earths from TESS data
-
- Journal:
- Publications of the Astronomical Society of Australia / Volume 41 / 2024
- Published online by Cambridge University Press:
- 11 April 2024, e030
-
- Article
-
- You have access
- HTML
- Export citation
-
NASA’s all-sky survey mission, the Transiting Exoplanet Survey Satellite (TESS), is specifically engineered to detect exoplanets that transit bright stars. Thus far, TESS has successfully identified approximately 400 transiting exoplanets, in addition to roughly 6 000 candidate exoplanets pending confirmation. In this study, we present the results of our ongoing project, the Validation of Transiting Exoplanets using Statistical Tools (VaTEST). Our dedicated effort is focused on the confirmation and characterisation of new exoplanets through the application of statistical validation tools. Through a combination of ground-based telescope data, high-resolution imaging, and the utilisation of the statistical validation tool known as TRICERATOPS, we have successfully discovered eight potential super-Earths. These planets bear the designations: TOI-238b (1.61
 $^{+0.09} _{-0.10}$ R
$^{+0.09} _{-0.10}$ R $_\oplus$), TOI-771b (1.42
$_\oplus$), TOI-771b (1.42 $^{+0.11} _{-0.09}$ R
$^{+0.11} _{-0.09}$ R $_\oplus$), TOI-871b (1.66
$_\oplus$), TOI-871b (1.66 $^{+0.11} _{-0.11}$ R
$^{+0.11} _{-0.11}$ R $_\oplus$), TOI-1467b (1.83
$_\oplus$), TOI-1467b (1.83 $^{+0.16} _{-0.15}$ R
$^{+0.16} _{-0.15}$ R $_\oplus$), TOI-1739b (1.69
$_\oplus$), TOI-1739b (1.69 $^{+0.10} _{-0.08}$ R
$^{+0.10} _{-0.08}$ R $_\oplus$), TOI-2068b (1.82
$_\oplus$), TOI-2068b (1.82 $^{+0.16} _{-0.15}$ R
$^{+0.16} _{-0.15}$ R $_\oplus$), TOI-4559b (1.42
$_\oplus$), TOI-4559b (1.42 $^{+0.13} _{-0.11}$ R
$^{+0.13} _{-0.11}$ R $_\oplus$), and TOI-5799b (1.62
$_\oplus$), and TOI-5799b (1.62 $^{+0.19} _{-0.13}$ R
$^{+0.19} _{-0.13}$ R $_\oplus$). Among all these planets, six of them fall within the region known as ‘keystone planets’, which makes them particularly interesting for study. Based on the location of TOI-771b and TOI-4559b below the radius valley we characterised them as likely super-Earths, though radial velocity mass measurements for these planets will provide more details about their characterisation. It is noteworthy that planets within the size range investigated herein are absent from our own solar system, making their study crucial for gaining insights into the evolutionary stages between Earth and Neptune.
$_\oplus$). Among all these planets, six of them fall within the region known as ‘keystone planets’, which makes them particularly interesting for study. Based on the location of TOI-771b and TOI-4559b below the radius valley we characterised them as likely super-Earths, though radial velocity mass measurements for these planets will provide more details about their characterisation. It is noteworthy that planets within the size range investigated herein are absent from our own solar system, making their study crucial for gaining insights into the evolutionary stages between Earth and Neptune.
















Querying ‘Global’ Music History: Significant Geographies between Goswami Pannalal and Queen Victoria
-
- Journal:
- Royal Musical Association Research Chronicle ,
- Published online by Cambridge University Press:
- 05 April 2024, pp. 1-12
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
569 Investigating the Role of FOXA2 During the Transition to Neuroendocrine Prostate Cancer
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue s1 / April 2024
- Published online by Cambridge University Press:
- 03 April 2024, pp. 148-149
-
- Article
-
- You have access
- Open access
- Export citation
Head and Neck Cancer: United Kingdom National Multidisciplinary Guidelines, Sixth Edition
-
- Journal:
- The Journal of Laryngology & Otology / Volume 138 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 14 March 2024, pp. S1-S224
- Print publication:
- April 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Astrobiological applications of μ-mapping X-ray fluorescence spectrometry
-
- Journal:
- International Journal of Astrobiology / Volume 23 / 2024
- Published online by Cambridge University Press:
- 04 March 2024, e8
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Trajectory of adjustment difficulties following disaster: 10-year longitudinal cohort study
-
- Journal:
- BJPsych Open / Volume 10 / Issue 2 / March 2024
- Published online by Cambridge University Press:
- 04 March 2024, e57
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The Natural Occurrence of Eta-Alumina (η-Al2O3) in Bauxite
-
- Journal:
- Clays and Clay Minerals / Volume 44 / Issue 5 / October 1996
- Published online by Cambridge University Press:
- 28 February 2024, pp. 658-664
-
- Article
-
- You have access
- Export citation
Analytical Electron Microscopy in Clays and Other Phyllosilicates: Loss of Elements from a 90-nm Stationary Beam of 300-keV Electrons
-
- Journal:
- Clays and Clay Minerals / Volume 46 / Issue 3 / June 1998
- Published online by Cambridge University Press:
- 28 February 2024, pp. 301-316
-
- Article
-
- You have access
- Export citation
Hisingerite: A Ferric Kaolin Mineral with Curved Morphology
-
- Journal:
- Clays and Clay Minerals / Volume 46 / Issue 4 / August 1998
- Published online by Cambridge University Press:
- 28 February 2024, pp. 400-413
-
- Article
-
- You have access
- Export citation
Tohdite (5Al2O3 · H2O) in Bauxites from Northern Australia
-
- Journal:
- Clays and Clay Minerals / Volume 42 / Issue 4 / August 1994
- Published online by Cambridge University Press:
- 28 February 2024, pp. 485-488
-
- Article
-
- You have access
- Export citation
