



Impact statement
Depression is the most frequent mental health problem. The international literature consistently reports a gender gap in depression. Also, an association between this gap and gender inequalities is supported by previous evidence. This study adds to the previous knowledge by examining if the advantage in life expectancy experienced by women compensates the higher prevalence of depressive symptoms across the life span through the assessment of gender differences in life expectancy free of depressive symptoms in 2003, 2010 and 2016 in Chile. Our findings showed a persistent gender gap, with women expecting to live 10 percent points or more of their remaining life with depressive symptoms, compared to men, at all ages and years considered. We analyzed the interaction of gender with other social dimensions that could exacerbate gender differences, and we observed that lower level of education and unemployment increased the probability of depressive symptoms among men and women, but the effect was larger and more persistent among women. The results of our research support the importance of including a gender approach in public policies aimed at reducing inequalities among the population in Chile, considering the intersection of gender and other social dimensions that amplify disadvantages among certain groups of the population. With respect to mental health care, efforts have been made in Chile to improve access, quality, opportunity and financial protection to health-care users via the Regime of Explicit Health Guarantees (GES program), which included depression in 2006. The guidelines of this program should be updated, considering gender perspective and tailored interventions, to improve not only the access of certain groups but also the relevance and effectiveness of treatments.
Introduction
Gender inequalities play an important role in shaping health and mental health gender gaps (King et al., Reference King, Kavanagh, Scovelle and Milner2018; Yu Reference Yu2018). Gender refers to the norms that a society prescribes according to at-birth sex (Colineaux et al., Reference Colineaux, Soulier, Lepage and Kelly-Irving2022). Gender is relational and intersects with multiple dimensions expressed in social norms, organization of relationships, role definition and power distribution, which differ across societies (Hammarström et al., Reference Hammarström, Johansson, Annandale, Ahlgren, Aléx, Christianson, Elwér, Eriksson, Fjellman-Wiklund, Gilenstam, Gustafsson, Harryson, Lehti, Stenberg and Verdonk2014). Hence, the magnitude of existing gender inequalities in health varies, but global tendencies can be identified. Men are more likely to experience violent mortality, suicide and diseases related to health risk behaviors, such as smoking or excess drinking (Weber et al., Reference Weber, Cislaghi, Meausoone, Abdalla, Mejía-Guevara, Loftus, Hallgren, Seff, Stark, Victora, Buffarini, Barros, Domingue, Bhushan, Gupta, Nagata, Shakya, Richter, Norris and Ngo2019; Ilic and Ilic, Reference Ilic and Ilic2022). Women are more vulnerable to common mental health problems, such as depression (GBD 2019 Mental Disorders Collaborators, 2022). According to previous research, the gender gap in depression is associated with both the distribution of statuses and roles for men and women, with an unequal exposure to social stressors and to cumulative advantages and disadvantages during the life course, which might increase gender inequalities in depression at old age (Bracke et al., Reference Bracke, Delaruelle, Dereuddre and Van de Velde2020). Previous studies about depression among the Chilean population have reported a considerable gender gap in the prevalence of depression from the 1990s to date (Araya et al., Reference Araya, Rojas, Fritsch, Acuña and Lewis2001; Vicente et al., Reference Vicente, Rioseco, Saldivia, Kohn and Torres2002; Markkula et al., Reference Markkula, Zitko, Peña, Margozzini and Retamal2017; Aravena et al., Reference Aravena, Saguez, Lera, Moya and Albala2020; Nazar et al., Reference Nazar, Gatica-Saavedra, Provoste, Leiva, Martorell, Ulloa, Petermann-Rocha, Troncoso-Pantoja, Celis-Morales and de Investigación ELHOC-Chile2021; Moreno et al., Reference Moreno, Gajardo and Monsalves2022a). Also, according to the estimates of the World Health Organization, depression is the main cause of years lost to disability and disability-adjusted life years (DALYs) for women in Chile, but it is not among the top 10 causes of DALYs for men (World Health Organization, 2021). The prevalence of depression is higher among women in Chile, but they are also more likely to access mental health care for depression compared to men (Vicente et al., Reference Vicente, Kohn, Saldivia, Rioseco and Torres2005; Aravena et al., Reference Aravena, Saguez, Lera, Moya and Albala2020; Moreno et al., Reference Moreno, Sánchez, Huerta, Cea, Márquez and Albala2022b). Additionally, the suicide rate among men was around 5 times as high as the rate among women between 2001 and 2018 (Bustamante et al., Reference Bustamante, Ramirez, Urquidi, Bustos, Yaseen and Galynker2016; Wiederkehr et al., Reference Wiederkehr, Mai, Cabezas, Rocha-Jiménez, Otzen, Montalva, Calvo and Castillo-Carniglia2022). Jiménez-Molina et al. (Reference Jiménez-Molina, Reyes and Rojas2021) found a socioeconomic gradient in the distribution of depressive symptoms among the urban adult population in Chile, which was more marked among women, considering level of education, occupation and household income. Another study found that people who reported unpaid domestic tasks as their main occupation were more likely to have depressive symptoms (González and Vives, Reference González and Vives2019). Also, people with a double role as workers and domestic caregivers were more than 3 times as likely to report depressive symptoms (Medina et al 2020).
