



Highlights
What is already known?
The CBM for NMA assumes treatment contrasts are exchangeable across the included studies, while the BM further assumes the baseline (or reference) treatment’s outcome level is also exchangeable across trials. A recent study showed that these two models may yield different results when the baseline risks vary across different designs of studies that compared different sets of treatments.
What is new?
We show that a key distinction between these two NMA models is similar to Lord’s Paradox, a statistical conundrum about whether a t-test or ANCOVA should be used to compare two groups according to a change in the outcome. We show that the CBM uses the observed treatment contrasts as the outcome in the analysis, while the BM uses adjusted treatment contrasts as the outcome. Alternatively, the CBM estimates the unconditional differences between one treatment and the baseline treatment, while the BM estimates the conditional difference by adjusting for the baseline effects.
Potential impact for RSM readers
The two NMA models make different assumptions about the relationship between treatment contrasts and the reference treatment effects. These differences in statistical assumptions reflect different perspectives on how the data were generated and how treatments impact patients. Therefore, choosing the appropriate model should depend on evaluating the validity of these assumptions in real-world scenarios.
1 Introduction
Network meta-analysis (NMA) combines direct and indirect evidence to compare the benefits and harms of multiple treatments.Reference Dias, Sutton, Ades and Welton 1 – Reference Salanti 3 Several approaches have been proposed to estimate relative effects between treatments; differences in their model specifications reflect different assumptions about how treatments should be compared.Reference Hong, Chu, Zhang and Carlin 4 , Reference White, Turner, Karahalios and Salanti 5 The contrast-based model (CBM), also called the Lu and Ades model, uses the difference in outcome between a pair of treatments in a given study, i.e., a treatment contrast, as the unit of analysis, assuming that a given treatment contrast is exchangeable across studies.Reference Shih and Tu 6 , Reference Tu 7 The baseline model (BM) further assumes that the reference treatment’s outcome levels are exchangeable across studies.Reference Dias, Sutton, Ades and Welton 1 , Reference White, Turner, Karahalios and Salanti 5 Although these two models are closely related, there has been debate as to which should be preferred.Reference Hong, Chu, Zhang and Carlin 4 – Reference Shih and Tu 6 , Reference Hong, Chu, Zhang and Carlin 8 , Reference Dias and Ades 9
White et al.Reference Dias, Sutton, Ades and Welton 1 , Reference White, Turner, Karahalios and Salanti 5 discussed when the CBM and BMs yield different results. We aim to illuminate a key difference between these two models and to show that this difference is analogous to Lord’s Paradox, a conundrum about whether a t-test or analysis of covariance (ANCOVA) should be used to compare two groups according to a change in an outcome.Reference Lord 10 , Reference Lord 11
Our article is organized as follows. First, we give a brief overview of the CBM and BM and their assumptions. We then describe Lord’s Paradox and how the paradox occurs, after which we discuss how the assumptions of the two NMA models are related to Lord’s Paradox, using directed acyclic graphs (DAGs) to illustrate the relation. Finally, we discuss how Lord’s Paradox can illuminate the differences between the two NMA models.
2 NMA models and their statistical assumptions
Both NMA models were initially described within the Bayesian statistical framework.Reference Dias, Sutton, Ades and Welton 1 , Reference Hong, Chu, Zhang and Carlin 4 , Reference Dias, Welton, Sutton and Ades 12 For simplicity, we use the frequentist framework.
2.1 Contrast-based model
The CBM assumes a given treatment contrast is exchangeable across studies, as standard pairwise meta-analysis does. The CBM can be written as
 $$\begin{align*}{y}_{ik} = {s}_{b(i)}+{\delta}_{ib(i)k}+{\varepsilon}_{ik}\end{align*}$$
$$\begin{align*}{y}_{ik} = {s}_{b(i)}+{\delta}_{ib(i)k}+{\varepsilon}_{ik}\end{align*}$$
 $$\begin{align}{\varepsilon}_{ik}\sim N\left(0,{se}_{ik}^2\right)\end{align}$$
$$\begin{align}{\varepsilon}_{ik}\sim N\left(0,{se}_{ik}^2\right)\end{align}$$
 $$\begin{align*}{\delta}_{ib(i)k}\sim N\left({d}_{b(i)k},{\tau}^2\right),{d}_{b(i)k} = {d}_{Ak}-{d}_{Ab(i)},{d}_{AA} = 0,\end{align*}$$
$$\begin{align*}{\delta}_{ib(i)k}\sim N\left({d}_{b(i)k},{\tau}^2\right),{d}_{b(i)k} = {d}_{Ak}-{d}_{Ab(i)},{d}_{AA} = 0,\end{align*}$$
where
 ${y}_{ik}$
is treatment k’s response in study i with standard error
${y}_{ik}$
is treatment k’s response in study i with standard error
 ${se}_{ik}$
;
${se}_{ik}$
;
 ${\delta}_{ib(i)k}$
is treatment k’s trial-specific effect relative to trial i’s baseline treatment
${\delta}_{ib(i)k}$
is treatment k’s trial-specific effect relative to trial i’s baseline treatment
 $b(i)$
;
$b(i)$
;
 ${d}_{b(i)k}$
is the average of the contrast between k and
${d}_{b(i)k}$
is the average of the contrast between k and
 $b(i)$
;
$b(i)$
;
 ${\tau}^2$
, a variance, describes heterogeneity between trials in this contrast, and
${\tau}^2$
, a variance, describes heterogeneity between trials in this contrast, and
 ${d}_{Ak}$
is the difference between the average of treatment k and a reference treatment A. The heterogeneity
${d}_{Ak}$
is the difference between the average of treatment k and a reference treatment A. The heterogeneity
 ${\tau}^2$
is usually assumed identical for all treatment contrasts, so their covariances are
${\tau}^2$
is usually assumed identical for all treatment contrasts, so their covariances are
 $\frac{1}{2}{\tau}^2$
. For binary data,
$\frac{1}{2}{\tau}^2$
. For binary data,
 $y$
is usually the log odds or log risk, so
$y$
is usually the log odds or log risk, so
 $\delta$
and
$\delta$
and
 $d$
are the log odds ratio or log risk ratio between two treatments. For continuous data,
$d$
are the log odds ratio or log risk ratio between two treatments. For continuous data,
 $y$
is the outcome or change in outcome from the start of observation, so
$y$
is the outcome or change in outcome from the start of observation, so
 $\delta$
and
$\delta$
and
 $d$
are the mean difference in the outcome between two treatment groups. For either type of data,
$d$
are the mean difference in the outcome between two treatment groups. For either type of data,
 ${s}_{b(i)}$
is a fixed-effect parameter specific to study i, often interpreted as a study effect, while
${s}_{b(i)}$
is a fixed-effect parameter specific to study i, often interpreted as a study effect, while
 ${\delta}_{ib(i)k}$
is a random effect following a normal distribution, implying that it is exchangeable across studies.
${\delta}_{ib(i)k}$
is a random effect following a normal distribution, implying that it is exchangeable across studies.
