

Preparation for a natural disaster, terrorist attack, or pandemic influenza finds many municipalities seeking innovative methods for improving the efficiency and effectiveness of emergency planning and response activities, including new approaches for operating mass vaccination clinics. A primary goal of these clinics is to ensure that a high percentage of the candidate population is vaccinated quickly and with the least amount of burden to the community and local public health responders. Site selection and logistical considerations in planning for a mass vaccination clinic include accessibility for the public, ability to accommodate and process large numbers of people, availability on a limited notice, site security, and public safety. An increasingly popular method to address these needs is to use a drive-through clinic.Reference Zerwekh, McKnight and Hupert1, Reference Hansen and Dunn2
Drive-through clinics allow people to stay in their vehicles while being processed and vaccinated. This is extremely beneficial to older adults, people with physical disabilities, and families with children. It eliminates the burden of finding a parking spot, walking into the clinic, and standing in line to be processed. Drive-through clinics also alleviate the need to find a building that can accommodate a large number of vaccinees or to require vaccinees to stand outside during adverse weather conditions.Reference Zerwekh, McKnight and Hupert1
By having people remain in their vehicles, properly managed drive-through clinics can be advantageous to maintain orderly queues, minimize interactions and disturbances between people, and allow vaccinees to wait in a familiar and comfortable environment. Misinformation, rumors, and other disturbances are also known to emerge when people stand and wait in line during a stressful situation. To help ensure a consistent flow of information during a drive-through clinic, vehicle occupants can be provided with standardized messages and updates through their car radio using inexpensive and readily available short-range broadcast equipment (similar to the “talking house” devices used in home sales).
Potential disadvantages of drive-through clinics include the need to own or have access to a vehicle, limited access to restroom facilities for the waiting public, local traffic congestion, and worker safety issues, such as the potential for being struck/injured by a vehicle.Reference Zerwekh, McKnight and Hupert1 An additional concern is the exposure of clinicians, volunteers, public health responders, and the public to vehicle exhaust emissions including carbon monoxide (CO) when clinics are held within parking garages, bus garages, tents, or other enclosed structures.Reference Hansen and Dunn2
CO is a colorless and odorless gas produced by the incomplete combustion of carbon-based materials such as gasoline and diesel fuel and is readily absorbed into the body through inhalation. CO is an insidious poison that reduces the body's ability to transport oxygen due to its higher affinity to bind with hemoglobin in the blood (forming carboxyhemoglobin). Once carried into the bloodstream, CO binds with tissues and cells in the body and interferes with their normal function. 3–5
The risk of CO poisoning is influenced by the concentration of CO, the duration of exposure, level of activity, and individual susceptibility. Early onset of CO poisoning is characterized by nonspecific symptoms, such as headache, nausea, dizziness, and vomiting that may be mistaken as symptoms of a cold, the flu, or food poisoning. Thus, the presence of elevated levels of CO may go unrecognized, allowing exposure to continue. More severe poisoning may result in confusion, weakness, seizure, coma, and death. Fetuses of pregnant women and people with preexisting heart disease are particularly susceptible to the effects of CO poisoning. 3–5
The federal Occupational Safety and Health Administration (OSHA) has established a permissible exposure limit for CO of 50 parts per million (ppm) in air as an 8-hour time-weighted average (TWA).6 The American Conference of Governmental Industrial Hygienists (ACGIH), a nongovernmental scientific association, recommends that 8-hour TWA exposures be limited to 25 ppm.7
The OSHA and ACGIH levels are based on exposure of a healthy worker for a 40-hour work week and, therefore, are not necessarily applicable to the disparate groups present during a typical public mass vaccination program (eg, older adults, people with infirmities, children, and nonpaid community volunteers). The World Health Organization (WHO) recommends that indoor air levels for CO be kept below an average of 9 ppm for any 8-hour period and below 87 ppm for any 15-minute period.5
METHODS
We monitored CO levels during indoor drive-through clinics held on the same day at 2 separate locations in a rural upstate New York county. Both clinics were held in school bus garages located about 30 mi apart. Each clinic was operated for 2 hours (10 am to noon), during which seasonal flu vaccines were administered to county residents as they remained within their vehicles. At each location, vehicle engines remained operating within the garage for 4 stages of the vaccination process: initial completion of forms by the vaccinees, forms review, medical screening, and vaccination/final forms review.
