


Suicide is one of the leading causes of death and it represents a serious public health concern. Over the past 45 years worldwide suicide rates have increased by 60%, the population of adolescents and youths registering the highest increase, 1 making suicide the second cause of death in the group aged 15–29 years. 2 There are few cases of attempted suicide before puberty, but a substantial increase occurs when individuals reach adolescence and young adulthood, especially between the ages of 19 and 23 years. In recent years studies have shown that lesbian, gay and bisexual (LGB) adolescents and youths have higher rates of suicidal ideation and suicide attempts than their heterosexual peers. Reference Borges, Angst, Nock, Ruscio and Kessler3–Reference Brent and Mann5 It has been suggested that risk factors for suicidal behaviours differ between heterosexual and LGB groups, owing to the interaction of these markers with sexual orientation. Reference Remafedi and French6 Lesbian, gay and bisexual adolescents and youths are exposed to greater stigma, discrimination and victimisation within their families and romantic relationships compared with their heterosexual peers. Reference Haas, Eliason, Mays, Mathy, Cochran and D'Augelli7 Exposure to these factors may predispose these individuals to more mental health problems and suicide attempts. Reference McLaughlin, Hatzenbuehler and Keyes8,Reference Díaz, Ayala, Bein, Henne and Marin9 Minority stress theory, conceptualised as the burden of the perception of being different from others, Reference Coker, Austin and Schuster10 may explain the higher levels of health risk behaviours in LGB youth, and is related to greater stigmatisation, marginalisation and a hostile social environment. Reference Meyer11 In 2011 Marshal et al published a meta-analysis evaluating mental health in young LGB participants. Reference Marshal, Dietz and Friedman12 Their results showed an estimated overall effect size for the association between sexual orientation and suicidality of OR = 2.92 (95% CI 2.11–4.03). However, that review was limited in several ways: first, suicide attempts were analysed as a single overall variable labelled ‘suicidality’, which included suicidal ideation, suicidal plan and suicide attempt without stratified analysis; second, the population age range was 18–25 years, lacking information on adolescents; third, the majority of the articles included in their meta-analysis were cross-sectional (only one was a cohort study); and finally only studies up to 2009 were taken into account.
For our review we adopted a more general and robust approach: suicide attempts and suicide were separated for the analyses, in order to assess associations that could be specific for these outcomes, and age range inclusion criteria were enhanced, rendering our results applicable to a wider population, consistent with international recommendations. 13 Research published up to June 2015 was included, adding relevant recent information. More importantly, we assessed specific risk factors for suicidal behaviours and suicide death in the LGB population, thus contributing to filling a gap in knowledge about sexual minority groups in the adolescent and young adult populations, which have been little studied. An important characteristic of our review is that we included longitudinal studies only (either prospective cohorts or case-control studies). In fact, all except one of the articles analysed here were based on prospective cohort data. This ensured that exposure to the factors assessed preceded the outcome, making the evidence generated more relevant to establishing the temporal order of events, as well as minimising bias, improving the quality of included data and allowing us to establish valid and robust conclusions. Reference Garg, Hackam and Tonelli14,Reference Tooth, Ware, Bain, Purdie and Dobson15 There is still a need to improve understanding of suicidal behaviours of adolescent and young adult LGB populations, as well as to quantify more accurately the risk and protective factors for suicide. There is also a need to develop evidence-based public health strategies to reduce the prevalence of suicide attempts and suicide deaths among this high-risk population. We therefore undertook a systematic review of the literature, aiming to assess the extent to which sexual orientation is a risk factor for suicide attempts and suicide, and to identify risk factors for suicide attempts and suicide among LGB adolescents and young adults. The review was registered with the International Prospective Register of Systematic Reviews (PROSPERO; CRD42013005775). Reference Alonso, Castellvi, Pares, Gabilondo, Cebria and Rodriguez Marin16
Method
Recommendations from the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines for systematic reviews, Reference Stroup, Berlin and Morton17 in relation to handling and reporting of results, were taken into account. Our initial search strategy was broad in scope and inclusive, with no restriction as to population or age, in order to identify predictors of suicidal-related behaviours. Text words, titles and MeSH terms were used as search terms, including suicide, suicidal behaviour, suicide attempt, suicidality, risk factor, causality, association, protective factor, incidence, longitudinal study, observational study, cohort study, case control study, prospective study, retrospective study, follow-up, and others, resulting initially in 23 682 references after duplicates were removed. Detailed information about all the keywords used for inclusion and exclusion, and search terms used to identify suicide attempt, suicidal behaviour, population and study design are provided in online supplement DS1. The following databases were first searched up to October 2013 and updated June 2015 in order to include the most accurate data: Cochrane Library, Medline, PsycINFO, EMBASE and Web of Science. We searched grey literature using the OpenGrey European database, and reference lists from previous reviews and books were examined. No restriction of language or year of publication was applied. Corresponding authors for articles written in languages other than Spanish and English were contacted. For the broad-scope review, studies were included if they met all of the following criteria:
-
(a) reported suicide attempt or suicide as a dependent variable;
-
(b) assessed at least one risk factor for any of these outcomes;
-
(c) the study population age ranged between 12 years and 26 years, both inclusive;
-
(d) were population-based longitudinal studies (non-clinical and non-institutional sample cohorts) or case-control studies where the control group was of the same age range (non-clinical and non-institutional).
Using an expert consensus reported previously, suicide was defined as any act done with the intention of taking one's own life, whereas suicide attempt was defined as any act of self-injury with intention to die. Reference Silverman and Berman18 Other suicide-related behaviours such as suicide ideation were excluded. Using these criteria we identified 197 studies for qualitative synthesis from the broader review. To these studies we applied the following specific selection criteria: first, studies that assessed LGB orientation as a risk factor for suicide attempts or suicide compared with a heterosexual peer group of the same age range; and second, studies that evaluated risk factors for suicide attempt or suicide within LGB populations. Studies assessing only the transsexual population were excluded, owing to certain conceptual differences. It has been reported that sexual orientation is a multidimensional concept referring to an enduring pattern of emotional, romantic and/or sexual attraction to males, females or both genders, Reference Coker, Austin and Schuster10 whereas gender identity is one's own sense or conviction of maleness or femaleness. Reference Money19 Moreover, transsexual individuals are considered to constitute a clinical population because transsexualism is classified as a type of gender identity disorder, 20 and although this is a controversial issue, we are convinced that risk and protective factors may have different mechanisms of action and deserve further and specific research. Furthermore, during data synthesis, information corresponding to the transsexual population was not included.
Study selection
A multidisciplinary team of psychiatrists, psychologists, statisticians, epidemiologists and public health professionals was established to perform the review. Five groups of independent peer reviewers assessed all references. During the title review terms listed in online supplement DS1 were used, and discrepancies between reviewers were included. During the title and abstract review phases, reviewers were masked to the article's author, journal and year of publication to minimise selection bias. A third independent reviewer resolved any discrepancies during abstract and full-text review.
