


Depressive and anxiety disorders are among the most common, Reference Kessler, Chiu, Demler and Walters1 persistent Reference Kessler, Merikangas and Wang2 and disabling Reference Kessler, Chiu, Demler and Walters1,Reference Kroenke, Spitzer, Williams, Monahan and Löwe3,Reference Judd, Paulus, Wells and Rapaport4 psychiatric disorders. In addition to research on ways to expand and improve the effectiveness of mental healthcare for those with depressive or anxiety disorders, recent efforts have been aimed at preventive interventions. Reference Cuijpers, Van Straten, Smit, Mihalopoulos and Beekman5,Reference Muñoz, Cuijpers, Smit, Barrera and Leykin6 In order to increase the effectiveness of preventive psychosocial or pharmacological strategies it is necessary to know which individuals are at highest risk. Individuals with a history of episodes of depressive disorder are at a greater risk of suffering subsequent episodes, Reference Angst, Gamma, Sellaro, Lavori and Zhang7,Reference Vuorilehto, Melartin and Isometsä8 as are those with depressive symptoms that do not meet the criteria for major depressive disorder, i.e. subthreshold depression. Reference Cuijpers and Smit9,Reference Merikangas, Zhang, Avenevoli, Acharyya, Neuenschwander and Angst10 The same holds true for anxiety disorders, for which past episodes Reference Kessler, Merikangas and Wang2,Reference Merikangas, Zhang, Avenevoli, Acharyya, Neuenschwander and Angst10 and subthreshold anxiety Reference Batelaan, De Graaf, Spijker, Smit, Van Balkom and Vollebergh11,Reference Acarturk, Smit, De Graaf, Van Straten, Ten Have and Cuijpers12 also predict occurrence. However, history of disorder and subthreshold symptoms are seldom evaluated in a single study, although this is important in order to unravel their unique contribution to the prediction of depression or anxiety. Moreover, their simultaneous evaluation can reveal whether people with both a history of disorder and subthreshold symptoms are at increased risk compared with those with either alone. Information on the relative weight of history and subthreshold symptoms in predicting depression or anxiety may form a resource for targeting efficiently those who might benefit most from preventive measures. The present study aims to determine the predictive value of both factors, separately and in combination. It uses data from a large cohort study on depression and anxiety disorders in The Netherlands. We first report the 2-year occurrence rates for common depressive (major depressive disorder and dysthymia) and anxiety disorders (social phobia, panic disorder, agoraphobia and generalised anxiety disorder). Subsequently, we examine the extent to which a history of a disorder, subthreshold symptoms and a combination of the two determine the risk for the occurrence of depressive and anxiety disorders over a 2-year period.
Method
Procedure
Data were derived from an 8-year longitudinal cohort study, the Netherlands Study of Depression and Anxiety (NESDA). Reference Penninx, Beekman, Smit, Zitman, Nolen and Spinhoven13 The study examines the aetiology and predictors of the long-term course of depressive and anxiety disorders. Its rationale and methods have been described elsewhere. Reference Penninx, Beekman, Smit, Zitman, Nolen and Spinhoven13 Assessments consisted of 4 h face-to-face interviews with additional data collection by means of written questionnaires. The present study reports on data from the baseline and 2-year follow-up assessments. The general exclusion criteria of NESDA were the presence of a clinical diagnosis of major psychiatric disorders other than depressive or anxiety disorder (e.g. psychosis, bipolar disorder, severe addictive disorder) or lack of fluency in the Dutch language. In the present study focusing on the occurrence of depressive or anxiety disorder, participants who had experienced depressive or anxiety disorder in the 6 months before baseline were excluded from analyses.
Participants
To represent various settings and stages of psychopathology, NESDA recruited respondents from three different settings: the general population (n = 564), primary care (n = 1610) and mental health organisations (n = 807), resulting in a total of 2981 respondents. Participants from the general population were selected from previous studies for their increased risk of depressive or anxiety disorder (participants with either a history of disorder or with a parent with a mood or anxiety disorder). Reference Penninx, Beekman, Smit, Zitman, Nolen and Spinhoven13 Participants from primary care consisted of individuals who had screened positive as well as a random subset of screen-negative individuals in a two-step screening approach involving the written extended Kessler Psychological Distress Scale (EK–10) Reference Donker, Comijs, Cuijpers, Terluin, Nolen and Zitman14 and a telephone screen using the Composite International Diagnostic Interview–Short Form (CIDI–SF). Reference Kessler, Andrews, Mroczek, Üstü and Wittchen15 The EK–10 included the 10-item Kessler Psychological Distress Scale (K10), Reference Kessler, Andrews, Colpe, Hiripi, Mroczek and Normand16 extended with five anxiety questions, previously shown to yield higher sensitivity for depressive and anxiety disorders. Reference Donker, Comijs, Cuijpers, Terluin, Nolen and Zitman14 A screen-positive score on the EK–10 was defined as a K–10 score of ≥ 20 or a positive score on any of the added anxiety questions. A screen-positive CIDI–SF was defined as a positive score on the depression sections (major depressive disorder or dysthymia) or the anxiety sections (social phobia, panic disorder, agoraphobia or generalised anxiety disorder). Mental healthcare patients were recruited when they were newly enrolled at participating mental health organisation locations.