Outdoor air temperatures at each location ranged from 35° to 37°F. Sustained outdoor wind speeds at a local weather monitoring station were approximately 10 to 12 mph with recorded gusts up to 31 mph.8 Although we did not measure wind speeds or dilution airflow rates within the garages, there was a strong and steady flow of outdoor air throughout the clinic period at each location. Paperweights were needed to keep forms from blowing off the tables and metal music stands that served as sign holders were knocked over by the wind gusts. Each garage was equipped with a ceiling-mounted ventilation system, but these were not used while the clinics were in session. Likewise, no heating was provided and the indoor temperatures after the garage bay doors had been opened were at or a few degrees above the outdoor air temperatures.
Description of Clinic A
The bus garage for clinic A measured approximately 75 × 120 × 20 ft. There were 8 bay doors on either side of the building and each door was about 10 × 12 ft. The clinic processed 6 lanes of traffic and the remaining 2 sets of bay doors remained closed, except for a brief period when 1 additional set of doors was opened to increase airflow dilution in response to a worker complaint (see Results). Because of the wind and cold, the 6 sets of bay doors through which cars traveled were only partially opened to a height of about 9 ft. Traffic volume was consistent during the 2-hour period resulting in a continuous density of 24 idling vehicles within the building (6 lanes of traffic each including 4 processing stations). Overall, 192 vehicles were processed with an average processing time of 3.75 minutes per vehicle.
Description of Clinic B
The bus garage for clinic B measured approximately 80 × 105 × 18 ft. There were 4 bay doors on either side of the building and each door was about 20 × 15 ft. The clinic processed 4 lanes of traffic. Because of the wind and cold, the bay doors were only partially opened to a height of about 10 ft. Traffic volume tapered during the last half-hour and 3 sets of bay doors were closed reducing throughput to 1 lane. Traffic had been consistent for the first 90 minutes of the clinic period, resulting in a density of 16 idling vehicles within the building (4 lanes of traffic each including 4 processing stations). Overall, 113 vehicles were processed with an average processing time of 4.25 minutes per vehicle.
Air Sampling Methods
CO levels were measured by 2 industrial hygiene/environmental health specialists at each facility using real-time, direct-reading instruments. One person operated an MP Surveyor II (Solomat, Norwalk, CT) and the other used a MultiRae Plus (Rae Systems, San Jose, CA) gas monitor. The Solomat and MultiRae instruments have CO detection limits of 0.1 and 1 ppm, respectively. The ambient level of CO varies, but it is generally <5 ppm. In addition to CO, the Solomat device measures carbon dioxide (CO2), temperature, and relative humidity, and the MultiRae measures nitrogen dioxide (NO2).
CO2 is a primary product of combustion and is also released from people in expired breath. Outdoor levels of CO2 are approximately 350 ppm. The CO2 detection range of the Solomat instrument is 100 to 5000 ppm. NO2 is a combustion byproduct of vehicle engines. National average ambient NO2 levels are <0.053 ppm9 and the detection limit of the Multi-Rae instrument is 0.1 ppm.
The instruments were handheld at breathing-zone height and carried around through the different stations for the entire clinic session. Readings for all measured parameters were recorded on a written log at approximately 5-minute intervals. When levels of CO above 2 ppm were detected, additional readings were taken near exhaust tailpipes to identify the source vehicle.
Control readings were taken outdoors and away from the building and vehicles before and after each clinic session. Instruments were pre- and postcalibrated using standardized calibration gases and in accordance with the manufacturers' specifications.
RESULTS
Clinic A
CO levels remained below 1 ppm for the majority of the clinic session. Two spikes in CO levels were detected at separate periods and each was associated with a single vehicle present within the garage at the time of the reading. The source vehicles were characterized as older model gasoline-powered pickup trucks that appeared and sounded to be in disrepair. The vehicles were present in the garage for less than 5 minutes each and the CO levels returned to background (<1 ppm) shortly after the vehicles exited. The highest breathing-zone levels measured during these 2 excursions were 8 and 10 ppm, respectively.