Data extraction
We adapted a Cochrane Collaboration data collection form for this review. Each reviewer extracted data and an independent reviewer examined the data entered in the form, checking that the information was entered properly and attempting to complete any missing data. In case of discrepancies, consensus among reviewers was established. For each article the following data were extracted: sample size; number of LGB participants included; age range; mean age; country of recruitment; study design; type of outcome (suicide death or attempt); type of sample recruited; and ethics committee approval. From cohort studies additional data were extracted: weeks of follow-up; number of suicide attempts during follow-up; and number of suicides during follow-up. Information about risk factors was obtained as odds ratios and 95% confidence intervals; multivariate analysis prevailed over bivariate analysis. If available, stratified analysis was taken into consideration.
Quality of studies
The Newcastle–Ottawa Scale (NOS) was used for assessing the quality of non-randomised studies. Reference Wells, Shea, O'Connell, Peterson, Welch and Losos21 This uses a ‘star’ system, in which a study is evaluated on three broad perspectives: the selection of the study groups, the comparability of the groups and the ascertainment of either the exposure or outcome of interest for case–control or cohort studies respectively. The scale consists of eight questions with different responses; the response indicating the highest quality is given a star. The highest-quality studies are awarded up to nine stars.
Statistical analysis
Suicide attempt and suicide were analysed comparing LGB and heterosexual groups. Additional analyses assessing specific risk factors of suicidal attempt and suicide within the LGB group were carried out. In the case of multiple publications of the same sample and predictive factors, results from the largest sample and longest follow-up were selected. Meta-analyses were performed for each variable for which there was a minimum of two studies with usable data; adjusted OR with 95% CI were used when these data were provided in the articles; if not, unadjusted ORs were taken into account. Population attributable risk (PAR) was also calculated using the formula:

where P is the prevalence of being LGB obtained through data from some of the cohort studies included in meta-analysis, Reference Fergusson, Horwood and Beautrais22–Reference Whitlock, Muehlenkamp, Eckenrode, Purington, Baral Abrams and Barreira27 and RR is the relative risk of suicide attempt in LGB v. heterosexual groups based on data from the cohort studies included. To convert the OR to RR the following formula was used:
where OR is the odds ratio of suicide attempt in LGB v. heterosexual groups and P 0 is the prevalence of suicide attempts in the heterosexual group, Reference Zhang and Yu28 calculated through meta-analysis using data from four of the included articles. Reference Fergusson, Horwood and Beautrais22–Reference Silenzio, Pena, Duberstein, Cerel and Knox25 Stata software version 13 was used to conduct the meta-analysis.
Random effect methods were used for the meta-analysis. Statistical heterogeneity was assessed by visual inspection of forest plots, by Galbraith plots, by chi-squared tests to calculate P value and by Higgins' test (I 2), which describes the percentage of observed heterogeneity that would not be expected by chance. If P was less than 0.10 heterogeneity was considered to be significant, and moderate if I 2 was 30–50% and severe if I 2 exceeded 50%. Reference Higgins and Thompson29 Small study effects (including publication bias) were assessed through visual inspection of funnel plots and Harbord's modification of Egger's test, which has been recommended for binary outcomes with effects measured as odds ratios. Reference Harbord, Egger and Sterne30 For fewer than three studies the Begg test was used. Sensitivity analyses were performed for cohort studies according to two criteria: first, length of follow-up corresponding to outcome assessment in the NOS score (less than 6 years), considering that the incidence of suicidal attempts and suicide is very low in non-clinical samples; and second, the country of origin of the samples, classified as USA v. non-USA. Because only three samples came from countries other than the USA, these could be a source of heterogeneity since there could be differences between countries in terms of social acceptance and stigma about sexual orientation.
Results
After duplicates were removed, 23 682 articles were retrieved. After reviewing titles and abstracts the full text of 1575 potentially eligible articles were reviewed and 1561 were excluded for the following reasons: 397 were not population-based cohorts or case-control studies in which the control group was non-clinical; 436 did not involve participants aged 12–26 years; 183 did not concern LGB people or assess sexual orientation as a risk factor; 350 did not treat suicide or suicide attempt as a dependent variable; and 95 did not assess any risk factor (Fig. 1). After these exclusions a total of 14 articles were identified, including five articles that had not been reviewed by Marshal et al, Reference Marshal, Dietz and Friedman12 even though the papers were published before 2009 and met their inclusion criteria. Of the final set of articles, ten assessed sexual orientation as a risk factor of suicide attempts or suicide, Reference Fergusson, Horwood and Beautrais22–Reference Wichstrom and Hegna24,Reference Young, Riordan and stark26,Reference Whitlock, Muehlenkamp, Eckenrode, Purington, Baral Abrams and Barreira27,Reference Fergusson, Horwood, Ridder and Beautrais31–Reference Fried, Williams, Cabral and Hacker35 three assessed specific risk factors of these outcomes among LGB, Reference D'Augelli, Grossman, Salter, Vasey, Starks and Sinclair36–Reference Burns, Ryan, Garofalo, Newcomb and Mustanski38 and one assessed both sexual orientation as a risk factor and specific risk factors among LGB. Reference Silenzio, Pena, Duberstein, Cerel and Knox25