Of the 2981 respondents in NESDA, 1701 (57.1%) had had a depressive and/or an anxiety disorder within the 6 months before baseline and were excluded in the present study. Of the remaining 1280 respondents, 1177 (92.0%) participated in the 2-year follow-up interview, of which 1167 (99.2%) completed the required questionnaires. Non-response was significantly associated with two of the covariates used in the present study, i.e. higher number of somatic illnesses (P<0.001) and fewer years of education (P = 0.001), but not with age and gender. In short, the sample analysed in this study comprised 1167 respondents from the general population (n = 380) and primary care (n = 787) and constitutes a mixture of individuals in remission, individuals at risk of developing a first episode and individuals in neither of these categories.
Measures
Demographic and somatic health factors
Age, gender, years of education and number of somatic conditions were included as basic sociodemographic and clinical determinants, as they are commonly related to depression and anxiety. Reference Ansseau, Fischler, Dierick, Albert, Leyman and Mignon17 Age, gender and years of education were assessed in the baseline interview. As a general indicator of somatic health, we assessed the presence (yes/no) of 16 somatic conditions commonly assessed in Dutch epidemiological studies (e.g. Netherlands Mental Health Survey and Incidence Study (NEMESIS) Reference Bijl and Ravelli18 and the Longitudinal Aging Study Amsterdam (LASA) Reference Beekman, Penninx, Deeg, Ormel, Braam and Van Tilburg19 ) during the baseline interview: lung disease, heart conditions, diabetes, stroke, arthritis, cancer, hypertension, ulcers, intestinal disorders, liver disease, epilepsy, chronic fatigue syndrome, allergies, thyroid disease, head injuries and other injuries.
Mental disorders
History (yes/no) and occurrence (yes/no) of depressive (major depressive disorder, dysthymia) and anxiety disorders (social phobia, panic disorder, agoraphobia, generalised anxiety disorder) were assessed using the depression and anxiety sections of the Composite International Diagnostic Interview (CIDI, lifetime version 2.1). 20 History of a disorder was defined as the occurrence of the disorder at any time during the individual's lifespan (but not within the 6 months before baseline; these individuals were excluded from the analyses). Occurrence of a disorder was defined as the onset of the disorder anytime between the baseline and the 2-year follow-up measurement. The overall median time between baseline and 2-year follow-up was 735 days, with an interquartile range of 724 to 756 days.
Subthreshold mental disorders
Subthreshold depression at baseline was assessed with the Inventory of Depressive Symptomatology–Self Report (IDS–SR30). Reference Rush, Giles, Schlesser, Fulton, Weissenburger and Burns21 The IDS–SR30 is a 30-item self-report questionnaire assessing the severity of depressive symptoms. The items are rated on a four-point Likert scale ranging from zero to three. The total score is obtained by summing 28 of the 30 items, with a total score ranging from 0 to 84, which can be categorised according to severity: 0–13, normal; 14–25, mild depression; 26–38 moderate depression; 39–48, severe depression and 49–84, very severe depression. Reference Rush, First and Burns22 High concurrent validity has been shown between the IDS–SR30 and the depression factor of the Symptom Check List–90 items, Revised (SCL–90–R) Reference Corruble, Legrand, Duret, Charles and Guelfi23 and the Hamilton Rating Scale for Depression (HRSD). Reference Rush, Trivedi, Carmody, Ibrahim, Markowitz and Keitner24 Furthermore, high internal consistency was found for the IDS–SR30 overall, Reference Corruble, Legrand, Duret, Charles and Guelfi23,Reference Trivedi, Rush, Ibrahim, Carmody, Biggs and Suppes25 which was confirmed in our study (Cronbach's α = 0.84) without participants with full-syndromal depressive disorder. Subthreshold depression was defined as a score of at least 14 on the IDS–SR30. This was based on our previous study about the clinical relevance of subthreshold depressive disorder. We found that participants without depressive disorder but with a score of at least 14 (i.e. at least mild depression) on the IDS–SR30 experienced substantially more functional impairment than participants scoring within the normal range (0–13). Receiver operating characteristic (ROC) analyses indicated that this cut-off identified 60% of the most dysfunctional participants without major depressive disorder or dysthymia, with a sensitivity of 0.79 and a specificity of 0.84. Reference Karsten, Hartman, Ormel, Nolen and Penninx26
