1 Clinical Commentary/Editor’s Summary
Though progress in the practice of obstetrics over the past 50 years has significantly reduced the rate of stillbirth, especially intrapartum, stillbirths still occur and often without apparent warning. This Element examines the frequency of stillbirth, risk factors for it, and causes of the death. It reviews the impact of proactive interventions before and during pregnancy to lower rates. Finally, and arguably most importantly, clinical management of a pregnancy affected by this tragedy is discussed.
The most common etiologies of stillbirth include abrupt obstetrical complications, placental and umbilical cord abnormalities, fetal genetic or structural anomalies, infection, and hypertensive disorders. While fetal growth restriction is a significant risk factor, it is notable that more than half of nonanomalous stillbirths are appropriate for gestational age. Diagnostic evaluation is therefore crucial; genetic testing identifies a cause in 8% of structurally normal fetuses and in over 20% of those with anomalies. Despite this, only 20% of stillbirths have some type of fetal autopsy. This diagnostic gap creates a “knowledge void,” limiting the clinician’s ability to provide closure to grieving parents or to construct evidence-based management plans for subsequent high-risk pregnancies.
2 Definitions of Stillbirth
The US National Center for Health Statistics (NCHS) defines stillbirth as an intrauterine fetal death of ≥ 20 weeks’ gestational age, or should the gestational age be unknown, a fetal weight of ≥ 350 grams, which is the 50th percentile of weight at 20 weeks’ gestation.Reference Gregory, Valenzuela and Hoyert1 Fetal death at < 20 weeks’ gestational age (or < 350 grams if the gestational age is unknown) is classified as a spontaneous abortion.Reference Gregory, Valenzuela and Hoyert1 The stillbirth definition can be further categorized by the gestational age at which death occurred: Early stillbirth occurs between 20 and 27 6/7 weeks, late stillbirth occurs between 28 and 36 6/7 weeks, and term stillbirth occurs at ≥ 37 weeks.Reference Gregory, Valenzuela and Hoyert1 Pregnancy losses due to elective termination, induction for lethal fetal anomalies, or induction after previable premature rupture of membranes are excluded from the definition of fetal death and associated statistics. The definition of stillbirth does vary across countries. The World Health Organization (WHO) defines stillbirth as intrauterine fetal death after 28 weeks of pregnancy.Reference Frøen, Lawn, Heazell, Flenady, de Bernis and Kinney2
3 Epidemiology
Worldwide, stillbirth at ≥ 28 weeks’ gestation complicated approximately 1.9 million pregnancies in 2021, with 40% occurring intrapartum.3 The rate of stillbirth is highest in sub-Saharan Africa and South Asia, with these two regions accounting for three-quarters of all stillbirths at ≥ 28 weeks. In sub-Saharan Africa, the stillbirth rate of 21.0 per 1,000 total births is seven-times higher than the lowest regional rate of 2.9 per 1,000 total births found in Europe, Northern America, Australia, and New Zealand. Countries with the highest rates of stillbirth include India, Pakistan, Nigeria, the Democratic Republic of Congo, Ethiopia, and Bangladesh. These six countries accounted for almost half of the estimated stillbirths, but only 36% of global live births.3 Arguably of greater concern, sub-Saharan Africa’s portion of the global number of stillbirths increased from 26% in 2000 to 45% in 2021.
In the United States, a total of 21,105 stillbirths were reported in 2021, with a stillbirth rate of 5.73 per 1,000 total births, a rate higher than comparative high-resource countries.Reference Gregory, Valenzuela and Hoyert1 The stillbirth rate at 20–27 weeks’ gestation was 2.95 per 1,000 total births, which is a similar to the rate at ≥ 28 weeks’ gestation of 2.80 per 1,000 total births.Reference Gregory, Valenzuela and Hoyert1
4 Risk Factors
Many risk factors and possible etiologies have been associated with stillbirth. These include nulliparity, maternal age, non-Hispanic Black race, tobacco or alcohol use, obesity, pregestational diabetes, hypertension, multiple gestation, and prior poor pregnancy history (in particular, fetal growth restriction or stillbirth). Table 1 highlights the stillbirth rates according to risk factors.
| Risk factor | Estimated rate of stillbirth per 1,000 |
|---|---|
| All pregnanciesFootnote a | 5.73 |
| Chronic hypertensionFootnote b | 6–25 |
| Preeclampsia without severe featuresFootnote b | 9–51 |
| Preeclampsia with severe featuresFootnote b | 12–29 |
| Fetal growth restrictionFootnote b | 10–47 |
| OligohydramniosFootnote b | 14 |
| Gestational diabetes on dietFootnote b | 6–10 |
| Gestational diabetes on insulinFootnote b | 6–35 |
| TwinsFootnote a | 12.37 |
| Triplets or higher-orderFootnote a | 27.84 |
| Previous stillbirthFootnote b | 9–20 |
| Decreased fetal movementFootnote b | 13 |
| Systemic lupus erythematosusFootnote b | 40–150 |
| Renal diseaseFootnote b | 15–200 |
| Cholestasis of pregnancyFootnote b | 12–30 |
| Maternal age < 15 yearsFootnote a | 13.14 |
| Maternal age 15–19 yearsFootnote a | 7.19 |
| Maternal age 35–39 yearsFootnote a | 6.28 |
| Maternal age 40–44 yearsFootnote a | 8.52 |
| Maternal age ≥ 45 yearsFootnote a | 11.36 |
| Black maternal race (non-Hispanic)Footnote a | 9.89 |
| Body mass index > 30 kg/mReference Frøen, Lawn, Heazell, Flenady, de Bernis and Kinney2Footnote b | 13–18 |
| SmokingFootnote a | 9.62 |
a Data adapted from.Reference Gregory, Valenzuela and Hoyert1
b Data adapted from.Reference Signore, Freeman and Spong4
4.1 Social/Demographic Factors
4.1.1 Maternal Age
Stillbirth risk and maternal age follow a U-shaped curve, with the highest rates for those under the age of 15 (13.14 per 1,000 total births) and at or over the age of 45 (11.36 per 1,000 total births).Reference Gregory, Valenzuela and Hoyert1 These rates are two- to three-fold higher than women aged 30–34 years, who comprise the nadir of the U-shaped curve for stillbirth risk (5.13 per 1,000 total births).Reference Gregory, Valenzuela and Hoyert1 The higher rates at the extremes of maternal age are not entirely understood. In women of advanced maternal age, the increased stillbirth risk persists even when adjusting for medical comorbidities, parity, race, ethnicity, and fetal anomalies.Reference Reddy, Ko and Willinger5
4.1.2 Racial Disparities
There is significant racial disparity among US stillbirth rates, ranging from 3.94 per 1,000 total births for Asian individuals to 4.85 for non-Hispanic White individuals to 8.89 for non-Hispanic Black individuals in 2021.Reference Gregory, Valenzuela and Hoyert1 Among those of Hispanic ethnicity, the 2021 US stillbirth rate was 4.82 per 1,000 total birth.Reference Gregory, Valenzuela and Hoyert1 With these disparities in mind, a multisite prospective population-based, case-control study by the Eunice Kennedy Shriver National Institute of Child Health and Human Development Stillbirth Collaborative Research Network (SCRN) demonstrated that the higher proportion of stillbirths occurring in non-Hispanic Black women compared to the non-Hispanic White and Hispanic women was associated with obstetric complications (43.5% vs. 23.7%; p < 0.001) and infections (25.2% vs. 7.8%; p < 0.001).6