There are no studies in Chile that have examined gender differences in the trends in depressive symptoms in the last two decades and assessed the impact of depression on health expectancies among the Chilean population. The analysis of health expectancies considers healthy and unhealthy years to be lived by a population or subgroup, taking into account specific health problems and life expectancy (Saito et al., Reference Saito, Robine and Crimmins2014). Although women have a longer life expectancy, the prevalence of depression is also higher among them (Salk et al., Reference Salk, Hyde and Abramson2017). Consistently, previous research has shown a differential impact of depression on healthy life expectancies, depending on gender, with women at all ages expecting to live a higher proportion of their life with depression (Andrade et al., Reference Andrade, Wu, Lebrão and Duarte2016; Alves and Pereira, Reference Alves and Pereira2018; García et al., Reference García, Garcia, Chiu, Rivera and Raji2019; Wu et al., Reference Wu, Zheng, Liu, Wang, Chen, Yu, Liu and Hu2021; Bramajo, Reference Bramajo2022).
To date, research about gender differences in health expectancies in Chile has focused on self-rated health and disability (Moreno et al., Reference Moreno, Lera and Albala2020, Reference Moreno, Lera, Moreno and Albala2021). A previous study found that the socioeconomic gradient in the proportion of years to be lived free of disability was more marked among women and increased with age (Moreno et al., Reference Moreno, Lera, Moreno and Albala2021). It is important to expand and update the existing evidence about a gender gap in the prevalence of depressive symptoms in Chile and to determine its impact on health expectancies. The aim of this study was to explore gender differences in life expectancy free of depressive symptoms among the adult population in Chile between 2003 and 2016.
Methods
This study is based on a secondary analysis of the National Survey of Health (NSH), a cross-sectional survey carried out in Chile in 2003, 2010 and 2016. The NSH is aimed at estimating the prevalence of the main health problems among the adult population in Chile and monitoring changes in the distribution of these problems among different sociodemographic groups (Ministerio de Salud n.d.a). Methodological characteristics of the NSH have been previously described (Moreno et al., Reference Moreno, Lera and Albala2020). Briefly, a nationally representative sample of people aged 17 years and above was recruited in the first wave in 2003 (Ministerio de Salud n.d.a). The samples recruited in the two last versions were representative of the Chilean population aged 15 years and above (Ministerio de Salud n.d.b, n.d.c). The three samples are representative of the rural and urban population. Stratified cluster random sampling was used in every wave. Hence, weights have been calculated to take into account this sampling design (Ministerio de Salud n.d.d).
Household interviews were carried out to collect the data. Sociodemographic and health variables were measured with a structured questionnaire. The main variables from the NSH considered in this study are gender (men or women), age and depressive symptoms. Depressive symptoms were measured with the Composite International Diagnostic Interview–Short Form (CIDI-SF) for Major Depression (Kessler et al., Reference Kessler, Andrews, Mroczek, Ustun and Wittchen1998). This is a screening tool for major depressive disorder, based on the fourth version of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) and the International Classification of Diseases (ICD-10) criteria (Pena-Gralle et al., Reference Pena-Gralle, Talbot, Trudel, Aubé, Lesage, Lauzier, Milot and Brisson2021). A cutoff score of 5 or more points, including dysphoria, anhedonia and at least three other symptoms, was used to determine the possible cases of major depressive disorder (Ministerio de Salud, 2018).
