


Introduction
A pregnancy that is either unwanted (i.e. occurred when no children, or no more children, were desired) or mistimed (i.e. occurred earlier than desired) at the time of conception is referred to as an unintended pregnancy (Abma et al., Reference Abma, Chandra, Mosher, Peterson and Piccinino1997). Unintended pregnancies harm women and their families through consequences like unsafe abortion, delayed prenatal care, poor maternal mental health, reduced mother–child relationship quality, poor developmental outcomes for children, physical abuse and violence against women, increased risk of low birth weight as well as increased maternal morbidity and mortality (Santelli et al., Reference Santelli, Rochat, Hatfield-Timajchy, Gilbert, Curtis, Cabral and Schieve2003; Singh et al., Reference Singh, Sedgh and Hussain2010; US Department of Health and Human Services & Health Resources and Services Administration, 2011). Beyond the direct health consequences, unintended pregnancies also contribute to unwanted population growth, which consequently compromises provision of adequate social services (Bradley et al., Reference Bradley, Croft and Rutstein2011). A study using data from the 2011 Nepal Demographic and Health Survey (NDHS 2011) showed that unintended pregnancy could have negative health consequences for mothers as well as newborns (Singh et al., Reference Singh, Singh and Thapa2013b). Similarly, studies from India showed that the consequences of unintended pregnancy could go as far as resulting in stunting alongside the immediate negative effect on vaccination (Singh et al., Reference Singh, Chalasani, Koenig and Mahapatra2012; Singh et al., Reference Singh, Singh and Mahapatra2013a), most probably as a result of the disadvantage the unwanted children face. The issue of disadvantage and neglect was explored in a multi-country study and the results in some of those countries suggested that not only were the unwanted children more likely to be stunted and less likely to be fully immunized, but the mothers were also less likely to receive antenatal care and supervised delivery (Marston & Cleland, Reference Marston and Cleland2003). A study from Bangladesh showed that the rates of neonatal and postnatal mortality were higher among unwanted children (Chalasani et al., Reference Chalasani, Casterline and Koenig2007).
In 2008, 41% of the 208 million pregnancies estimated worldwide were unintended (Singh et al., Reference Singh, Sedgh and Hussain2010). Among women aged 15–44 years in low- and middle-income countries, the rates of unintended pregnancies declined by 20% from 71 to 57 per 1000 from 1995 to 2008 (Singh et al., Reference Singh, Sedgh and Hussain2010). However, the figures are still high. In Nepal, 26.0% of the births corresponding to the period 2006–2011 were reported to be unintended (Ministry of Health and Population [Nepal] et al., 2012; Singh et al., Reference Singh, Singh and Thapa2013b). However, evidence shows that the actual level of unintended pregnancy could be much higher as retrospectively collected data on unintended pregnancies are known to be biased downward by as much as 11.5 percentage points (Koenig et al., Reference Koenig, Acharya, Singh and Roy2006). Some authors have presented the estimate of total unintended pregnancies in Nepal to be between 230,000 and 342,000 in 2011 (Singh et al., Reference Singh, Singh and Thapa2013b).
Some studies have explored the factors that are associated with unintended pregnancy. A study from Tanzania showed that young age (<20 years) was a significant predictor of both mistimed and unwanted pregnancies (Exavery et al., Reference Exavery, Kanté, Njozi, Tani, Doctor, Hingora and Phillips2014). A study conducted among low-income urban women in India showed that the risk of unintended pregnancy existed because of non-use of contraception resulting from the belief that they could not get pregnant (Kumar et al., Reference Kumar, Jyoti, Aruna, Poddar, Dhariwal and Shailendra2012).
It is important to understand unwanted and mistimed pregnancy as different aspects of unintended pregnancy and fertility as they have been found to have had differing effects on pregnancy outcomes. In general, mistimed pregnancies have been found to have better health outcomes for mothers and infants compared with unwanted pregnancies. It has been observed that women who carry a mistimed pregnancy to term are less likely to receive delayed prenatal care, to smoke and consequently to give birth to low-birth-weight infants compared with women who carry an unwanted pregnancy to term (D’Angelo et al., Reference D’Angelo, Gilbert, Rochat, Santelli and Herold2004). However, a seriously mistimed pregnancy resulting in a live birth (more than 24 hours) has been found to have had more serious consequences than a slightly mistimed pregnancy resulting in a live birth (less than 24 hours) (Pulley et al., Reference Pulley, Klerman, Tang and Baker2002).