2.2 Baseline model
The BM differs from the CBM in that the reference treatment’s level is modeled as a random effect with a separate draw from a normal distribution for each study. If we designate treatment A as the reference treatment, regardless of whether it was included in every study, we can write the BM (in arm-based form) asReference Dias, Welton, Sutton and Ades 12
 $$\begin{align*}{y}_{ik} = {s}_i+{\delta}_{iAk}+{\varepsilon}_{ik}\end{align*}$$
$$\begin{align*}{y}_{ik} = {s}_i+{\delta}_{iAk}+{\varepsilon}_{ik}\end{align*}$$
 $$\begin{align}{s}_i\sim N\left({\overline{s}}_A,{\sigma}_A^2\right),{\varepsilon}_{ik}\sim N\left(0,{se}_{ik}^2\right)\end{align}$$
$$\begin{align}{s}_i\sim N\left({\overline{s}}_A,{\sigma}_A^2\right),{\varepsilon}_{ik}\sim N\left(0,{se}_{ik}^2\right)\end{align}$$
 $$\begin{align*}{\delta}_{iAk}\sim N\left({d}_{Ak},{\tau}^2\right),{d}_{AA} = 0,\end{align*}$$
$$\begin{align*}{\delta}_{iAk}\sim N\left({d}_{Ak},{\tau}^2\right),{d}_{AA} = 0,\end{align*}$$
where
 ${s}_i$
is the (possibly hypothetical) true response for treatment A in study i, and
${s}_i$
is the (possibly hypothetical) true response for treatment A in study i, and
 ${\overline{s}}_A$
and
${\overline{s}}_A$
and
 ${\sigma}_A^2$
are the mean and variance across studies of this true response;
${\sigma}_A^2$
are the mean and variance across studies of this true response;
 ${\tau}^2$
is assumed identical for all treatment contrasts, so their covariances are
${\tau}^2$
is assumed identical for all treatment contrasts, so their covariances are
 $\frac{1}{2}{\tau}^2$
. The random effects
$\frac{1}{2}{\tau}^2$
. The random effects
 ${s}_i$
and
${s}_i$
and
 ${\delta}_{iAk}$
are assumed independent. (Model-2 is equivalent to Model 3 in the article by White et al. therein called the CBM with random study intercepts.)Reference White, Turner, Karahalios and Salanti
5
Different specifications of this model have been published. As specified in Model 2, the analysis results do not depend on the choice of reference treatment; as specified in White et al.Reference White, Turner, Karahalios and Salanti
5
, the results do depend on the choice of reference treatment. The Supplementary Material gives more details. Other parameters are as in the CBM. Thus, the baseline and CBMs differ in that
${\delta}_{iAk}$
are assumed independent. (Model-2 is equivalent to Model 3 in the article by White et al. therein called the CBM with random study intercepts.)Reference White, Turner, Karahalios and Salanti
5
Different specifications of this model have been published. As specified in Model 2, the analysis results do not depend on the choice of reference treatment; as specified in White et al.Reference White, Turner, Karahalios and Salanti
5
, the results do depend on the choice of reference treatment. The Supplementary Material gives more details. Other parameters are as in the CBM. Thus, the baseline and CBMs differ in that
 ${s}_i$
is a draw from a random effect in the former but a fixed effect in the latter.
${s}_i$
is a draw from a random effect in the former but a fixed effect in the latter.
2.3 Statistical assumptions of these NMA models
The study effect
 ${s}_{b(i)}$
in the CBM, a fixed effect, is the response of study i’s control group to the baseline treatment; the baseline treatment response is specific to each study and is not assumed exchangeable across studies. Rather, the difference in responses between two treatment groups—the treatment contrast or relative effect—is exchangeable.
${s}_{b(i)}$
in the CBM, a fixed effect, is the response of study i’s control group to the baseline treatment; the baseline treatment response is specific to each study and is not assumed exchangeable across studies. Rather, the difference in responses between two treatment groups—the treatment contrast or relative effect—is exchangeable.
This assumption that treatment contrasts are exchangeable further implies no association between study i’s baseline effect
 ${s}_{b(i)}$
and study i’s relative effect
${s}_{b(i)}$
and study i’s relative effect
 ${\delta}_{iAk}$
. Suppose all studies include the reference treatment A. The assumption is that if A has a large or small absolute effect in study i, this has no relation to the relative effect between A and the other treatments in study i. Even if the included studies come from different populations with different distributions of treatment effect modifiers, such as age, the relative treatment effects between A and other treatments in different studies remain similar by assumption, although the absolute effect of A may vary from study to study with differences in age.
${\delta}_{iAk}$
. Suppose all studies include the reference treatment A. The assumption is that if A has a large or small absolute effect in study i, this has no relation to the relative effect between A and the other treatments in study i. Even if the included studies come from different populations with different distributions of treatment effect modifiers, such as age, the relative treatment effects between A and other treatments in different studies remain similar by assumption, although the absolute effect of A may vary from study to study with differences in age.
The BM assumes baseline treatment A’s effect is exchangeable across studies, a random effect with a normal distribution. When a study’s patients are randomly assigned to A and other treatments, that study’s other treatments are thus randomly sampled from the same population, so the BM implicitly assumes all treatment effects are exchangeable across studies.Reference White, Turner, Karahalios and Salanti 5 We revisit this later when we discuss the selection of a baseline treatment.
3 Lord’s Paradox
We may gain insight into the differences between the CBM and BM from the literature about Lord’s Paradox.Reference Lord 10 , Reference Lord 11 This literature is vastReference Holland and Rubin 13 – Reference Wainer 16 ; we do not provide a comprehensive review.
In FM Lord’s original article, a university studied the effect on students’ body weight of the diet provided in the university dining halls. The study also asked whether males and females differed in the effects of the diet. Each student’s weight was measured upon their arrival in September and again the following June. Two statisticians analyzed the data independently.
3.1 A numerical example
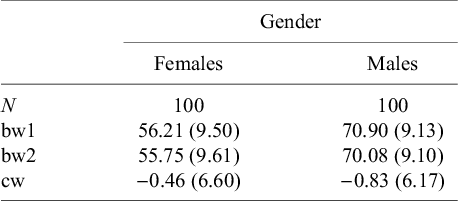
For our demonstration, we simulated body weights of 100 female and 100 male students. Table 1 summarizes the simulated data.
Summary statistics for the hypothetical body weight data with 100 male and 100 female students

Note: bw1, body weight measured at baseline; bw2, body weight measured at follow-up; cw, change in weight.
The first statistician calculates the mean weights of female students at the beginning and end of the year (56.20 kg and 55.75 kg, respectively) and finds the change (−0.46 kg) very small. The mean weights of male students at the beginning (70.90 kg) and end of the year (70.08 kg) are also similar, and the change (−0.83 kg) is also small. She compares weight change between females and males using a t-test, obtains a p-value of 0.68, and concludes that females and males did not differ in weight change. This t-test can be written as a linear regression model:
 $$\begin{align} B{W}_2-B{W}_1 = {a}_0+{a}_1 Gender+{e}^{(a)},\end{align}$$
$$\begin{align} B{W}_2-B{W}_1 = {a}_0+{a}_1 Gender+{e}^{(a)},\end{align}$$
where
 $B{W}_1$
and
$B{W}_1$
and
 $B{W}_2$
are body weights measured at baseline and follow-up, respectively, and Gender is a dummy variable with females coded 0 and males 1. The estimate of
$B{W}_2$
are body weights measured at baseline and follow-up, respectively, and Gender is a dummy variable with females coded 0 and males 1. The estimate of
 ${a}_0$
is −0.46 kg, the mean weight change in females, and
${a}_0$
is −0.46 kg, the mean weight change in females, and
 ${a}_1$
is −0.37 kg, suggesting no difference between sexes in mean weight change.