A set of variables measured in the NSH was used to carry out supplementary analyses to gain insights into structural variables related to gender roles and relations that could express social disadvantages (Hammarström et al., Reference Hammarström, Johansson, Annandale, Ahlgren, Aléx, Christianson, Elwér, Eriksson, Fjellman-Wiklund, Gilenstam, Gustafsson, Harryson, Lehti, Stenberg and Verdonk2014): marital status (married, single, divorced or widowed), area of residence (rural or urban), level of education (0-7 years: incomplete primary education, 8-11 years: incomplete secondary education or 12 years or above: complete secondary education or more) and occupation (employed, unemployed, student, unpaid domestic tasks or retired). Additionally, in 2010 and 2016, household head status and health insurance type were measured. Also, caregiving was included in 2016. Self-rated health was assessed in 2010 and 2016, and it was considered in these analyses as an indicator of general health status.
Analysis
The Sullivan method was used to calculate life expectancy free of depressive symptoms by gender for each wave of the NSH. Weighted prevalences of depressive symptoms for men and women were calculated. Abridged life tables for the Chilean population were retrieved from the Human Mortality Database. Our analyses considered people aged 20 or more years. To estimate life expectancy free of depressive symptoms, we first calculated the person-years to be lived without depressive symptoms as the product of person-years in each age-group by the proportion of people without depressive symptoms. Then, we calculated the total number of years without depressive symptoms by adding up the person-years without depressive symptoms of the successive age intervals. Finally, life expectancy free of depressive symptoms was the quotient of the total years free of depressive symptoms by the number of people surviving to the beginning age of the respective interval. We also calculated the proportion of life expectancy free of depressive symptoms and the difference between the proportion of life expectancy free of depressive symptoms in men and women. To estimate 95% confidence intervals (Cis), the standard error was calculated as the square root of the variance of life expectancy free of depressive symptoms, or as the addition of those standard errors, in the case of the difference between two proportions (Jagger et al., Reference Jagger, Oyen and Robine2014).
To examine the role of variables associated with social position on the gender gap in depression, we carried out supplementary analyses. We described and compared the distribution of sociodemographic and health variables that could interact with gender in the association with depressive symptoms. Chi-square test and t test were calculated to determine differences. Unadjusted and adjusted associations between each variable and depressive symptoms were estimated through logistic regression models. To explore the interaction between gender and other variables that could exacerbate or moderate the association between gender and depressive symptoms, a logistic model with interaction terms was performed, followed by the calculation of average marginal effects of depressive symptoms for different categories of the selected variables, to estimate the difference in the predicted probability of the outcome between men and women (Else-Quest and Hyde, Reference Else-Quest and Hyde2016).
The study protocol of the NSH was approved by the Ethics Committee of the Pontificia Universidad Católica de Chile (Pontifical Catholic University of Chile). Participants signed an informed consent before entering the study. Anonymized databases of the NSH are publicly available from the Chilean Ministry of Health website.
Results
The sample size of people aged 20 or more years in 2003 was 3462, of whom 3400 (98.2%) had data on depressive symptoms. In 2010, the sample size of people of the same age was 5069, and 5052 (99.7%) of them had data on depressive symptoms. In 2016, 5834 people were recruited, with no missing data on depressive symptoms.
In 2003, the prevalence of depressive symptoms among people aged 20 years and above was 17.8% (95% CI, 15.8%–19.9%). Considering the same age-group, the prevalence of depressive symptoms in 2016 was 15.6% (95% CI, 13.9%–17.4%) and 14.5% (95% CI, 12.7%–16.4%) in 2016. As observed in Figure 1, depressive symptoms were more frequent among women of all ages in every year. Statistically significant gender differences in prevalence were observed every year between ages 40 and 59 and for the group aged 30 to 39 in 2003 and 60 to 69 in 2010. The highest prevalence among women was observed in middle age (40 to 59 years), whereas the distribution of depressive symptoms among men varied by age-group and between years.

Figure 1. Prevalence of depressive symptoms in men and women in 2003, 2010 and 2016 in Chile and 95% confidence intervals.
Table 1 shows that men, until age 40, could expect to live more years free of depressive symptoms, compared to women, in the three years considered. Between 2003 and 2010, there was an increase in life expectancy free of depressive symptoms among men until 60 years, but this was not observed between 2010 and 2016, with the exception of men aged 60. In the case of women, an increase in life expectancy free of depressive symptoms was observed between 2010 and 2016 at all ages.
Table 1. Total life expectancy and life expectancy free of depressive symptoms in men and women, in 2003, 2010 and 2016 in Chile

LEFDS, life expectancy free of depressive symptoms; TLE, total life expectancy.
