


Introduction
Over the last few decades, clinical outcomes of neonates with CHD have demonstrated significant improvement. Outcome variation has traditionally been attributed to cardiac anatomical details, surgical technique and postoperative complications. In recent years, more emphasis has been placed on other neonatal patient related factors such as gestational Reference Costello, Pasquali and Jacobs1 age or foetal growth. Reference Steurer, Peyvandi and Costello2
The impact of maternal health on foetal and neonatal health and outcomes has an established history of clinical study in neonates without CHD. The foetal origin of adult disease was first described by Barker in 1986. Reference Barker and Osmond3 Since then, several studies have found associations between neonatal or childhood diseases and certain maternal conditions. Reference Ehr and Versen-Höynck4 For example, it has been shown that children and young adults born to mothers with preeclampsia have higher cardiovascular risk factors later in life. Reference Davis, Lazdam and Lewandowski5 Further, emerging evidence from a single-centre study suggested that maternal factors such as hypertensive disorders and diabetes might contribute to outcomes in neonates with CHD with the strongest effect in the single ventricle population. Reference Savla, Putt and Huang6
This concept has been referred to as impaired foetal environment. However, population-based studies have yielded inconsistent results with some identifying impaired foetal environment as an important contributor Reference Steurer, McCulloch and Santana7,Reference Steurer, Peyvandi and Baer8 while others did not see a significant impact Reference Kristensen, Omann and Ekelund9 on outcomes in neonates with CHD.
With this multicentre study, we aimed to prospectively collect detailed data regarding impaired foetal environment to assess the impact on mortality and morbidity in two ventricle and single ventricle neonates with CHD.
Materials and methods
The Pediatric Cardiac Critical Care Consortium is a quality improvement collaborative that collects data on all patients with primary cardiac disease admitted for cardiac intensive care at participating hospitals and maintains a clinical registry to support research and quality improvement. The data managers of each participating centre collect and enter data in accordance with the standardised Pediatric Cardiac Critical Care Consortium Data Definitions Manual. The Pediatric Cardiac Critical Care Consortium registry shares common terminology and definitions with applicable data points from the International Pediatric and Congenital Cardiac Code, The Society of Thoracic Surgeons Congenital Heart Surgery Database, and American College of Cardiology Improving Pediatric and Adult Congenital Treatment Registry. The University of Michigan Institutional Review Board provides oversight for the Pediatric Cardiac Critical Care Consortium Data Coordinating Center; this study was reviewed and approved with waiver of informed consent.
For this study, a module of prospectively collected maternal-foetal environment data was linked to established Pediatric Cardiac Critical Care Consortium data from June 2019 to July 2020. All neonates undergoing cardiothoracic surgery with or without cardiopulmonary bypass at less than 31 days of age were included in this study. Neonates receiving isolated surgical patent ductus arteriosus ligation, pacemaker/defibrillator placement, or cardiac catheterisation procedure were excluded. STS-European Association for Cardio-Thoracic Surgery Congenital Heart Surgery Mortality Score (STAT) v3.41 were implemented. Society of Thoracic Surgeons high-risk preoperative factors were defined as cardiac compressions within 48 hours prior to surgery, shock present at time of surgery, hepatic dysfunction, stroke or intraventricular haemorrhage > grade II 48 hours prior to surgery and continuous renal replacement therapy for acute kidney injury. Postoperative morbidities were defined as continuous renal replacement therapy for acute kidney injury, neurologic complications (stroke, intracranial haemorrhage or seizures), mechanical circulatory support, cardiac arrest, and unplanned cardiac reinterventions.
The outcome for this study was defined as in-hospital mortality.
Our primary predictor was the degree of impaired foetal environment that was present based on the prospectively collected maternal data fields. A priori, we defined the impaired foetal environment score as the sum of the hypertensive component and the impaired sugar homeostasis component. For the hypertensive component, chronic hypertension was given 1 point, gestational hypertension 2 points, preeclampsia 3 points, and eclampsia or haemolysis, elevated liver enzymes and low platelet syndrome 4 points. For the impaired glucose hemostasis, gestational diabetes was given 1 point, preexisting diabetes 2 points, and insulin-dependent preexisting or gestational diabetes 3 points. For each component, the highest number was assigned; thus, the impaired foetal environment score ranged from a minimum value of 0 and a maximum value of 7. We checked for overdispersion of the score for the mortality outcome. We then classified impaired foetal environment into 3 groups: no impaired foetal environment defined as an impaired foetal environment score of 0, mild impaired foetal environment was defined as a score 1 or 2, and significant impaired foetal environment was defined as a score ≥3. We performed univariable logistic regression analyses to predict mortality as a function of the categorical impaired foetal environment variable. The association between impaired foetal environment score and mortality are presented as odds ratios with 95% confidence intervals.