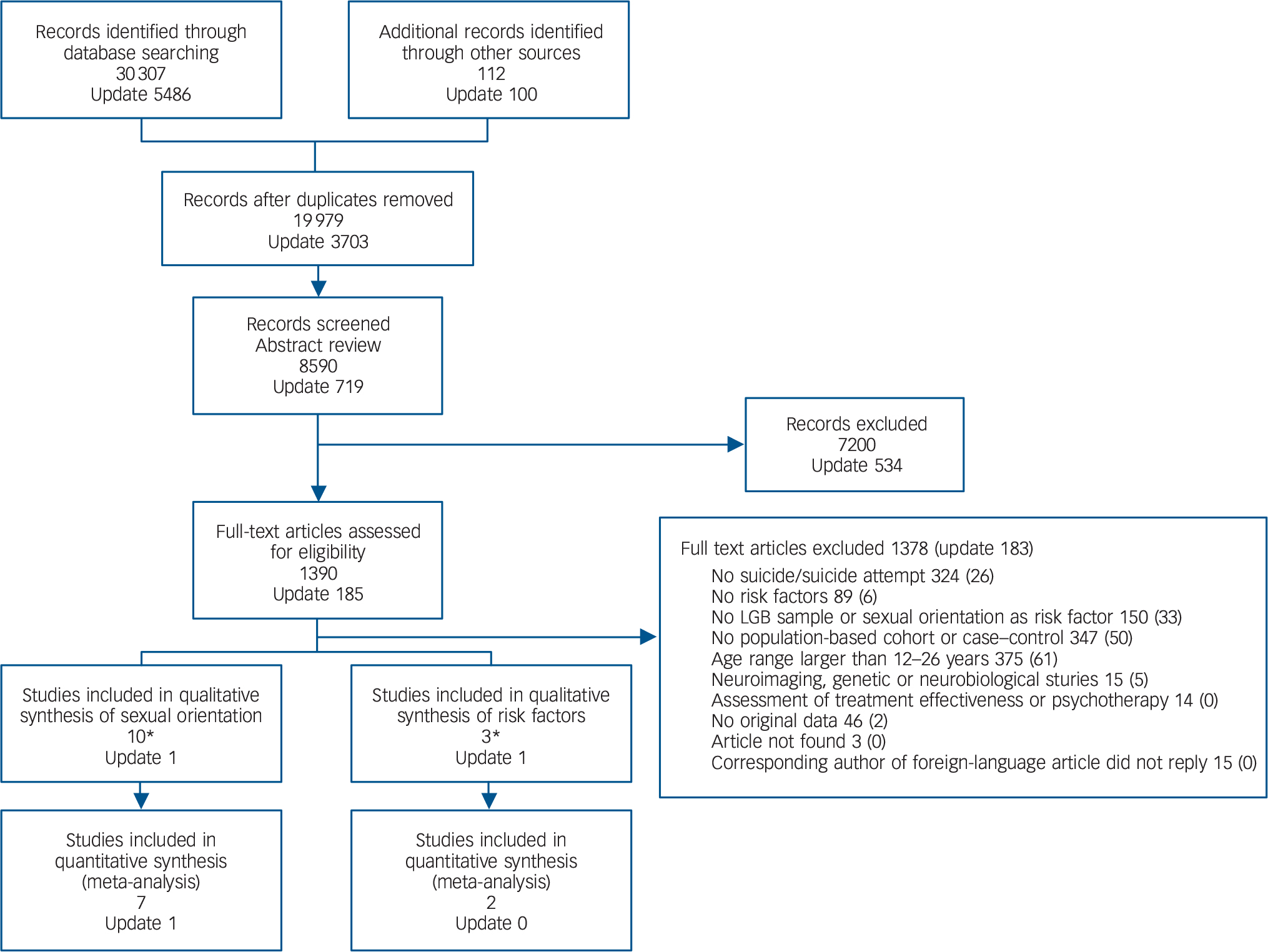
Fig. 1 Study selection. studies in the qualitative synthesis included that by *Silenzio et al which assessed both sexual orientation as a risk factor, and risk factors in the lesbian, gay and bisexual population. Reference Silenzio, Pena, Duberstein, Cerel and Knox25
Sexual orientation as risk factor
Eleven studies assessed LGB orientation as a risk factor for suicide attempt or suicide compared with heterosexual groups. These articles were published between 1995 and 2014, in four different countries: six from the USA, three from New Zealand, and one each from Norway and the UK (Table 1). Participation rates ranged from 30% to 100%. Reference Wichstrom and Hegna24,Reference Fried, Williams, Cabral and Hacker35 These studies contained data on 1634 LGB and 22117 heterosexual individuals and all of them included both male and female participants. Three studies were based on the general population, five recruited from high schools, one from a university and one among homeless adolescents. Based on data from seven of these articles, the prevalence of suicide attempts ranged from 1.5% to 3.5% in heterosexual adolescents and from 6% to 70% in LGB respondents. Ten studies assessed suicide attempt using a cohort design, Reference Fergusson, Horwood and Beautrais22–Reference Whitlock, Muehlenkamp, Eckenrode, Purington, Baral Abrams and Barreira27,Reference Fergusson, Horwood, Ridder and Beautrais31–Reference Noell and Ochs33,Reference Fried, Williams, Cabral and Hacker35 resulting in a total population of 23 484, but only one study assessed suicide using a case-control design (cases n = 120, controls n = 147); Table 1. Reference Shaffer, Fisher, Parides and Gould34
Table 1 Characteristics of included articles
| Study | Country | Study design |
Follow-up | Sample at baseline (% women) |
Sample at the end of follow-up (% attrition) |
Percentage of LGB in final sample |
Population | Outcome | Age (years) | Covariates used for adjustment |
Ethics committee approval |
|
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Range | Mean (s.d.) |
|||||||||||
| Fergusson et al (1999) Reference Fergusson, Horwood and Beautrais22 | New Zealand | Cohort | 25 years | 1265 (50) | 1007 | 2.7 | General | Suicide attempt | 14–21 | NR | Parental change, parental criminality | Yes |
| Noell et al (2001) Reference Noell and Ochs33 | USA | Cohort | 6 months | 536 | 532 (0.8) | 44.7 | Homeless | Suicide attempt | 13–20 | 18.2 (1.7) | None | Yes |
| Skegg et al (2003) Reference Skegg, Nada-Raja, Dickson, Paul and Williams23 | New Zealand | Cohort | 26 years | 1019 | 942 (7.5) | 18.2 | General | Suicide attempt | NR | NR | None | Yes |
| Wichstrom & Hegna (2003) Reference Wichstrom and Hegna24 |
Norway | Cohort | 5 years | 9679 | 2924 (69.7) | 6.5 | High school | Suicide attempt | 12–20 | 14.9 (1.7) | Previous suicide attempt depression | Yes |
| Bearman & Moody (2004) Reference Bearman and Moody32 | USA | Cohort | 1 year | 20 745 | 13 465 (35) | NR | High school | Suicide attempt | NR | NR | School clustering, grade range, school size, ethnic mix, region, urbanisation |
NR |
| Fergusson et al (2005) Reference Fergusson, Horwood, Ridder and Beautrais31 | New Zealand | Cohort | 25 years | 1265 (50) | 967 (23.5) | 11.9 | General | Suicide attempt | 21–25 | NR | Gender, childhood sexual abuse, childhood physical abuse, parental illicit drug use, novelty-seeking, parental criminality, parental attachment |
Yes |
| D'Augelli et al (2005) Reference D'Augelli, Grossman, Salter, Vasey, Starks and Sinclair36 | USA | Cohort | 2 years | 528 | 361 (31.6) | 100 | LGB | Suicide attempt | 15–19 | NR | None | Yes |
| Silenzio et al (2007) Reference Silenzio, Pena, Duberstein, Cerel and Knox25 | USA | Cohort | 9 months | 14 322 | 13 834(3.5) | 3.1 | High school | Suicide attempt | 18–26 | NR | Gender, age, ethnicity | Yes |
| Young et al (2011) Reference Young, Riordan and stark26 | UK | Cohort | 8 years | 2586 | 2157 (16.5) | 4.2 a | High school | Suicide attempt | NR | NR | Gender, gender non-conformity, social class, family structure, same-sex partner, religion, parental control, area deprivation |
Yes |
| Fried et al (2012) Reference Fried, Williams, Cabral and Hacker35 | USA | Cohort | 2 years | 1728 | 1728 | 4.3 | High school | Suicide attempt | 16–18 | NI | Cognitive development, smoking, failing grades, ethnicity, sexual abuse, depression, counselling, number of risk factors |
Yes |
| Mustanski & Liu (2013) Reference Mustanski and Liu37 | USA | Cohort | 4 years | 248 | 237 (4.4) | 100 | LGB | Suicide attempt | 16–20 | 18.7 (1.3) | Previous suicide attempt, depression, hopelessness |
Yes |
| Whitlock et al (2013) Reference Whitlock, Muehlenkamp, Eckenrode, Purington, Baral Abrams and Barreira27 | USA | Cohort | 3 years | 2320 | 1466 (36.8) | 24.5 | University | Suicide attempt | NR | NR | Gender, age, ethnicity, father's education level, sexual orientation, life orientation, acceptance of emotion, sense of meaning life, perceived social isolation |
Yes |
| Burns et al (2015) Reference Burns, Ryan, Garofalo, Newcomb and Mustanski38 | USA | Cohort | 2 years | 450 (0) | 449 | 100 | LGB | Suicide attempt | 16–20 | 18.9(1.3) | Ethnicity, age, sexual orientation | Yes |
| Shaffer et al (1995) Reference Shaffer, Fisher, Parides and Gould34 | USA | Case–control | NA | 267 (21) | NA | 1.1 | General | Suicide | NR | NR | NA | Yes |
LGB, lesbian, gay or bisexual; NA, not applicable; NR, not reported.