The proportion of life expectancy free of depressive symptoms was higher among men in every year and at all ages (Figure 2). Between 2003 and 2010, there was a compression of morbidity among middle-aged men (40–60 y). However, between 2010 and 2016, the proportion of life expectancy free of depressive symptoms decreased among men of all ages. Among women, the proportion of years to be lived free of depressive symptoms increased among women at younger (20–30 y) and older (60–70 y) ages. People aged 70 had a lower proportion of life expectancy free of depressive symptoms compared to younger ages.

Figure 2. Proportion of life expectancy free of depressive symptoms in men and women in 2003, 2010 and 2016 in Chile and 95% confidence intervals.
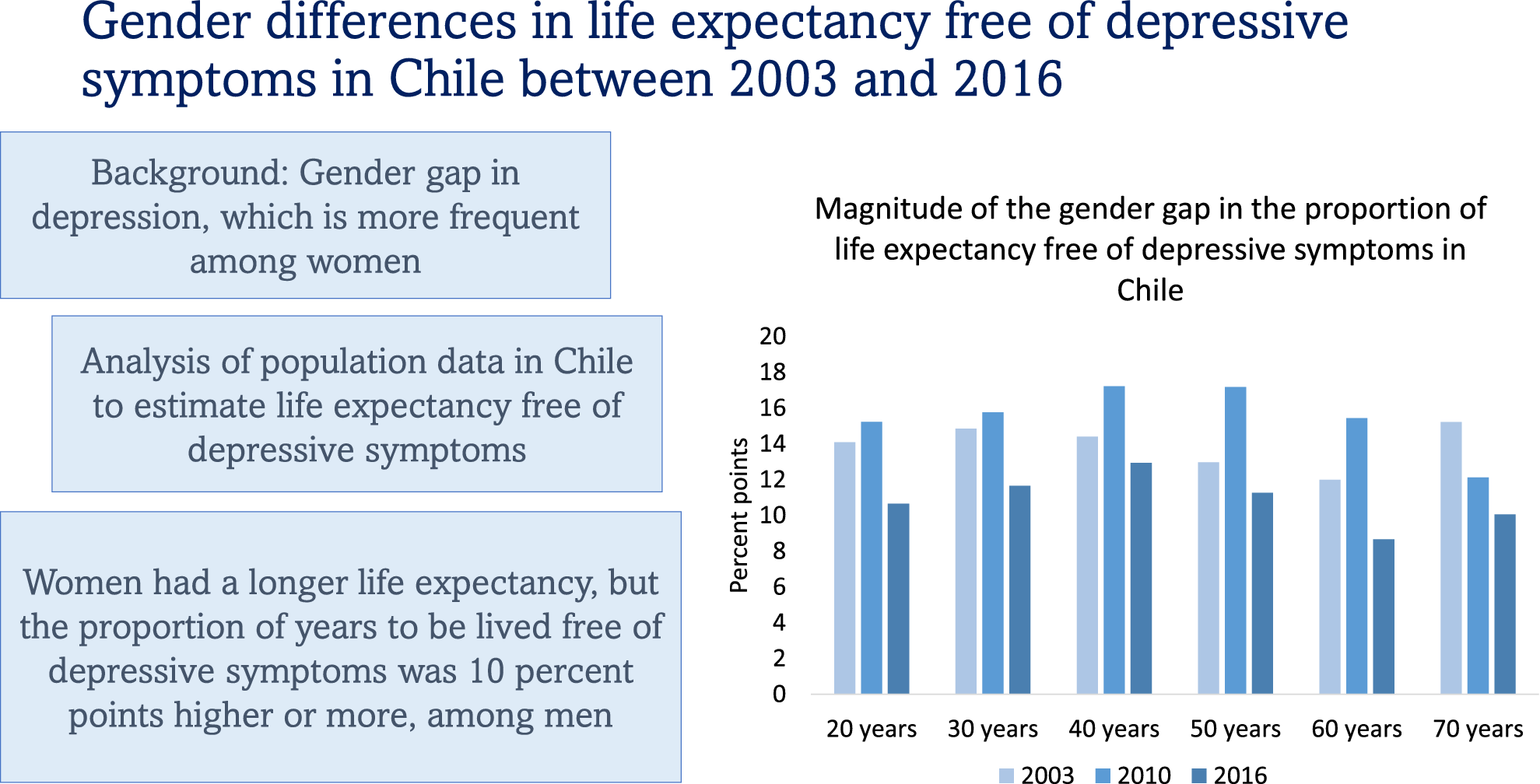
Although point estimates in Figure 3 suggest an increase in the gender gap between 2003 and 2010, and a subsequent decrease in 2016, these changes were not statistically significant, with the exception of a decrease between 2010 and 2016 among people aged 60. In every year and at all ages, but 60 years in 2016, the gender gap reached 10 percent points or more.