Racial disparities in stillbirth rates were demonstrated even among those with comparable prenatal care and high education levels.Reference Vintzileos, Ananth, Smulian, Scorza and Knuppel7,Reference Willinger, Ko and Reddy8 These racial disparities in stillbirth rates may be a downstream effect of structural, institutional, and interpersonal racism that impact access to health care.Reference Debbink, Stanhope and Hogue9 Structural racism is defined as the totality of ways in which societies foster racial discrimination through mutually reinforcing systems of housing, education, employment, earnings, benefits, credit, media, health care, and criminal justice.Reference Bailey, Krieger, Agénor, Graves, Linos and Bassett10 There is a growing body of literature supporting the replacement of race with racism as a risk factor for adverse perinatal conditions.Reference Ramos, Werner, Bird, Amutah-Onukagha and Siegel11,Reference Williams, Wallace, Nobles and Mendola12
4.1.3 Substance Use
The US stillbirth rate for pregnant smokers was more than 1.5-fold higher than nonsmokers during pregnancy (9.62 compared to 5.08 per 1,000 total births).Reference Gardosi, Madurasinghe, Williams, Malik and Francis13 Smoking in pregnancy has a clear dose–response effect, and quitting smoking is protective.Reference Marufu, Ahankari, Coleman and Lewis14 Pregnancies complicated by illicit drug use also had an increased risk of stillbirth (adjusted odds ratio [aOR] 1.94; 95% confidence interval [CI] 1.16–3.27).Reference Varner, Silver, Rowland Hogue, Willinger, Parker and Thorsten15 Cannabis use, which is increasing with legalization in the United States, has also been associated with an increased risk of stillbirth (odds ratio [OR] 2.34; 95% CI 0.13–4.81).Reference Varner, Silver, Rowland Hogue, Willinger, Parker and Thorsten15
4.2 Maternal History
4.2.1 Pregnancy History
Pregnancy history is the single strongest risk factor for stillbirth.16 Nulliparity and history of early-onset fetal growth restriction or stillbirth in a prior pregnancy independently increase the stillbirth risk. Compared to multiparous women without a history of pregnancy losses, increasing risks of stillbirth were noted in: nulliparas with an aOR of 1.98 (95% CI 1.51–2.60), nulliparas with previous losses at < 20 weeks’ gestation with an aOR of 3.13 (95% CI 2.06–4.75), and finally multiparas with a previous stillbirth with an aOR of 5.91 (95% CI 3.18–11.00).16 Multiparous women with prior pregnancy losses at < 20 weeks’ gestation did not have an increased risk of stillbirth. A history of a small-gestational-age infant born at < 34 weeks’ gestation was associated with an increased risk of stillbirth in subsequent pregnancies (OR 6.00; 95% CI 3.43–10.49).Reference Townsend, Sileo, Allotey, Dodds, Heazell and Jorgensen17
4.2.2 Maternal Obesity
Maternal obesity, defined as a prepregnancy body mass index, BMI, of > 30 kg/mReference Frøen, Lawn, Heazell, Flenady, de Bernis and Kinney2, not only increases the risk for hypertension and diabetes but is also an independent risk factor for stillbirth. There is a dose–dependent response to BMI and stillbirth risk as well. Compared to a normal BMI of < 25 kg/mReference Frøen, Lawn, Heazell, Flenady, de Bernis and Kinney2, women with a BMI of 25–30 kg/mReference Frøen, Lawn, Heazell, Flenady, de Bernis and Kinney2 had an aOR of 1.43 (95% CI 1.09–1.88), women with a BMI of 30–34 kg/mReference Frøen, Lawn, Heazell, Flenady, de Bernis and Kinney2 had an aOR of 1.72 (95% CI 1.22–2.43), and women with a BMI of > 35 kg/mReference Frøen, Lawn, Heazell, Flenady, de Bernis and Kinney2 had an aOR of 1.73 (95% CI 1.23–2.45).18 A meta-analysis of 38 studies that included 16,274 stillbirths noted absolute risks per 10,000 pregnancies of 40 (reference standard) for BMI level 20 kg/mReference Frøen, Lawn, Heazell, Flenady, de Bernis and Kinney2, 48 (95% CI 46–51) for BMI level 25 kg/mReference Frøen, Lawn, Heazell, Flenady, de Bernis and Kinney2, and 59 (95% CI 55–63) for BMI level 30 kg/mReference Frøen, Lawn, Heazell, Flenady, de Bernis and Kinney2.Reference Aune, Saugstad, Henriksen and Tonstad19
4.2.3 Multifetal Gestation
Compared to the stillbirth rate of 5.49 per 1,000 total births in singleton pregnancies, the stillbirth rate for twins is 2.5-fold higher (12.37 per 1,000 total births) and for triplets or higher-order multiples fivefold higher (27.84 per 1,000 total births).Reference Gregory, Valenzuela and Hoyert1 Compared to dichorionic twins, the stillbirth rate of monochorionic twins is approximately twofold higher due to abnormalities of placentation (twin-to-twin transfusion syndrome, selective growth restriction) and increased risk of aneuploidy and congenital anomalies.Reference Cheong-See, Schuit, Arroyo-Manzano, Khalil, Barrett and Joseph20 Since the stillbirth risk increases in all multiple gestations with advancing gestational age, delivery is often recommended before the estimated due date to reduce the risk of stillbirth.Reference Cheong-See, Schuit, Arroyo-Manzano, Khalil, Barrett and Joseph20
5 Pathogenesis
With the nonuniformity in data reporting and the multifactorial processes potentially involved in the pathogenesis of stillbirth, identifying the likely cause of a given stillbirth can be challenging. The Initial Causes of Fetal Death Evaluation (INCODE) algorithm was developed by the SCRN investigators as a standardized classification system to assign probable and possible causes of stillbirth based on information routinely collected during prenatal care and clinical evaluation of fetal death.Reference Dudley, Goldenberg, Conway, Silver, Saade and Varner21
Stillbirth etiologies are further categorized into probable cause, possible cause, and present cause. A condition is a probable cause of stillbirth if it has a high likelihood of directly causing fetal death. If a condition was not a direct cause of the stillbirth but possibly involved in a pathophysiologic sequence that led to the fetal death, it is considered a possible cause. A present cause is a condition that is documented but in remission, controlled with medications, or not deemed to be involved in the etiology of fetal death.Reference Dudley, Goldenberg, Conway, Silver, Saade and Varner21 For example, diabetes would be a probable cause if the fetus had diabetic embryopathy or if the stillbirth occurred during an episode of maternal diabetic ketoacidosis; a possible cause if the mother had poor glycemic control and the fetus had abnormal growth; and a present condition if the diabetic mother had good glycemic control and the fetus had no other abnormalities. Present conditions are potential risk factors for, rather than causes of, stillbirth.