We performed stratified analyses based on gestational age and single vs. biventricular circulation. Gestational age was defined as term versus preterm (i.e., ≥ or <37 weeks of gestational age at birth). We defined single ventricular (single ventricle) circulation based on the fundamental diagnosis provided by Pediatric Cardiac Critical Care Consortium for lesions that are consistent with single ventricular physiology.
Centres who had >50% missing data in one of the fields contributing to the impaired foetal environment scores were excluded from the analyses. Cases with missing hospital mortality were excluded as well. We then proceeded with a complete case analysis (i.e., all cases with complete data were used). To check for potential bias due to missing data, we performed sensitivity analyses by a) analysing the cases with missing impaired foetal environment data as a separate category, b) only including data from centres with <10% missing impaired foetal environment data, c) setting all missing impaired foetal environment scores to maximum (severe impaired foetal environment), and d) setting all impaired foetal environment scores to minimum (no impaired foetal environment).
All analyses were performed using STATA Version 18 (Stata Corp, College Station, TX).
Results
There were a total of 1913 neonates included in this study from 26 different centres. 55 neonates from 1 centre were excluded because that centre had >50% of missing impaired foetal environment data, and 26 neonates were excluded due to missing hospital mortality, leaving 1832 neonates for our analysis. 218 patients had at least 1 missing impaired foetal environment data field (11.8%). 1380 (75.3%) patients had a biventricular circulation and 452 (24.7%) had a single ventricle circulation. A total of 266 (14.5%) patients were born preterm (<37 weeks of gestation).
Supplemental Table 1 shows baseline characteristics. Patients with single ventricle circulation were more likely to be born at term (89.5% versus 84.5%, p = 0.007). As expected, hospital mortality was higher in the single ventricle circulation population (12.4% versus 5.2%, p < 0.001).
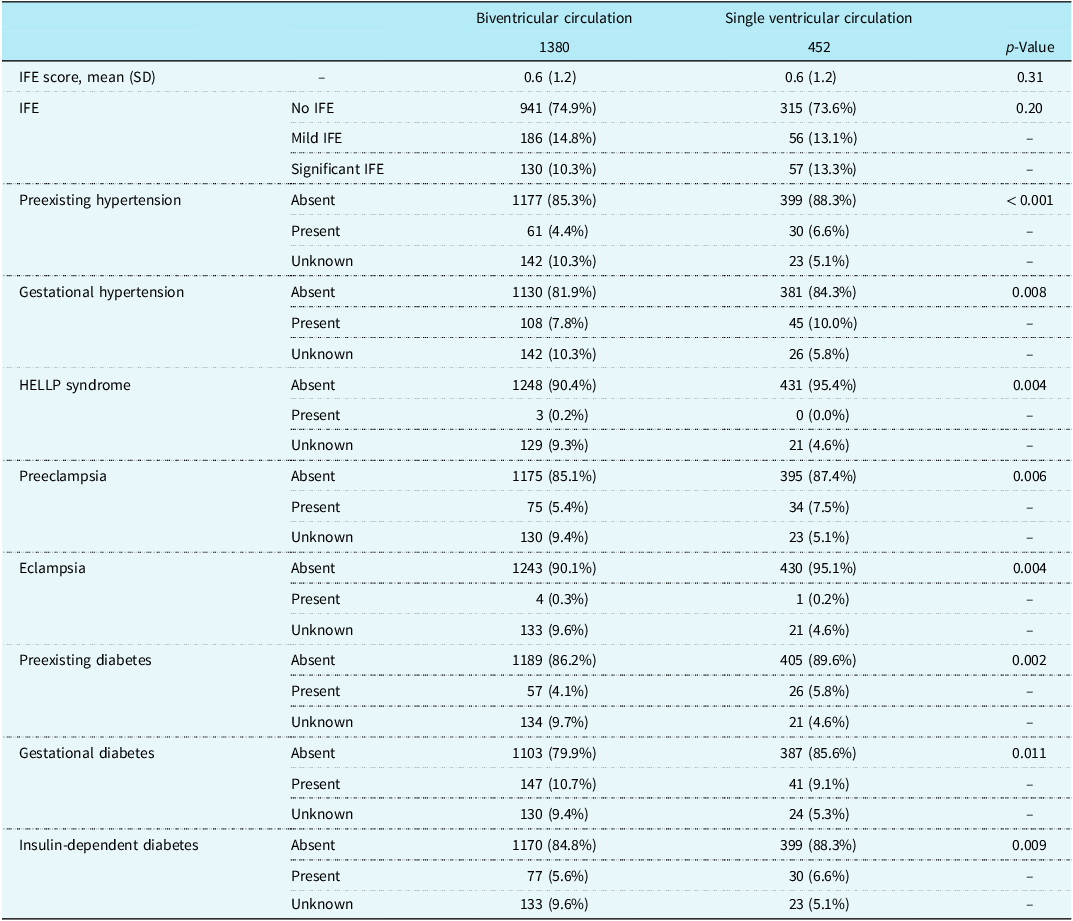
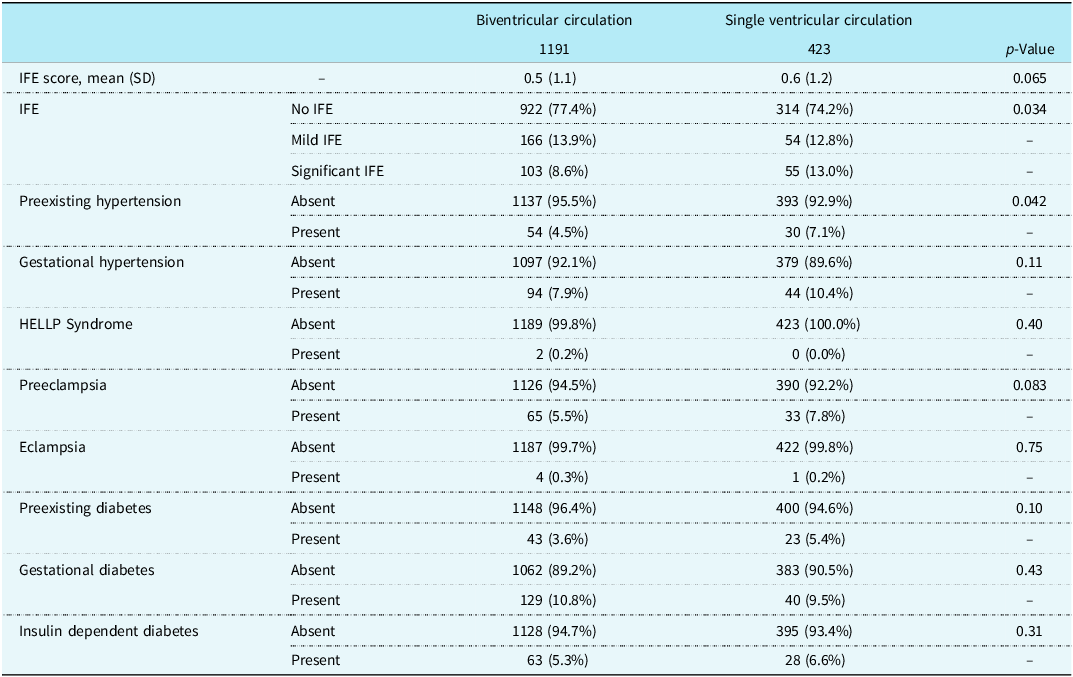
Table 1 shows the incidence of maternal conditions contributing to impaired foetal environment in the single ventricle and biventricular circulations. While the impaired foetal environment categories were not significantly different between the two groups, preexisting and gestational hypertension, preeclampsia, preexisting, and insulin-dependent diabetes were more frequent in the single ventricle population, while haemolysis, elevated liver enzymes and low platelet syndrome, eclampsia and gestational diabetes were more frequent in the biventricular population (p < 0.05, Table 1). Table 2 shows the same data limited to patients without any missing data. The incidence of impaired foetal environment is higher in the single ventricle circulation group (p = 0.034). However, from all maternal conditions only preexisting hypertension was significantly more frequent in the single ventricle group (7.1% versus 4.5%, p-value 0.042).