Figure 3. Absolute difference in the proportion of life expectancy free of depressive symptoms between men and women in 2003, 2010 and 2016 in Chile.
The supplementary analysis showed gender differences in the distribution of the selected variables across the three years (Supplementary material S1). Women were more frequently divorced or widowed compared to men, and men were more frequently married compared to women. Men more frequently reported to be the head of the household. A higher proportion of women reported incomplete primary education. In 2003, the proportion of men who reported being employed was more than twice as high as that of women, and the difference was still marked in 2016 (73.44% men; 42.41% women). In 2003, only women reported household tasks as their main occupation (51.09%), and the frequency of men who reported this occupation was remarkably low in 2010 (1.86%) and 2016 (1.24%). Women were more frequently in the lowest income group of health insurance, compared to men, whereas men were more frequently enrolled in the private health insurance system. In 2016, women were more frequently caregivers, particularly without receiving help (3.37% men; 22.99% women), compared to men. About half of women reported their health as less than good in 2010 and 2016 compared to near one-third of men.
In adjusted models (Supplementary material S2), women were more likely to have depressive symptoms compared to men (odds ratio [OR], 2.4 in 2003; OR, 2.13 in 2010; OR, 1.82 in 2016). The odds of depressive symptoms slightly decreased with age, and it was lower among people living in rural areas. However, when ethnicity was considered in 2016, area of residence was not associated with the outcome, and belonging to an indigenous group or nation decreased the likelihood of depressive symptoms. Unemployed people, and those who reported their health as less than good, more frequently had depressive symptoms. In 2003 and 2010, a higher level of education was negatively associated with depressive symptoms. Being single in 2003 and being divorced in 2010 were associated with higher odds of the outcome. According to the analysis of interactions, the gender gap in depressive symptoms was less marked among single people, compared to those who were married, and among those who lived in rural areas.
With respect to the average marginal effects (Table 2), as age increased, the predicted probability of depressive symptoms slightly decreased between 0.2 and 0.3 percent points among men and women and across the three years considered. In 2003, men and women with a higher level of education had a lower probability of depressive symptoms compared to those with a lower level of education, but the difference among women doubled the difference among men (10.58 and 5.22 percent points, respectively). In 2010, this difference between level of education was observed among women only, and it was half than that observed in the previous period. In 2003, unemployed women and men had a higher probability of depressive symptoms compared to those employed (7.15 percent points in men; 9.73 percent point in women). In 2010, the probability of the outcome was 13.03 percent points higher among unemployed women, and those who carried out unpaid domestic tasks also had a predicted probability of depressive symptoms which was 5.49 percent points higher compared to women who were employed. In 2003, men who lived in rural areas had a lower predicted probability of depressive symptoms compared to men living in urban areas, and the same was observed among women who lived in rural areas in 2010, but not among men. In 2016, women who belonged to an indigenous group or nation had a lower probability depressive symptoms. In 2010 and 2016, both men and women who reported less than good self-rated health had a higher predicted probability of the outcome, compared to people who rated their health as good, but the difference was more marked among women, reaching a difference of 20.91 percent points (14.32 in men) in 2010 and 11.48 percent points (8.92 in men) in 2016.
Table 2. Average marginal effects of depressive symptoms with statistical significance, by selected variables, in Chile

* p value < 0.05,
** p value < 0.01,
*** p value < 0.001.
Discussion
A persistent gender gap in life expectancy free of depressive symptoms was observed between 2003 and 2016 in Chile. Men until 40 years of age had a longer life expectancy free of depressive symptoms compared to women of the same age. Furthermore, women at all ages had a shorter proportion of years to be lived free of depressive symptoms. With respect to trends, a compression of morbidity among men aged 40 to 60 years was observed between 2003 and 2010. Among younger and older women, a compression of morbidity occurred between 2010 and 2016.