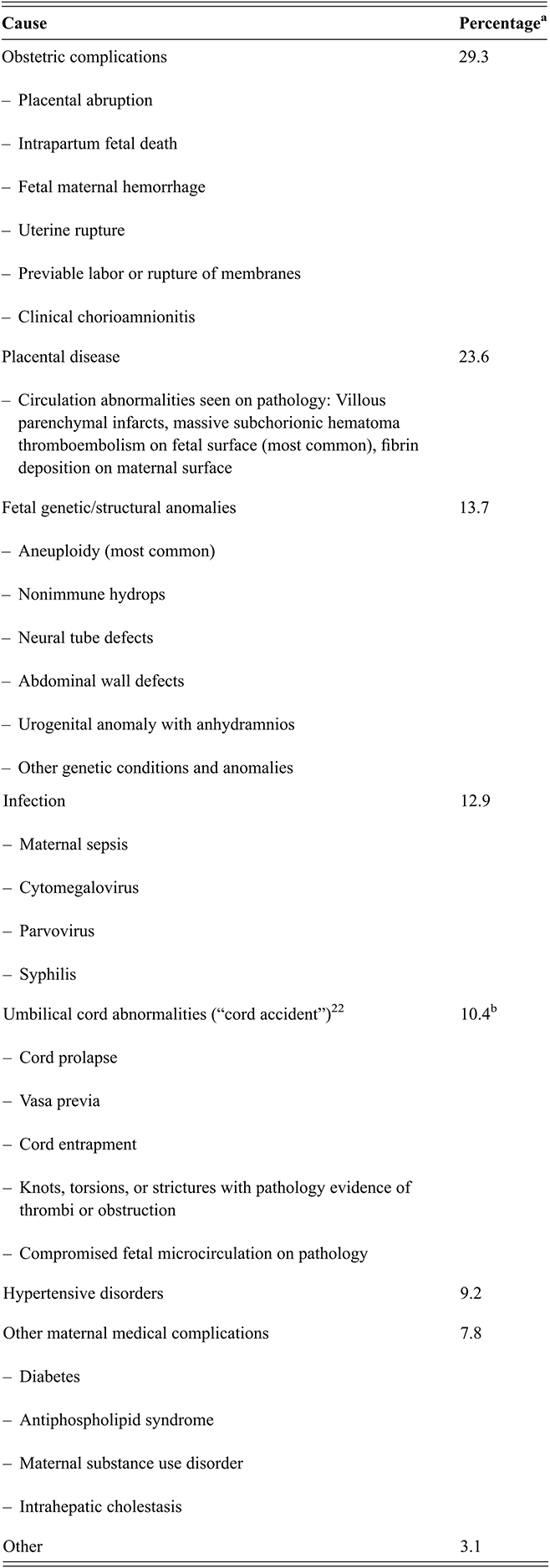
A “probable cause of stillbirth” was identified in approximately 61% of cases and a “possible” or “probable cause of stillbirth” was found in 76% of cases in the SCRN study.6 Table 2 highlights the breakdown of most common probable or possible causes of stillbirth in that study.
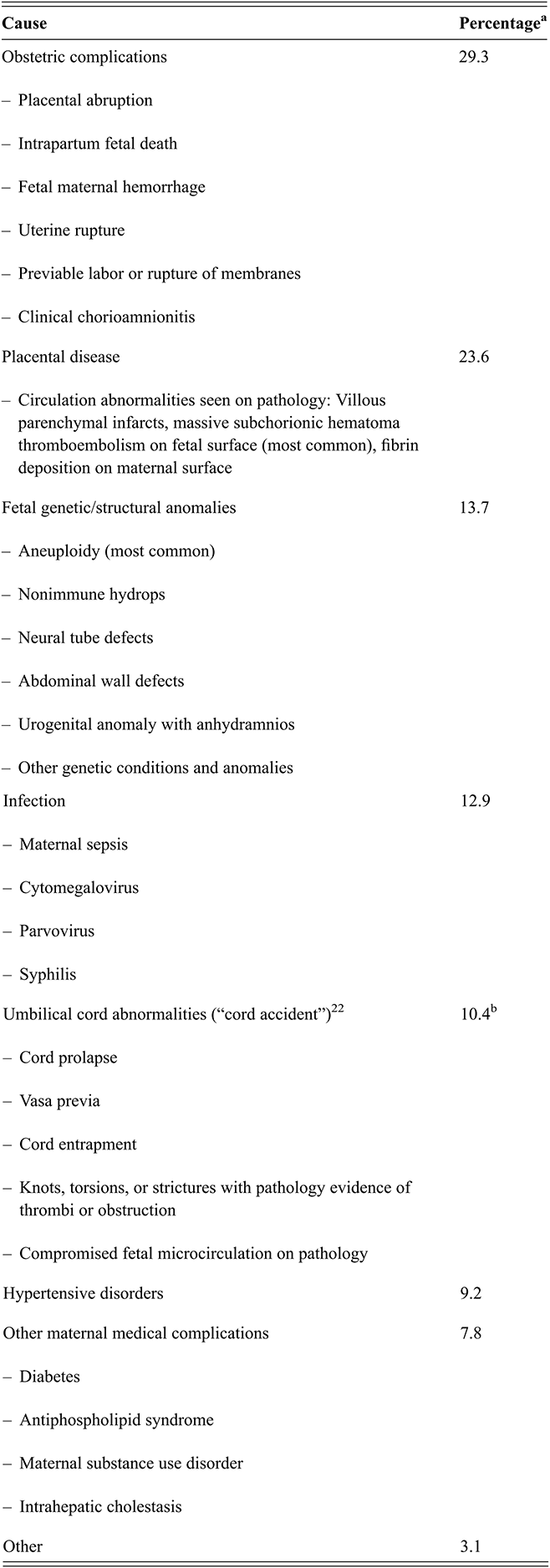
Table 2 Long description
The table consists of two columns: cause and percentage. Percentage is followed by an asterisk, which indicates that some stillbirths had more than 1 probable cause. The row-wise data is as follows. Row 1. Obstetric Complications: placental abruption, intrapartum fetal death, fetal maternal hemorrhage, uterine rupture, previable labor or rupture of membranes, clinical chorioamnionitis; 29.3%. Row 2. Placental disease: circulation abnormalities seen on pathology: villous parenchymal infarcts, massive subchorionic hematoma thromboembolism on fetal surface (most common), fibrin deposition on maternal surface; 23.6%. Row 3. Fetal genetic/structural anomalies: aneuploidy (most common), non-immune hydrops, neural tube defects, abdominal wall defects, urogenital anomaly with anhydramnios, other genetic conditions and anomalies; 13.7%. Row 4. Infection: maternal sepsis, cytomegalovirus, parvovirus, syphilis; 12.9%. Row 5. Umbilical cord abnormalities (cord accident) (Hammad et al., 2020): cord prolapse, vasa previa, cord entrapment, knots, torsions, or strictures with pathology evidence of thrombi or obstruction, compromised fetal microcirculation on pathology; 10.4% and followed by double asterisks that read umbilical vein thrombosis was not included in original analysis. Inclusion of umbilical vein thrombosis increases the rate of umbilical cord abnormality-associated stillbirth to 19% (20). Row 6. Hypertensive disorders: 9.2%. Row 7. Other maternal medical complications: diabetes, antiphospholipid syndrome, maternal substance use disorder, intrahepatic cholestasis; 7.8%. Row 8. Other: 3.1%.