a. Calculated from a sample of 1091 individuals.
Quality of studies
Of the 11 studies that assessed sexual orientation as a risk factor, no difference in quality was seen in selection domains in the cohort studies; in terms of comparability criteria eight articles were awarded two stars because relevant confounding factors were taken into consideration in the adjustment. Reference Fergusson, Horwood and Beautrais22,Reference Wichstrom and Hegna24–Reference Whitlock, Muehlenkamp, Eckenrode, Purington, Baral Abrams and Barreira27,Reference Fergusson, Horwood, Ridder and Beautrais31,Reference Bearman and Moody32,Reference Mustanski and Liu37 However, different covariables were taken into account: one study considered demographic, psychosocial, history of mental illness, and formal and informal help-seeking variables; Reference Whitlock, Muehlenkamp, Eckenrode, Purington, Baral Abrams and Barreira27 another included antecedents of suicidal behaviour; Reference Wichstrom and Hegna24 and yet another took into account variables related to parental characteristics. Reference Fergusson, Horwood and Beautrais22 More detailed information is presented in Table 1. Regarding outcome domains, none of the studies achieved a star for ascertainment of outcome because data were self-reported by the participants and no confirmatory check of medical records was performed. The most significant difference was in length of follow-up, which was adequate only in five studies (Tables 2 and 3). Reference Fergusson, Horwood and Beautrais22–Reference Wichstrom and Hegna24,Reference Young, Riordan and stark26,Reference Fergusson, Horwood, Ridder and Beautrais31
Table 2 Quality assessment of included cohort studies
| Selection | Comparability | Outcome | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Study | Representativeness of exposed cohort a |
Selection of non-exposed cohort a |
Ascertainment of exposure a |
Demonstration outcome of interest not present at start of study a |
Comparability of cohorts on the basis of design or analysis b |
Ascertainment of outcome a |
Adequate length of follow up a |
Adequacy of follow up a |
Total stars c |
| Fergusson et al (1999) Reference Fergusson, Horwood and Beautrais22 | * | * | * | * | ** | - | * | * | 8 |
| Noell et al (2001) Reference Noell and Ochs33 | * | * | * | * | * | - | - | * | 6 |
| Skegg et al (2003) Reference Skegg, Nada-Raja, Dickson, Paul and Williams23 | * | * | * | * | * | - | * | * | 7 |
| Wichstrom & Hegna (2003) Reference Wichstrom and Hegna24 | * | * | * | * | ** | - | * | - | 7 |
| Bearman & Moody (2004) Reference Bearman and Moody32 | * | * | * | * | ** | - | - | * | 7 |
| Fergusson et al (2005) Reference Fergusson, Horwood, Ridder and Beautrais31 | * | * | * | * | ** | - | * | * | 8 |
| D'Augelli et al (2005) Reference D'Augelli, Grossman, Salter, Vasey, Starks and Sinclair36 | * | * | * | * | * | - | - | * | 6 |
| Silenzio et al (2007) Reference Silenzio, Pena, Duberstein, Cerel and Knox25 | * | * | * | * | ** | - | - | * | 7 |
| Young et al (2011) Reference Young, Riordan and stark26 | * | * | * | * | ** | - | * | * | 8 |
| Fried et al (2012) Reference Fried, Williams, Cabral and Hacker35 | * | * | * | * | ** | - | - | * | 7 |
| Mustanski & Liu (2013) Reference Mustanski and Liu37 | * | * | * | * | ** | - | - | * | 7 |
| Whitlock et al (2013) Reference Whitlock, Muehlenkamp, Eckenrode, Purington, Baral Abrams and Barreira27 | * | * | * | * | ** | - | - | - | 6 |
| Burns et al (2015) Reference Burns, Ryan, Garofalo, Newcomb and Mustanski38 | * | * | * | * | * | - | - | * | 6 |
a. A maximum of one star can be allotted in this category.
b. A maximum of two stars can be allotted in this category.
c. Highest-quality studies are awarded up to nine stars (–, no star awarded).
Table 3 Quality assessment of case–control study

| Study | Case definition a |
Representativeness of cases a |
Selection of controls a |
Definition of controls a |
Comparability of cases and controls b |
Ascertainment of exposure a |
Same method of ascertainment in both groups a |
Non response rate a |
Total stars c |
|---|---|---|---|---|---|---|---|---|---|
| Shaffer et al (1995) Reference Shaffer, Fisher, Parides and Gould34 | - | – | * | * | * | – | * | * | 5 |
a. A maximum of one star can be allotted in this category.
b. A maximum of two stars can be allotted in this category.
c. Highest-quality studies are awarded up to nine stars (–, no star awarded).