${a}_1$
is −0.37 kg, suggesting no difference between sexes in mean weight change.
The second statistician notices that males are larger than females at baseline on average (70.9 kg vs 56.2 kg), so she uses ANCOVA to adjust for the baseline difference in body weight. The ANCOVA model can also be written as a linear regression:
 $$\begin{align}B{W}_2 = {b}_0+{b}_1 Gender+{b}_2B{W}_1+{e}^{(b)}.\end{align}$$
$$\begin{align}B{W}_2 = {b}_0+{b}_1 Gender+{b}_2B{W}_1+{e}^{(b)}.\end{align}$$
The estimate of
 ${b}_0$
is 12.49 kg, the estimated mean body weight at the end of the year for females whose baseline body weight is zero, so
${b}_0$
is 12.49 kg, the estimated mean body weight at the end of the year for females whose baseline body weight is zero, so
 ${b}_0$
has no practical meaning. The estimate of
${b}_0$
has no practical meaning. The estimate of
 ${b}_1$
is 3.02 kg, the estimated difference in follow-up body weight between females and males with the same baseline body weight. The estimate of
${b}_1$
is 3.02 kg, the estimated difference in follow-up body weight between females and males with the same baseline body weight. The estimate of
 ${b}_2$
is 0.77, the estimated difference in follow-up body weight between students of a given gender whose baseline body weights differ by 1 kg. Because
${b}_2$
is 0.77, the estimated difference in follow-up body weight between students of a given gender whose baseline body weights differ by 1 kg. Because
 ${b}_1$
is statistically significant, the second statistician concludes that, on average, males gain 3 kg more than females. The horizontal and vertical axes of Figure 1’s scatterplot are the baseline and follow-up body weights, respectively. Red and blue circles represent females and males. Red and blue lines are fitted parallel regression lines for females and males, respectively, both with slope
${b}_1$
is statistically significant, the second statistician concludes that, on average, males gain 3 kg more than females. The horizontal and vertical axes of Figure 1’s scatterplot are the baseline and follow-up body weights, respectively. Red and blue circles represent females and males. Red and blue lines are fitted parallel regression lines for females and males, respectively, both with slope
 ${b}_2 = 0.77$
. Their intercepts differ by
${b}_2 = 0.77$
. Their intercepts differ by
 ${\widehat{b}}_1 = 3.02$
.
${\widehat{b}}_1 = 3.02$
.
Scatterplot of the hypothetical data with 100 male (blue circles) and 100 female (red circles) students. The blue and red solid lines are the fitted regression lines for male and female students, respectively. The black solid line has an intercept of zero and a slope of 1.

3.2 How does Lord’s Paradox happen?
When the difference between males and females in mean body weight change is small, the regression coefficient
 ${a}_1$
in Equation (Reference Dias, Sutton, Ades and Welton1) will be close to 0. However,
${a}_1$
in Equation (Reference Dias, Sutton, Ades and Welton1) will be close to 0. However,
 ${b}_1$
in Equation (Reference Lu and Ades2) equals 0 only under very special conditions.
${b}_1$
in Equation (Reference Lu and Ades2) equals 0 only under very special conditions.
Equation (Reference Dias, Sutton, Ades and Welton1) can be rearranged as
 $$\begin{align}B{W}_2 = {a}_0+{a}_1 Gender+1\times B{W}_1+{e}^{(a)}.\end{align}$$
$$\begin{align}B{W}_2 = {a}_0+{a}_1 Gender+1\times B{W}_1+{e}^{(a)}.\end{align}$$
The t-test is thus a linear regression in which
 $B{W}_2$
is regressed on
$B{W}_2$
is regressed on
 $Gender$
and
$Gender$
and
 $B{W}_1$
with
$B{W}_1$
with
 $B{W}_1'$
s coefficient constrained to
$B{W}_1'$
s coefficient constrained to
 ${b}_2 = 1$
, represented by Figure 1’s black line. When
${b}_2 = 1$
, represented by Figure 1’s black line. When
 ${a}_1$
is close to 0 as in our example, the fitted black lines for males and females are indistinguishable. Comparing Equations (Reference Salanti3) and (Reference Lu and Ades2), we see that Lord’s Paradox arises when
${a}_1$
is close to 0 as in our example, the fitted black lines for males and females are indistinguishable. Comparing Equations (Reference Salanti3) and (Reference Lu and Ades2), we see that Lord’s Paradox arises when
 ${b}_2$
is substantially less than 1 in Equation (Reference Lu and Ades2), in which case the two statisticians will give different conclusions.
${b}_2$
is substantially less than 1 in Equation (Reference Lu and Ades2), in which case the two statisticians will give different conclusions.
We can rearrange Equation (Reference Lu and Ades2) as
 $$\begin{align}B{W}_2-{b}_2{BW}_1 = {b}_0+{b}_1 Gender+{e}^{(b)}.\end{align}$$
$$\begin{align}B{W}_2-{b}_2{BW}_1 = {b}_0+{b}_1 Gender+{e}^{(b)}.\end{align}$$
Comparing Equations (Reference Dias, Sutton, Ades and Welton1) and (Reference Hong, Chu, Zhang and Carlin4), Lord’s Paradox can be interpreted as follows: The first statistician regresses the observed weight change
 $B{W}_2-B{W}_1$
on
$B{W}_2-B{W}_1$
on
 $Gender$
, while the second regresses the adjusted weight change
$Gender$
, while the second regresses the adjusted weight change
 $B{W}_2-{b}_2B{W}_1$
on
$B{W}_2-{b}_2B{W}_1$
on
 $Gender$
. If
$Gender$
. If
 $B{W}_2\approx B{W}_1$
, as in our example, then
$B{W}_2\approx B{W}_1$
, as in our example, then
 ${BW}_2-{b}_2B{W}_1\approx \left(1-{b}_2\right)B{W}_1$
. Because both males and females have tiny observed weight changes,
${BW}_2-{b}_2B{W}_1\approx \left(1-{b}_2\right)B{W}_1$
. Because both males and females have tiny observed weight changes,
 $B{W}_2\approx B{W}_1$
for both genders, so the two genders show a negligible difference in weight change. Thus, the first statistician finds no difference in weight change between females and males. In contrast, males have greater
$B{W}_2\approx B{W}_1$
for both genders, so the two genders show a negligible difference in weight change. Thus, the first statistician finds no difference in weight change between females and males. In contrast, males have greater
 $B{W}_1$
than females, so males have greater adjusted weight change. In our example, the average adjusted weight changes for males and females are
$B{W}_1$
than females, so males have greater adjusted weight change. In our example, the average adjusted weight changes for males and females are
 $70.1-0.77\times 70.9 = 15.5$
and
$70.1-0.77\times 70.9 = 15.5$
and
 $55.8-0.77\times 56.2 = 12.5$
, respectively, so the difference is about 3 kg, as the ANCOVA estimates.
$55.8-0.77\times 56.2 = 12.5$
, respectively, so the difference is about 3 kg, as the ANCOVA estimates.