Incidence of maternal conditions by single and bi-ventricular circulation

Table 1 Long description
The table compares the incidence of maternal conditions contributing to an impaired fetal environment in single ventricle and biventricular circulations. It has 12 rows and 5 columns. The columns are labeled Biventricular circulation, Single ventricular circulation, and p-Value. The rows are labeled with different maternal conditions and their categories. Row 1: IFE score, mean (SD), Biventricular circulation: 1380, Single ventricular circulation: 452, p-Value: 0.31. Row 2: IFE, Biventricular circulation: No IFE 941 (74.9 percent), Mild IFE 186 (14.8 percent), Significant IFE 130 (10.3 percent), Single ventricular circulation: No IFE 315 (73.6 percent), Mild IFE 56 (13.1 percent), Significant IFE 57 (13.3 percent), p-Value: 0.20. Row 3: Preexisting hypertension, Biventricular circulation: Absent 1177 (85.3 percent), Present 61 (4.4 percent), Unknown 142 (10.3 percent), Single ventricular circulation: Absent 399 (88.3 percent), Present 30 (6.6 percent), Unknown 23 (5.1 percent), p-Value: less than 0.001. Row 4: Gestational hypertension, Biventricular circulation: Absent 1130 (81.9 percent), Present 108 (7.8 percent), Unknown 142 (10.3 percent), Single ventricular circulation: Absent 381 (84.3 percent), Present 45 (10.0 percent), Unknown 26 (5.8 percent), p-Value: 0.008. Row 5: HELLP syndrome, Biventricular circulation: Absent 1248 (90.4 percent), Present 3 (0.2 percent), Unknown 129 (9.3 percent), Single ventricular circulation: Absent 431 (95.4 percent), Present 0 (0.0 percent), Unknown 21 (4.6 percent), p-Value: 0.004. Row 6: Preeclampsia, Biventricular circulation: Absent 1175 (85.1 percent), Present 75 (5.4 percent), Unknown 130 (9.4 percent), Single ventricular circulation: Absent 395 (87.4 percent), Present 34 (7.5 percent), Unknown 23 (5.1 percent), p-Value: 0.006. Row 7: Eclampsia, Biventricular circulation: Absent 1243 (90.1 percent), Present 4 (0.3 percent), Unknown 133 (9.6 percent), Single ventricular circulation: Absent 430 (95.1 percent), Present 1 (0.2 percent), Unknown 21 (4.6 percent), p-Value: 0.004. Row 8: Preexisting diabetes, Biventricular circulation: Absent 1189 (86.2 percent), Present 57 (4.1 percent), Unknown 134 (9.7 percent), Single ventricular circulation: Absent 405 (89.6 percent), Present 26 (5.8 percent), Unknown 21 (4.6 percent), p-Value: 0.002. Row 9: Gestational diabetes, Biventricular circulation: Absent 1103 (79.9 percent), Present 147 (10.7 percent), Unknown 130 (9.4 percent), Single ventricular circulation: Absent 387 (85.6 percent), Present 41 (9.1 percent), Unknown 24 (5.3 percent), p-Value: 0.011. Row 10: Insulin-dependent diabetes, Biventricular circulation: Absent 1170 (84.8 percent), Present 77 (5.6 percent), Unknown 133 (9.6 percent), Single ventricular circulation: Absent 399 (88.3 percent), Present 30 (6.6 percent), Unknown 23 (5.1 percent), p-Value: 0.009.
IFE = impaired foetal environment.
Incidence of maternal conditions by single and bi-ventricular circulation for patients without any missing data

IFE = impaired foetal environment.