Despite these differences, the precursors and effects of unintended pregnancies have usually been studied by lumping the data for unwanted and mistimed pregnancies together (Eggleston, Reference Eggleston1999; Beck et al., Reference Beck, Morrow, Lipscomb, Johnson, Gaffield, Rogers and Gilbert2002; Faye et al., Reference Faye, Speizer, Fotso, Corroon and Koumtingue2013; Ikamari et al., Reference Ikamari, Izugbara and Ochako2013), with some exceptions (Adams et al., Reference Adams, Bruce, Shulman, Kendrick and Brogan1993; Dye et al., Reference Dye, Wojtowycz, Aubry, Quade and Kilburn1997; Hellerstedt et al., Reference Hellerstedt, Pirie, Lando, Curry, McBride, Grothaus and Nelson1998; Kost et al., Reference Kost, Landry and Darroch1998; Joyce et al., Reference Joyce, Kaestner and Korenman2000). Doing this undermines the importance that unwanted and mistimed pregnancies have in their own right and also misses exploration of the conditions under which they occur. Since these two aspects differ from each other in many regards, their separate analysis is more likely to better reflect women’s pregnancy intentions and thus be more useful in understanding the overall impact of unintended pregnancy (Santelli et al., Reference Santelli, Rochat, Hatfield-Timajchy, Gilbert, Curtis, Cabral and Schieve2003).
Although an attempt has been made to explore the consequences of unintended pregnancies among Nepali women using NDHS 2011 data (Singh et al., Reference Singh, Singh and Thapa2013b), evidence has yet to be generated on what factors are predisposing mistimed pregnancy and unintended pregnancy separately among Nepali women. The study thus aims to fill that knowledge gap. Additionally, since studies have reported that intendedness of pregnancy helps in predicting the utilization of maternity services (Fotso et al., Reference Fotso, Ezeh, Madise, Ziraba and Ogollah2009; Wado et al., Reference Wado, Afework and Hindin2013) and also significantly affects maternal and newborn health alongside childcare practices (Joyce et al., Reference Joyce, Kaestner and Korenman2000; Korenman et al., Reference Korenman, Kaestner and Joyce2002), knowledge about predictors of unintended pregnancy could be useful to health managers in designing interventions for child spacing and fertility limiting, targeting needy areas and population groups.
Methods
The NDHS 2011 (http://dhsprogram.com/Data/) was the sixth round of the nationally representative, comprehensive demographic and health survey in Nepal. The survey had a two-stage cluster sampling design. At the first stage, the country was divided into thirteen sample domains, and these were further divided into 25 sample strata. Secondly, 289 sampling units were created in sample strata as primary sampling units (PSUs). Households were selected randomly from the PSU according to the probability-proportionate-to-size technique. The overall response rate for the NDHS 2011 was 97.6%. Details of the survey and sampling procedure have been published elsewhere (Ministry of Health and Population [Nepal] et al., 2012). This analysis is based on the child dataset of the NDHS 2011. A total of 5391 women of reproductive age (15–49 years) who had become pregnant within five years before the survey were included in the analysis. The analysis considered only the latest pregnancy experienced by women.
Definitions of variables
During the survey, participants were asked about their intention of becoming pregnant at the time when they became pregnant. The first question was: ‘When you got pregnant, did you want to get pregnant at that time?’ The response was coded as (1) yes or (2) no. If the answer was yes, it was labelled as an ‘intended pregnancy’. If the answer was no, the participants were further asked: ‘Did you want to have a baby later on or did you not want any [more] children?’ The response was recorded as (1) later or (2) no more. The response ‘later’ was categorized as ‘mistimed’ and the response ‘no more’ was categorized as ‘unwanted’ pregnancy.