3.3 An alternative formulation of Lord’s Paradox
Alternatively, we can consider the difference between the first and second statisticians as arising from their differing assumptions about the relationship between change score and baseline body weight. The first statistician assumes no relationship between weight change and baseline body weight, because Equation (Reference Dias, Sutton, Ades and Welton1) can be expressed as
 $$\begin{align}B{W}_2-B{W}_1 = {a}_0+{a}_1 Gender+0\times B{W}_1+{e}^{(a)}.\end{align}$$
$$\begin{align}B{W}_2-B{W}_1 = {a}_0+{a}_1 Gender+0\times B{W}_1+{e}^{(a)}.\end{align}$$
The coefficient for
 $B{W}_1$
is 0, so Equation (Reference Dias, Sutton, Ades and Welton1) assumes weight change is not related to baseline body weight. Thus, although males have greater body weight than females, on average, that plays no role in comparing their weight changes.
$B{W}_1$
is 0, so Equation (Reference Dias, Sutton, Ades and Welton1) assumes weight change is not related to baseline body weight. Thus, although males have greater body weight than females, on average, that plays no role in comparing their weight changes.
The second statistician assumes there is a relationship between weight change and baseline weight, as seen when Equation (Reference Lu and Ades2) is reexpressed as
 $$\begin{align}B{W}_2-B{W}_1 = {b}_0+{b}_1 Gender+\left({b}_2-1\right)B{W}_1+{e}^{(b)}.\end{align}$$
$$\begin{align}B{W}_2-B{W}_1 = {b}_0+{b}_1 Gender+\left({b}_2-1\right)B{W}_1+{e}^{(b)}.\end{align}$$
The two statisticians reach the same conclusion if
 ${b}_2\approx 1$
. Because of random errors in weight measurements and natural variation in body weight within each student,
${b}_2\approx 1$
. Because of random errors in weight measurements and natural variation in body weight within each student,
 ${b}_2$
is likely to be rather less than 1.Reference Shiffrin
14
,
Reference Reichardt
17
This is what FM Lord tried to demonstrate in his short article.Reference Lord
10
${b}_2$
is likely to be rather less than 1.Reference Shiffrin
14
,
Reference Reichardt
17
This is what FM Lord tried to demonstrate in his short article.Reference Lord
10
4 The relation between NMA models and Lord’s Paradox
We use an NMA with treatments X, Y, and Z to show how Lord’s Paradox illuminates the differences between the two NMA models. Following White et al.Reference Dias, Sutton, Ades and Welton 1 , Reference White, Turner, Karahalios and Salanti 5 , our NMA includes only trials comparing two treatments, one of which is treatment X. Thus, this NMA includes only two types of trials, also called designs in the NMA literatureReference White, Barrett, Jackson and Higgins 18 : one comparing X with Y (design XY) and the other comparing X with Z (design XZ). X is each trial’s baseline treatment and also the network’s reference treatment, so it is treatment “A” in Model-1 (the CB model) and Model-2 (the BM) above. We wish to know whether Z’s effect differs from Y’s.
The CBM for this NMA can be expressed (in contrast-based form) as a regression model:
 $$\begin{align*}{y}_{i2}-{y}_{iX} = {\delta}_{iX2}+{e}_{i,2X},{e}_{i,2X} = {\varepsilon}_{i2}-{\varepsilon}_{iX}\sim N\left(0,{se}_{iX}^2+{se}_{i2}^2\right),\kern2.00em\end{align*}$$
$$\begin{align*}{y}_{i2}-{y}_{iX} = {\delta}_{iX2}+{e}_{i,2X},{e}_{i,2X} = {\varepsilon}_{i2}-{\varepsilon}_{iX}\sim N\left(0,{se}_{iX}^2+{se}_{i2}^2\right),\kern2.00em\end{align*}$$
where group 2 is either Y or Z; group 1 is always X so the subscript “1” has been replaced by X. Model 1’s trial-specific effect of treatment k relative to trial i’s baseline treatment
 $b(i)$
,
$b(i)$
,
 ${\delta}_{ib(i)k}$
, can be expressed as
${\delta}_{ib(i)k}$
, can be expressed as
 $$\begin{align*}{\delta}_{iX2} = {d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}+{b}_{i2}-{b}_{iX}\end{align*}$$
$$\begin{align*}{\delta}_{iX2} = {d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}+{b}_{i2}-{b}_{iX}\end{align*}$$
where
 ${d}_{XY}$
and
${d}_{XY}$
and
 ${d}_{XZ}$
are as in Model 1;
${d}_{XZ}$
are as in Model 1;
 ${1}_{XY(i)} = $
1 when study i has design XY and 0 when study i has design XZ;
${1}_{XY(i)} = $
1 when study i has design XY and 0 when study i has design XZ;
 ${1}_{XZ(i)} = 1$
when study i has design XZ and 0 when study i has design XY; and
${1}_{XZ(i)} = 1$
when study i has design XZ and 0 when study i has design XY; and
 ${b}_{ij}\sim N\left(0,{\tau}^2\right)$
captures heterogeneity. The CBM is then
${b}_{ij}\sim N\left(0,{\tau}^2\right)$
captures heterogeneity. The CBM is then
 $$\begin{align}{y}_{i2}-{y}_{iX} = {d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}+{b}_{i2}-{b}_{iX}+{e}_{i,2X},\end{align}$$
$$\begin{align}{y}_{i2}-{y}_{iX} = {d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}+{b}_{i2}-{b}_{iX}+{e}_{i,2X},\end{align}$$
where the subscript 2 for
 ${y}_{i2}$
represents each study’s second treatment group, Y or Z. We can add
${y}_{i2}$
represents each study’s second treatment group, Y or Z. We can add
 $0\times {y}_{iX}$
to Equation (Reference Tu7), so it becomes clear that the CBM assumes no relationship between the treatment contrast and the baseline treatment:
$0\times {y}_{iX}$
to Equation (Reference Tu7), so it becomes clear that the CBM assumes no relationship between the treatment contrast and the baseline treatment:
 $$\begin{align}{y}_{i2}-{y}_{iX} = {d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}+0\times {y}_{iX}+{b}_{i2}-{b}_{iX}+{e}_{i,2X}.\end{align}$$
$$\begin{align}{y}_{i2}-{y}_{iX} = {d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}+0\times {y}_{iX}+{b}_{i2}-{b}_{iX}+{e}_{i,2X}.\end{align}$$
Equation (Reference Hong, Chu, Zhang and Carlin8) can be further rearranged by moving
 $-{y}_{iX}$
to the right side, yielding:
$-{y}_{iX}$
to the right side, yielding:
 $$\begin{align}{y}_{i2} = {d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}+1\times {y}_{iX}+{b}_{i2}-{b}_{iX}+{e}_{i,2X}.\end{align}$$
$$\begin{align}{y}_{i2} = {d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}+1\times {y}_{iX}+{b}_{i2}-{b}_{iX}+{e}_{i,2X}.\end{align}$$
The CBM can thus be viewed as regressing the test treatment level on the reference treatment level, with the regression coefficient fixed at 1. In all these ways, the CBM’s analysis is like the first statistician’s analysis in Lord’s Paradox.