There is evidence that supports the association between gender inequalities and population health outcomes such as life expectancy, healthy life expectancy and DALYs (Veas et al., Reference Veas, Crispi and Cuadrado2021). Although women have an advantage in life expectancy, the pattern of morbidity varies by gender and age, and the evidence suggests that these differences are socially determined (World Health Organization, 2011; Crimmins et al., Reference Crimmins, Shim, Zhang and Kim2019). An analysis of data from Organization for Economic Co-operation and Development countries has concluded that public policies aimed at reducing gender inequalities could improve population health outcomes (Veas et al., Reference Veas, Crispi and Cuadrado2021). Gender inequalities are also associated with the gender gap in depression (Yu, Reference Yu2018). A study carried out in Europe found that in more gender unequal countries, a broader gap in depression was observed, with a cumulative effect of inequalities on this gender gap over the life course (Bracke et al., Reference Bracke, Delaruelle, Dereuddre and Van de Velde2020). Hence, in countries with marked gender inequalities, along with a considerable gender gap in depression, the difference broadened at older ages. Our results showed a significant gender gap not only in depressive symptoms but also in the proportion of life expectancy free of depressive symptoms, with a difference of 10 percent points or more, in spite of the advantage in life expectancy among women. However, there were no statistically significant differences by age within every year. Chile reached the 70th place out of 144, in the global index of the gender gap in 2016, and the place 119 in gender equality in economic participation and opportunity (World Economic Forum, 2016). Also, the gender inequality index was 0.395 in 2004, 0.339 in 2010 and 0.259 in 2016, below the world average, but above several European and Latin American countries (Human Development Reports n.d).
Although men experienced an initial compression of morbidity, this was not observed in the subsequent period. Previous studies suggest that men are more likely than women to develop depressive symptoms in the context of economic recession (Guerra and Eboreime, Reference Guerra and Eboreime2021). A systematic review found that income inequality is associated with depression in men but not in women (Yu, Reference Yu2018). The increase in the proportion of life expectancy free of depressive symptoms among men during the first period only could be associated with the economic context in Chile. During the first decade of this century, there was a higher per capita growth and a moderate reduction in economic inequalities, compared to previous years in Chile, followed by a drop in the gross domestic product in 2009 (Ffrench-Davis, Reference Ffrench-Davis2017).
The compression of morbidity among women, during the last period, is consistent with the findings of Bramajo (Reference Bramajo2022) in Argentina, who reported that the increase of healthy years among women in that country is associated with a compression of morbidity due to depression. We can hypothesize that this finding reflects, to a certain extent, the impact of the inclusion of depression in the Regime of Explicit Health Guarantees (GES) program of the Chilean Ministry of Health. Previous research has reported that after this program was implemented, there was an increase in the access to diagnosis and treatment of depression among women and those with lower levels of education (Araya et al., Reference Araya, Zitko and Markkula2018). Our supplementary analyses showed that in 2003, before the GES program was introduced, people with the lowest level of education had a higher probability of depressive symptoms, but the difference was more marked among women compared to men. In 2010, the difference still was present among women, but it decreased, and this difference was not observed in 2016. This trend could suggest that the GES program could have had an impact not only in reducing the morbidity among women, but it could have also partly reduced the gap in access to treatment by education level among women, with a reduction in the difference in prevalence in subsequent years. Previous research questions the impact of access to mental health care to reduce the prevalence of common mental disorders (Jorm et al., Reference Jorm, Patten, Brugha and Mojtabai2017), but Skinner et al. (Reference Skinner, Occhipinti, Song and Hickie2022) found in Australia a modest but significant effect of increasing access to care on population mental health, which was less apparent in periods of incidence of high psychological distress.
Although mental health policies of the last two decades in Chile have improved the access of women to depression treatment, our results have shown that the gender gap in life expectancy free of depressive symptoms persisted. A study about life expectancy free of depressive symptoms among older adults in Brazil, between 2000 and 2010, reported similar results (Andrade et al., Reference Andrade, Wu, Lebrão and Duarte2016). The existing evidence suggests that multiple dimensions, at different levels, intersect with gender and are associated with health outcomes (Hammarström et al., Reference Hammarström, Johansson, Annandale, Ahlgren, Aléx, Christianson, Elwér, Eriksson, Fjellman-Wiklund, Gilenstam, Gustafsson, Harryson, Lehti, Stenberg and Verdonk2014). During their life course, women are more likely to be in a position of social disadvantage, to have less access to education and to full-time employment, to carry out unpaid care work and to experience intimate partner violence (United Nations Women, 2018; Oram et al., Reference Oram, Fisher, Minnis, Seedat, Walby, Hegarty, Rouf, Angénieux, Callard, Chandra, Fazel, Garcia-Moreno, Henderson, Howarth, MacMillan, Murray, Othman, Robotham, Rondon, Sweeney, Taggart and Howard2022). Our descriptive analysis showed that women were more frequently divorced or widowed, a higher proportion had less than primary education, were less frequently employed and more likely to carry out unpaid domestic tasks, were more often enrolled in the low income group of public health insurance and were more frequently caregivers without receiving help (Supplementaty file 1). The findings of a Chilean study that observed that the socioeconomic gap in depressive symptoms was more marked in women (Jiménez Molina et al 2021) support the intersection of gender and other dimensions of social position to explain gender differences in depression. Accordingly, we found that lower education and unemployment increased the probability of depressive symptoms among men and women, but the effect was higher among women.