a Some stillbirths had more than one probable cause.
b Umbilical vein thrombosis was not included in the original analysis. Inclusion of umbilical vein thrombosis increases the rate of umbilical cord abnormality-associated stillbirth to 19%.Reference Hammad, Blue, Allshouse, Silver, Gibbins and Page22
Hypertensive disorders are an important cause of stillbirth, and in the SCRN study were associated with 9.2% of all stillbirths. Chronic hypertension is associated with a two- to four-fold higher risk of stillbirth compared to the general population.Reference Metz, Berry, Fretts, Reddy and Turrentine23 Adopting the American College of Cardiology and American Heart Association’s recently modified criteria for diagnosing hypertension in nonpregnant adults to be a blood pressure of >130/80 increases the number of patients entering pregnancy with a diagnosis of chronic hypertension. According to the Chronic Hypertension and Pregnancy (CHAP) trial, a US-based randomized trial of over 2,400 pregnant individuals with mild chronic hypertension, antihypertensive treatment with tight blood pressure control (< 140/90) compared with less tight control was associated with a decrease in a primary composite outcome of preeclampsia with severe features, medically indicated preterm birth at < 35 weeks’ gestation, placental abruption, or fetal or neonatal death, with no increased risk of being small for gestational age.Reference Tita, Szychowski, Boggess, Dugoff, Sibai and Lawrence24
Progression to severe maternal hypertension with concern for maternal end-organ involvement is also associated with increased risk of stillbirth. In a prospective study of 1,948 individuals with hypertension during pregnancy, those who developed preeclampsia with or without underlying chronic hypertension were at increased risk of perinatal mortality compared with women who had gestational hypertension.Reference Ray, Burrows, Burrows and Vermeulen25 Considering the impact of pregnancy on normal blood pressure, obstetricians have historically underestimated the frequency of chronic hypertension during pregnancy and have the opportunity to improve pregnancy outcomes by initiating antihypertensive therapy at ≥ 130/80.
Pregestational diabetes is associated with about 4% of stillbirths.26 Achieving a prepregnancy HgbA1c of < 7% and euglycemia during pregnancy are recommended to reduce the risk of stillbirth.Reference Starikov, Dudley and Reddy27
Other maternal medical conditions that have been associated with increased stillbirth risk include poorly controlled thyroid disease, chronic kidney disease, systemic lupus erythematosus, antiphospholipid antibody syndrome, sickle cell disease, and intrahepatic cholestasis of pregnancy.
Fetal and placental conditions encompass the remainder of suspected causes for stillbirth. Fetal etiologies include red cell and platelet alloimmunization, chromosomal abnormalities, structural anomalies, and fetal-maternal hemorrhage.Reference Korteweg, Erwich, Timmer, van der Meer, Ravisé and Veeger28,Reference Korteweg, Bouman, Erwich, Timmer, Veeger and Ravisé29 Placental and umbilical cord causes include placental abruption, placenta previa, vasa previa, cord prolapse, cord occlusion, and placental/cord abnormalities, especially among twin gestations (twin-to-twin transfusion syndrome, unequal placental sharing, velamentous insertion, cord entanglement).6,Reference Ananth, Berkowitz, Savitz and Lapinski30
It is estimated that almost 25% of stillbirths in the United States are potentially preventable with appropriate care during the pregnancy (e.g. achieving euglycemia with diabetes and/or normotension with hypertension).Reference Page, Thorsten, Reddy, Dudley, Hogue and Saade31 Stillbirth risk from placental dysfunction as demonstrated by fetal growth restriction may be mitigated with increased prenatal surveillance and earlier delivery. Of note, approximately half of stillbirths occur in appropriately-grown-for-gestational-age (AGA) fetuses.Reference Gardosi, Madurasinghe, Williams, Malik and Francis13 Many of these pregnancies display poor interval growth likely from abnormal placentation (either function or size) but may not fall below an estimated fetal weight or abdominal circumference tenth percentile threshold to meet the diagnosis of fetal growth restriction,Reference Martins, Biggio and Abuhamad32 and thus are not closely monitored prenatally. One study by MacDonaldReference MacDonald, Hui, Tong, Robinson, Dane and Middleton33 demonstrated that reduced growth velocity between 28- and 36-weeks’ gestation among AGA fetuses was associated with increased odds of cerebral redistribution, neonatal acidosis, and low neonatal body fat percentage, which are all markers of placental dysfunction.Reference MacDonald, Hui, Tong, Robinson, Dane and Middleton33 Additional prospective research is needed to quantify the risk of poor interval fetal growth in AGA pregnancies to determine whether prenatal testing has the potential to mitigate this risk.
Finally, optimization of maternal medical conditions such as hypertension and diabetes prior to pregnancy also decreases stillbirth risk.
6 Management Options
6.1 Index Pregnancy
6.1.1 Diagnosis and Clinical Evaluation
The diagnosis of stillbirth is often made when there is cardiac asystole on ultrasound at or after 20 weeks’ gestation. A thorough evaluation at that scan to identify a potential cause can help inform future pregnancy care and recurrence risk as well as provide closure and bereavement for grieving families. It can also facilitate research on etiology and management strategies.
A complete and detailed medical and obstetric history should be taken once the diagnosis of stillbirth is established. A review of any pertinent circumstances, family history, and risk factors may help identify possible causes and guide further testing. Relevant information to review is detailed in Table 3 and includes looking for a history of diabetes, hypertension, autoimmune disease, venous thromboembolism, fetal growth restriction, oligohydramnios, genetic screening/testing, maternal infections, and trauma.
Past medical history
Diabetes
Hypertension
Venous thromboembolism/thrombophilia
Autoimmune disorders (lupus, antiphospholipid syndrome)
Substance use disorder
Intrahepatic cholestasis of pregnancy
Epilepsy
Obstetric history
Recurrent pregnancy loss
Previous pregnancy with adverse outcome (small for gestational age, stillborn, abruption)
Confirm pregnancy dating with menses and earliest ultrasound
Assess estimated fetal weight based on confirmed due date
Genetic screening and prenatal anatomy ultrasounds
Screen for infectious signs or symptoms in current pregnancy
Assess for maternal trauma
Family history
Congenital anomalies or genetic conditions
History of stillbirth or sudden infant death
Developmental delay
Consanguinity
Venous thromboembolism
6.1.2 Other Evaluation
Placental Examination
Gross and microscopic examination of the placenta, umbilical cord, and fetal membranes by a trained pathologist is considered to have the highest diagnostic utility in stillbirth evaluation.Reference Metz, Berry, Fretts, Reddy and Turrentine23,Reference Korteweg, Erwich, Timmer, van der Meer, Ravisé and Veeger28,Reference Page, Christiansen-Lindquist, Thorsten, Parker, Reddy and Dudley34 Gross evaluation includes placental weight compared to gestational age norms and assessment for signs of abruption, umbilical cord thrombosis, chorioangioma, velamentous cord insertion, and vasa previa. In multifetal gestations, chronicity should be confirmed and vascular anastomoses across shared placental circulation documented.