Subthreshold anxiety at baseline and 2-year follow-up was assessed using the Beck Anxiety Inventory (BAI). Reference Beck, Epstein, Brown and Steer27 The BAI is a 21-item self-report questionnaire developed to assess anxiety, with a focus on somatic symptoms. The items are rated on a four-point Likert scale ranging from zero (not at all) to three (severely: I could barely stand it). The total score ranges from 0 to 63 and is commonly categorised as follows: 0–9, normal or no anxiety; 10–18, mild to moderate anxiety; 19–29, moderate to severe anxiety; and 30–63, severe anxiety. Reference Rush, First and Burns22 As an indication of concurrent validity, moderate to high correlation was found between the BAI and the SCL–90–R anxiety factor Reference Steer, Ranieri, Beck and Clark28 and a moderate correlation between the BAI and the Hamilton Rating Scale for Anxiety (HRSA). Reference Beck and Steer29 Furthermore, high internal consistency was found in several studies Reference Steer, Ranieri, Beck and Clark28,Reference Borden, Peterson and Jackson30 and confirmed in our study (Cronbach's α = 0.86) without participants with full-syndromal anxiety disorders. Subthreshold anxiety was defined as a score of at least 11 on the BAI. In a recent study, we found that participants without anxiety disorders but with a BAI score of at least 11 (i.e. at least mild anxiety) experienced more functional impairment than participants with a BAI score within the normal anxiety range (0–9). The ROC analyses indicated that a cut-off score of 11 on the BAI identified the 36% of most dysfunctional participants without social phobia, panic disorder, agoraphobia or generalised anxiety disorder. Reference Karsten, Nolen, Penninx and Hartman31
Statistical analyses
First, we calculated the occurrence rates of depressive disorders, i.e. major depressive disorder or dysthymia, since the baseline interview. We differentiated between respondents with and without subthreshold depression at baseline, and respondents with and without a history of depressive disorder. Similarly, we calculated the occurrence rates of anxiety disorders, i.e. social phobia, panic disorder, agoraphobia or generalised anxiety disorder, since the baseline interview, while differentiating between respondents with and without subthreshold anxiety at baseline on the one hand, and respondents with and without a history of anxiety on the other.
Second, we used univariate and multiple logistic regression analyses to assess the extent to which subthreshold symptoms, history and combinations of both predicted the occurrence of depressive disorder and anxiety disorder over 2 years. To this end, we combined these two variables into a single variable divided into four categories (using three dummy variables): (a) without a history of disorder, without subthreshold symptoms, (b) with a history of disorder, without subthreshold symptoms, (c) without a history of disorder, with subthreshold symptoms, (d) with a history of disorder, with subthreshold symptoms. Gender, age, years of education and number of somatic illnesses were also included in these analyses as basic sociodemographic and clinical predictors.
The value of the full model as a predictor of occurrence was estimated using the concordance statistic (c-statistic, i.e. the area under the ROC curve). Concordance statistics between 0.7 and 0.8 are generally considered as acceptable, those between 0.8 and 0.9 as excellent. Reference Hosmer and Lemeshow32
Results
Sample characteristics
Sample characteristics at baseline are provided inTable 1.
Table 1 Sociodemographic and clinical characteristics at baseline (n = 1167)

| Characteristics | |
|---|---|
| Gender: male, n (%) | 399 (34.2) |
| Subthreshold depression, n (%) | 369 (31.6) |
| Subthreshold anxiety, n (%) | 227 (19.5) |
| No history of depressive or anxiety disorder, n (%) | 598 (51.2) |
| No history of depressive disorder, n (%) | 701 (60.1) |
| No history of anxiety disorder, n (%) | 846 (72.5) |
| History of major depressive disorder, n (%)a | 458 (39.2) |
| History of dysthymia, n (%) | 110 (9.4) |
| History of social phobia, n (%) | 124 (10.6) |
| History of panic disorder, n (%) | 98 (8.4) |
| History of agoraphobia, n (%) | 84 (7.2) |
| History of generalised anxiety disorder, n (%) | 130 (11.1) |
| Age, mean (s.d.) | 42.6 (13.9) |
| Number of somatic conditions, mean (s.d.) | 1.6 (1.3) |
| Years of education, mean (s.d.) | 12.8 (3.2) |
| Inventory of Depressive Symptomatology–Self Report–30 score mean (s.d.) | 11.1 (8.5) |
| Beck Anxiety Inventory score, mean (s.d.) | 5.5 (5.7) |
Occurrence of depressive and anxiety disorders
The rates of depressive disorders (major depressive disorder or dysthymia) are shown inTable 2 andFig. 1. Of the 369 respondents with baseline subthreshold depression, 27.9% reported one or more depressive disorders since baseline, which is four times more than among the 798 respondents without subthreshold depressive disorder at baseline (7.1%). Of the 466 respondents with a history of depressive disorder, 23.0% had developed a depressive disorder by the time of the 2-year follow-up, an occurrence three times higher than among the 701 respondents without a history of depressive disorder (7.6%).
