
106 results
Strategies to promote language inclusion at 17 CTSA hubs
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 25 March 2024, e67
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A survey of weed research priorities: key findings and future directions
-
- Journal:
- Weed Science / Volume 71 / Issue 4 / July 2023
- Published online by Cambridge University Press:
- 13 June 2023, pp. 330-343
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Proactive and reactive aggression: Developmental trajectories and longitudinal associations with callous–unemotional traits, impulsivity, and internalizing emotions
-
- Journal:
- Development and Psychopathology , First View
- Published online by Cambridge University Press:
- 03 April 2023, pp. 1-9
-
- Article
- Export citation
Anthropometric criteria for best-identifying children at high risk of mortality: a pooled analysis of twelve cohorts
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 4 / April 2023
- Published online by Cambridge University Press:
- 03 February 2023, pp. 803-819
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Prognostic value of different anthropometric indices over different measurement intervals to predict mortality in 6–59-month-old children
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 01 February 2023, pp. 1210-1221
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Severe acute respiratory coronavirus virus 2 (SARS-CoV-2) outbreaks in nursing homes involving residents who had completed a primary coronavirus disease 2019 (COVID-19) vaccine series—13 US jurisdictions, July–November 2021
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 16 January 2023, pp. 1005-1009
- Print publication:
- June 2023
-
- Article
- Export citation
A randomized implementation trial to increase adoption of evidence-informed consent practices
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 14 December 2022, e28
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Conducting a pediatric randomized clinical trial during a pandemic: A shift to virtual procedures
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 6 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 25 August 2022, e115
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Chapter 18 - Narrating Nature
- from Part III - Applications
-
-
- Book:
- Nature and Literary Studies
- Published online:
- 22 July 2022
- Print publication:
- 04 August 2022, pp 325-338
-
- Chapter
- Export citation
Characteristics of healthcare personnel who reported concerns related to PPE use during care of COVID-19 patients
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s8-s9
-
- Article
-
- You have access
- Open access
- Export citation
-
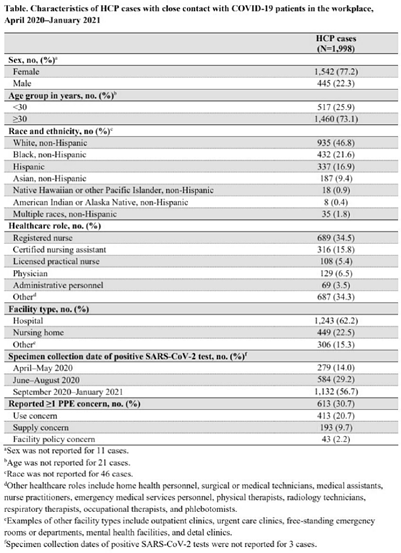
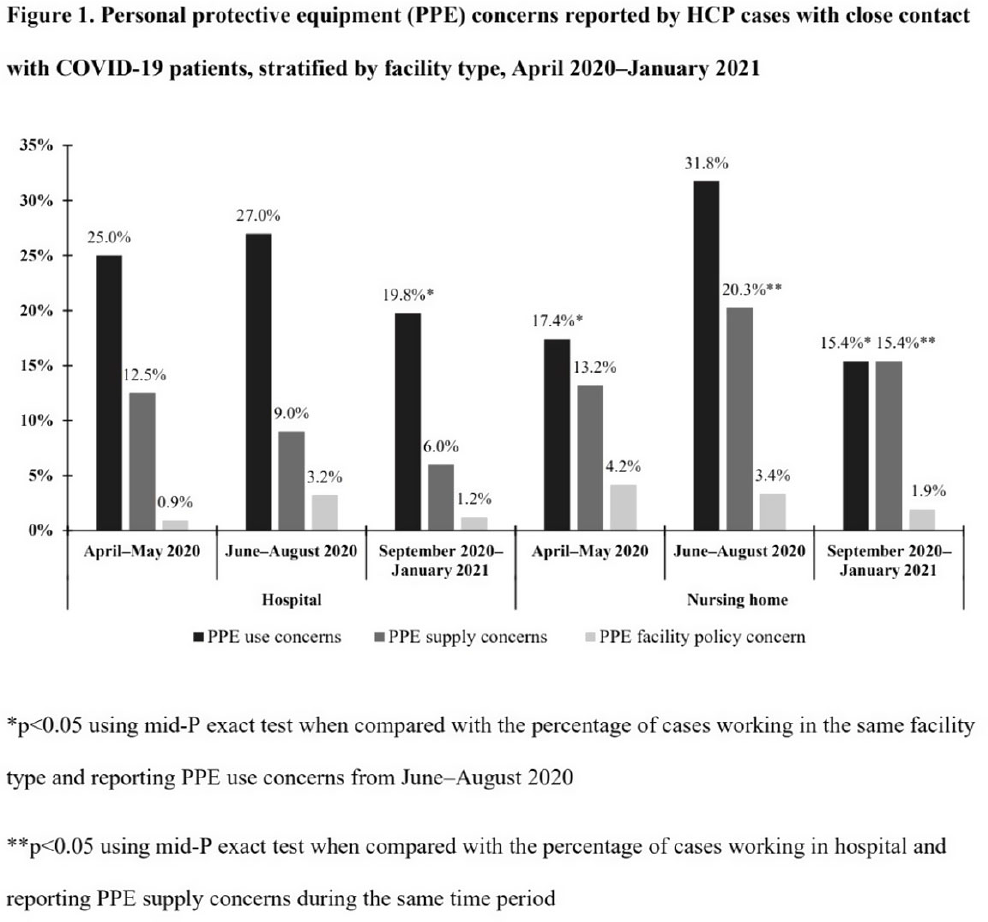