Microscopic examination of the placenta may reveal information regarding circulation abnormalities and infection. Infection can cause stillbirth via three pathways: (1) direct infection; (2) placental damage; and (3) severe maternal illness. While direct infections via TORCH pathogens are more common in low-resource countries, ascending bacterial infections are the most common infectious cause of stillbirth in high-resource settings.Reference McClure, Dudley, Reddy and Goldenberg35 Interpretation of placental pathologic findings may be challenging as such features do not always indicate causation. For example, pathology findings of isolated incidental histologic chorioamnionitis may be extensive polymorphonuclear cell invasion of the placental membranes and would be considered a present condition, especially without clinical diagnosis of chorioamnionitis. Whereas histologic funisitis, in which there is extensive polymorphonuclear cell invasion of the umbilical cord indicating a fetal inflammatory response to an infectious process is considered causal for stillbirth.Reference Dudley, Goldenberg, Conway, Silver, Saade and Varner21
When placental pathologic findings occur in association with a maternal or fetal condition (for instance, placental infarcts in the setting of antiphospholipid syndrome [APS]), the clinical condition itself is considered the possible or probable cause of stillbirth rather than the placental pathology.Reference Dudley, Goldenberg, Conway, Silver, Saade and Varner21
Of note, the presence of umbilical cord knots or tangling should be interpreted with caution, as these findings commonly occur in uncomplicated healthy live births. Before concluding that an umbilical cord accident is the likely cause of stillbirth, findings of hypoxia on perinatal postmortem examination or on placental/cord histology should be assessed and documented. Since nuchal cords, cord entrapment, and true knots are common incidental findings in even healthy live births, in the absence of such histopathologic confirmation, the presence of these umbilical cord abnormalities cannot imply a cause of stillbirth.Reference Hammad, Blue, Allshouse, Silver, Gibbins and Page22
Fetal Autopsy
Fetal autopsy is the second most useful diagnostic test in stillbirth evaluation, after placental examination, especially when there are dysmorphic features, inconsistent growth measurements, anomalies, or hydrops present.Reference Korteweg, Erwich, Timmer, van der Meer, Ravisé and Veeger28,Reference Page, Christiansen-Lindquist, Thorsten, Parker, Reddy and Dudley34 The height, weight, foot length, and head circumference of the fetus are measured and compared to gestational age norms. Frontal and profile photographs of the whole body, face, extremities, palms, and any abnormalities or dysmorphic features can be obtained to supplement documentation. The autopsy is valuable at detecting subtle findings that can inform possible causes of stillbirth such as infection, anemia, hypoxia, and metabolic abnormalities.Reference Faye-Petersen, Guinn and Wenstrom36 Direct fetal infection as a cause of stillbirth requires histologic evidence of fetal organ damage plus positive culture, histologic, or polymerase chain reaction (PCR) evidence of a presence of a specific organism, especially in an internal fetal organ.Reference McClure, Dudley, Reddy and Goldenberg35
A review of US fetal death certificate data revealed only 20% of stillbirth cases had a fetal autopsy.Reference Oliver, Finneran, Rood, Ma’ayeh, Berghella and Silver37 Underutilization of fetal autopsy for stillbirth evaluation is likely due to a variety of challenges including lack of trained perinatal pathologists, financial costs, difficulty counselling grieving parents, and cultural beliefs regarding the invasive nature of autopsy. Due to limited availability of trained perinatal pathologists at local or regional hospitals, where many patients with stillbirth commonly present, transfer of the fetus and placenta to a higher center that has the necessary expertise is strongly encouraged given the high diagnostic potential of this examination.Reference Gibbins, Vora, Subramaniam, Page, Riches and Rothwell38 If parents are hesitant with complete autopsy, partial autopsy, gross examination by a trained pathologist, and further imaging (ultrasonography, magnetic resonance imaging [MRI], and endoscopic) may be offered. Allow parents to spend bonding time with the baby and perform cultural or religious activities before the autopsy.
Genetic Testing
Genetic testing is the next most useful diagnostic test in stillbirth evaluation and should be offered in all cases. A thorough family history with a three-generation pedigree including a record of stillborn infants should be reviewed and consanguinity sought to increase the diagnostic yield of genetic testing.Reference Metz, Berry, Fretts, Reddy and Turrentine23 Historically, karyotype was the initial test and, at times, the only genetic test option offered for stillbirth evaluation. The rate of karyotype abnormalities detected range from 6 to 13% among all cases, and greater than 20% of cases with anatomic abnormalities or growth restriction will have an abnormal karyotype.6,Reference Korteweg, Bouman, Erwich, Timmer, Veeger and Ravisé29,Reference Pauli, Reiser, Lebovitz and Kirkpatrick39
Since karyotype requires cell culture and 50% of cultures fail after delivery, an amniocentesis is recommended for better diagnostic yield. If amniocytes cannot be obtained, the next preferred options include an unfixed placental sample (1 × 1 cm) from below the cord insertion including the chorionic plate, an umbilical cord segment (1.5 cm), or internal fetal tissue specimen (costochondral junction or patella; skin is not recommended). These specimens should be placed in sterile tissue culture medium of lactated Ringer’s solution and stored at room temperature. The sample should not be placed in formalin.Reference Metz, Berry, Fretts, Reddy and Turrentine23
Due to the limitations of karyotype testing, microarray is presently the first-line test for genetic evaluation of stillbirth as live cells are not required.40 Microarray analysis is also more robust, detecting deletions or duplications as small as 50 kilobases. In the SCRN study of 532 stillbirths, microarray increased the diagnostic yield more than karyotype (87.4% vs. 70.5%; p < 0.001) and provided a higher detection of genetic abnormalities (e.g. aneuploidy or pathogenic copy-number variants) (8.3 vs. 5.8%; p = 0.007).Reference Reddy, Page, Saade, Silver, Thorsten and Parker41 Microarray analysis also identified more genetic abnormalities among 443 antepartum stillbirths (8.8 vs. 6.5%; p = 0.02) and 67 stillbirths with congenital anomalies (29.9 vs. 19.4%; p = 0.008).Reference Reddy, Page, Saade, Silver, Thorsten and Parker41 Limitations of microarray testing include inability to detect balanced translocations or low-level mosaicism, higher costs, copy number variants of uncertain clinical significance, and the uncertainty regarding these findings.
Whole exome and genome sequencing may increase the diagnostic yield in stillbirth evaluation as they detect single nucleotide changes and duplications or deletions. Live culture cells are not required. In the SCRN study cohort, whole exome sequencing was performed on 246 stillbirths without a clearly defined cause of death and with a normal microarray. It demonstrated a cumulative diagnostic yield of 6.1% with 15 of the 246 stillborn cases receiving a molecular diagnosis in a known disease gene.Reference Stanley, Giordano, Thorsten, Buchovecky, Thomas and Ganapathi42 An additional 6 cases (2.4%) had a “suggestive” genotype for either a known stillbirth gene or a gene candidate for phenotype expansion, thus yielding a probable molecular diagnosis rate of 8.5% in total cases.Reference Stanley, Giordano, Thorsten, Buchovecky, Thomas and Ganapathi42 Whole genome and exome sequencing will likely become the preferred genetic tests for stillbirth evaluation as costs decline and they become more widely available.