Table 2 Occurrence rates of depressive disorders between baseline and 2-year follow-upa

| n | Any depressive disorder, n (%) | Dysthymia, n (%) | Major depressive disorder, n (%) | |
|---|---|---|---|---|
| No subthreshold depressive disorder at baseline | 798 | 57 (7.1) | 6 (0.8) | 55 (6.9) |
| History of dysthymia | 43 | 10 (23.3) | 1 (2.3) | 10 (23.3) |
| History of major depressive disorder | 245 | 36 (14.7) | 5 (2.0) | 34 (13.9) |
| No history of dysthymia/major depressive disorder | 549 | 21 (3.8) | 1 (0.2) | 21 (3.8) |
| Subthreshold depression at baseline | 369 | 103 (27.9) | 12 (3.3) | 102 (27.6) |
| History of dysthymia | 67 | 28 (41.8) | 6 (9.0) | 28 (41.8) |
| History of major depressive disorder | 213 | 70 (32.9) | 8 (3.8) | 70 (32.9) |
| No history of dysthymia/major depressive disorder | 152 | 32 (21.1) | 4 (2.6) | 31 (20.4) |
| Total | 1167 | 160 (13.7) | 18 (1.5) | 157 (13.5) |
The rates of anxiety disorders are shown inTable 3 andFig. 2. Of the 227 respondents with baseline subthreshold anxiety, 25.6% reported one or more anxiety disorders since baseline, an occurrence over three times higher than among the 940 respondents without subthreshold anxiety (7.6%). Of the 321 respondents with a history of anxiety disorder, 21.2% developed an anxiety disorder by the time of the 2-year follow-up, almost three times more than among the 846 respondents without a history of anxiety disorder (7.2%).
Table 3 Occurrence rates of anxiety disorders between baseline and 2-year follow-upa

| n | Any anxiety disorder, n (%) | Social phobia, n (%) | Panic disorder, n (%) | Agoraphobia, n (%) | General anxiety disorder, n (%) | |
|---|---|---|---|---|---|---|
| No subthreshold anxiety disorder at baseline | 940 | 71 (7.6) | 26 (2.8) | 19 (2.0) | 17 (1.8) | 15 (1.6) |
| History of social phobia | 91 | 18 (19.8) | 12 (13.2) | 6 (6.6) | 3 (3.3) | 3 (3.3) |
| History of panic disorder | 65 | 6 (9.2) | 2 (3.1) | 2 (3.1) | 2 (3.1) | 1 (1.5) |
| History of agoraphobia | 54 | 12 (22.2) | 4 (7.4) | 3 (5.6) | 9 (16.7) | 2 (3.7) |
| History of GAD | 87 | 15 (17.2) | 5 (5.7) | 5 (5.7) | 4 (4.6) | 2 (2.3) |
| No history of anxiety | 719 | 34 (4.7) | 11 (1.5) | 9 (1.3) | 5 (0.7) | 8 (1.1) |
| Subthreshold anxiety at baseline | 227 | 58 (25.6) | 18 (7.9) | 24 (10.6) | 12 (5.3) | 14 (6.2) |
| History of social phobia | 33 | 9 (27.3) | 6 (18.2) | 3 (9.1) | 2 (6.1) | 1 (3.0) |