Independent variables were selected based on literature review (Scott & Binns, Reference Scott and Binns1999; Adhikari et al., Reference Adhikari, Soonthorndhada and Prasartkul2009; Khanal et al., Reference Khanal, Sauer and Zhao2013c; Singh et al., Reference Singh, Singh and Thapa2013b). Three specific geographical variables were used: place of residence (urban, rural), ecological zone (mountain, hill, terai) and administrative regions (Eastern, Central, Western, Mid-Western and Far-Western development region). The development regions are the five north–south vertical divisions of the country. The Central development region is where the capital of the country is situated. Regions vary in their development status (Government of Nepal et al., 2014)
Some other socio-demographic variables were also included. Women’s education status was categorized into ‘no education’, ‘primary education’ and ‘secondary/higher education’, and husband’s education was categorized in accordance with woman’s education status. Participant’s occupation was categorized as ‘not working’, ‘agriculture’ and ‘other paid jobs’ (Khanal et al., Reference Khanal, Adhikari, Sauer, Zhao, Egata, Berhane and Heyman2013b). Likewise, husband’s occupation was divided into three categories: ‘agriculture’, ‘paid job’ and ‘other’. If a woman read newspapers or listened to radio or watched television more than once a week she was considered as having some exposure to mass media; otherwise she was labelled as having had no exposure (Singh et al., Reference Singh, Singh and Thapa2013b). Women’s autonomy represented women’s involvement in the household-level decision-making process, including decisions about: own health care, large household purchases, visiting family and relatives and what to do with the money their husband earns. Women who said that they could make household-level decisions by themselves on all four areas were considered to have full autonomy, women having no involvement in any decision-making were coded as having no autonomy, and the rest were coded as having some autonomy (Singh et al., Reference Singh, Singh and Thapa2013b). Ethnicity was first classified into seven groups according to the classification criteria used by the NDHS (Bennett et al., Reference Bennett, Dahal and Govindasamy2008) and was further grouped into three categories (relatively advantaged ethnicities including Brahmin and Chhetri, relatively disadvantaged ethnicities including Newar, Janajati, Muslims, Madheshi and other unidentified ethnicities, and the disadvantaged including Dalits). Wealth quintile was calculated using principal component analysis (Vyas & Kumaranayake, Reference Vyas and Kumaranayake2006) and was divided into five equal categories (poorest, poorer, middle, richer and richest), each comprising 20% of the population. In this analysis the quintiles were re-coded into three categories to form an economic status variable: the lowest 40% (poorest and poor) as poor; the middle 40% (middle and rich) as middle; and the upper 20% (richest) as rich (see Agho et al., Reference Agho, Dibley, Odiase and Ogbonmwan2011; Khanal et al., Reference Khanal, Adhikari, Sauer, Zhao, Egata, Berhane and Heyman2013b).
Some fertility-related variables including women’s age (<20 years, 20–34 years, ≥35 years) and parity (1, 2, 3 or more) were also included in the analysis. Women were classified into two groups on the basis of their knowledge about ovulation: knowledgeable and not knowledgeable. If the participants knew that the fertile period lies in the middle of the menstruation cycle they were considered knowledgeable; not knowledgeable otherwise. Participants were grouped into the categories of ‘current user’, ‘intend to use in future’ and ‘do not intend to use in future’ based on their intention to use family planning services. A visit to family planning workers within the past 12 months (yes, no) was also included in the analysis.
Statistical analysis
Analysis was performed using STATA 13.0 and using the survey analysis technique, considering sample weight assigned by the NDHS and cluster design. Explorative descriptive analysis was performed for sample distribution. The chi-squared test was used to assess the association between background characteristics and mistimed and unwanted pregnancy. Adjusted odds ratios and 95% CI of adjusted odds ratios were calculated using multiple logistic regression for each dependent variable. Standard errors were calculated by the Taylor linearization method. Statistical significance was at p<0.05.
Ethical clearance
The NDHS obtained ethical approval from the Nepal Health Research Council, Kathmandu, Nepal and Macro Institutional Review Board, MD, USA (Ministry of Health and Population [Nepal] et al., 2012). Written consent was obtained from the participants before interview. The Measure DHS Program granted authorization to analyse the DHS dataset. Therefore, no separate ethical approval was needed for this study.
Results
Participant characteristics
The results are based on a total of 5391 weighted women of reproductive age who had experienced at least one pregnancy within the five years before the survey. More than nine in every ten participants were from rural areas (90.66%), and the majority of them (52.55%) were from the terai ecological zone. About half of the participant women (47.29%) and nearly a quarter (23.74%) of the participants’ husbands had no school education. The majority of respondents (68.49%) were involved in agriculture and slightly more than half (54.42%) had some access to mass media. More than a quarter (26.76%) had no autonomy in decision-making at the household level. Nearly one in two (47.71%) belonged to the poor economic status group. About two-thirds (65.62%) were 20–34 years old, only 22.81% had knowledge about the ovulatory cycle and one-fifth (21.45%) had visited a family planning worker within the past 12 months (Table 1).