Laboratory Studies: Routine and Selective
Routine laboratory studies for stillbirth evaluation include testing for APS and fetal-maternal hemorrhage (FMH) testing. An acquired autoimmune disorder, APS is defined by the presence of persistent circulating antiphospholipid antibodies with associated clinical features. Only one clinical criteria is required and can include vascular thrombosis or pregnancy morbidity defined as: premature delivery before 34 weeks’ gestation from preeclampsia or placental dysfunction, one or more unexplained fetal deaths of a morphologically normal fetus at ≥ 10 weeks’ gestation, three or more consecutive spontaneous abortions at < 10 weeks’ gestation.43 In addition to one clinical criteria, one laboratory criteria is required for an APS diagnosis and includes the presence of lupus anticoagulant, anti-β2-glycoprotein IgM/IgG or anticardiolipin IgM/IgG with elevated values > 99th percentile on two or more occasions, at least 12 weeks apart.43 Testing for other inheritable thrombophilias is not routinely recommended.Reference Metz, Berry, Fretts, Reddy and Turrentine23
Testing for APS has a higher yield in stillbirth evaluation if associated with fetal growth restriction, severe preeclampsia, or other signs of placental dysfunction. In the SCRN study, over 500 stillbirth cases and over 1,500 live born cases underwent cardiolipin IgG testing. The risk of stillbirth in those testing positive was an OR of 3.43 (95% CI 1.79–6.60) compared to those that tested negative.Reference Silver, Parker, Reddy, Goldenberg, Coustan and Dudley44 After further analysis excluding cases with fetal anomalies, genetic disorders, or obstetric complications, the OR for stillbirth increased to 5.30 (95% CI 2.39–11.76) in those with cardiolipin antibodies.Reference Silver, Parker, Reddy, Goldenberg, Coustan and Dudley44
A total of 4% of stillbirths in the SCRN study was due to FMH.6 This may be considered a cause when a large volume hemorrhage, defined as 20 ml/kg or > 25% of fetal blood volume, is documented.Reference Laube and Schauberger45,Reference Rubod, Deruelle, Le Goueff, Tunez, Fournier and Subtil46 However, the results of FMH testing must be interpreted with caution, as a small number of fetal cells may be detected in uncomplicated pregnancies resulting in a live birth. Testing for FMH should be performed before the induction of labor or dilation and evacuation because delivery itself can confound results. If predelivery testing is not possible, FMH testing postpartum may still be considered as most deliveries do not result in a significant FMH. Either Kleihauer-Betke or flow cytometry may be used for FMH testing as a large volume hemorrhage is needed to be considered clinically significant to cause stillbirth.
The remainder of the laboratory studies should be tailored to the history and autopsy and placental pathology results obtained at the initial evaluation for stillbirth.Reference Page, Bardsley, Thorsten, Allshouse, Varner and Debbink47 For instance, routine serology screening of infectious etiologies (cytomegalovirus, parvovirus, syphilis, toxoplasmosis, rubella, or herpes simplex virus) in the absence of clinical or histopathologic evidence is likely of low utility and not cost-effective.Reference Metz, Berry, Fretts, Reddy and Turrentine23 Furthermore, a positive infectious screen in the absence of clinical or pathology findings may not necessarily correlate to a potential cause of stillbirth. If autopsy, placental pathology, or history is suggestive of an infectious cause, then further evaluation should be performed. This could include maternal or neonatal serology, special tissue stains, and PCR testing for bacterial or viral nucleic acids. Infection accounted for 12.9% of stillbirth causes in the SCRN study.6 Infection may result in stillbirth by direct fetal infection, placental dysfunction, severe maternal illness such as sepsis, or by triggering spontaneous preterm birth. The most common causal pathogens included Escherichia coli, group B streptococcus, enterococcus, and cytomegalovirus. Infectious testing was performed in the setting of positive clinical history or pathology findings.6
Additional laboratory testing should be guided by history, physical examination, and clinical findings. For example, testing for diabetes is warranted in the setting of a large-for-gestational-age fetus, testing for parvovirus is reasonable in the setting of fetal hydrops, and testing for intrahepatic cholestasis of pregnancy is recommended in the setting of maternal pruritis or elevated liver enzymes.Reference Page, Christiansen-Lindquist, Thorsten, Parker, Reddy and Dudley34,Reference Silver, Parker, Goldenberg, Reddy, Dudley and Saade48 In summary, standard stillbirth evaluation should include offering placental pathology, fetal autopsy, genetic testing, APS testing, and FMH testing. The remainder of the investigations should be guided by clinical findings.
6.1.3 Delivery
The timing and mode of delivery after stillbirth depend on gestational age at which the death occurred, maternal obstetric history, clinical circumstances, institutional expertise, and patient preference. Although most patients desire prompt delivery, urgency is not medically required as clinical coagulopathy and intrauterine infections are uncommon with expectant management.
Delivery of a stillbirth during the second trimester is via dilation and evacuation or labor induction. Limitations of a dilation and evacuation procedure include lack of access to an experienced provider, limited ability to grossly examine for structural anomalies, and inability to hold or see the fetus after removal.Reference Metz, Berry, Fretts, Reddy and Turrentine23 The risks of induction of labor should also be reviewed, which include possibly needing a dilation and curettage for removal of the placenta after delivery of the fetus and increased risk of infection requiring antibiotics.
Several studies have compared the efficacy and risks of the two delivery modes. A retrospective cohort study of 297 women who underwent either dilation and evacuation or medical abortion between 14 and 24 weeks demonstrated that the overall complication rate was significantly lower in patients who underwent dilation and evacuation than patients who underwent medical abortion (4 vs. 29%; p < 0.001).Reference Autry, Hayes, Jacobson and Kirby49 Another retrospective cohort study of almost 400 second-trimester abortions via labor induction or dilation and evacuation between 13 and 24 weeks’ gestation also demonstrated that labor induction has a higher complication rate with an adjusted risk ratio of 8.5 (95% CI 3.7–19.8).Reference Bryant, Grimes, Garrett and Stuart50 Retained tissue requiring an additional procedure or manual removal of the placenta was the most frequent complication in the labor induction group.Reference Bryant, Grimes, Garrett and Stuart50 Providers should review the risks and benefits of each approach with patients, as well as consider institutional expertise (availability of experienced dilation and evacuation providers), and together arrive at a decision via shared decision-making.
For labor induction at less than 28 weeks’ gestation, misoprostol is the most effective method at achieving uterine evacuation within 48 hours, regardless of cervical Bishop score.Reference Ponce, de León and Wing51 The route of administration, dose, and dosing interval of misoprostol varies across institutional protocols. Suggested misoprostol dosing for less than 28 weeks’ gestation is 400–600 micrograms vaginally every 3–6 hours.Reference Metz, Berry, Fretts, Reddy and Turrentine23 This dosing may need to be adjusted based on the presence of uterine scar and individualized risk of uterine rupture. Administration of mifepristone 200 mg 24–48 hours before starting misoprostol decreases the time from start to delivery.Reference Metz, Berry, Fretts, Reddy and Turrentine23 After 28 weeks’ gestation, labor induction should be managed according to standard obstetric protocols.