Sexual orientation and suicide attempts
Three of the included studies reported a statistically significant higher risk for suicide attempt in LGB adolescents compared with a heterosexual group (adjusted OR 2.96–6.20), Reference Fergusson, Horwood and Beautrais22,Reference Silenzio, Pena, Duberstein, Cerel and Knox25,Reference Whitlock, Muehlenkamp, Eckenrode, Purington, Baral Abrams and Barreira27 whereas three studies showed a non-significant increment of risk. Reference Young, Riordan and stark26,Reference Bearman and Moody32,Reference Fried, Williams, Cabral and Hacker35 Two articles presented rates of recent suicide attempts, values ranging from 5.4% to 17.6% for males and 2.1% to 15.5% for females. Reference Fergusson, Horwood, Ridder and Beautrais31,Reference Noell and Ochs33 There were differences in terms of how sexual orientation was classified. Two studies used five categories: 100% heterosexual, mostly heterosexual, bisexual, mostly homosexual and 100% homosexual; Reference Whitlock, Muehlenkamp, Eckenrode, Purington, Baral Abrams and Barreira27,Reference Noell and Ochs33 four articles used only three categories: opposite-sex attraction only or heterosexual, minor same-sex attraction or bisexual, and persistent major same-sex attraction or homosexual; Reference Fergusson, Horwood and Beautrais22,Reference Skegg, Nada-Raja, Dickson, Paul and Williams23,Reference Silenzio, Pena, Duberstein, Cerel and Knox25,Reference Fergusson, Horwood, Ridder and Beautrais31 and the other studies used a single item to assess sexual orientation in two categories: LGB and non-LGB. Reference Wichstrom and Hegna24–Reference Young, Riordan and stark26,Reference Bearman and Moody32,Reference Fried, Williams, Cabral and Hacker35
Eight studies were included in the meta-analysis. Adjusted OR and 95% CI from results of each article were used. A single OR value for the whole population was not provided in two studies: Skegg et al presented values stratified by gender, Reference Skegg, Nada-Raja, Dickson, Paul and Williams23 and Whitlock et al reported OR for three sexual orientation categories, Reference Whitlock, Muehlenkamp, Eckenrode, Purington, Baral Abrams and Barreira27 resulting in eleven samples included for meta-analysis. Three studies were excluded because data were either non-extractable or in a format that did not permit comparisons with the other studies. Random effect models were used because severe heterogeneity was observed (I 2 = 60%, P = 0.005). The overall pooled estimate in meta-analysis of cohort studies of suicide attempt showed a significantly higher risk for LGB youths when compared with heterosexual youths (OR = 2.32, 95% CI 1.59–3.39). Two studies appeared to be sources of heterogeneity: one assessed sexual orientation through three different categories, Reference Whitlock, Muehlenkamp, Eckenrode, Purington, Baral Abrams and Barreira27 whereas in the other the LGB sample size was only 28 but there were 979 in the heterosexual group. Reference Fergusson, Horwood and Beautrais22 Furthermore, on the Galbraith plot, these two studies were outliers. After exclusion of these two studies the new OR was 2.26 (95% CI 1.60–3.20; I 2 = 35%, P = 0.161). Visual inspection of the funnel plot does not suggest any publication bias, as small studies tend to lead to lower estimates of the effect than larger studies (Fig. 2). Although the Harbord test was not significant (P = 0.4) it is important to note that these results should be interpreted with caution, since the small number of studies means there is insufficient power to distinguish chance from real asymmetry.
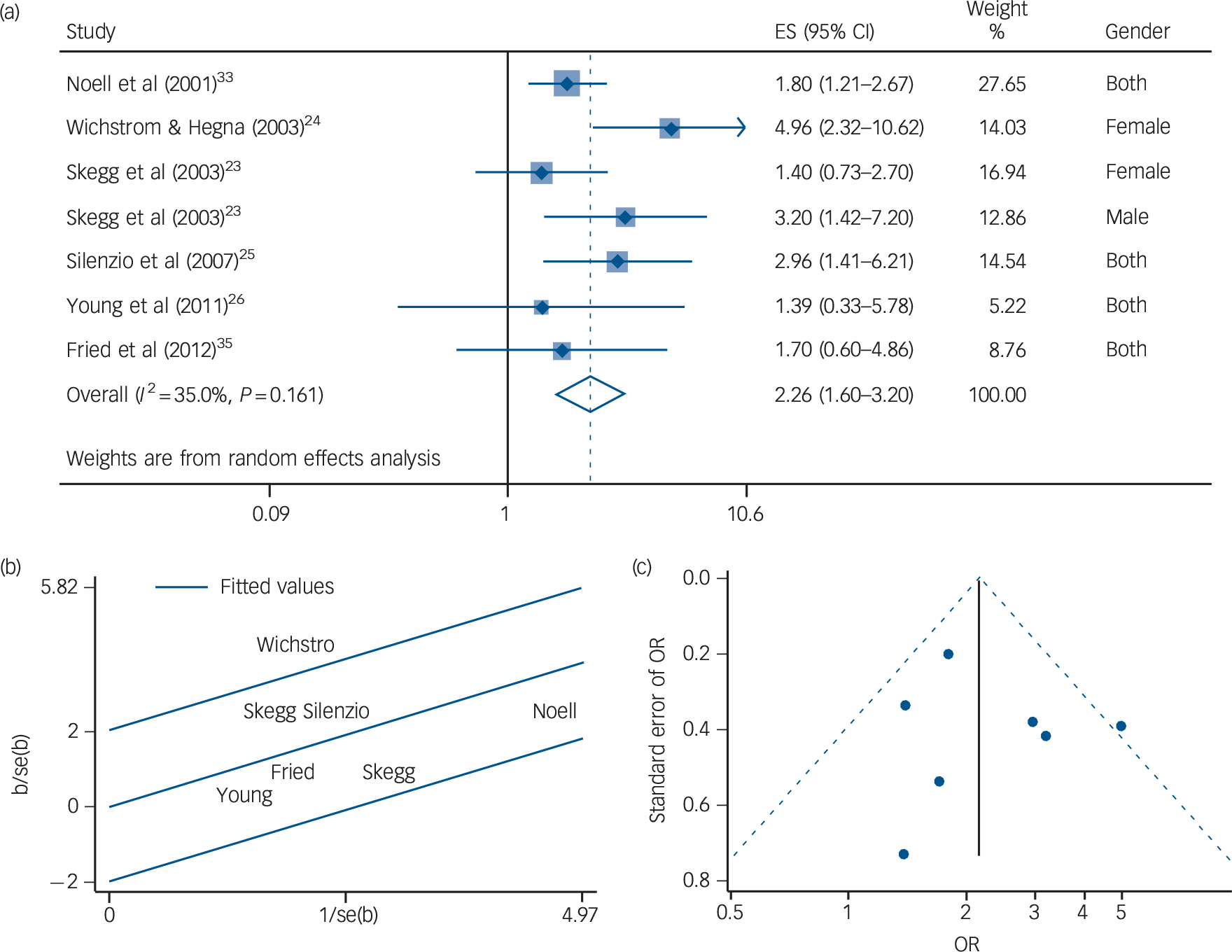
Fig. 2 Sexual orientation as risk factor for suicide attempts: (a) forest plot; (b) Galbraith plot; (c) funnel plot (Harbord test P = 0.43). ES, effect size.
