
659 results
The Future of Qualitative Research in Healthcare
- The Role and Management of Digital Methods
- Coming soon
-
- Expected online publication date:
- November 2024
- Print publication:
- 30 November 2024
-
- Book
- Export citation
Testing maternal effects of vitamin-D and omega-3 levels on offspring neurodevelopmental traits in the Norwegian Mother, Father and Child Cohort Study
-
- Journal:
- Psychological Medicine , First View
- Published online by Cambridge University Press:
- 09 September 2024, pp. 1-11
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
An Audit of the First Stage of Service Development Initiatives Undertaken as Part of a Quality Improvement Process to Improve the Screening and Management of Older Adults Presenting With Delirium in Queen's Hospital (NELFT)
-
- Journal:
- BJPsych Open / Volume 10 / Issue S1 / June 2024
- Published online by Cambridge University Press:
- 01 August 2024, p. S159
-
- Article
-
- You have access
- Open access
- Export citation
BRUTALISED, BOUND AND BLED: A CASE OF LATER IRON AGE HUMAN SACRIFICE FROM WINTERBORNE KINGSTON, DORSET
-
- Journal:
- The Antiquaries Journal , First View
- Published online by Cambridge University Press:
- 14 May 2024, pp. 1-27
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Our experience of a Speech and Language Therapist led Swallow Disorder Clinic
-
- Journal:
- The Journal of Laryngology & Otology / Accepted manuscript
- Published online by Cambridge University Press:
- 30 April 2024, pp. 1-15
-
- Article
- Export citation
Head and Neck Cancer: United Kingdom National Multidisciplinary Guidelines, Sixth Edition
-
- Journal:
- The Journal of Laryngology & Otology / Volume 138 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 14 March 2024, pp. S1-S224
- Print publication:
- April 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Endocannabinoid levels in plasma and neurotransmitters in the brain: a preliminary report on patients with a psychotic disorder and healthy individuals
-
- Journal:
- Psychological Medicine , First View
- Published online by Cambridge University Press:
- 23 February 2024, pp. 1-11
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Highly pathogenic avian influenza causes mass mortality in Sandwich Tern Thalasseus sandvicensis breeding colonies across north-western Europe
-
- Journal:
- Bird Conservation International / Volume 34 / 2024
- Published online by Cambridge University Press:
- 02 February 2024, e6
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The predictive role of symptoms in COVID-19 diagnostic models: A longitudinal insight
-
- Journal:
- Epidemiology & Infection / Volume 152 / 2024
- Published online by Cambridge University Press:
- 22 January 2024, e37
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Striving to be the fittest: quantitative P2/N95 respirator fit test results among hospital staff during the COVID-19 pandemic
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 15 December 2023, e233
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Sentience: The Invention of Consciousness By Nicholas Humphrey Oxford University Press. 2022. £16.99 (hb). 256 pp. ISBN 9780198858539
-
- Journal:
- The British Journal of Psychiatry / Volume 223 / Issue 4 / October 2023
- Published online by Cambridge University Press:
- 17 October 2023, pp. 494-495
- Print publication:
- October 2023
-
- Article
- Export citation
Hyperendemic carbapenem-resistant Acinetobacter baumannii at a hospital in Botswana: Insights from whole-genome sequencing
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s115-s116
-
- Article
-
- You have access
- Open access
- Export citation
-
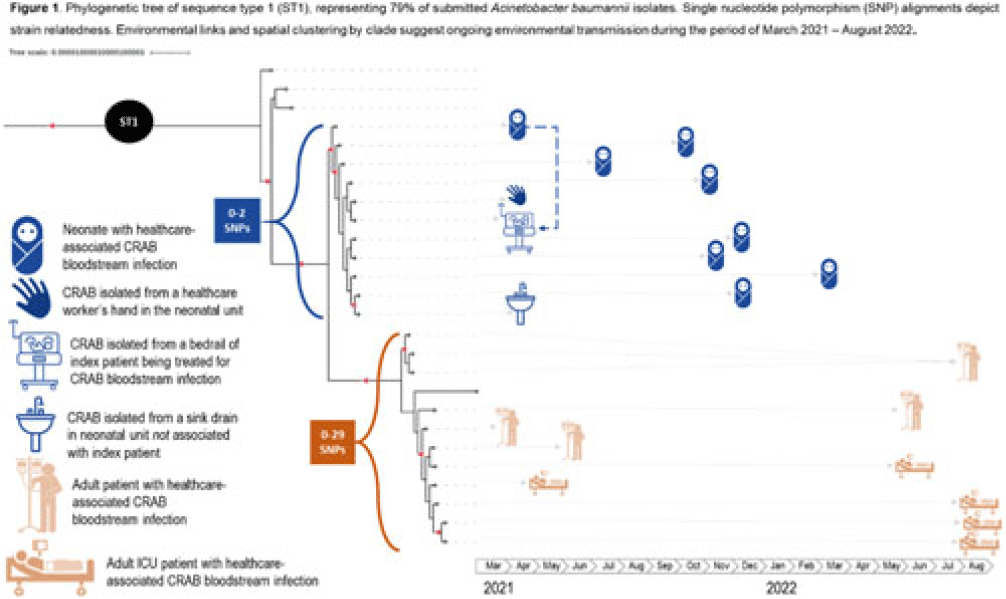
Background: Carbapenem-resistant Acinetobacter baumannii (CRAB) has emerged as a major cause of bloodstream infection among hospitalized patients in low- and middle-income countries (LMICs). CRAB infections can be difficult to treat and are devastating in neonates (~30% mortality). CRAB outbreaks are hypothesized to arise from reservoirs in the hospital environment, but outbreak investigations in LMICs seldom incorporate whole-genome sequencing (WGS). Methods: WGS (Illumina NextSeq) was performed at the National Institute for Communicable Diseases (South Africa) on 43 preserved A. baumannii isolates from a 530-bed referral hospital in Gaborone, Botswana, from March 2021–August 2022. This included 23 blood-culture isolates from 21 unique patients (aged 2 days–69 years) and 20 environmental isolates collected at the 36-bed neonatal unit in April–June 2021. Infections