6.1.4 Bereavement Care
Bereavement care starts as the diagnosis of a stillbirth is made and should be provided by all health professionals involved in the care of the family. As with delivery planning, bereavement care should be provided in an individualized fashion, considering the parents’ personal, cultural, and religious beliefs. Families should be offered keepsake items such as handprints or footprints, special blankets, or clothing. Other principles of bereavement care include good communication with avoidance of terms such as fetus/embryo, shared decision-making, recognition of parenthood, and acknowledgment of the partner’s and family’s grief. It is important to recognize that the grief journey is different for each person, providing options for burials, cremation, or funeral; providing information on professional and peer-to-peer support services, and that health professionals having access to self-care, as this journey can take a toll on health providers as well.Reference Metz, Berry, Fretts, Reddy and Turrentine23 Timely delivery of test results from the stillbirth evaluation is important for closure even when no specific etiology is identified.Reference Laing52
6.2 Future Pregnancies
6.2.1 Pregnancy and Prenatal Management
Overall Care
Limited data exist regarding recommendations for the management of subsequent pregnancy after stillbirth. Parents often experience more anxiety and distress in pregnancies after a stillbirth, and providers should be sensitive to emotional difficulties. Rainbow Clinics are examples of measures that have been established to provide sensitive personalized prenatal care for expecting parents who have endured a pregnancy loss.Reference Le Vance, Plant, Saba, Heazell, Morris and Morton53 They are equipped with additional resources including increased mental health support, nutritional guidance, access to advocacy groups, and more frequent fetal testing and ultrasound evaluations.Reference Heazell, Barron and Fockler54 Consultation with maternal fetal medicine specialists or genetic counselors may be offered especially to discuss parental genetic testing.
Risk recurrence depends on the etiology of the stillbirth. Parents should be encouraged to focus on reducing modifiable risk factors (optimizing glycemic control in the setting of diabetes, gaining appropriate pregnancy weight, optimizing the control of blood pressure before and during pregnancy, and discontinuing smoking and substance use). Compared to women who had a live-born first infant, the risk of subsequent stillbirth is 2.5-times higher in those with a previous stillborn pregnancy.Reference Surkan, Stephansson, Dickman and Cnattingius55 The recurrence risk after an unexplained stillbirth varies across studies, with reported adjusted risk of 3.11 (95% CI 0.72–13.50) and 4.18 (95% CI 1.36–12.89).Reference Gordon, Raynes-Greenow, McGeechan, Morris and Jeffery56,Reference Measey, Espaignet, Charles and Douglass57
Individualized care plans should be established for each pregnant individual that address the presumed etiology of the prior stillbirth. Diabetes, hypertension, substance use, and obesity are some common modifiable risk factors. Stillbirth associated with either early onset preeclampsia or placental abnormalities leading to early onset growth restriction may benefit from low-dose aspirin begun by 14 weeks’ gestation. Success requires patient education and planning before conceiving. We recommend caregivers refer to the relevant Element for details.
Fetal Surveillance
Data on antepartum surveillance in subsequent pregnancies after stillbirth is very limited and the optimal frequency for testing remains unknown. Recommendations are often guided more by emotion than fact. For example, for patients with a prior stillbirth at or after 32 weeks’ gestation, once or twice a week prenatal surveillance is recommended starting at 32 weeks’ or 1–2 weeks before the gestational age of the prior stillbirth.Reference Metz, Berry, Fretts, Reddy and Turrentine23 However, it could be argued that the circumstances of the current pregnancy are relevant. If the prior loss was associated with a prior major malformation or early onset growth restriction but the current pregnancy has normal fetal structure and growth, does the same recommendation hold? There are no studies that support twice-weekly surveillance for what appears a to be a structurally normal fetus with normal blood flow studies. For a prior stillbirth that occurred before to 32 weeks’ gestation, timing of prenatal surveillance may be individualized taking into consideration the potential for morbidity (e.g. iatrogenic prematurity for a false-positive test), cost, and parental anxiety.Reference Metz, Berry, Fretts, Reddy and Turrentine23 Parents are encouraged to be vigilant for fetal movements and report if these are reduced.
6.2.2 Delivery Timing
Delivery timing for subsequent pregnancy after stillbirth should be based in great part on the circumstances of the prior loss and the current pregnancy. Increased parental anxiety is the norm. Delivery before 39 weeks’ gestation is associated with an increased risk of admission to neonatal intensive care units and other morbidities.Reference Metz, Berry, Fretts, Reddy and Turrentine23 Preterm delivery of a healthy fetus is not a treatment for anxiety and increases risk for other problems. Communication and education is key. In cases of severe patient anxiety, when there is a patient preference to proceed with early-term delivery (38 0/7 weeks to 38 6/7 weeks) constitutes a relatively safe compromise. Support and reassurance should be provided every step of the way from antepartum to intrapartum and finally to postpartum.
7 Summary of Management Options
7.1 Definition and Epidemiology
Definitions of stillbirth vary around the world. The US NCHS defines stillbirth as intrauterine fetal death at or after 20 weeks’ gestational age.
The highest stillbirth rates are found in sub-Saharan Africa (21.0 per 1,000 total births) and Southern Asia. The lowest regional rates are in Europe, Northern America, Australia, and New Zealand, with rates about 3 per 1,000 total births.