| History of panic disorder | 33 | 13 (39.4) | 3 (9.1) | 6 (18.2) | 6 (18.2) | 4 (12.1) |
| History of agoraphobia | 30 | 11 (36.7) | 5 (16.7) | 5 (16.7) | 4 (13.3) | 3 (10.0) |
| History of GAD | 43 | 12 (27.9) | 3 (7.0) | 6 (14.0) | 2 (4.7) | 2 (4.7) |
| No history of anxiety | 127 | 27 (21.3) | 7 (5,5) | 10 (7.9) | 4 (3.1) | 6 (4.7) |
| Total | 1167 | 129 (11.1) | 44 (3.8) | 43 (3.7) | 29 (2.5) | 29 (2.5) |
History and subthreshold disorder as predictors of the occurrence of depressive disorders
Odds ratios (ORs) and 95% confidence intervals for the occurrence of any depressive disorder in the 2 years following baseline are listed inTable 4. Univariate regression analyses show that the occurrence of any depressive disorder was predicted by the combination of a history of depression and subthreshold depression, a combination of a history of anxiety and subthreshold anxiety, a history of depressive or anxiety disorder alone and subthreshold depression or anxiety alone. Using multiple regression analysis, a history of anxiety and subthreshold anxiety on their own dropped below significance levels, and only the combination of a history of anxiety and subthreshold anxiety at baseline predicted the occurrence of depressive disorder. In contrast, subthreshold depression alone, a history of depressive disorder alone and the combination of the two remained predictors of the occurrence of depressive disorder. Note that the effect of history and subthreshold symptoms combined (OR = 10.00) can be characterised as additive relative to either effect on its own, as the expected value of an additive effect would correspond to the sum of 4.15 and 6.23 minus 1, which is roughly midway in the confidence interval of the estimated combined effect 5.49–18.20. Reference Darroch33,Reference Ormel, Oldehinkel and Brilman34 A higher number of somatic illnesses and fewer years of education also predicted the occurrence of depressive disorder in univariate analyses, but not in the multiple regression analysis. Older age predicted a lower occurrence of depression using multiple regression analysis. For predicting the occurrence of depressive disorder within 2 years, the c-statistic of the total model was 0.74, indicating a reasonable discriminative ability.
Table 4 Baseline predictors of depressive disorders and anxiety disorders: odds ratios (OR) and 95% confidence intervals (n = 1167)