were considered healthcare-associated if the culture was obtained >72 hours after hospital arrival (or sooner in inborn infants). Blood cultures were incubated using an automated system (BACT/ALERT, BioMérieux) and were identified using manual methods. Environmental isolates were identified using selective or differential chromogenic media (CHROMagarTM). Taxonomic assignment, multilocus sequence typing (MLST), antimicrobial resistance gene identification, and phylogenetic analyses were performed using publicly accessible analysis pipelines. Single-nucleotide polymorphism (SNP) matrices were used to assess clonal lineage. Results: All 23 blood isolates and 5 (25%) of 20 environmental isolates were confirmed as A. baumannii; thus, 28 A. baumannii isolates were included in the phylogenetic analysis. MLST revealed that 22 (79%) of 28 isolates were sequence type 1 (ST1), including all 19 healthcare-associated blood isolates and 3 (60%) of 5 environmental isolates. Genes encoding for carbapenemases (blaNDM-1, blaOXA-23) and biocide resistance (qacE) were present in all 22 ST1 isolates; colistin resistance genes were not identified. Phylogenetic analysis of the ST1 clade demonstrated spatial clustering by hospital unit. Related isolates spanned wide ranges in time (>1 year), suggesting ongoing transmission from environmental sources (Fig. 1). An exclusively neonatal clade (0–2 SNPs) containing all 8 neonatal blood isolates was closely associated with 3 environmental isolates from the neonatal unit: a sink drain, bed rail, and a healthcare worker’s hand. Conclusions: WGS analysis of clinical and environmental A. baumannii revealed the presence of unit-specific CRAB clones, with evidence of ongoing transmission likely driven by persistent environmental reservoirs. This research highlights the potential of WGS to detect hospital outbreaks and reaffirms the importance of environmental sampling to identify and remediate reservoirs (eg, sinks) and vehicles (eg, hands and equipment) within the healthcare environment.
Disclosures: None

An approach for collaborative development of a federated biomedical knowledge graph-based question-answering system: Question-of-the-Month challenges
-
- Journal:
- Journal of Clinical and Translational Science / Volume 7 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 14 September 2023, e214
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The Expression of the Emotions in Man and Animals: Darwin's forgotten masterpiece
-
- Journal:
- BJPsych Advances / Volume 30 / Issue 3 / May 2024
- Published online by Cambridge University Press:
- 11 September 2023, pp. 192-194
- Print publication:
- May 2024
-
- Article
- Export citation
The Fragility of Peace: Song China's Northwestern Frontier and Erosion of the Chanyuan Paradigm in the Mid-Eleventh Century
-
- Journal:
- Journal of Chinese History , First View
- Published online by Cambridge University Press:
- 05 September 2023, pp. 1-29
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Agricultural Research Service Weed Science Research: Past, Present, and Future
-
- Journal:
- Weed Science / Volume 71 / Issue 4 / July 2023
- Published online by Cambridge University Press:
- 16 August 2023, pp. 312-327
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Developing a Neuromodulation Approach for Treating Working Memory Deficits in Severe Mental Illness
-
- Journal:
- BJPsych Open / Volume 9 / Issue S1 / July 2023
- Published online by Cambridge University Press:
- 07 July 2023, pp. S46-S47
-
- Article
-
- You have access
- Open access
- Export citation
Quality Improvement Project on Improving Patient and Family Experience in Psychiatric Inpatient Unit at Derby (Tissington House)
-
- Journal:
- BJPsych Open / Volume 9 / Issue S1 / July 2023
- Published online by Cambridge University Press:
- 07 July 2023, pp. S104-S105
-
- Article
-
- You have access
- Open access
- Export citation
Banging the drum: evolutionary and cultural origins of music and its implications for psychiatry
-
- Journal:
- BJPsych Bulletin / Volume 47 / Issue 5 / October 2023
- Published online by Cambridge University Press:
- 14 June 2023, pp. 251-254
- Print publication:
- October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Reciprocity, Incentives, and Off-Ramps: Faculty–Undergraduate Collaboration and Comparative Politics Research
-
- Journal:
- PS: Political Science & Politics / Volume 56 / Issue 4 / October 2023
- Published online by Cambridge University Press:
- 28 April 2023, pp. 475-480
- Print publication:
- October 2023
-
- Article
- Export citation