Table 1 Background characteristics of study participants (NDHS 2011), N=5391

a Weighted total.
Characteristics of women experiencing mistimed and unwanted pregnancies
Of the total respondents, 75.41% intended to become pregnant, 13.30% said their last pregnancy was unwanted and 11.29% said their last pregnancy was mistimed (Table 2). Surprisingly, the percentage of women reporting mistimed pregnancy was greater among women with primary or secondary education compared with women with no education, and a similar trend was observed for partner’s education status. The proportion of mistimed pregnancy was higher in the rich wealth quintile in comparison with middle and poor quintiles. Women less than 20 years of age were found to be more likely to report mistimed pregnancy in comparison with other age groups. The percentage of women reporting mistimed pregnancy was virtually equal, irrespective of whether they had visited a family planning worker (Table 3).
Table 2 Intendedness of last pregnancy among the women who became pregnant within the five years before the survey (NDHS 2011), N=5391

a Weighted total.
Taylor linearization method was used to estimate the standard error.
CI: confidence interval.
Table 3 Percentage distribution of women who experienced mistimed or unwanted pregnancy within the five years before the survey (NDHS 2011), N=5391
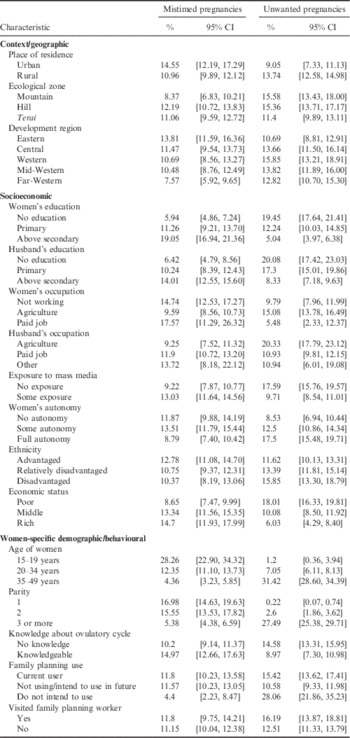
CI: confidence interval.
Unlike mistimed pregnancy, the proportion of women reporting unwanted pregnancy was found to decrease with an increase in women’s education, their partner’s education and in rich wealth quintile. Contrary to what was observed in the case of mistimed pregnancy, women from higher age groups experienced more unwanted pregnancy in comparison to the younger age group (Table 3).
Factors influencing mistimed pregnancies
The odds of mistimed pregnancy were higher in the hill ecological zone (OR: 1.40; 95% CI: 1.00, 1.95) in comparison with mountain and terai zones. Of the five development regions, the Western and Far-Western development regions (OR: 0.54; 95% CI: 0.39, 0.75) had significantly lower odds of mistimed pregnancy. The odds of mistimed pregnancy were higher among women with primary education (OR: 1.55; 95% CI: 1.11, 2.16) and those with above-secondary education (OR: 3.10; 95% CI: 2.16, 4.46) in comparison with women with no education. The odds of mistimed pregnancy were found to be lower among the women who had some exposure to mass media (OR: 0.76; 95% CI: 0.60, 0.97) and women who worked in agriculture (OR: 0.70; 95% CI: 0.53, 0.93) compared with their counterparts. The odds of reporting mistimed pregnancy were lower among women with full autonomy (OR: 0.70; 95% CI: 0.51, 0.98). The odds of mistimed pregnancy were significantly lower among women aged 24–34 years (OR: 0.40; 95% CI: 0.28, 0.56) and further decreased for women aged 35–49 years (OR: 0.19; 95% CI: 0.12, 0.32) compared with young women (15–19 years). Women who had already given birth three or more times had lower odds of mistimed pregnancy (OR=0.52; 95% CI 0.29, 0.92) compared with women who had given birth just once (Table 4).