| Depressive disorder, OR (95% CI) | Anxiety disorder, OR (95% CI) | |||
|---|---|---|---|---|
| Univariate | Multiple regression | Univariate | Multiple regression | |
| Gender | 1.13 (0.79–1.61) | 0.85 (0.58–1.25) | 1.74 (1.14–2.65)* | 1.36 (0.87–2.15) |
| Age | 0.99 (0.98–1.00) | 0.98 (0.97–0.99)* | 1.00 (0.99–1.01) | 0.99 (0.98–1.01) |
| Years of education | 0.94 (0.90–0.99)* | 0.98 (0.93–1.04) | 0.95 (0.89–1.00) | 0.99 (0.93–1.06) |
| Number of somatic illnesses | 1.17 (1.04–1.31)** | 1.06 (0.93–1.21) | 1.11 (0.98–1.27) | 1.01 (0.87–1.17) |
| Depressive disorder | ||||
| History of depressive disorder | 4.25 (2.42–7.45)*** | 4.15 (2.32–7.44)*** | 2.81 (1.54–5.12)** | 2.02 (1.07–3.79)* |
| Subthreshold depression | 6.71 (3.74–12.04)*** | 6.23 (3.31–11.74)*** | 5.68 (3.12–10.33)*** | 3.47 (1.78–6.78)*** |
| History of depressive disorder and subthreshold depression | 12.23 (7.27–20.57)*** | 10.00 (5.49–18.20)*** | 8.54 (5.01–14.54)*** | 4.07 (2.18–7.59)*** |
| Anxiety disorder | ||||
| History of anxiety | 2.47 (1.60–3.82)*** | 1.38 (.86–2.22) | 4.05 (2.47 – 6.64)*** | 2.82 (1.66–4.79)*** |
| Subthreshold anxiety | 2.88 (1.60–3.82)*** | 1.07 (0.60–1.92) | 5.44 (3.15–9.40)*** | 2.65 (1.41–4.99)** |
| History of anxiety and subthreshold anxiety | 6.02 (3.69–9.83)*** | 2.04 (1.15–3.61)* | 9.05 (5.24–15.63)*** | 4.17 (2.22–7.85)*** |
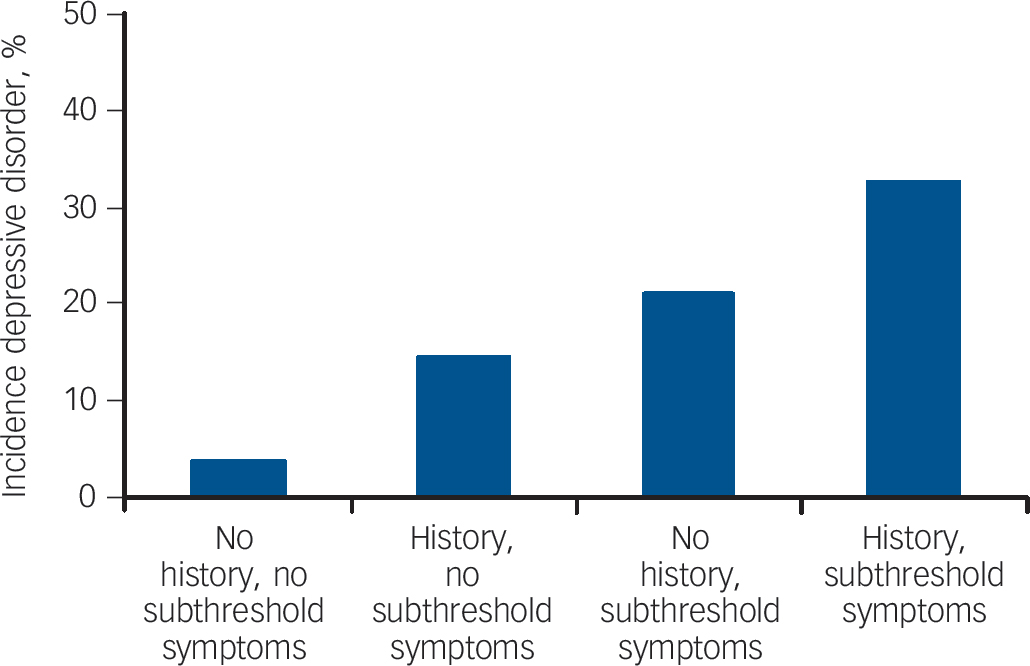
Fig. 1 Occurrence of depressive disorder by history of depressive disorder and subthreshold depression at baseline.
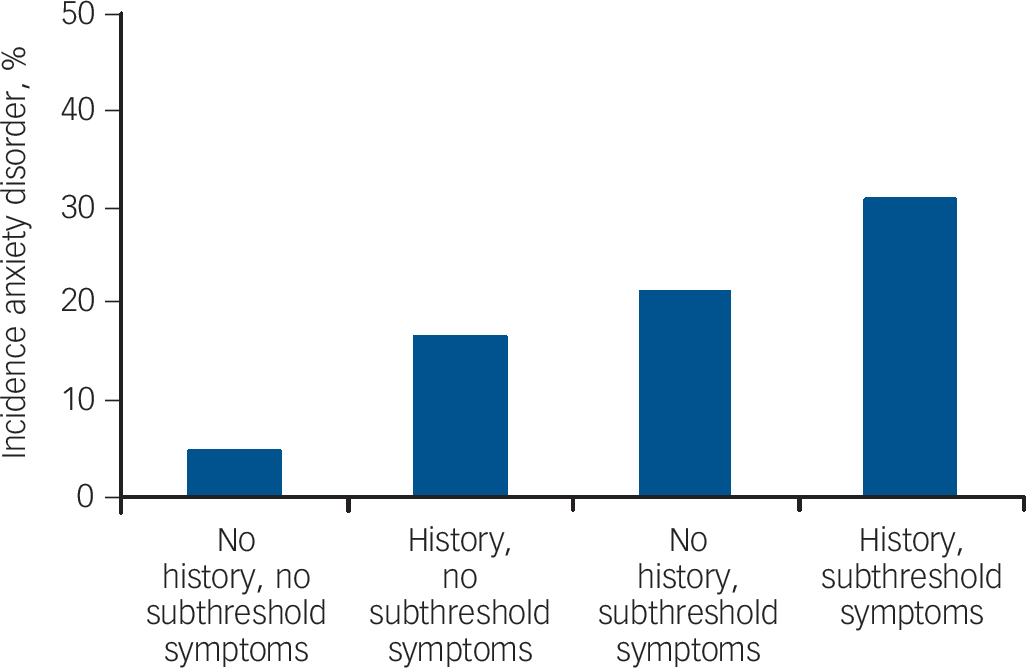
Fig. 2 Occurrence of depressive disorder by history of anxiety disorder and subthreshold anxiety at baseline.
Of the 160 individuals who developed a depressive disorder between baseline and 2-year follow-up, 63 also developed a comorbid anxiety disorder. The multiple regression analysis was repeated excluding these 63 individuals. The combination of a history of anxiety disorder and subthreshold anxiety no longer predicted the occurrence of depressive disorder, leaving a combination of a history of depression and subthreshold depression (OR = 11.35, 95% CI 5.41–23.81), subthreshold depression alone (OR = 7.97, 95% CI 3.68–17.24) and a history of depression (OR = 4.85, 95% CI 2.37–9.94) as predictors for the occurrence of depressive disorder.