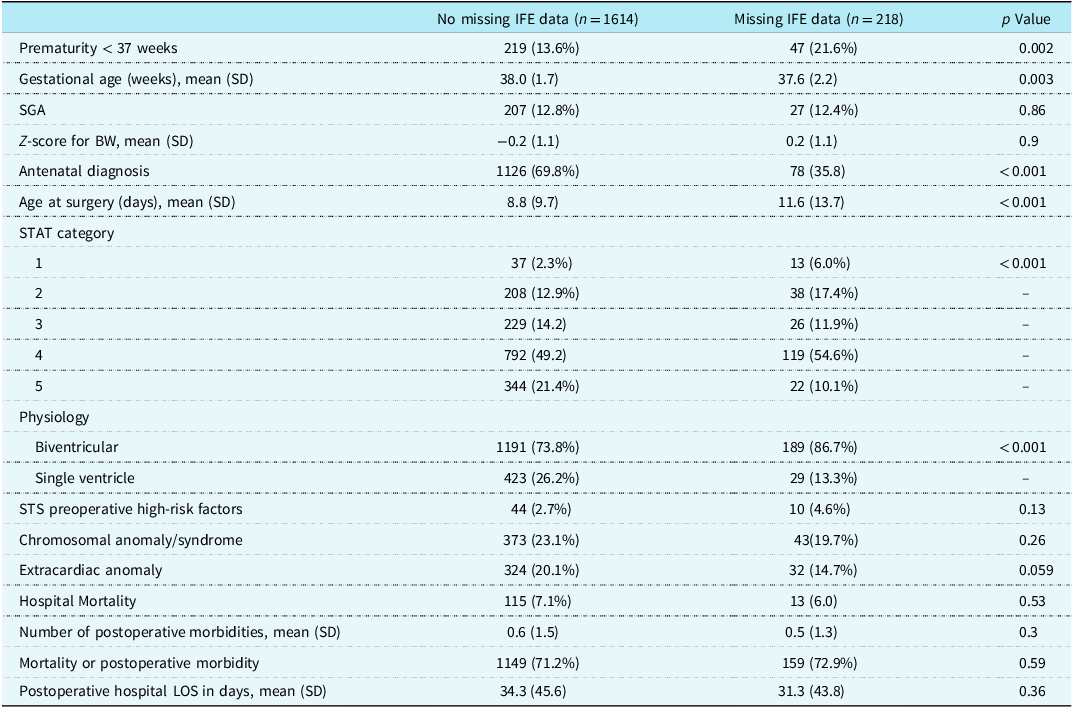
Table 3 shows the association of missing data with certain patient characteristics. Data were more likely to be missing in neonates born preterm or with biventricular circulation, in the absence of prenatal diagnosis, or with lower STAT score categories.
Association of factors with missing impaired foetal environment data

BW = birth weight; GA = gestational age; IFE = impaired foetal environment; SD = standard deviation; SGA = small for gestational age; STS = society of thoracic surgeons; STAT = cardio-thoracic surgery congenital heart surgery mortality categories.
There was no difference in mortality by impaired foetal environment category in the biventricular circulation group. Interestingly, there was a trend towards higher mortality with increase in impaired foetal environment severity in patients with single ventricle circulation: 11.5% for patients without impaired foetal environment and 16.4% in patients with significant impaired foetal environment; however, this did not reach statistical significance, odds ratio 1.27, 95% confidence interval 0.87, 1.85 (Figure 1 and Supplemental Table 2). Considering gestational age, no mortality difference by impaired foetal environment score was identified among preterm or term neonates with biventricular circulation (Figure 1 and Table 3). However, in the preterm single ventricle population, a strong trend was observed, with mortality rates of 8.7% in patients without impaired foetal environment and 33.3% in patients with significant impaired foetal environment. Due to the small patient number in this group (n = 38), this trend did not reach statistical significance (odds ratio 2.35, 95% confidence interval 0.93–5.88, Figure 1 and Table 3).
Mortality based on impaired foetal environment categories. IFE = Impaired Foetal Environment; SV = Single Ventricular; BV = Biventricular.

Figure 1 Long description
Panel A: A bar graph depicts hospital mortality percentages in neonates based on impaired foetal environment categories. The x-axis represents different categories of impaired foetal environment (IFE): no IFE, mild IFE, significant IFE, and missing IFE. The y-axis represents hospital mortality percentage. The graph compares two types of circulation: BV circulation (blue bars) and SV circulation (orange bars). The sample sizes for each category are provided below the x-axis. Panel B: A bar graph depicts hospital mortality percentages in term neonates based on impaired foetal environment categories. The x-axis represents different categories of impaired foetal environment: no IFE, mild IFE, significant IFE, and missing IFE. The y-axis represents hospital mortality percentage. The graph compares two types of circulation: BV circulation (blue bars) and SV circulation (orange bars). The sample sizes for each category are provided below the x-axis. Panel C: A bar graph depicts hospital mortality percentages in preterm neonates based on impaired foetal environment categories. The x-axis represents different categories of impaired foetal environment: no IFE, mild IFE, significant IFE, and missing IFE. The y-axis represents hospital mortality percentage. The graph compares two types of circulation: BV circulation (blue bars) and SV circulation (orange bars). The sample sizes for each category are provided below the x-axis.