There are some recommendations for public policies that we can outline. In Chile, the GES program to improve the equity in access to diagnosis and treatment of depression is an important public health measure that, according to previous research, has improved the access to mental health care among women (Araya et al., Reference Araya, Zitko and Markkula2018). In line with that, in Chile, only 16.2% of people who are treated for depression are men (Aguayo, Reference Aguayo2022). Previous studies addressing depression in old age in Chile have found that between 28% and 32% of men with a positive screen for depression had not been diagnosed (Aravena et al., Reference Aravena, Saguez, Lera, Moya and Albala2020; Moreno et al., Reference Moreno, Gajardo and Monsalves2022a). Hence, it is important that this program develops a gender-based approach that considers intersectionality to increase the access among men. The hegemonic norms associated with masculinity make men less likely to acknowledge health needs and to search for health care (Etienne, Reference Etienne2018). Also, depression among men might have atypical symptoms or being masked as rage, which is a culturally more acceptable emotion for men (Aguayo, Reference Aguayo2022). Furthermore, it should be further assessed if, in spite of a higher access to mental health care among women, there are undetected inequalities for women as well. For instance, migrant population in Chile has a higher proportion of health uninsurance and lower consultation in case of accident or illness (Oyarte et al., Reference Oyarte, Cabieses, Rada, Blukacz, Espinoza and Mezones-Holguin2022). Previous research has shown that there is a broad mental health gap among women if socioeconomic position is considered (Jiménez-Molina et al., Reference Jiménez-Molina, Reyes and Rojas2021). Additionally, a marked socioeconomic gap in life expectancy among women in Chile has been reported, which is broader than that observed among men (Bilal et al., Reference Bilal, Alazraqui, Caiaffa, Lopez-Olmedo, Martinez-Folgar, Miranda, Rodriguez, Vives and Diez-Roux2019). Hence, we consider that public policies should address the intersection of different dimensions that underlie considerable gender inequalities in Chile, which are associated with gender differences in depression and in life expectancy free of depressive symptoms. As the international evidence suggests (Yu, Reference Yu2018; Bracke et al., Reference Bracke, Delaruelle, Dereuddre and Van de Velde2020), improving gender equality in Chile should decrease the gender gap in depression, and it should also decrease depression levels among men and women.
It is important to update the research about depression, life expectancy free of depressive symptoms and gender differences, considering more recent data. In Chile, an analysis considering data from 2016 to 2019 suggests an increasing trend of depressive symptoms among the population (Duarte and Jiménez-Molina, Reference Duarte and Jiménez-Molina2022). It is important to consider that a general deterioration in social and economic conditions in the country might have been occuring during that period, since Chile experienced a social uprising in 2019, just before the COVID-19 pandemic, with an impact on mental health (Fischman and Irarrazaval, Reference Fischman and Irarrazaval2020). An increase in psychological distress during two waves of the pandemics in 2020 was reported in Chile, affecting younger people and women more frequently (Duarte and Jiménez-Molina, Reference Duarte and Jiménez-Molina2022). A study that compared depressive symptoms among older adults, before and during the pandemics, found an increase between both periods (Herrera et al., Reference Herrera, Elgueta, Fernández, Giacoman, Leal, Marshall, Rubio and Bustamante2021). Furthermore, an analysis of data on the use of mental health services in Chile suggests that the demand for mental health care increased during the pandemics, but the admissions to the Regime of Explicit Health Guarantees program for people with depression and other mental health conditions decreased, resulting in a higher individual expenditure to access mental health care (Toro-Devia and Leyton, Reference Toro-Devia and Leyton2023).