History and subthreshold disorder as predictors of the occurrence of anxiety disorders
Both univariate and multiple regression analyses showed that the occurrence of anxiety disorders was best predicted by a combination of a history of anxiety disorder and subthreshold anxiety, closely followed by a combination of a history of depressive disorder and subthreshold depression (Table 4). Subthreshold anxiety alone, subthreshold depression alone, a history of anxiety disorder alone, and a history of depressive disorder alone all predicted the occurrence of anxiety disorder as well, although a history of depressive disorder dropped below significance in multiple regression analysis. Again, the effect of symptoms history and subthreshold combined can be characterised as additive relative to either effect on its own, as the expected values are within the confidence intervals for anxiety (2.22–7.85) as well as depressive disorder (2.18–7.59). Reference Darroch33,Reference Ormel, Oldehinkel and Brilman34 To a small extent, female gender also predicted the occurrence of anxiety disorder in the univariate analysis, but not in the multiple regression analysis. For predicting the occurrence of anxiety disorder within 2 years, the c-statistic of the total model was 0.72, indicating a reasonable discriminative ability. Of the 129 individuals who developed anxiety disorder between baseline and 2-year follow-up, 63 developed a comorbid depressive disorder. To determine the predictors specifically for anxiety disorder, the multiple regression analysis was repeated, excluding these 63 individuals. A history of depressive disorder no longer significantly predicted the occurrence of anxiety disorder. Otherwise results remained very similar to the prior analyses with the 63 participants included, i.e. combinations of history and subthreshold symptoms of either disorder, and subthreshold symptoms alone of either disorder predicted the occurrence of anxiety disorder, as did a history of anxiety alone.
Post hoc analyses
The finding that depression predicted the occurrence of anxiety disorders led us to explore post hoc the predictive value of depression for the individual anxiety disorders of social phobia, panic disorder, agoraphobia and generalised anxiety disorder. Multiple regression analyses indicated that depression predicted the occurrence of social phobia and generalised anxiety disorder, but not panic disorder or agoraphobia. More specifically, social phobia was predicted by subthreshold depression alone (OR = 3.28, 95% CI 1.29–8.3), and by a combination of depressive disorder and subthreshold depression (OR = 2.98, 95% CI 1.23–7.20), whereas generalised anxiety disorder was predicted by a combination of depressive disorder and subthreshold depression (OR = 14.07, 95% CI 3.67–53.91), followed by a history of depressive disorder alone (OR = 5.90, 95% CI 1.54–22.67) and subthreshold depression alone (OR = 6.05, 95% CI 1.37–26.64). It should be noted however, as can be seen inTable 3, that the occurrence rates in this study are rather low for any definite conclusions on the individual anxiety disorders.
Discussion
Main findings
In this study, we investigated whether a history of a depressive disorder or anxiety disorder and subthreshold symptoms were predictors for the occurrence of depressive or anxiety disorder over 2 years. Two conclusions follow from our findings. First, both a history and subthreshold symptoms of a given disorder independently predicted the occurrence of the disorder within 2 years, with a combination of the two carrying the highest, additive risk. Second, a history of depressive disorder and subthreshold depression signalled the occurrence of either depressive or anxiety disorder, whereas a history of anxiety disorder or subthreshold anxiety signalled the occurrence of anxiety only.
The finding that depression predicted the occurrence of anxiety disorder, separately from depressive disorder, may be explained by the diverse nature of anxiety disorders. Although some are characterised by explicit fear, others are based on anxious worry. Post hoc exploration indicated that depression predicted generalised anxiety disorder and social phobia (but not panic disorder or agoraphobia). Thus, depression predicted those anxiety disorders that, like depression, emphasise worrying.
Predictors directly related to disorder (history and subthreshold symptoms) were much stronger predictors for the occurrence of a disorder than sociodemographic factors such as gender or level of education. The fact that they did not predict the occurrence of depressive or anxiety disorders, not even in univariate analyses, may be explained by the way participants were recruited. Recruitment in NESDA was based mostly on the presence of (or risk of) depressive or anxiety disorder. Thus, the 2-year occurrence rates consisted more of recurrence than of first occurrence of depressive or anxiety disorder. Although gender and socioeconomic status are known predictors of first occurrence of disorder, they are not for recurrence. Reference Burcusa and Iacono35
We found that 13.7% of our sample developed a depressive disorder and 11.1% an anxiety disorder within 2 years, which is much higher than the 3-year occurrence rates in, for example, the Dutch general population study NEMESIS (4.7% and 3.7%, respectively). Reference De Graaf, Bijl, Ten Have, Beekman and Vollebergh36 Again this finding should be seen in light of recruitment in NESDA. About half the participants in the present sample had a history of psychopathology. When we narrowed our sample down to those without a history of depressive or anxiety disorder (n = 598), as in the aforementioned study from NEMESIS, 6.7% developed a depressive disorder within 2 years, and 5.7% developed an anxiety disorder within 2 years; which is more in line with NEMESIS findings.