Approximately 45 minutes after the clinic began, 1 vaccinator reported having a headache and nausea. She left the garage to rest in a separate but adjoining area of the building and returned to her station after about 20 minutes. At the time of symptom onset, the odor of diesel emissions was noted, but the concentration of CO and other measured parameters were within normal ranges. To help dissipate the odor, 1 additional set of bay doors was opened for a short time. No other people at her station or elsewhere in the building reported feeling ill.
Outdoor CO levels before and after the clinic session were below detection. Indoor and outdoor NO2 levels were also below detection for all of the measurements. Indoor CO2 levels fluctuated throughout the session, but were within the range that is typical for office buildings (ie, <1000 ppm).
Clinic B
Data recorded at a single location near the center of the garage are presented in Figure 1. CO levels remained below 1 ppm for the majority of the clinic session. Two spikes in CO levels were detected at separate periods and each was associated with a single vehicle present within the garage at the time of the reading. One vehicle was a pickup truck and the other was a 4-door sedan. Both vehicles were older models and in obvious disrepair. The vehicles were present in the garage for <5 minutes each.
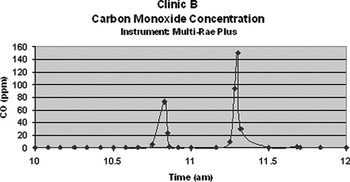
FIGURE 1 CO levels in clinic B
Measured breathing-zone CO concentrations reached 73 ppm for the first vehicle. This level dropped to 23 ppm within 1 minute after the vehicle left the garage and to 2 ppm after an additional minute.
The breathing-zone concentration associated with the second vehicle peaked at 150 ppm when it was idling at the final (vaccination) station. The operator shut the vehicle off at our request and within 1 minute the CO level dropped to 30 ppm. The CO level continued to decline after the vehicle left the building and reached 1 ppm in 12 minutes. The 15-minute time-weighted average exposure during this event was <40 ppm.
Outdoor CO levels before and after the clinic session were below detection. Indoor and outdoor NO2 levels were also below detection for all of the measurements. Indoor CO2 levels fluctuated throughout the session, but were within the range that is typical for office buildings (ie, <1000 ppm).
DISCUSSION
A primary goal in developing new and innovative public health planning and response measures is to reduce morbidity and mortality associated with an emergency. To this end, drive-through mass vaccination clinics offer the potential for increased timeliness, coverage, accessibility, efficiency, and convenience compared with traditional clinic arrangements, particularly in the rural setting.
The advantages of this new approach to mass vaccination, however, are accompanied by unique considerations for ensuring that the process is completed successfully and with minimum risk to all of the participants. Our findings from 2 indoor, drive-through mass vaccination clinics conducted in a rural New York county indicate the potential for short-term, high exposures to CO.
Despite the relative high density of idling vehicles within the garages, exposures were found to be associated with only a small number of individual vehicles that were in apparent disrepair. Measurable CO emissions were identified from <2% of all of the vehicles processed during the 2-hour long clinic sessions. Because of the efficient rate at which these vehicles were processed, exposure duration to any 1 vehicle within the garage was limited to less than 5 minutes. Relatively strong and consistent winds sweeping through the buildings helped to dilute and remove the CO produced by the vehicles. Outdoor air dilution rates may have been higher if the bay doors had been opened fully and all bay doors had been opened for the entire clinic session.
In our study, CO exposures remained below the TWA threshold limits established by OSHA, ACGIH, and WHO. However, for a brief period in clinic B, concentrations climbed rapidly and reached 150 ppm, upon which the identified source vehicle was turned off. Had we not been actively monitoring for CO, it is likely that the peak concentration and emission duration would have been greater resulting in a higher short-term TWA exposure.
This study was limited to 2 clinics operated in a single county on the same day, and the degree to which our findings are generalizable to other drive-through clinic settings is unknown. Although New York State law requires that all vehicles have annual emissions inspections, regulations may differ in other states and localities. Our findings indicate that the required annual emissions inspections are not a guarantee that all vehicles will have low CO emissions.