Now consider the BM for this NMA, Model 2. Suppose we have an estimate
 ${\widehat{s}}_i^s$
for
${\widehat{s}}_i^s$
for
 ${s}_i$
. Such an estimate using Model 2, a mixed linear model, will be shrunk (hence the superscript) toward
${s}_i$
. Such an estimate using Model 2, a mixed linear model, will be shrunk (hence the superscript) toward
 ${\widehat{\overline{s}}}_X$
, an estimate of
${\widehat{\overline{s}}}_X$
, an estimate of
 ${\overline{s}}_X$
, the mean of
${\overline{s}}_X$
, the mean of
 ${s}_i'$
s distribution, so
${s}_i'$
s distribution, so
 ${\widehat{s}}_i^s$
can be written
${\widehat{s}}_i^s$
can be written
 $$\begin{align*}{\widehat{s}}_i^s = {\widehat{\overline{s}}}_X+{q}_i\left({\widehat{s}}_i^u-{\widehat{\overline{s}}}_X\right),\end{align*}$$
$$\begin{align*}{\widehat{s}}_i^s = {\widehat{\overline{s}}}_X+{q}_i\left({\widehat{s}}_i^u-{\widehat{\overline{s}}}_X\right),\end{align*}$$
where
 ${q}_i$
is the shrinkage factor and
${q}_i$
is the shrinkage factor and
 ${\widehat{s}}_i^u$
is the unshrunk estimate of
${\widehat{s}}_i^u$
is the unshrunk estimate of
 ${s}_i$
from a CBM fit, where the baseline treatment is a fixed effect. Each study and arm has its own sampling-error variance (usually treated as known), so
${s}_i$
from a CBM fit, where the baseline treatment is a fixed effect. Each study and arm has its own sampling-error variance (usually treated as known), so
 ${q}_i$
is a complex function of the heterogeneity
${q}_i$
is a complex function of the heterogeneity
 ${\tau}^2$
and reference-group random-effect variance
${\tau}^2$
and reference-group random-effect variance
 ${\sigma}^2,$
but it is easy to show that as
${\sigma}^2,$
but it is easy to show that as
 ${\sigma}^2\uparrow \infty$
i.e., as the BM tends toward the CBM,
${\sigma}^2\uparrow \infty$
i.e., as the BM tends toward the CBM,
 ${q}_i\uparrow 1$
.
${q}_i\uparrow 1$
.
Now
 ${\widehat{s}}_i^u = {s}_i+{\gamma}_i$
and
${\widehat{s}}_i^u = {s}_i+{\gamma}_i$
and
 ${\widehat{\overline{s}}}_X = {\overline{s}}_X+\xi$
, where
${\widehat{\overline{s}}}_X = {\overline{s}}_X+\xi$
, where
 ${\gamma}_i$
and
${\gamma}_i$
and
 $\xi$
have mean zero because the respective estimates are unbiased. Therefore,
$\xi$
have mean zero because the respective estimates are unbiased. Therefore,
 $$\begin{align*}{\widehat{s}}_i^s = \left(1-{q}_i\right){\overline{s}}_X+{q}_i{s}_i+{\omega}_i,\end{align*}$$
$$\begin{align*}{\widehat{s}}_i^s = \left(1-{q}_i\right){\overline{s}}_X+{q}_i{s}_i+{\omega}_i,\end{align*}$$
where
 ${\omega}_i = {q}_i{\gamma}_i+\left(1-{q}_i\right)\xi$
has mean 0. If we replace the hypothetical true response for treatment
${\omega}_i = {q}_i{\gamma}_i+\left(1-{q}_i\right)\xi$
has mean 0. If we replace the hypothetical true response for treatment
 $X$
for study i,
$X$
for study i,
 ${s}_i$
, in Model 2 with its estimate,
${s}_i$
, in Model 2 with its estimate,
 ${\widehat{s}}_i^s$
, then
${\widehat{s}}_i^s$
, then
 $$\begin{align*}{y}_{i2} = \left(1-{q}_i\right){\overline{s}}_X+{q}_i{s}_i+{d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}+{b}_{i2}+{\varepsilon}_{i2}+{\omega}_i.\end{align*}$$
$$\begin{align*}{y}_{i2} = \left(1-{q}_i\right){\overline{s}}_X+{q}_i{s}_i+{d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}+{b}_{i2}+{\varepsilon}_{i2}+{\omega}_i.\end{align*}$$
where the sum of the last three terms has a mean of zero.
Now
 ${y}_{i1} = {s}_i+{b}_{i1}+{\varepsilon}_{i1}$
, so
${y}_{i1} = {s}_i+{b}_{i1}+{\varepsilon}_{i1}$
, so
 $$\begin{align}{y}_{i2}-{y}_{i1} &= \left(1-{q}_i\right)\left({\overline{s}}_X-{s}_i\right)+{d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}\nonumber\\& \quad +\left({b}_{i2}-{b}_{i1}\right)+\left({\varepsilon}_{i2}-{\varepsilon}_{i1}\right)+{\omega}_i,\end{align}$$
$$\begin{align}{y}_{i2}-{y}_{i1} &= \left(1-{q}_i\right)\left({\overline{s}}_X-{s}_i\right)+{d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}\nonumber\\& \quad +\left({b}_{i2}-{b}_{i1}\right)+\left({\varepsilon}_{i2}-{\varepsilon}_{i1}\right)+{\omega}_i,\end{align}$$
where the second line of Equation (Reference Lord10) has a mean of zero.
Equation (Reference Lord10) can be rewritten in ways that are analogous to Equations (Reference Hong, Chu, Zhang and Carlin4) and (Reference Shih and Tu6). First, recall that
 ${y}_{i1} = {s}_i+{b}_{i1}+{\varepsilon}_{i1}$
. Gather these items from Equation (Reference Lord10)’s right side to give
${y}_{i1} = {s}_i+{b}_{i1}+{\varepsilon}_{i1}$
. Gather these items from Equation (Reference Lord10)’s right side to give
 $$\begin{align}{y}_{i2}-{y}_{i1}& = \left(1-{q}_i\right){\overline{s}}_X+\left({q}_i-1\right){y}_{i1}+{d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}\nonumber\\& \quad +\left({b}_{i2}-{q}_i{b}_{i1}\right)+\left({\varepsilon}_{i2}-{q}_i{\varepsilon}_{i1}\right)+{\omega}_i,\end{align}$$
$$\begin{align}{y}_{i2}-{y}_{i1}& = \left(1-{q}_i\right){\overline{s}}_X+\left({q}_i-1\right){y}_{i1}+{d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}\nonumber\\& \quad +\left({b}_{i2}-{q}_i{b}_{i1}\right)+\left({\varepsilon}_{i2}-{q}_i{\varepsilon}_{i1}\right)+{\omega}_i,\end{align}$$
where Equation (Reference Lord11)’s second line has mean zero. Equation (Reference Lord11) and Equation (Reference Shih and Tu6) have the same form: The BM implicitly assumes the study-specific treatment contrast and baseline effect are associated, while the CBM assumes they are independent.
Finally, we can move
 $\left({q}_i-1\right){y}_{i1}$
to the left-hand side of Equation (Reference Lord11), giving
$\left({q}_i-1\right){y}_{i1}$
to the left-hand side of Equation (Reference Lord11), giving
 $$\begin{align}{y}_{i2}-{q}_i{y}_{i1} &= \left(1-{q}_i\right){\overline{s}}_X+{d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}\nonumber\\& \quad +\left({b}_{i2}-{q}_i{b}_{i1}\right)+\left({\varepsilon}_{i2}-{q}_i{\varepsilon}_{i1}\right)+{\omega}_i,\end{align}$$
$$\begin{align}{y}_{i2}-{q}_i{y}_{i1} &= \left(1-{q}_i\right){\overline{s}}_X+{d}_{XY}{1}_{XY(i)}+{d}_{XZ}{1}_{XZ(i)}\nonumber\\& \quad +\left({b}_{i2}-{q}_i{b}_{i1}\right)+\left({\varepsilon}_{i2}-{q}_i{\varepsilon}_{i1}\right)+{\omega}_i,\end{align}$$
where the second line of Equation (Reference Dias, Welton, Sutton and Ades12) has mean zero. Equation (Reference Dias, Welton, Sutton and Ades12) and Equation (Reference Hong, Chu, Zhang and Carlin4) have the same form: The BM, in effect, has as its dependent variable an adjusted difference between the non-reference and reference treatments, where the adjustment depends on the shrinkage induced by the random effect used to model the reference treatment.