Implications
The findings of this study have implications for mental healthcare and research. We have shown that only two indicators – history and subthreshold symptoms – have an independent and reasonable discriminative ability (overall c-statistic 0.72–0.74) to predict who will suffer from depressive or anxiety disorder within a 2-year period. Being able to predict which individuals are most likely to develop a depressive disorder or an anxiety disorder may aid in directing preventive interventions to those most at risk. Preventive interventions have been shown as an effective strategy in reducing the occurrence of depressive and anxiety disorders, in a variety of settings, Reference Muñoz, Cuijpers, Smit, Barrera and Leykin6 lowering the burden of these high-impact and widespread disorders. In a recent review, Muñoz et al Reference Muñoz, Cuijpers, Smit, Barrera and Leykin6 concluded that at least 22% and up to 50% of cases of major depressive disorder could be prevented each year. Studies on risk factors such as this one can improve the effectiveness of preventive intervention by pointing out who is most likely to benefit from the intervention. Future research may further narrow down the population most at risk. For example, Cuijpers et al Reference Cuijpers, Smit and Willemse37 found that a family history of depressive disorder and chronic illnesses predicted the occurrence of major depressive disorder among those with subthreshold depression.
Outside of the research context, the cooperation of participants in interventions is known to drop. This may be especially true for preventive interventions, when there are no symptoms that are discomforting or impairing. However, it is not a good reason to give up on the prevention of depressive or anxiety disorder. Given the large numbers of people involved and the large impact these disorders have on quality of life and functioning, even if only a relatively small percentage of those eligible are engaged, prevention would yield both considerable and worthwhile gains. Studies that can pinpoint those most at risk can improve adherence rates. Knowing with a degree of certainty that a depressive or anxiety disorder is likely to be a reality in the near future may motivate those at risk. Keeping preventive interventions as non-intrusive as possible may also improve cooperation. Stepped-care models, ranging from (prolonged) monitoring, to self-help programmes, to counsellor-guided programmes and to medication, may decrease the burden of participating and improve adherence.
On a conceptual level, the finding of this study, that a history of an episode of a disorder predicts the occurrence of a subsequent episode, indicates its recurrent nature. The finding that subthreshold disorder predicts the occurrence of a full-blown episode supports the concept of a gradual onset or remission, as opposed to an ‘all-or-nothing’ occurrence. Our findings are therefore in line with a gradual shift in focus on dimensions of psychopathology, as opposed to categories, in DSM–5. Reference Andrews, Anderson, Slade and Sunderland38
Strengths and weaknesses
The present study has both weaknesses and strengths. First, although the total sample was quite large, our focus on occurrence did not allow the exploration of interactions between subthreshold disorder, a history of disorder and sociodemographic factors. Future studies may focus on this, as well as investigating additional tell-tale risk factors for the occurrence of depressive or anxiety disorders. Second, the sample size did not allow differentiation in the occurrence of the different depressive (major depressive disorder and dysthymia) and anxiety disorders (social phobia, panic disorder, agoraphobia and generalised anxiety disorder) or differentiation between different cohorts. A particular strength of this study is the prospective design, which enabled us to go beyond retrospectively collected or cross-sectional associations between risk factor and mental illness.
Summary
In conclusion, we found that a prior history of a disorder and subthreshold symptoms of this disorder both independently predicted the disorder's occurrence within 2 years with the highest risk for individuals having both. Whereas anxiety (subthreshold, in lifetime or both) predicted the occurrence of an anxiety disorder only, depression (a prior history of, subthreshold or both) predicted the occurrence of both depressive and anxiety (generalised anxiety disorder and social phobia) disorders. The ability to predict to a certain degree which individuals will develop a depressive or anxiety disorder in the near future may provide opportunities for preventive interventions for and monitoring of those most at risk.
Funding
The infrastructure for the NESDA study (www.nesda.nl) is funded through the Geestkracht programme of the Netherlands Organisation for Health Research and Development (Zon-Mw, grant number ) and is supported by participating universities and mental healthcare organisations: VU University Medical Center, GGZ inGeest, Arkin, Leiden University Medical Center, GGZ Rivierduinen, University Medical Center Groningen, Lentis, GGZ Friesland, GGZ Drenthe, Scientific Institute for Quality of Healthcare (IQ healthcare), Netherlands Institute for Health Services Research (NIVEL) and Netherlands Institute of Mental Health and Addiction (Trimbos Institute).







eLetters
No eLetters have been published for this article.