This study has some limitations. As mentioned above, previous studies have shown gender differences in the marked socioeconomic gap in life expectancy in Chile (Bilal et al., Reference Bilal, Alazraqui, Caiaffa, Lopez-Olmedo, Martinez-Folgar, Miranda, Rodriguez, Vives and Diez-Roux2019) and in the socioeconomic gap of depressive symptoms (Jiménez-Molina et al., Reference Jiménez-Molina, Reyes and Rojas2021). However, we were not able to assess a socioeconomic gradient in the gender gap of life expectancy free of depressive symptoms due to a limited sample size to estimate the prevalence of depressive symptoms by other relevant categories, such as educational level or occupation and the unavailability of disaggregated population and mortality data to calculate life tables for those categories. The use of a screening test for depression is another limitation of this study. The CIDI-SF cannot rule out that the symptoms are due to other mental health problems or grief. However, previous studies about life expectancy free of depressive symptoms have used screening tools for depression (Drummond Andrade et al., Reference Andrade, Wu, Lebrão and Duarte2016) or self-reported diagnosis (Alves and Pereira, Reference Alves and Pereira2018; Wu et al., Reference Wu, Zheng, Liu, Wang, Chen, Yu, Liu and Hu2021). When interpreting the results of our study, it is important to take into account that the prevalence of depressive symptoms overestimates the prevalence of depression. Nevertheless, a previous study to assess the performance of the CIDI-SF in Canada reported that three quarters of participants with a positive screen were confirmed cases, according to the gold standard, and among those who did not fulfill the criteria for major depressive disorder, a proportion presented less severe depressive disorders (Patten et al., Reference Patten, Brandon-Christie, Devji and Sedmak2000).
Conclusions
Gender differences in depression have been previously reported, but only a few studies have addressed life expectancy free of depressive symptoms. This is the first study in Chile about the gender gap in life expectancy free of depressive symptoms. Although women had a longer life expectancy, men up to 40 years had a longer life expectancy free of depressive symptoms. A gender gap in the proportion of life expectancy free of depressive symptoms of 10 percent points or more was observed at almost all ages and periods. Public policies should consider the intersection of gender with other structural dimensions to improve gender equality, which has an impact on gender gaps in depression.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2024.9.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/gmh.2024.9.
Data availability statement
The data that support the findings of this study are openly available on the website of the Department of Epidemiology of the Chilean Ministry of Health, at http://epi.minsal.cl/bases-de-datos/, and on the website of the Human Mortality Databse webiste, at https://www.mortality.org/Country/Country?cntr=CHL.
Acknowledgements
This research analyzed information from the databases of the National Health Survey, which are Health Surveys for the epidemiological surveillance of the Chilean Undersecretary of Public Health. The authors acknowledge the Ministry of Health for providing access to the databases. The results of the study are responsibility of the authors, and they do not in any way commit that institution.
Author contribution
X.M. designed the study, analyzed the data and drafted the manuscript. X.M., M.J.M., P.D. and F.B. obtained funding to carry out the study. M.J.M. and S.R. contributed to interpret the results of the study and to draft the manuscript. M.J.M., S.R., P.D. and F.B. revised the manuscritpt. All authors approved the final version.
Financial support
The results reported in this article are part of a study funded by the Fourth Version of the Public Policies Award (Cuarto Concurso de Políticas Públicas) from the Instituto de Políticas Públicas en Salud de la Universidad San Sebastián (IPSUSS), project number 2535. SR was supported by the ANID Millennium Science Initiative Program (ICS2019_024).
Competing interest
The author declare none.
Ethics statement
The study protocol of the NSH was approved by the Ethics Committee of the Pontificia Universidad Católica de Chile (Pontifical Catholic University of Chile). Participants signed an informed consent before entering the study. Anonymized databases of the NSH are publicly available from the Chilean Ministry of Health website.








 Open access
Open access
Comments
Dear Editor-in-Chief
Please consider our research article ‘Gender differences in life expectancy free of depressive symptoms in Chile between 2003 and 2016’, for publication in Cambridge Prisms: Global Mental Health.
Gender differences in the prevalence of depression are broadly documented. However, research about life expectancy free of depressive symptoms is scarce, and this is the first study to address this topic in Chile. This is an important indicator of population health, both to assess differences between groups, and to monitor changes across time. We have estimated life expectancy free of depressive symptoms among Chilean men and women, between 2003 and 2016. During this period, national public programs aimed at improving the access to diagnosis and treatment of depression were implemented in Chile. Our results suggest a compression of morbidity for men and women, in different periods. Furthermore, we observed a persistent gender gap, with women expecting to live a higher proportion of their lives with depressive symptoms. We believe that the results of our study support the fact that mental health programs require an intersectoral approach and tailored interventions, to address the social determinants that underlie these inequalities.
This manuscript has not been published and is not under consideration by any other journal. All authors have approved both the manuscript, and this submission.
None of the authors have competing interests to declare in relation to the manuscript submitted.
Thank you for considering our manuscript. We appreciate your time and look forward to your response.
Best wishes,
The authors