We make two comments about the BM. First, the shrinkage factor
 ${q}_i$
has the same role that
${q}_i$
has the same role that
 ${b}_2$
has in Lord’s Paradox in Equations (Reference Hong, Chu, Zhang and Carlin4) and (Reference Shih and Tu6), but
${b}_2$
has in Lord’s Paradox in Equations (Reference Hong, Chu, Zhang and Carlin4) and (Reference Shih and Tu6), but
 ${b}_2$
and
${b}_2$
and
 ${q}_i$
differ in other ways:
${q}_i$
differ in other ways:
 ${b}_2$
is the same for all students in Lord’s example, while
${b}_2$
is the same for all students in Lord’s example, while
 ${q}_i$
takes different values for different studies
${q}_i$
takes different values for different studies
 $i$
, and
$i$
, and
 ${b}_2$
is estimated by fitting the regression in Equation (Reference Hong, Chu, Zhang and Carlin4), while the
${b}_2$
is estimated by fitting the regression in Equation (Reference Hong, Chu, Zhang and Carlin4), while the
 ${q}_i$
depend on the data indirectly through the study sample sizes, the estimates
${q}_i$
depend on the data indirectly through the study sample sizes, the estimates
 ${\widehat{\sigma}}^2$
and
${\widehat{\sigma}}^2$
and
 ${\widehat{\tau}}^2$
, and the
${\widehat{\tau}}^2$
, and the
 ${se}_{ij}^2$
. The
${se}_{ij}^2$
. The
 ${q}_i$
will be close to zero only for very small studies. Second,
${q}_i$
will be close to zero only for very small studies. Second,
 $\left(1-{q}_i\right){\overline{s}}_X$
is present in Equations (Reference Lord11) and (Reference Dias, Welton, Sutton and Ades12) but has no analog in Equations (Reference Hong, Chu, Zhang and Carlin4) and (Reference Shih and Tu6). From Equation (Reference Lord11), biases in the BM’s estimates of treatment effects are a function of these terms.
$\left(1-{q}_i\right){\overline{s}}_X$
is present in Equations (Reference Lord11) and (Reference Dias, Welton, Sutton and Ades12) but has no analog in Equations (Reference Hong, Chu, Zhang and Carlin4) and (Reference Shih and Tu6). From Equation (Reference Lord11), biases in the BM’s estimates of treatment effects are a function of these terms.
4.1 NMA models and the two statisticians in Lord’s Paradox
Comparing Equations (Reference White, Turner, Karahalios and Salanti5) and (Reference Hong, Chu, Zhang and Carlin8) and Equations (Reference Shih and Tu6) and (Reference Dias, Welton, Sutton and Ades12), the CBM is the first statistician, while the BM is the second statistician. Each student has two measurements of body weight, as each trial has two treatments. Each student’s weight change corresponds to the treatment contrast in each trial. Males and females correspond to designs XZ and XY, respectively. The two statisticians’ approaches yield different results when males have larger baseline body weight; the two approaches to NMA may yield different results when the effects of baseline (and reference) treatment X differ between the two trial designs.
5 Graphical comparisons of NMA models
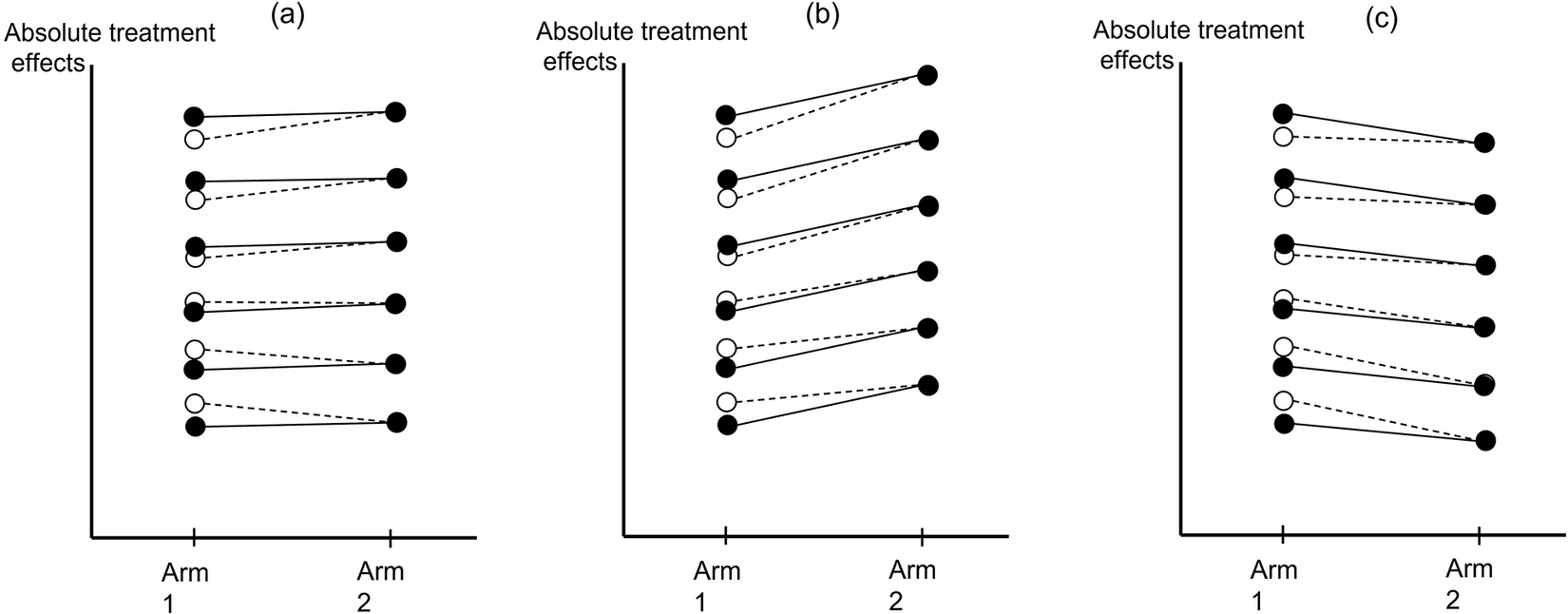
Figure 2 graphically explains the difference between the two models’ results in different scenarios. In terms of the preceding development for the BM, Figure 2 connects most directly to Equation (Reference Lord10). In Figure 2, two filled circles connected with a solid line represent a trial comparing two treatments, Arms 1 and 2. The horizontal axis is the treatment arms, and the vertical axis is the absolute treatment effects. In Figure 2a, the two arms in each of the six trials have the same outcome levels. In Figures 2b and 2c, the two arms have different outcome levels, but the difference between the two arms is identical in all trials. The open circles are the BM’s shrunken estimates for Arm 1, which are “shrunk” toward Arm 1’s average level.