Variables that may affect CO exposures in these settings include the following:
• Total number of cars producing elevated CO levels during the clinic session
• Number of cars simultaneously producing elevated CO levels
• Building's natural ventilation characteristics (eg, size and shape of the building, number and size of open bay doors)
• Outdoor wind speeds and direction
• Availability and use of mechanical ventilation or supplemental air moving equipment (eg, fans)
• Vehicle processing times
Ideally, problematic vehicles should be identified before they enter the building and processed either outdoors or at an expedited rate indoors. Direct-reading CO monitors are often available through local fire departments, health departments, and power utilities. Given that these organizations are stakeholders in emergency preparedness activities, they may be solicited to provide active CO monitoring during a drive-through clinic. Individual CO monitors that can be worn by clinic workers are also commercially available. In the absence of a CO monitor, vehicles that are older or in obvious disrepair can be separated out for special processing.
The findings from this study were used to develop written guidelines for planning and operating an indoor drive-through clinic. These guidelines were provided to emergency response managers in all New York counties through the New York State Association of County Health Organizations and are reprinted in the Appendix.
CONCLUSIONS
CO exposures may be minimized by identifying and separately processing problematic vehicles before they enter the clinic. Direct reading CO monitors can help to identify these vehicles.
APPENDIX
Indoor Air Quality Concerns Associated With Drive-through Health Clinics: A Guide to Minimizing Exposure
The following are indoor air quality concerns to consider when planning for drive-through health clinics. The potential for carbon monoxide (CO) exposure from idling cars and heating sources, such as propane and gas-fired units, should always be considered when the clinic is inside a structure (eg, pole barns, garages). Questions on this fact sheet can be directed to the New York State Department of Health, Bureau of Occupational Health, at (518) 402-7900.
I. Selecting the Best Facility
A. Select facilities that have good airflow and ventilation.
B. Select sites with ventilation systems specifically designed for idling vehicles (eg, repair centers, parking garages).
II. Precautions for Reducing Indoor CO Levels
A. Weather conditions can significantly affect indoor CO levels. Consider how wind, humidity, temperature, and rain conditions could impact ventilation in the building on the day of the clinic, and to the extent possible, cars waiting to enter the facility should be downwind (ie, traffic flow should be directed into the wind).
B. During the clinic, keep the maximum number of overhead doors open for airflow.
C. Understand how the mechanical ventilation system in the structure works and have access to activate or adjust the system during the clinic.
D. Triage vehicles with more than 2 occupants and/or children to a high occupancy lane and assign more vaccinators to this lane as appropriate.
E. Limit the number of cars in the high-occupancy lane waiting for the vaccination station. Whenever possible, conduct form review and screening outside the structure.
F. Older vehicles and those in obvious disrepair should remain outside whenever possible.
G. Space vehicles to minimize the number idling inside the structure. Vehicles outside should be staged at a sufficient distance from the bay door(s) to keep exhaust from entering the structure.
H. Consider having a designated vaccination process outside for old or poorly maintained vehicles and possibly diesel-powered vehicles. Vehicles in poor repair often emit greater amounts of CO and other pollutants, and diesel odors are offensive to some individuals.
III. Air Monitoring During the Clinic
A. Trained personnel could periodically measure CO levels with continuous direct-read instruments. First responders, particularly fire professionals, typically have qualified, trained personnel and the appropriate equipment.
B. If monitoring occurs, then it should be performed in areas where staff are working and where air may be stagnant.
C. If CO monitors are not available, then the condition of the vehicle should be considered and any vehicle that is old or in obvious disrepair should remain outside whenever possible.
D. When direct-read instruments read 35 ppm of CO, measured at head height of any clinic worker, take action to reduce these levels. These actions can include the following:
1. Turn on any mechanical ventilation system in the structure.
2. Limit the number of idling vehicles in the structure.
3. Have vehicles emitting high levels turned off during the vaccination process to limit emissions.
4. Stop additional vehicles from entering the structure until the CO levels have dropped.
Use of a drive-through clinic is a valuable tool for the administration of vaccinations. Potential carbon monoxide exposure should not stop a clinic from occurring but should be considered during the planning process. Most if not all municipalities are preparing for the need for a mass vaccination clinic and knowledge of the experiences of others can help staff consider and plan for potential problems well in advance of an event.
Authors' Disclosures
The authors report no conflicts of interest.
Acknowledgments
The authors thank Ralph Van Houten and Judith Grillo for coordinating the field visits and assisting with the data collection.