Table 4 Factors associated with mistimed and unwanted pregnancies among women who became pregnant within five years before the survey (NDHS 2011), N=5391
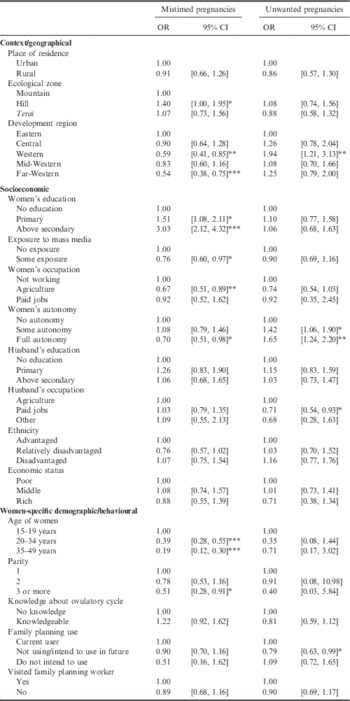
OR=odds ratio; CI=confidence interval.
*p<0.05; **p<0.01; ***p<0.001.
Factors influencing unwanted pregnancies
Geographically speaking, the Western development region had the highest odds of unwanted pregnancy (OR: 1.94; 95% CI: 1.21, 3.13). Partner’s occupation was found to be associated with unwanted pregnancy. The odds ratio was lower among women with husbands having paid jobs (OR: 0.71; 95% CI: 0.54, 0.93). Non-user women with an intention to use contraception in the future had lower odds of unwanted pregnancies (OR: 0.79; 95% CI: 0.63, 0.99) compared with current users (Table 4).
Discussion
Because of many undesirable consequences for the health of women and children, along with several far-reaching social and economic consequences, unintended pregnancy qualifies as an important public health issue. Identification of the factors influencing unintended pregnancy can prove useful in developing policies and designing programmes aimed at women who are at high risk of such pregnancies. This study aimed to discern some of the factors influencing the two aspects of unintended pregnancy – unwanted and mistimed pregnancy – separately, by utilizing data from the nationally representative demographic and health survey of Nepal.
Trends in unintended pregnancies
About a quarter of the pregnant women reported that their last pregnancy was unintended. The proportion of women that reported mistimed pregnancy (11.2%) was slightly less than that of women who reported unwanted pregnancy (13.4%). Previous demographic surveys showed fairly unchanged proportions of mistimed pregnancy: 13.8% and 14.4% in 2001 and 2006 respectively. However, the proportion of reported unwanted pregnancy was 26.1% in 2001, and it further reduced to 16.4% in 2006 (Ministry of Health [Nepal] et al., 2002; Ministry of Health and Population [Nepal] et al., 2007). The reduced reporting of unwanted pregnancies between the three consecutive NDHSs might be because of the decline in total fertility rate (TFR), from 4.1 in 2001 to 2.6 in 2011, i.e. reduction in the number of total births per woman. It could be further explained by an increase in the contraceptive prevalence rate (CPR) of modern methods from 35.5% in 2001 to 43.2% in 2011 (Karki & Krishna, Reference Karki and Krishna2008; Kumar et al., Reference Kumar, Jyoti, Aruna, Poddar, Dhariwal and Shailendra2012; Ministry of Health [Nepal] et al., 2002; Ministry of Health and Population et al., 2007).
Geographical area and unintended pregnancies
Whether the women were from rural or urban areas had no significant association with either mistimed or unwanted pregnancy. A separate analysis among currently pregnant women from the NDHS 2001 also reported no significant difference in the likelihood of unintended pregnancy according to the urban/rural distribution (Adhikari et al., Reference Adhikari, Soonthorndhada and Prasartkul2009).
Women from the hill region had higher odds of mistimed pregnancy. This finding could potentially be related to a finding from the NDHS Reference Agho, Dibley, Odiase and Ogbonmwan2011, that the use of traditional contraceptive methods (such as withdrawal) in the hill region was higher (6.2%) than in the mountains (3.8%) and terai (4.9%). Furthermore, the lower level of demand satisfaction with the use of modern methods in this region (51.7%) compared with the mountain (58.4%) and terai regions (58.8%) over the same period also adds to the argument (Ministry of Health and Population [Nepal] et al., 2012). Significantly lower odds of mistimed pregnancies were observed in the Western and Far-Western development regions. For the Far-Western region, this finding is in agreement with a sharp decline in TFR in the region between 2006 and 2011, alongside a fairly high CPR compared with the national standard. On the other hand, this analysis showed significantly higher odds of unwanted pregnancy in the Western development region. However, a decent decline in TFR in the Western development region, alongside a 6% increase in CPR between 2006 and 2011 (Khanal et al., Reference Khanal, Shrestha, Pant and Mehata2013a), makes these findings of effects in opposite directions for mistimed and unwanted pregnancies in the same region difficult to explain. The reason behind it could be a separate topic of enquiry and the results should be interpreted with caution.