Line plots for comparing contrast-based and baseline models. The two filled circles connected with a solid line represent a trial comparing two treatments, Arms 1 and 2. The open circles are the shrunken estimates of Arm 1 given by the baseline model; these open circles are “shrunk” closer to the average effect of Arm 1. The horizontal axis is the treatment arms, and the vertical axis is the absolute treatment effects. In (a), the two arms in each of the six trials have the same treatment effects. In (b), Arm 2 is better than Arm 1, and in (c), Arm 1 is better than Arm 2. The difference between the two arms is identical in every trial.

Suppose we include two types of trials in the analysis: design XY and design XZ. X is Arm 1, each study’s baseline treatment, and the network’s reference treatment, and we aim to know whether Z differs from Y. In the CBM, the difference between the two arms’ outcomes in each trial is the difference between the values of each trial’s two filled circles. In the BM, however, the difference in treatment levels is the difference between the open circle on the left and the solid circle on the right, connected by the dashed line. Because X’s level is modeled as a random effect, for trials with above-average levels of X, their estimated levels of X are shrunk downward, and for trials with below-average X, their estimated X are shrunk upward.
When designs XY and XZ have the same distribution of X, e.g., each design includes all six trials in Figure 2, Y and Z do not differ using the CBM or BM. But if the top three trials have design XZ and the bottom three trials have design XY, the two models give different results. In Figure 2a, the CBM finds no difference between Z and Y, but the BM finds Z is better than Y (because Z is better than X in design XZ, and X is better than Y in design XY). In Figure 2b, the CBM finds that both Z and Y are better than X, and Z and Y do not differ. The BM, however, finds that both Z and Y are better than X, but Z is also better than Y. In Figure 2c, the CBM finds that X is better than Z and Y, and again Z and Y do not differ. The BM now finds that X is slightly better than Z but much better than Y, so Z is better than Y.
6 Directed acyclic graphs for Lord’s Paradox and NMA models
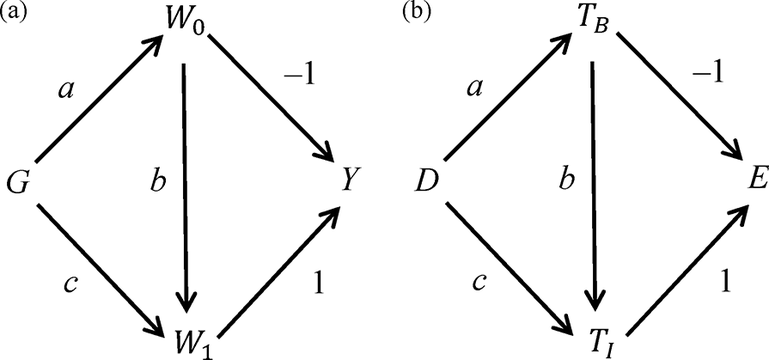
Figure 3a is a DAG for Lord’s Paradox, slightly modified from Pearl’s DAG.Reference Pearl
19
Each node represents a variable in the model; an arrow’s direction describes the relation between the two nodes. In Figure 3a, node G, gender, is a cause of baseline body weight (
 ${W}_0$
) and final weight (
${W}_0$
) and final weight (
 ${W}_1$
), while
${W}_1$
), while
 ${W}_0$
is a cause of
${W}_0$
is a cause of
 ${W}_1$
and weight gain (
${W}_1$
and weight gain (
 $Y$
), and
$Y$
), and
 ${W}_1$
is a cause of
${W}_1$
is a cause of
 $Y$
. The letter or number associated with an arrow denotes the strength of the path represented by the arrow and can be interpreted as a regression coefficient. For example, because on average, weight does not change for either males or females, the effect of
$Y$
. The letter or number associated with an arrow denotes the strength of the path represented by the arrow and can be interpreted as a regression coefficient. For example, because on average, weight does not change for either males or females, the effect of
 $G$
on
$G$
on
 ${W}_0$
is equal to its effect on
${W}_0$
is equal to its effect on
 ${W}_1$
, which can be written as
${W}_1$
, which can be written as
 $$\begin{align*}c+ ab = a,\mathrm{which}\kern0.17em \mathrm{implies}\;c = a\left(1-b\right).\end{align*}$$
$$\begin{align*}c+ ab = a,\mathrm{which}\kern0.17em \mathrm{implies}\;c = a\left(1-b\right).\end{align*}$$
Statistician 1 considers the total effect of
 $G$
on
$G$
on
 $Y$
, the sum of three paths from
$Y$
, the sum of three paths from
 $G$
to
$G$
to
 $Y$
,
$Y$
,
 $G\to {W}_0\to {W}_1\to Y$
,
$G\to {W}_0\to {W}_1\to Y$
,
 $G\to {W}_0\to Y$
, and
$G\to {W}_0\to Y$
, and
 $G\to {W}_1\to Y$
, so the total effect is
$G\to {W}_1\to Y$
, so the total effect is
 $ab-a+c = c-a\left(1-b\right) = 0$
. Statistician 2, however, considers the conditional effect of
$ab-a+c = c-a\left(1-b\right) = 0$
. Statistician 2, however, considers the conditional effect of
 $G$
on
$G$
on
 $Y$
by blocking paths through
$Y$
by blocking paths through
 ${W}_0$
; this conditional effect is
${W}_0$
; this conditional effect is
 $c = a\left(1-b\right)$
. The two statisticians have the same result if
$c = a\left(1-b\right)$
. The two statisticians have the same result if
 $a = 0$
or
$a = 0$
or
 $b = 1$
, i.e., (respectively) males and females do not differ in baseline body weight, or the regression of final weight on baseline weight has a coefficient of 1.
$b = 1$
, i.e., (respectively) males and females do not differ in baseline body weight, or the regression of final weight on baseline weight has a coefficient of 1.
Directed acyclic graphs for (a) Lord’s Paradox:
 $G$
represents gender;
$G$
represents gender;
 ${W}_0$
and
${W}_0$
and
 ${W}_1$
denote the baseline body weight and final weight, respectively;
${W}_1$
denote the baseline body weight and final weight, respectively;
 $Y$
is the weight gain and (b) NMA models:
$Y$
is the weight gain and (b) NMA models:
 $D$
represents study design (XY vs XZ);
$D$
represents study design (XY vs XZ);
 ${T}_B$
and
${T}_B$
and
 ${T}_I$
denote the effects of baseline treatment
${T}_I$
denote the effects of baseline treatment
 $X$
and the intervention treatment (Y or Z);
$X$
and the intervention treatment (Y or Z);
 $E$
is the difference in the effects between
$E$
is the difference in the effects between
 $Y$
and
$Y$
and
 $Z$
.
$Z$
.

Figure 3b shows an analogous DAG for NMA. Node
 $D$
represents design (XY vs XZ), which influences the effects of both the baseline treatment
$D$
represents design (XY vs XZ), which influences the effects of both the baseline treatment
 $X$
(
$X$
(
 ${T}_B$
) and the intervention treatment Y or Z (
${T}_B$
) and the intervention treatment Y or Z (
 ${T}_I$
).
${T}_I$
).