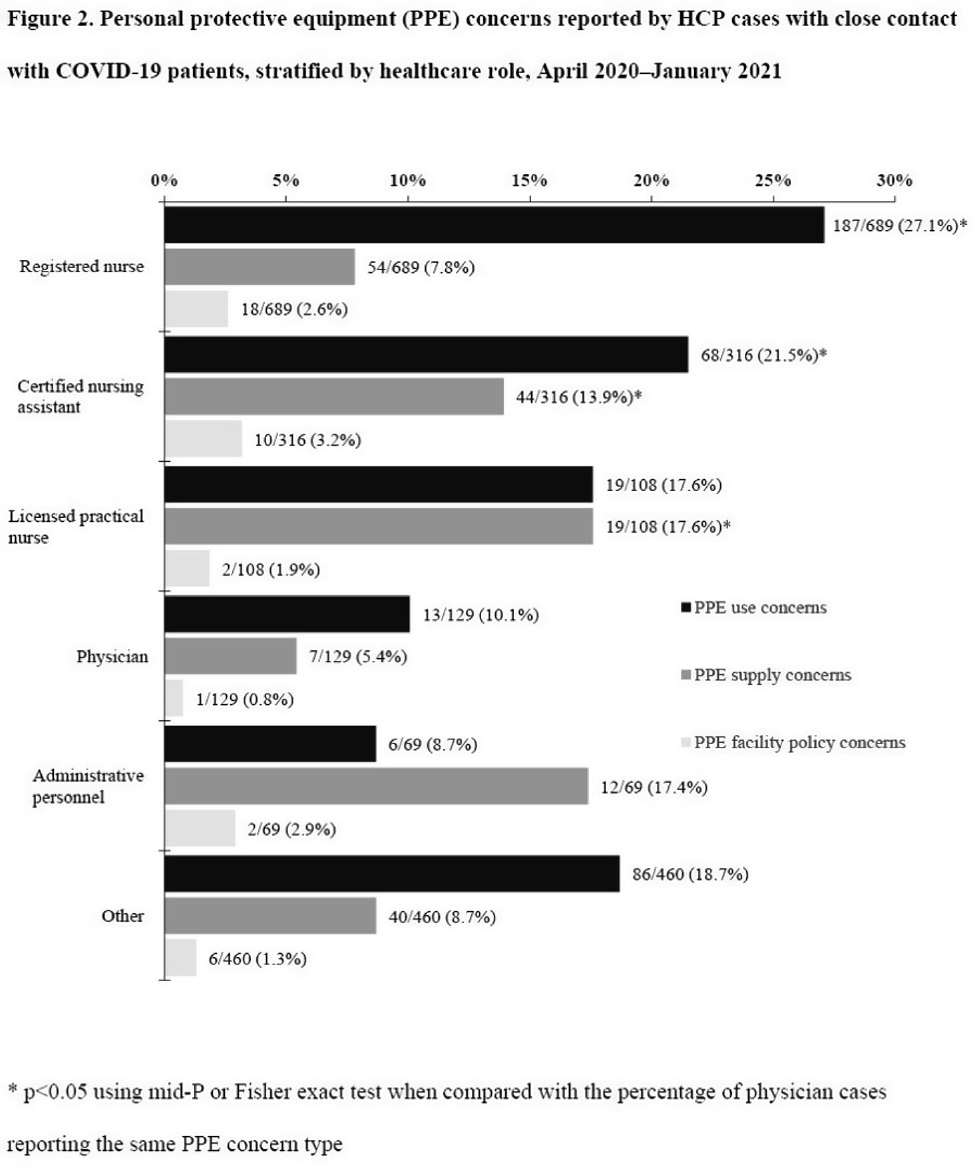
Background: Healthcare facilities have experienced many challenges during the COVID-19 pandemic, including limited personal protective equipment (PPE) supplies. Healthcare personnel (HCP) rely on PPE, vaccines, and other infection control measures to prevent SARS-CoV-2 infections. We describe PPE concerns reported by HCP who had close contact with COVID-19 patients in the workplace and tested positive for SARS-CoV-2. Method: The CDC collaborated with Emerging Infections Program (EIP) sites in 10 states to conduct surveillance for SARS-CoV-2 infections in HCP. EIP staff interviewed HCP with positive SARS-CoV-2 viral tests (ie, cases) to collect data on demographics, healthcare roles, exposures, PPE use, and concerns about their PPE use during COVID-19 patient care in the 14 days before the HCP’s SARS-CoV-2 positive test. PPE concerns were qualitatively coded as being related to supply (eg, low quality, shortages); use (eg, extended use, reuse, lack of fit test); or facility policy (eg, lack of guidance). We calculated and compared the percentages of cases reporting each concern type during the initial phase of the pandemic (April–May 2020), during the first US peak of daily COVID-19 cases (June–August 2020), and during the second US peak (September 2020–January 2021). We compared percentages using mid-P or Fisher exact tests (α = 0.05). Results: Among 1,998 HCP cases occurring during April 2020–January 2021 who had close contact with COVID-19 patients, 613 (30.7%) reported ≥1 PPE concern (Table 1). The percentage of cases reporting supply or use concerns was higher during the first peak period than the second peak period (supply concerns: 12.5% vs 7.5%; use concerns: 25.5% vs 18.2%; p Conclusions: Although lower percentages of HCP cases overall reported PPE concerns after the first US peak, our results highlight the importance of developing capacity to produce and distribute PPE during times of increased demand. The difference we observed among selected groups of cases may indicate that PPE access and use were more challenging for some, such as nonphysicians and nursing home HCP. These findings underscore the need to ensure that PPE is accessible and used correctly by HCP for whom use is recommended.
Funding: None
Disclosures: None



From paper to screen: regulatory and operational considerations for modernizing the informed consent process
-
- Journal:
- Journal of Clinical and Translational Science / Volume 6 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 28 March 2022, e71
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Do Physiological Variables Predict the Need for Transport to Hospital From Music Festivals? An Analysis of Australian Festival Data