Sensitivity analyses
Taking into consideration only the studies that did not appear as possible sources of heterogeneity, sensitivity analyses were carried out according to length of follow-up and country of origin of the samples. Removing three studies with insufficient length of follow-up, results were not altered substantially with respect to the association between sexual orientation and suicide attempt (OR = 2.59, 95% CI 1.58–4.26), whereas heterogeneity decreased compared with the first meta-analysis (I 2 = 45%, P = 0.122). Possible explanations for observed heterogeneity could be the differences among covariables used for the adjustment, and gender differences because one study reported results for female participants, Reference Wichstrom and Hegna24 another for males and females, Reference Skegg, Nada-Raja, Dickson, Paul and Williams23 and two studies presented a single value for both genders together. Reference Silenzio, Pena, Duberstein, Cerel and Knox25,Reference Young, Riordan and stark26 Similar results were obtained when samples from the USA were taken into account in the analyses, i.e. an increased risk in LGB youths (OR = 1.98, 95% CI 1.42–2.75) with no heterogeneity (P = 0.488).
Gender stratification
According to one study the lifetime prevalence of suicide attempts in gay and bisexual men was 4.8%, but 12.6% in lesbian and bisexual women in the same sample. Reference Skegg, Nada-Raja, Dickson, Paul and Williams23 Only two cohort studies assessed sexual orientation as a risk factor of suicide attempts stratified according to gender, Reference Skegg, Nada-Raja, Dickson, Paul and Williams23,Reference Bearman and Moody32 and one study presented results only for women. Reference Wichstrom and Hegna24 One of these articles found a significantly increased risk for lifetime suicide attempts in gay and bisexual men compared with heterosexual men (OR = 3.2, 95% CI 1.4–7.2). Reference Skegg, Nada-Raja, Dickson, Paul and Williams23 Similar results were found for the risk of lifetime suicide attempts among lesbian and bisexual women; one study reported a risk almost five times higher (OR = 4.96, 95% CI 2.29–10.62). Reference Wichstrom and Hegna24 In the other studies results in men showed that homosexual orientation was not associated with higher risk (OR = 1.71, 95% CI 0.92–3.17); Reference Bearman and Moody32 findings were similar in women: OR = 1.4 (95% CI 0.7–2.7), Reference Skegg, Nada-Raja, Dickson, Paul and Williams23 and OR = 1.25 (95% CI 0.80–1.96). Reference Bearman and Moody32
Meta-analysis found an increased risk of suicide attempts in gay or bisexual men compared with heterosexual men (OR = 2.21, 95% CI 1.21–4.04) (online Fig. DS1(a)). The Galbraith plot showed that the studies fell within confidence limits (online Fig. DS1(b)) and no publication bias was observed (Begg test, P = 0.317) (online Fig. DS1(c)). Being a lesbian or bisexual woman was associated with higher risk of suicide attempts, but this was not significant (OR = 1.97, 95% CI 0.90–4.30) (online Fig. DS2(a)) and severe heterogeneity was observed (I 2 = 79%, P = 0.008). In the Galbraith plot one study appeared as a cause of variability (online Fig. DS2(b)); Reference Wichstrom and Hegna24 after excluding this study the OR was 1.29 (95% CI 0.89–1.88). As in the analyses for men, no publication bias was observed (Begg test, P = 0.117) (online Fig. DS2(c)). Meta-analysis comparing gay with heterosexual men showed significantly increased risk (OR = 8.36, 95% CI 1.88–37.11) (online Fig. DS3(a)); a similar situation occurred when bisexual men were compared with heterosexual men (OR = 2.44, 95% CI 1.16–5.16) (online Fig. DS(3)b). The results obtained in meta-analysis of lesbian v. heterosexual women demonstrated increased risk of suicide attempt (OR = 4.31, 95% CI 1.89–9.86) (online Fig. DS3(c)); and also in bisexual v. heterosexual women, although not significant (OR = 1.56, 95% CI 0.66–3.69) (online Fig. DS3(d)).
Sexual orientation and suicide
Only one case–control psychological autopsy study evaluated completed suicide. The objective was to assess risk profiles of all people who died by suicide under 20 years of age, through interviews with their parents (or other caregiver at the time of the death), a sibling or a friend – in one case a schoolteacher who had known about the person's behaviour was interviewed. Cases were suicide deaths, controls were a random sample from telephone subscribers in the study area. Out of 120 cases that were completely investigated 79% of the individuals were male, of whom 3 were gay. No one in the control group reported any homosexual experience. Even though no odds ratio value was reported, it was stated that the difference was not significant (P = 0.088). None of the women who died by suicide was lesbian. Reference Shaffer, Fisher, Parides and Gould34
Population attributable risk
Using different values of the prevalence of being LGB corresponding to different scenarios (8%, range 4–13) and assuming the relationship between sexual orientation and suicide attempt is causal and not confounded (RR = 2.15, 95% CI 1.56–2.94), calculations suggest that 8% (range 4–13) of suicide attempts in adolescents and young adults could be attributed to sexual orientation (see online Table DS1).
Risk factors
Four studies that assessed specific risk factors for suicide attempts among the LGB population were identified (but none assessing suicide). These studies took place in the USA and were published in 2005 and 2015. Reference Silenzio, Pena, Duberstein, Cerel and Knox25,Reference D'Augelli, Grossman, Salter, Vasey, Starks and Sinclair36–Reference Burns, Ryan, Garofalo, Newcomb and Mustanski38 Participation rates ranged between almost 70% to 99.7%. Reference D'Augelli, Grossman, Salter, Vasey, Starks and Sinclair36,Reference Burns, Ryan, Garofalo, Newcomb and Mustanski38 All of them used a cohort design and together contained data on 1476 LGB people, with representation of both genders (Table 1).
Quality of studies
According to our quality assessment, no difference was seen in selection domains between the four studies. Sample sizes ranged from n = 20 to n = 449; one study analysed data from a nationally representative sample of adolescents and young adults, Reference Silenzio, Pena, Duberstein, Cerel and Knox25 whereas the other three studies recruited participants from different US cities. Reference D'Augelli, Grossman, Salter, Vasey, Starks and Sinclair36–Reference Burns, Ryan, Garofalo, Newcomb and Mustanski38 In the comparability domain, two studies achieved two stars because important confounders were taken into account in the design and/or the analysis. Two studies considered age and ethnicity as covariables for the analysis, Reference Silenzio, Pena, Duberstein, Cerel and Knox25,Reference Mustanski and Liu37,Reference Burns, Ryan, Garofalo, Newcomb and Mustanski38 whereas Burns et al also included sexual orientation. Reference Burns, Ryan, Garofalo, Newcomb and Mustanski38 The other study considered only age during the recruitment. Reference D'Augelli, Grossman, Salter, Vasey, Starks and Sinclair36 For the ascertainment of the outcome, none of the studies had a star because suicide attempts were self-reported by the participants and no reference to records had been done to confirm. In terms of length of follow-up, none of the studies achieved a star; however, in the category that assessed the adequacy of follow-up the four articles had the highest rating because attrition during the study was not related to the exposure or the assessed outcome. In general, all these studies had high overall quality (see Table 2).
