
338 results
South East Asian Nutrition Surveys (SEANUTS) II - a multi-country evaluation of nutrition and lifestyle indicators in children aged 12 years and below: Rationale and Design
-
- Journal:
- Public Health Nutrition / Accepted manuscript
- Published online by Cambridge University Press:
- 19 April 2024, pp. 1-29
-
- Article
-
- You have access
- Open access
- Export citation
VaTEST III: Validation of 8 Potential Super-Earths from TESS Data
-
- Journal:
- Publications of the Astronomical Society of Australia / Accepted manuscript
- Published online by Cambridge University Press:
- 11 April 2024, pp. 1-22
-
- Article
- Export citation
-
NASA’s all-sky survey mission, the Transiting Exoplanet Survey Satellite (TESS), is specifically engineered to detect exoplanets that transit bright stars. Thus far, TESS has successfully identified approximately 400 transiting exoplanets, in addition to roughly 6000 candidate exoplanets pending confirmation. In this study, we present the results of our ongoing project, the Validation of Transiting Exoplanets using Statistical Tools (VaTEST). Our dedicated effort is focused on the confirmation and characterization of new exoplanets through the application of statistical validation tools. Through a combination of ground-based telescope data, high-resolution imaging, and the utilization of the statistical validation tool known as TRICERATOPS, we have successfully discovered eight potential super-Earths. These planets bear the designations: TOI-238b (
 R⊕), TOI-771b (
R⊕), TOI-771b ( R⊕), TOI-871b (
R⊕), TOI-871b ( R⊕), TOI-1467b (
R⊕), TOI-1467b ( R⊕), TOI-1739b (
R⊕), TOI-1739b ( R⊕), TOI-2068b (
R⊕), TOI-2068b ( R⊕), TOI-4559b (
R⊕), TOI-4559b ( R⊕), and TOI-5799b (
R⊕), and TOI-5799b ( R⊕). Among all these planets, six of them fall within the region known as ’keystone planets,’ which makes them particularly interesting for study. Based on the location of TOI-771b and TOI-4559b below the radius valley we characterized them as likely super-Earths, though radial velocity mass measurements for these planets will provide more details about their characterization. It is noteworthy that planets within the size range investigated herein are absent from our own solar system, making their study crucial for gaining insights into the evolutionary stages between Earth and Neptune.
R⊕). Among all these planets, six of them fall within the region known as ’keystone planets,’ which makes them particularly interesting for study. Based on the location of TOI-771b and TOI-4559b below the radius valley we characterized them as likely super-Earths, though radial velocity mass measurements for these planets will provide more details about their characterization. It is noteworthy that planets within the size range investigated herein are absent from our own solar system, making their study crucial for gaining insights into the evolutionary stages between Earth and Neptune.
 R
R R
R R
R R
R R
R R
R R
R R
RDelivery of a telehealth supported home exercise program with dietary advice to increase plant-based protein intake in people with non-alcoholic fatty liver disease: a 12-week randomised controlled feasibility trial
-
- Journal:
- British Journal of Nutrition , First View
- Published online by Cambridge University Press:
- 25 January 2024, pp. 1-11
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
ResearchMatch on FHIR: Development and evaluation of a recruitment registry and electronic health record system interface for volunteer profile completion
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 13 October 2023, e222
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Are We Adequately Assessing Delirium? An Analysis Of Liaison Psychiatry Referrals
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S518-S519
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Delirium is characterised by an acute, fluctuating change in cognition, attention and awareness (Wilson et al. Nature Reviews 2020; 6). This presentation can make the diagnosis of delirium extremely challenging to clinicians (Gofton., Canadian Journal of neurological sciences. 2011; 38 673-680). It is commonly reported in hospitalised patients, particularly in those over the age of sixty five (NICE. Delirium: prevention, diagnosis and management. 2010).
ObjectivesOur aim is to identify which investigations and cognitive assessments are completed prior to a referral to the liaison psychiatry services in patients with symptoms of delirium.
MethodsReferrals (N = 6012) to the liaison psychiatry team at Croydon University Hospital made between April and September 2022 were screened. Search parameters used to identify referrals related to a potential diagnosis of delirium were selected by the authors. The terms used were confusion; delirium; agitation; aggression; cognitive decline or impairment; disorientation; challenging behaviour. Data was collected on the completion rates of investigations for delirium as advised by the NICE clinical knowledge summaries. Further data was gathered on neuroimaging (CT or MRI), cognitive assessment tools (MOCA/MMSE) and delirium screening tools (4AT/AMTS).