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 17 / 2023
- Published online by Cambridge University Press:
- 03 March 2022, e105
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Divergent effects of sex and calcium/vitamin D supplementation on serum magnesium and markers of bone structure and function during initial military training
-
- Journal:
- British Journal of Nutrition / Volume 128 / Issue 9 / 14 November 2022
- Published online by Cambridge University Press:
- 24 November 2021, pp. 1730-1737
- Print publication:
- 14 November 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The Occupational Health Effects of Responding to a Natural Gas Pipeline Explosion Among Emergency First Responders – Lincoln County, Kentucky, 2019
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 16 / Issue 5 / October 2022
- Published online by Cambridge University Press:
- 21 September 2021, pp. 1997-2004
-
- Article
- Export citation

How We Got to Where We're Going
-
- Published online:
- 31 August 2021
- Print publication:
- 30 September 2021
-
- Element
- Export citation
Perceived barriers to assessing understanding and appreciation of informed consent in clinical trials: A mixed-method study
-
- Journal:
- Journal of Clinical and Translational Science / Volume 5 / Issue 1 / 2021
- Published online by Cambridge University Press:
- 28 June 2021, e164
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Practices and activities among healthcare personnel with severe acute respiratory coronavirus virus 2 (SARS-CoV-2) infection working in different healthcare settings—ten Emerging Infections Program sites, April–November 2020
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 8 / August 2022
- Published online by Cambridge University Press:
- 02 June 2021, pp. 1058-1062
- Print publication:
- August 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
2 - The Indivisibility of Human Dignity and Sustainability
- from Part I - Frameworks
-
-
- Book:
- The Cambridge Handbook of Environmental Justice and Sustainable Development
- Published online:
- 26 March 2021
- Print publication:
- 01 April 2021, pp 23-38
-
- Chapter
- Export citation
DOHaD in the land down under: 11th World Congress 2019
- Part of
-
- Journal:
- Journal of Developmental Origins of Health and Disease / Volume 11 / Issue 6 / December 2020
- Published online by Cambridge University Press:
- 29 September 2020, pp. 543-544
-
- Article
-
- You have access
- HTML
- Export citation
Both unmedicated and medicated individuals with schizophrenia show impairments across a wide array of cognitive and reinforcement learning tasks
-
- Journal:
- Psychological Medicine / Volume 52 / Issue 6 / April 2022
- Published online by Cambridge University Press:
- 17 August 2020, pp. 1115-1125
-
- Article
- Export citation