Education level and unintended pregnancies
The high likelihood of mistimed pregnancy among women with primary or above secondary education was unexpected but similar to the findings of studies from adjoining states in India (Sebastian et al., Reference Sebastian, Khan and Sebastian2014), Jordan (Kiersten et al., Reference Kiersten, Zoubi and Wulfe2004) and Ecuador (Odimegwu, Reference Odimegwu1999). High but not differential relative risk was observed in Tanzania (Exavery et al., Reference Exavery, Kanté, Njozi, Tani, Doctor, Hingora and Phillips2014). It can potentially be explained by the high percentage of unmet need for family planning among educated women (Sebastian et al., Reference Sebastian, Khan and Sebastian2014) and also because educated women might have more modest expectations of their ability to control the timing of their pregnancies (Odimegwu, Reference Odimegwu1999). This could also be simply because more educated women are more likely to be candid in reporting their last pregnancy as mistimed. On the other hand, no significant association was seen between the education level of the respondent women’s husbands and the likelihood of either mistimed or unwanted pregnancy. No significant difference was observed between the ethnicity and economic status of the respondent and the odds of either mistimed or unwanted pregnancy.
Employment and unintended pregnancies
Women involved in agriculture (both employed and self-employed) were less likely to report mistimed pregnancy. This could, in general, be because women working in agriculture might be less likely to label a given pregnancy as mistimed due to having higher fertility aspirations as more children could possibly mean more helping-hands. But at the same time, that might contradict the argument that women contributing to the labour force tend to have fewer children (Siegel, Reference Siegel2012) and are more likely to use contraceptives (World Health Organization & UNICEF, 1993; Shapiro & Tambashe, Reference Shapiro and Tambashe1994; Miles-Doan & Brewster, Reference Miles-Doan and Brewster1998). Contrary to expectation, no significant difference was found in the odds of mistimed pregnancy between women with no occupation and those with paid jobs.
In this study, a woman whose husband was in a paid job was found to be less likely to experience unwanted pregnancy compared with her counterparts. Economic deprivation, having an unemployed husband and being in an inappropriate job have been found to be associated with increased likelihood of unwanted pregnancy (Naravage et al., Reference Naravage, Vichit-Vadakan, Sakulbumrungsil and Van der Putten2005; Todd et al., Reference Todd, Mountvarner and Lichenstein2005; Ayoola et al., Reference Ayoola, Brewer and Nettleman2006). A Zimbabwean study has shown that women whose husbands earned no income were at higher risk of unwanted pregnancy (Mbizvo et al., Reference Mbizvo, Bonduelle, Chadzuka, Lindmark and Nystrom1997). A similar result was found by a study in Egypt (Shaheen et al., Reference Shaheen, Diaaeldin, Chaaya and El Roueiheb2007). Husband’s involvement in a paid job could contribute towards preventing unwanted pregnancy, either as a proxy for better education and/or in attempting to maintain a stable family under given financial limits.
Women’s autonomy and unintended pregnancies
Lower odds of mistimed pregnancies among women with full autonomy can be explained by empowered women having strong participation in their household decisions and are also more likely to have a strong role in planning their pregnancy. A study based on the Bangladesh DHS observed that autonomous women were more likely to discuss contraceptive methods with their spouses, and more likely to use modern family planning services or intend to do so in the future (Rahman et al., Reference Rahman, Mostofa and Hoque2014). Women with autonomy can decide themselves or jointly with their partners about the timing of a pregnancy, reducing the probability of having mistimed pregnancies.
This study found women’s autonomy to be a significant predictor of unwanted pregnancy. But contrary to what might be expected, and what has been suggested in the literature (Mason, Reference Mason1987) about the direction of association, the likelihood of unwanted pregnancy was found to increase with an increase in the level of autonomy. However, a similar finding was found in a previous study that employed NDHS data (Adhikari et al., Reference Adhikari, Soonthorndhada and Prasartkul2009). This is potentially a reflection of the fact that women with increased autonomy might be more likely to label a past pregnancy as unwanted (because of lower fertility aspirations) and not necessarily that more autonomous women are at increased risk of unwanted pregnancy (D’Angelo et al., Reference D’Angelo, Gilbert, Rochat, Santelli and Herold2004).