Data syntheses
D'Augelli et al evaluated an important number of risk factors for suicide attempts; results showed that 61 individuals of the entire sample (n = 361) of LGB youths made a suicide attempt. Reference D'Augelli, Grossman, Salter, Vasey, Starks and Sinclair36 Risk factors such as having been more open about being LGB with their families, more often called ‘sissy’ or ‘tomboy’ by parents, more gender atypical in childhood, having experienced parental psychological abuse and a family history of depression or suicidality all presented higher prevalence or median values. Mustanski & Liu reported that having a history of suicide attempts represented an increased risk of subsequent suicide attempt whereas hopelessness and depression were not significant. Reference Mustanski and Liu37 The results obtained by Silenzio et al indicated that problem drinking, depression and problem drug use were not related to increased risk of suicide attempts in LGB respondents, contrary to findings in non-LGB participants. Reference Silenzio, Pena, Duberstein, Cerel and Knox25 Finally, results from the USA reported by Burns et al suggest that in some young LGB males from minority ethnic groups such as native Americans there is a 3-fold risk of suicide attempts compared with young White LGB men. Reference Burns, Ryan, Garofalo, Newcomb and Mustanski38 However, Black or Hispanic men do not seem to have higher risk. More details of the risk factors assessed are presented in online Table DS2. Meta-analysis of depression as a risk factor for suicide attempts in LGB adolescents showed increased risk (OR = 1.05, 95% CI 0.93–1.19; I 2 = 38%, P = 0.204) (online Fig. DS4(a)), but the result was not significant. Using a Galbraith plot no heterogeneity was observed (online Fig. DS4(b)). No publication bias was found, according to the Begg test (P = 0.317) (online Fig. DS4(c)).
Discussion
Our systematic review shows that sexual orientation is significantly associated with suicide attempts, based on meta-analysis of longitudinal studies. Nevertheless, not enough studies were found to associate sexual orientation with suicide. Sexual minority men were more likely to make suicide attempts than heterosexual men. Among women, a similar association was found but it did not reach statistical significance, probably owing to the small number of studies assessed. Few studies were found evaluating risk factors for either suicide attempts or suicide among LGB populations. Further research assessing specific risk factors is needed.
Strengths and limitations
Our systematic review has several strengths: a broad-scope search in several databases and different languages was conducted, with peer review in the screening phase, independent review in the data extraction phase and use of methods for minimising bias; corresponding authors for articles written in languages other than Spanish and English were contacted for further information; a manual search and grey literature search were also carried out; and as far as we are aware no PAR calculation of sexual orientation as a risk factor for suicide attempts has been done in previous systematic reviews.
In relation to a previous systematic review, Reference Marshal, Dietz and Friedman12 our study extended the search strategy to three additional databases and a grey literature search was also performed; we used a wider age range as an inclusion criterion, considering adolescents, and also included studies published after 2009. This resulted in 13 additional studies, 5 of which were considered for meta-analysis, adding new, relevant and useful information for the assessment of causes and mechanisms, despite our having excluded other suicide-related outcomes, such as suicidal ideation and plan, and cross-sectional studies, which had been included in the previous review. Reference Marshal, Dietz and Friedman12 These additional articles added relevant and useful new information about the risk of sexual minority groups for future suicidal behaviours and death. Moreover, our results suggest the need for further assessment about the causes and mechanisms of suicidal behaviours and death among this population. A limitation is that our search strategy was not applied to the CINAHL and Sociological Abstracts databases. Additional papers might have been retrieved if these databases had been searched; however, we searched the databases most recommended for psychiatric research, including Web of Science and PsycINFO, Reference Lohonen, Isohanni, Nieminen and Miettunen39 and also performed a manual search. Further, we searched grey literature only in OpenGrey, a European database; although it includes access to Greynet data (an international grey literature database) there is no certainty that our search was exhaustive. Overall, the use of the six particular databases in this study is in line with most strict systematic reviews and provides important coverage security. An additional limitation of our review is that the articles included came from a broader search strategy, as has been done in other systematic reviews. Reference Devries, Mak, Bacchus, Child, Falder and Petzold40–Reference Maxwell, Devries, Zionts, Alhusen and Campbell42 However, in accordance with the initial inclusion criteria, both ‘LGB population’ and ‘sexual orientation’ as a risk factor were included in the search phase. Also, we included population-based studies in our review, which could have resulted in a higher heterogeneity. However, after excluding studies that seemed to be sources of heterogeneity, OR values became similar. Finally, we used the Newcastle-Ottawa Scale to assess the quality of the studies reviewed because it had been used in previous systematic reviews, Reference Holler, Bech, Henriksen, Mikkelsen, Pedersen and Lassen43–Reference Overdevest, Jacobs, Vleggeert-Lankamp, Thome, Gunzburg and Peul46 and also because it was designed for longitudinal studies. However, evidence about its validity is still limited. Reference Wells, Shea, O'Connell, Peterson, Welch and Losos21
Comparison with other studies
Consistent with other reviews, sexual minority adolescents and youths were more likely to have made suicide attempts than their heterosexual peers. We estimated a 2-fold risk, which is similar to the risk ratios reported by King et al, which ranged from 1.96 to 2.76 in 12-month prevalence of suicide attempts, for LGB population of any age range. Reference King, Semlyen, Tai, Killaspy, Osborn and Popelyuk47 Also, Marshal et al showed a risk of 2.92 in LGB young people aged from 18 to 25 years, Reference Marshal, Dietz and Friedman12 slightly higher than our results, probably because most of the included studies were cross-sectional and their OR values ranged from 1 to 10 (ours ranged from 1.30 to 5). These facts may lead to overestimation of the risk; however, this must be interpreted with caution. We estimated the risk of suicide attempts according to sexual orientation, stratifying by gender. Our results are consistent with previous original studies which stated that being a gay or bisexual male is associated with higher risk of suicide attempt than being a heterosexual male. Longitudinal studies have found that sexual orientation is an independent risk factor for suicide attempts among young males, more so than among females. Reference Garofalo, Wolf, Wissow, ER and Goodman48 This finding could be related to results from other studies where elevated rates of suicide attempts in gay and bisexual adolescent men have been reported. Reference Botnick, Heath, Cornelisse, Strathdee, Martindale and Hogg49–Reference Russell and Toomey52 During adolescence models of gender, masculinity and femininity are reinforced; a possible explanation for observed data could be that during this stage of life these models may be affected by heteronormativity. It is important to note that gender definition covers aspects related to social categories and different life spheres, including sexual facets. Heterosexuality or homosexuality must be understood only as forms of sexual expression, since there are interrelations between non-sexual and sexual spheres. Reference Jackson53 In adolescents, the self-perception of failure to conform with this kind of model may affect different aspects of mental health. Reference Harter, Feldman and Elliott54
Among lesbian or bisexual women an increased risk of suicide attempt was found; however, it was not statistically significant, probably because few studies were identified. Our results also indicated that being bisexual is associated with higher risk of suicide attempt, but not in women; again, a possible reason could be the small number of studies. A previous systematic review summarised available research about bisexuality as a risk factor; it was associated with suicidal behaviour to a greater extent than heterosexuality. Reference Pompili, Lester, Forte, Seretti, Erbuto and Lamis55 There is no clear explanation or identification of specific risk factors acting among those with bisexual orientation. It seems therefore plausible that the same risks and mechanisms – such as more psychological distress and mental health problems (bisexuality and suicide) – act among all LGB categories.