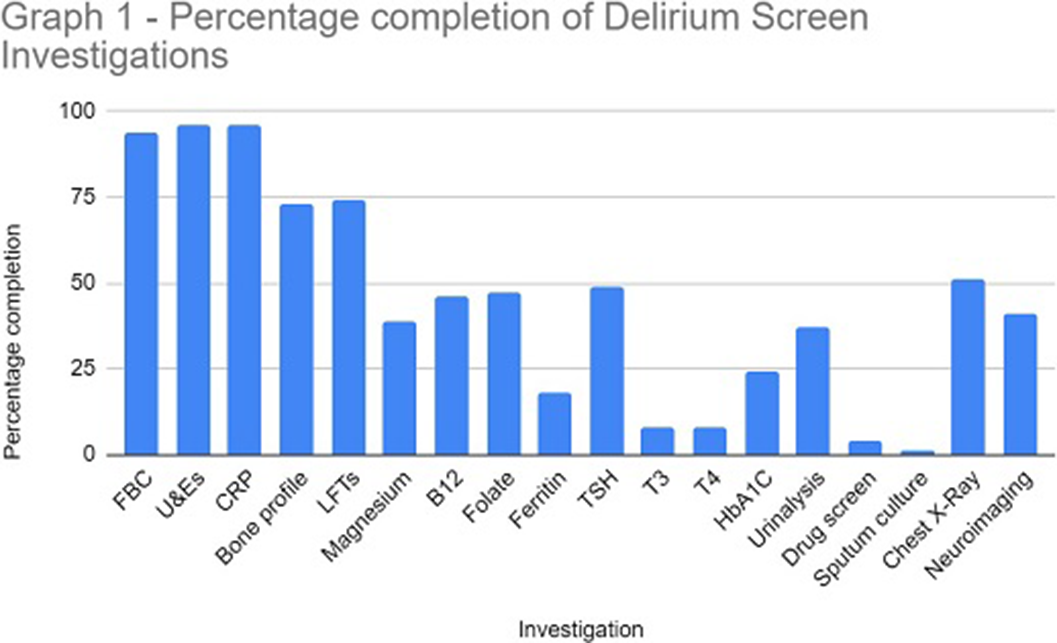
ResultsThe study sample identified 114 referrals (61 males and 53 females), with 82% over 65 years at the time of referral. In 96% of referrals, U&E and CRP were performed. Sputum culture (1%), urine toxin screen (4%) and free T3/4 (8%) were the tests utilised the least. Neuroimaging was completed in 41% of referrals (see Graph 1 for a full breakdown of results).
A formal cognitive assessment or delirium screening tool was completed in 32% of referrals. The AMTS and 4AT tools were documented for 65% and 24% respectively. A total of 19 referrals explicitly stated the patient was suspected to have dementia. A delirium screening tool was documented in 47% of these cases however, a formal cognitive assessment was documented in only 5% of these patients.
Following psychiatric assessment 47% of referrals were confirmed as delirium.
Image:
 Conclusions
ConclusionsOur data highlights the low level completion of the NICE recommended delirium screen prior to referral to liaison psychiatry. The effective implementation of a delirium screen and cognitive assessment is paramount to reduce the number of inappropriate psychiatric referrals in hospital and helps to identify reversible organic causes of delirium. This in turn will ensure timely treatment of reversible causes of delirium and reduce the length of hospital admission.
Disclosure of InterestNone Declared

Facing the COVID-19 pandemic – an assessment of students’ mental health and major coping strategies during the COVID-19 pandemic – an international study
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S152-S153
-
- Article
-
- You have access
- Open access
- Export citation
P.017 Convergent and contrasting modulation of saccade and pupil responses by several neurodegenerative diseases during free viewing of video clips
-
- Journal:
- Canadian Journal of Neurological Sciences / Volume 50 / Issue s2 / June 2023
- Published online by Cambridge University Press:
- 05 June 2023, p. S62
-
- Article
-
- You have access
- Export citation
The impact of strict lockdowns on the mental health and well-being of people living in Australia during the first year of the COVID-19 pandemic
-
- Journal:
- BJPsych Open / Volume 9 / Issue 3 / May 2023
- Published online by Cambridge University Press:
- 24 May 2023, e90
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Examining the impact of racial disparities on Clostridioides difficile infection outcomes at a Southern California academic teaching hospital
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 11 / November 2023
- Published online by Cambridge University Press:
- 04 May 2023, pp. 1861-1865
- Print publication:
- November 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
39 Prenatal antibiotic exposure and risk of childhood asthma among children with Down syndrome
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue s1 / April 2023
- Published online by Cambridge University Press:
- 24 April 2023, p. 10
-
- Article
-
- You have access
- Open access
- Export citation
Dietary resistant starch alters gut microbiota, microbially produced metabolites and albuminuria in diabetic mice
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E183
-
- Article
-
- You have access
- HTML
- Export citation
Screen to Intervene; establishing a dedicated metabolic clinic for patients with chronic mental illness in an Irish Metal Health Service
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, pp. S198-S199
-
- Article
-
- You have access
- Open access
- Export citation
Resting-state EEG networks characterized by intramodular and global hyperconnectivity in depressive sample
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, pp. S213-S214
-
- Article
-
- You have access
- Open access
- Export citation
Beta-band network modularity in resting-state EEG negatively correlates with level of intelligence
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S639
-
- Article
-
- You have access
- Open access
- Export citation
Stability of Fe Electrode in Alkaline Electrolyte
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 830-832
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Beyond In Situ ETEM Imaging: Unveiling the Size-dependent Oxidation Mechanism of Metallic Nanoparticles by Individual Nanoparticle-level Oxidation Kinetic Analysis
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 160-161
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Convolutional Neural Network as a Solution to Segment and Classify High Resolution TEM Images to Obtain 3D Information
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 3024-3026
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Field Experiments in the Global South: Assessing Risks, Localizing Benefits, and Addressing Positionality—ADDENDUM
-
- Journal:
- PS: Political Science & Politics / Volume 55 / Issue 4 / October 2022
- Published online by Cambridge University Press:
- 15 July 2022, p. 835
- Print publication:
- October 2022
-
- Article
- Export citation
P.002 Saccade parameters reveal cognitive impairment and differentially associate with cognitive domains across neurodegenerative diseases
-
- Journal:
- Canadian Journal of Neurological Sciences / Volume 49 / Issue s1 / June 2022
- Published online by Cambridge University Press:
- 24 June 2022, p. S8
-
- Article
-
- You have access
- Export citation
Frontal sinus obliteration with beta-tricalcium phosphate putty: case series with long-term radiological follow up
-
- Journal:
- The Journal of Laryngology & Otology / Volume 137 / Issue 2 / February 2023
- Published online by Cambridge University Press:
- 20 June 2022, pp. 163-168
- Print publication:
- February 2023
-
- Article
- Export citation
