
43 results
Changes in evening-shifted loss of control eating severity following treatment for binge-eating disorder
-
- Journal:
- Psychological Medicine , First View
- Published online by Cambridge University Press:
- 28 February 2024, pp. 1-8
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A novel remote assessment pathway to streamline the management of two-week-wait suspected head and neck cancer referrals: a prospective analysis of 660 patients
-
- Journal:
- The Journal of Laryngology & Otology , First View
- Published online by Cambridge University Press:
- 19 January 2024, pp. 1-5
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The relative effects of parental alcohol use disorder and maltreatment on offspring alcohol use: Unique pathways of risk
-
- Journal:
- Development and Psychopathology , First View
- Published online by Cambridge University Press:
- 31 October 2023, pp. 1-12
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Child maltreatment and youth suicide risk: A developmental conceptual model and implications for suicide prevention
-
- Journal:
- Development and Psychopathology / Volume 35 / Issue 4 / October 2023
- Published online by Cambridge University Press:
- 13 September 2022, pp. 1732-1755
-
- Article
- Export citation
The attention atlas virtual reality platform maps three-dimensional (3D) attention in unilateral spatial neglect patients: a protocol
-
- Journal:
- Brain Impairment / Volume 24 / Issue 3 / December 2023
- Published online by Cambridge University Press:
- 30 May 2022, pp. 548-567
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Retrospective cohort analysis of the safety of outpatient parenteral antimicrobial therapy (OPAT) in an academic hospital
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s59
-
- Article
-
- You have access
- Open access
- Export citation
-
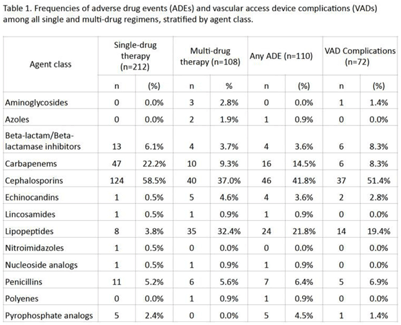
Background: Although many infectious conditions can be safely treated with oral antimicrobials, select circumstances require parenteral antimicrobial therapy. Benefits of OPAT include prevention of hospital-associated conditions and significant cost savings. However, risks of OPAT include adverse drug events (ADEs) and vascular access device (VAD) complications. We analyzed the safety of OPAT regimens as part of implementing a collaborative OPAT program. Methods: We reviewed adult patients discharged home from an academic hospital between January 2019 and June 2021. Patients with cystic fibrosis were excluded. Data on OPAT agents, ADEs, and VAD complications were collected from electronic medical records by 2 reviewers using a standardized REDCap instrument. The institutional review board approved this study. Results: The cohort comprised 265 unique patients; 212 (80%) received single-drug therapy and 53 (20%) received multidrug therapy. In total, 81 patients (31%), who received a total of 110 antimicrobials, experienced an ADE. In total, 55 patients (21%), who received a total of 72 antimicrobials, experienced a VAD complication. Patients who received >1 antimicrobial were more likely to experience an ADE (53% vs 25%; P = .0002) or a VAD complication (32% vs 18%; P = .04). Cephalosporins were the most frequently prescribed antimicrobial class (Table 1). Conclusions: ADEs and VAD complications were frequent in patients on OPAT. Local data should inform (1) the selection of OPAT therapy and (2) the standardized monitoring of patients who receive OPAT going forward in the implementation of this collaborative OPAT program.
Funding: None
Disclosures: None

102 Characterization of Hub and Spoke Facilities for Study of Surgical Care within United States Health Systems
-
- Journal:
- Journal of Clinical and Translational Science / Volume 6 / Issue s1 / April 2022
- Published online by Cambridge University Press:
- 19 April 2022, p. 1
-
- Article
-
- You have access
- Open access
- Export citation
South Africa’s Health Promotion Levy on pricing and acquisition of beverages in small stores and supermarkets
-
- Journal:
- Public Health Nutrition / Volume 25 / Issue 5 / May 2022
- Published online by Cambridge University Press:
- 07 March 2022, pp. 1300-1309
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Trends in referrals to liaison psychiatry teams from UK emergency departments for patients over 65
-
- Journal:
- BJPsych Open / Volume 7 / Issue S1 / June 2021
- Published online by Cambridge University Press:
- 18 June 2021, pp. S311-S312
-
- Article
-
- You have access
- Open access
- Export citation
Chapter 9 - Hemolytic Disease of the Fetus and Newborn
- from Section III - Erythrocyte Disorders
-
-
- Book:
- Neonatal Hematology
- Published online:
- 30 January 2021
- Print publication:
- 18 February 2021, pp 133-154
-
- Chapter
- Export citation
Learning from health system reform trajectories in seven Canadian provinces
-
- Journal:
- Health Economics, Policy and Law / Volume 16 / Issue 4 / October 2021
- Published online by Cambridge University Press:
- 06 August 2020, pp. 383-399
-
- Article
- Export citation
Absorption and metabolism of isothiocyanates formed from broccoli glucosinolates: effects of BMI and daily consumption in a randomised clinical trial
-
- Journal:
- British Journal of Nutrition / Volume 120 / Issue 12 / 28 December 2018
- Published online by Cambridge University Press:
- 30 November 2018, pp. 1370-1379
- Print publication:
- 28 December 2018
-
- Article
-
- You have access
- HTML
- Export citation
Trainee experiences of intellectual disability psychiatry and an innovative leaderless support group: A qualitative study
-
- Journal:
- BJPsych Bulletin / Volume 41 / Issue 4 / August 2017
- Published online by Cambridge University Press:
- 02 January 2018, pp. 228-233
- Print publication:
- August 2017
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Chapter 12 - Anthologizing Early Modern Women's Poetry
- from Part III - Out of the Archives, into the Classroom
-
-
- Book:
- Editing Early Modern Women
- Published online:
- 05 August 2016
- Print publication:
- 21 July 2016, pp 215-231
-
- Chapter
- Export citation
Contributors
-
-
- Book:
- Trauma Anesthesia
- Published online:
- 05 April 2015
- Print publication:
- 09 April 2015, pp vii-x
-
- Chapter
- Export citation
Contributors
-
-
- Book:
- The Cambridge Companion to Modernist Culture
- Published online:
- 05 November 2014
- Print publication:
- 27 October 2014, pp xi-xiv
-
- Chapter
- Export citation
TRACKING CHANGES IN STATES OF CONTRACEPTIVE USE OVER TIME IN SUB-SAHARAN AFRICA THROUGH COHORT AND PERIOD ANALYSES
-
- Journal:
- Journal of Biosocial Science / Volume 47 / Issue 3 / May 2015
- Published online by Cambridge University Press:
- 27 March 2014, pp. 329-344
-
- Article
- Export citation
Experimental Taphonomy of Foraminifera
-
- Journal:
- The Paleontological Society Special Publications / Volume 13 / 2014
- Published online by Cambridge University Press:
- 26 July 2017, pp. 122-123
- Print publication:
- 2014
-
- Article
- Export citation
List of Contributors
-
-
- Book:
- The Cambridge Companion to Ancient Mediterranean Religions
- Published online:
- 05 December 2013
- Print publication:
- 25 November 2013, pp xi-xi
-
- Chapter
- Export citation
6 - Hemolytic disease of the fetus and newborn
- from Section II - Erythrocyte disorders
-
-
- Book:
- Neonatal Hematology
- Published online:
- 05 February 2013
- Print publication:
- 10 January 2013, pp 65-90
-
- Chapter
- Export citation