Few studies were identified that evaluated risk factors for suicide attempts and suicide in LGB adolescents and youths. As a consequence, we could only perform a meta-analysis for the role of depression. According to our results depression does not seem to be related to suicide attempts in LGB population-based studies, in contrast to reports for the heterosexual population; however, these results should be interpreted with caution, because the lack of effect may be due to the insufficient number of included studies. Some authors suggest that minority stress theory may explain differences between the mechanisms of action of risk factors in the LGB population compared with the heterosexual population. This theory shows how specific external stressors such as victimisation, discrimination or stigma, or an internal stressor such as internalised homophobia, could increment suicide and suicidal behaviour risk. Discrimination involves anti-gay behaviour, including rejection, acts of physical violence and verbal assaults against gay men and other sexual minorities based on actual or assumed sexual orientation. Reference Machado56 Internalised homophobia refers to internalised societal homophobic attitudes, Reference Meyer57 and includes negative attitudes toward homosexuality, displeasure with sexual orientation of others, disconnectedness from other LGB individuals, and discomfort with same-sex sexual activity. Reference Meyer, Dean and Herek58
Negative ‘coming out’ reactions from family and friends, the experience of sexuality-oriented victimisation and having used drugs or alcohol to confront problems relating to their lesbian or gay identity increase the risk of attempted suicide in adolescents who discover their same-sex preference early in adolescence. Reference Hammelman59 Parental intolerance and rejection in response to the disclosure of an adolescent's sexual orientation, considered as forms of discrimination, are associated with specific risks, including depression, suicidal ideation, isolation, homelessness, prostitution, substance use, unprotected sex and sexually transmitted disease. Reference Hammelman59–Reference Ryan, Huebner, Diaz and Sanchez61 Finally, internalised homophobia was found to be significantly related to psychological distress: guilt, sex difficulties, suicide (ideation and/or behaviour) and AIDS-related traumatic stress response. Other factors such as stigma and experience of prejudice events were also significantly related to most of the measures of distress; however, internalised homophobia was reliably the most potent predictor. The interaction between these three factors causes psychological maladjustment, known as ‘psychologically injurious effects’. Reference Meyer57
Lesbian, gay and bisexual adolescents and young adults present significant differences compared with their heterosexual peers in relation to mechanisms by which risk factors act and are correlated. Risk factors such as depression, alcohol and drug misuse may be similar among LGB and heterosexual young people, but the mechanisms of action are completely different.
Generalisation of the findings
Some additional issues should be taken into consideration before generalising these results. First, the assessment of sexual orientation differed between included studies: one study assessed sexual orientation by asking if the person had ever had a sexual relation with another person of the same gender; this could be considered a sexual behaviour rather than sexual orientation. Reference Gecas and Libby62 It is important to differentiate sexual orientation from sexual behaviour. Sexual orientation is composed of emotional, romantic and/or sexual attraction, as well as an individual's sense of personal and social identity. 63 A person who has engaged in homosexual or bisexual behaviour should not necessarily be identified as lesbian, gay or bisexual. Second, we found important differences in the inclusion of confounding variables in multivariate models between the original studies. Some of them did not even adjust for any confounding variable, an important source of heterogeneity. Third, the length of follow-up in most of the cohort studies included was less than 5 years. Considering that the incidence of suicidal behaviour in the general population is low, 2 it is important to take latency into account because studies allowing for latent periods found higher incidence of the outcomes than those that ignored latency. Reference Stroup, Berlin and Morton17 However, apparently this issue did not result in heterogeneity, as may be seen in the sensitivity analyses. Finally, although no publication bias was observed according to the Harbord test, we cannot firmly exclude it owing to the small number of studies analysed, well below the overall recommendation of a minimum of 10 studies for the assessment of asymmetry. Reference O'Connor, Green, Higgins, Higgins and Green64 Even though the funnel plot should be interpreted with caution owing to the small sample size and the problems previously reported when applied to a binary outcome, Reference O'Connor, Green, Higgins, Higgins and Green64 visual inspection of the graph suggests that if any, asymmetry would be in the sense of small studies tending to lead to lower estimates of the effect than larger studies, and thus publication bias does not seem to be explaining the asymmetry. Reference Sterne, Sutton, Ioannidis, Terrin, Jones and Lau65
Future research
Although a significant association between sexual orientation and suicide attempt has been established, research is needed in several areas. Sexual orientation and gender identity ought to be measured in a homogeneous way, or using the same definition by expert consensus, to allow comparisons between studies. Information about sexual orientation could be obtained from national surveys or registers, and there is a need for an appropriate method to determine the sexual orientation of people who have died by suicide. Longitudinal studies are needed to assess mediators such as victimisation, stigmatisation and discrimination to identify causal pathways between sexual orientation and suicidal behaviour. Public health prevention strategies ought to be developed that could reduce suicide attempts by around 9%, according to our PAR calculations, which indicated that sexual orientation is a major contributor to suicidal behaviour. Inclusion of LGB participants should be encouraged in research about effective public health strategies to reduce risk factors and suicidal behaviour among the LGB population, and research should be extended to other settings, such as developing countries. Sexual orientation is associated with increased risk of suicide attempts in LGB adolescents and young adults, and gay and bisexual men are more likely to make suicide attempts; this is probably the case in women as well but our results were inconclusive. Further research is needed to establish causality between sexual orientation and suicide, and specific risk factors among the LGB population. Public health strategies for prevention of mental disorders including suicidal behaviour must be considered among the LGB population, a high-risk group in which specific factors are acting.
Funding
A.M.M. was fully supported by the Secretaria Nacional de Educacion Superior, Ciencia, Tecnologla e Innovacion, Ecuador. Additional funding for this study was provided by Institute de Salud Carlos III (), ISCIII-FEDER (), ISCIII-FIS (), ISCIII ECA07/059 and AGAUR 2014 SGR 748, Spain.
Acknowledgements
Special acknowledgements are due to Dave MacFarlane for his assistance with management of the data extraction form, and to Alejandro De La Torre for his cooperation in statistical analyses.







eLetters
No eLetters have been published for this article.