7.2 Risk Factors (see Tables 1 and 2)
Social/demographic
Maternal history
7.3 Index Pregnancy
Diagnosis
– Documentation of cardiac asystole on real-time ultrasound after 20 weeks’ gestation
Clinical evaluation (see Table 3)
Other evaluation (see Table 4)
– Placental examination
– Fetal autopsy (or alternative that is acceptable to parents such as ultrasound and/or MRI)
– Genetic testing
– Laboratory studies both routine and selective based on other findings
Delivery
– Options should be discussed with the woman:
1. Expectant
2. Dilatation and evacuation at < 24 weeks
3. Under 28 weeks’ gestation, mifepristone followed by misoprostol
4. Beyond 28 weeks’ gestation, standard induction protocols (cervical ripening followed by oxytocin administration)
Bereavement care
– This starts as soon as the diagnosis is made; it should be individualized based on personal, cultural, and religious beliefs
– Offer parents the opportunity to see, hold, and create keepsakes of their infant such as hand/footprints and photos
– Offer a detailed discussion of possible causes and implications for future pregnancies
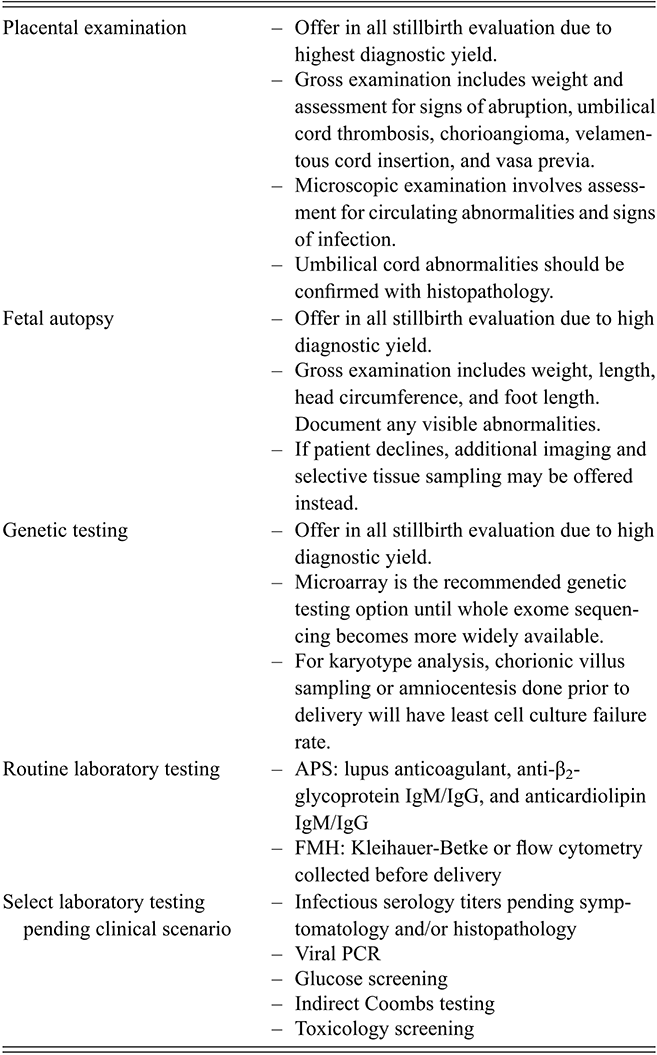
Table 4 Long description
The table consists of two columns. It reads as follows. Row 1. Placental examination: Offer in all stillbirth evaluation due to highest diagnostic yield. Gross examination includes weight and assessment for signs of abruption, umbilical cord thrombosis, chorioangioma, velamentous cord insertion and vasa previa. Microscopic examination involves assessment for circulating abnormalities and signs of infection. Umbilical cord abnormalities should be confirmed with histopathology. Row 2. Fetal autopsy: Offer in all stillbirth evaluation due to high diagnostic yield. Gross examination includes weight, length, head circumference, and foot length. Document any visible abnormalities. If patient declines, additional imaging and selective tissue sampling may be offered instead. Row 3. Genetic testing: Offer in all stillbirth evaluation due to high diagnostic yield. Microarray is the recommended genetic testing option until whole exome sequencing becomes more widely available. For karyotype analysis, chorionic villus sampling or amniocentesis done prior to delivery will have least cell culture failure rate. Row 4. Routine laboratory testing: A P S: lupus anticoagulant, anti-β 2-glycoprotein I g M/I g G, and anticardiolipin I g M/I g G. F M H: Kleihauer-Betke or flow cytometry collected before delivery. Row 5. Select laboratory testing pending clinical scenario: Infectious serology titers pending symptomatology and/or histopathology. Viral P C R. Glucose screening. Indirect Coombs testing. Toxicology screening.
7.4 Future Pregnancy
Prepregnancy and prenatal
– Provide additional emotional and psychological support throughout.
– Rediscuss the index birth, the possible etiologies, and create an individualized plan to optimize the management of any maternal medical conditions and change potentially modifiable risk factors.
– Management during pregnancy should be in or assisted by a specialized fetal medicine center.
– Prediction of recurrence is poor.
– Fetal surveillance is commonly implemented. However, this should be tailored to the cause and timing of the previous stillbirth. With a normally formed fetus that is growing normally, there is no evidence that such fetal surveillance is of benefit. In such cases, it can have opposite effects, providing reassurance to some parents but anxiety in others.
– Women should be vigilant for fetal movements and report a reduction in these urgently.
Delivery
– Timing and mode of delivery should be a joint decision with the parents and based on the evidence of risk in the current pregnancy.
– Delivery before 39 weeks’ gestation is associated with an increased maternal and fetal morbidity. Thus, it could be argued that it should only occur when there is a valid clinical indication.
– The route of delivery should reflect the findings in the current pregnancy.
Professor David James
Emeritus Professor, University of Nottingham, UK
David James was Professor of Fetomaternal Medicine at the University of Nottingham from 1992–2009. The post involved clinical service, especially the management of high-risk pregnancies, guideline development, research and teaching and NHS management. From 2009–14 he was Clinical Director of Women’s Health at the National Centre for Clinical Excellence for Women’s and Children’s Health. He was also Clinical Lead for the RCOG/RCM/ eLfH eFM E-Learning Project. He is a recognised authority on the management of problem/ complicated pregnancies with over 200 peer-reviewed publications. He has published 16 books, the best-known being High-Risk Pregnancy: Management Options.
Professor Philip Steer
Emeritus Professor, Imperial College, London, UK
Philip Steer is Emeritus Professor of Obstetrics at Imperial College London, having been appointed Professor in 1989. He was a consultant obstetrician for 35 years. He was Editor-in-Chief of BJOG – An International Journal of Obstetrics and Gynaecology – from 2005–2012, and is now Editor Emeritus. He has published more than 150 peer-reviewed research papers, 109 reviews and editorials and 66 book chapters/books, the best known and most successful being High-Risk Pregnancy: Management Options. The fifth edition was published in 2018. He has been President of the British Association of Perinatal Medicine and President of the Section of Obstetrics and Gynaecology of the Royal Society of Medicine. He is an honorary fellow of the College of Obstetricians and Gynaecologists of South Africa, and of the American Gynecological & Obstetrical Society.
Professor Carl Weiner
Creighton University School of Medicine, Phoenix, AZ, USA
Carl Weiner is presently Head of Maternal Fetal Medicine for the CommonSpirit Health System, Arizona, Director of Maternal Fetal Medicine, Dignity St Joseph’s Hospital, Professor, Obstetrics and Gynecology, Creighton School of Medicine, Phoenix, and Professor, College of Health Solutions, Arizona State University. He is the former Krantz Professor and Chair of Obstetrics and Gynecology, Division Head Maternal Fetal Medicine and Professor Molecular and Integrative Physiology at the University of Kansas School of Medicine, Kansas City, KS and the Crenshaw Professor and Chair of Obstetrics, Gynecology and Reproductive Biology, Division Head Maternal Fetal Medicine, and Professor of Physiology at the University of Maryland School of Medicine, Baltimore. Dr Weiner has published more than 265 peer-reviewed research articles and authored/edited 18 textbooks including High-Risk Pregnancy: Management Options. His research was extramurally funded for more than 30 years without interruption.
Professor Stephen C. Robson
Newcastle University, UK
Stephen C. Robson is Emeritus Professor of Fetal Medicine for the Population and Health Sciences Institute at The Medical School, Newcastle University. He is also a Consultant in Fetal Medicine for Newcastle upon Tyne Hospitals NHS Foundation Trust. He has published over 400 peer-reviewed articles and edited several; books, the highly successful being High-Risk Pregnancy: Management Options. The fifth edition was published in 2018. He has been President of the British Maternal and Fetal Medicine.
About the Series
Most pregnancies are uncomplicated. However, for some (‘high-risk’ pregnancies) an adverse outcome for the mother and/or the baby is more likely. Each Element in the series covers a specific high-risk problem/condition in pregnancy. The risks of the condition will be listed followed by an evidence-based review of the management options. Once the series is complete, the Elements will be collated and printed in a sixth edition of High-Risk Pregnancy: Management Options.