Age, parity, mass media exposure, knowledge about ovulation, contraceptive use and unintended pregnancies
Young women were more likely to report mistimed pregnancies and this finding is in line with the findings of previous studies (D’Angelo et al., Reference D’Angelo, Gilbert, Rochat, Santelli and Herold2004; Kiersten et al., Reference Kiersten, Zoubi and Wulfe2004; Takahashi et al., Reference Takahashi, Tsuchiya, Matsumoto, Suzuki, Mori and Takei2012). This could potentially be explained by the argument that for young women, the purpose of sexual intercourse might be other than childbearing, and pregnancy could represent the undesired consequence of such sexual relationships (Exavery et al., Reference Exavery, Kanté, Njozi, Tani, Doctor, Hingora and Phillips2014).
The odds of mistimed pregnancy among women who had already given birth three times or more were lower. Similar results were obtained from an earlier study in the United States (D’Angelo et al., Reference D’Angelo, Gilbert, Rochat, Santelli and Herold2004). After having a desired number of children, women want to limit their fertility and succeeding pregnancies are more likely to be perceived as unwanted pregnancies rather than mistimed pregnancies (D’Angelo et al., Reference D’Angelo, Gilbert, Rochat, Santelli and Herold2004). However, this study does not confirm the higher likelihood of reporting unwanted pregnancies compared with reporting mistimed pregnancies among women who have had three or more previous childbirths. Although the finding was not statistically significant, this study found that the number of children the women previously had has a strong predictive effect on whether the index pregnancy was wanted or not. A similar finding was observed in a previous study by Kiersten et al. (Reference Kiersten, Zoubi and Wulfe2004).
The lower odds of mistimed pregnancies among women who had access to mass media can be explained by the role these have in the promotion of family planning services. Radio and television are the most widely accessed forms of mass media in Nepal, and women’s access to these has been found to be associated with a high rate of contraceptive method use elsewhere (Westoff & Rodriguez, Reference Westoff and Rodriguez1995; Odimegwu, Reference Odimegwu1999). This study found no significant association between women’s knowledge about the ovulatory cycle and the reporting of mistimed and unwanted pregnancies. However, women who were not using any contraceptive device at present but who had an intention to use one in the future were significantly less likely to have had an unwanted pregnancy. Intention to use family planning measures among current non-users is a summary indicator of attitude towards contraception and thus could reflect women’s awareness about unwanted pregnancy and preparedness to avoid it (Kiersten et al., Reference Kiersten, Zoubi and Wulfe2004). However, this finding contradicts what was found in an analysis of Morocco DHS data, which argued that when fertility preferences are weakly held, even the intentions shown at a point in time do not necessarily get reflected in action in the future (Curtis & Westoff, Reference Curtis and Westoff1996). Although not statistically significant, women’s visit to a family planning worker in the past 12 months showed no difference in their having had mistimed or unwanted pregnancies.
Strengths and limitations of this study
This is a population-based study using nationwide survey data with a relatively large sample size, thus promising better precision and external validity. The findings represent the intendedness of the last pregnancy of women who became pregnant within the five years before the survey, not only currently pregnant women. Therefore, the findings are comparable with studies conducted elsewhere. Unlike previous research, segregated analysis for mistimed and unwanted pregnancies was done, which means that the findings could be useful in designing interventions for child spacing and fertility limiting, targeting needy areas and population groups. It should be noted that this is a cross-sectional study; therefore a causal inference to any of the factors is not possible. Similarly, the chances of some recall bias cannot be overruled because women who became pregnant within the five years before the survey were interviewed for the purpose of this study. The magnitude of mistimed and unwanted pregnancies may therefore be underestimated, a suggestion also made by other researchers (Koenig et al., Reference Koenig, Acharya, Singh and Roy2006; Singh et al., Reference Singh, Singh and Thapa2013b).
Conclusion
Separate analysis for mistimed and unwanted pregnancies was done in this study. This can be justified since the effect on mistimed and unwanted pregnancies was seen to be different for variables like development region, women’s education status and women’s autonomy. However, due to the overall pervasiveness of unintended pregnancies in the study populations, differences became significant only between certain sub-populations. Addressing the factors identified in this study through a nationwide integrated approach could help reduce mistimed and unwanted pregnancies among Nepali women.
Acknowledgments
The authors are grateful to the Measure DHS program for providing access to the dataset. The authors’ sincere thanks go to all the women who participated in the survey.





 Open access
Open access