 ${T}_B$
is a cause of
${T}_B$
is a cause of
 ${T}_I$
and of the difference in the effects of
${T}_I$
and of the difference in the effects of
 $Y$
and
$Y$
and
 $Z$
(
$Z$
(
 $E$
), and
$E$
), and
 ${T}_I$
is a cause of
${T}_I$
is a cause of
 $E$
. Suppose the average relative treatment effect (difference between treatments) is the same in designs XY and XZ, so the effects of Y and Z relative to X do not differ, on average. Then the effect of
$E$
. Suppose the average relative treatment effect (difference between treatments) is the same in designs XY and XZ, so the effects of Y and Z relative to X do not differ, on average. Then the effect of
 $D$
on
$D$
on
 ${T}_B$
and
${T}_B$
and
 ${T}_I$
are the same, which implies
${T}_I$
are the same, which implies
 $$\begin{align*}c+ ab = a,\mathrm{thus}\;c = a\left(1-b\right)\end{align*}$$
$$\begin{align*}c+ ab = a,\mathrm{thus}\;c = a\left(1-b\right)\end{align*}$$
The CBM considers the total effect of
 $D$
on
$D$
on
 $E$
, the sum of three paths from
$E$
, the sum of three paths from
 $D$
to
$D$
to
 $E$
:
$E$
:
 $D\to {T}_B\to {T}_I\to E$
,
$D\to {T}_B\to {T}_I\to E$
,
 $D\to {T}_B\to E$
, and
$D\to {T}_B\to E$
, and
 $D\to {T}_I\to E$
, so the total effect is
$D\to {T}_I\to E$
, so the total effect is
 $ab-a+c = c-a\left(1-b\right) = 0$
. The BM estimates the conditional effect of
$ab-a+c = c-a\left(1-b\right) = 0$
. The BM estimates the conditional effect of
 $D$
on
$D$
on
 $E$
by blocking paths through
$E$
by blocking paths through
 ${T}_B$
; this conditional effect is
${T}_B$
; this conditional effect is
 $c = a\left(1-b\right)$
. The two models give the same result if
$c = a\left(1-b\right)$
. The two models give the same result if
 $a = 0$
or
$a = 0$
or
 $b = 1$
, i.e., (respectively) X has the same effect in designs XY and XZ, or the regression of the intervention treatment (Y or Z) on the baseline treatment (X) has a coefficient of 1.
$b = 1$
, i.e., (respectively) X has the same effect in designs XY and XZ, or the regression of the intervention treatment (Y or Z) on the baseline treatment (X) has a coefficient of 1.
Figure 3a shows that the t-test and ANCOVA give the same result if either the average baseline body weights are identical or the coefficient for regressing final body weight on baseline body weight is 1. In his 1967 article, FM Lord was more concerned about the latter, as this coefficient tended to be less than 1 because of natural fluctuations in body weights and measurement errors, causing imperfect correlation between two body weight measurements. In a NMA, even if the differences in the average treatment effects between X and Y and between X and Z are the same, the correlations (across studies) between treatment effects are unlikely to be 1, so the CBM and BM give different results.
7 Discussion
7.1 Comparing the two NMA models
When the baseline effects have similar distributions in the different trial designs, the contrast-based and BMs yield similar results. This is analogous to using the t-test or ANCOVA to analyze change scores from a randomized trial: both tests yield the same results because the treatment groups have similar baseline values.Reference Senn 20 The key question, therefore, is which model is more appropriate when trial designs have different baseline effects.
Variation between trials in the effect modifiers of individual patients can lead to differences in baseline effects. Including study-level effect modifiers in the analysis may reduce unexplained variation between trials, but caution is still necessary. Moreover, some effect modifiers may be unknown or unavailable. Also, trials with similarly distributed effect modifiers may still have different baseline effects. If the baseline and CBM show substantially different results, this suggests that baseline effects are heterogeneous across trial designs. Caution is therefore needed in interpreting results from either model, as this heterogeneity may reflect an imbalance in the distribution of some effect modifiers, resulting in violation of the transitivity assumption. We may need to reassess the eligibility of individual trials against the prespecified criteria in the systematic review’s protocol.
Figure 3’s DAGs offer another perspective on the differences between the two models. The BM estimates the adjusted difference between Y and Z in the treatment effects conditional on the effect of X, while the CBM estimates the total, unadjusted difference. Whether the adjusted or unadjusted difference is more clinically meaningful is likely to be context specific. For instance, suppose the effect modifiers are distributed similarly in trials of different designs, while the effects of X are on average slightly higher in design XZ than in design XY. The BM may give a more precise estimate for the difference between Y and Z by adjusting for the heterogeneity in X’s effect. In contrast, if patients’ characteristics differ substantially in designs XZ and XY, neither of these two models can provide a definitive answer about the difference between Y and Z.
7.2 Different formulations of NMA models and selection of the baseline treatment
In our discussion of the two NMA models, the treatment X was included in every trial, so it was the natural candidate for both the baseline and reference treatment. However, it is rare for a treatment to be included in all trials, so our single-level formulation of the BM in Equations (10)–(12), with treatment contrasts as the unit of analysis, is not applicable to most NMAs. Nevertheless, we used this formulation to show the similarity between these NMA models and Lord’s Paradox. A more practical formulation of these NMA models uses treatment arms as the unit of analysis, in which case any treatment can be the reference or baseline treatment (if Model 2’s specification is used; see the Supplementary Material).
In a previous study, Shi and TuReference Shih and Tu 6 used structural equation modeling to show that the CBM is a BM with the variance of the random study effects approaching infinity. This implies that results from the BM are not affected by the selection of reference treatment. There are, in fact, two versions of the BM that differ in their specification of random effects.Reference White, Turner, Karahalios and Salanti 5 , Reference Shih and Tu 6 The choice of a reference treatment affects the results in one specification but not the other. The Supplementary Material gives a more thorough technical discussion of the BM’s two specifications and of how the choice of the reference treatment affects their results differently.
Finally, although we used a specific NMA to demonstrate the analogy between Lord’s Paradox and the two NMA models, the conclusions and implications of this analogy extend beyond the specific NMA. For instance, we showed that the CBM uses observed treatment contrasts as outcomes, while the BM uses adjusted treatment contrasts. Thus, if the baseline treatment’s effect varies substantially across different designs of trials, these two models may yield different results. We refer readers to our previous article on bias propagation in NMA for simulations and a complex example in which results from these models can differ greatly.Reference Li, Shih, Song and Tu 21
8 Conclusion
This article used Lord’s Paradox to provide a framework for comparing the CBM and BMs for NMA. These two models make different assumptions about the relationships between baseline and relative treatment effects. When they yield substantially different results, we need to be cautious in interpreting either model’s results.
Author contributions
Y.-K.T. conceived the idea for this project. Y.-K.T. and J.S.H. contributed to the design of the study and interpretation of the results. Y.-K.T. wrote the first draft of the manuscript, and J.S.H. prepared the Supplementary Material. J.S.H. contributed to critical revisions of the draft. Both authors approved the final version of the article.
Competing interest statement
The authors declare that no competing interests exist.
Data availability statement
The R code for generating the example data used in this study is available in the Supplementary Material.
Funding statement
This study was partly supported by a grant from the National Science and Technology Council in Taiwan (Grant No. NSTC 112-2314-B-002-210-MY3).
Supplementary material
To view supplementary material for this article, please visit http://doi.org/10.1017/rsm.2025.10036.















 Open access
Open access