Several analyses support the randomness of missing data. Supplemental Table 2 and Figure 1 demonstrate no significant difference in mortality by gestational age and physiology between missing data set to significant impaired foetal environment and no impaired foetal environment. Sensitivity analysis showed similar results (Figure 2).
Sensitivity analyses for mortality. IFE = Impaired Foetal Environment; SV = Single Ventricular; BV = Biventricular.

Discussion
This is the first multicentre prospective study aimed to evaluate the association between impaired foetal environment and postoperative mortality in neonates with CHD. While the overall cohort did not demonstrate a statistically significant relationship between impaired foetal environment and mortality, a notable trend emerged among preterm infants with single-ventricle physiology, suggesting increased mortality associated with more severe impaired foetal environment. The absence of statistical significance in this subgroup is likely attributable to the limited sample size and the substantial proportion of missing data.
The impact of impaired foetal environment on postoperative outcomes in neonates with CHD was first described by Gaynor et al. in 2018. In this single-centre study, impaired foetal environment was commonly identified in pregnancies in which the foetus had CHD. Among neonates undergoing cardiac surgery, the presence of impaired foetal environment was associated with lower survival at 36 months of age for the entire cohort and for the subgroup with hypoplastic left heart syndrome. Reference Gaynor, Parry and Moldenhauer10 However, prematurity was included in their definition of impaired foetal environment, potentially contributing to this large effect. In a follow-up study of 273 single ventricle infants after stage 1 Norwood palliation which did not include prematurity in the definition of impaired foetal environment (instead used it as a mediator), the hazard ratio of death at 36 months remained significantly elevated among infants exposed to impaired foetal environment (hazard ratio 6.05; 95% confidence interval, 3.59–10.21). Reference Savla, Putt and Huang6 Population-based studies have shown conflicting results. The study using an administrative California-wide database confirmed the association of impaired foetal environment and 1-year mortality in infants with CHD, although the effect size was attenuated with a hazard ratio of 1.55 (95% confidence interval 1.34–1.78). Reference Steurer, Peyvandi and Baer8 This decrease in effect size is not surprising, as administrative datasets rely on ICD codes and non-differential misclassification that biases the effect size towards the null is common. The same study demonstrated that small for gestational age status and placental abruption are the main driver behind the increased mortality rates in neonates with impaired foetal environment and CHD. Reference Steurer, Peyvandi and Baer8 Interestingly, using the same database impaired foetal environment was shown to be a significant mediator explaining some of the racial and ethnic disparities. Reference Santana, Peyvandi and Costello11 In contrast, Kristensen et al. showed no association of impaired foetal environment and mortality in children with CHD undergoing cardiac operations in Denmark from 1994 to 2018. Reference Kristensen, Omann and Ekelund9 Possibly, these findings may be reflective of the marked difference in maternal health and prenatal health service of that country, as well as secondary to differences in the composition of CHD and age at surgery. In our prospective multicentre study, we found a trend towards higher mortality in preterm infants with single ventricle physiology exposed to impaired foetal environment. This is in accordance with the studies by Gaynor Reference Gaynor, Parry and Moldenhauer10 and Savla Reference Savla, Putt and Huang6 who also found the biggest impact on infants undergoing Stage 1 Norwood palliation.
The lack of statistical significance in our study may be attributed to decreased power due to the degree of absent data. Collecting prenatal maternal data in the neonatal cardiac population is a unique challenge, even above typical neonatal studies. In the past, these patients would often be admitted to a neonatal ICU and then transferred a cardiac ICU post-operatively. However, over the past decade we have seen a shift toward admission directly to a cardiac ICU from the delivery hospital Reference Chaudhry, Sen and Steurer12 with variable involvement of a neonatal team. This leads to a lower likelihood of maternal data being recorded at the time of admission, as cardiac ICU staff are less likely (especially in the case of term neonates) to include such factors on initial documentation. Impaired foetal environment a neonate with CHD is born preterm and remains in the neonatal ICU prior to admission to the cardiac ICU, this information may be more easily collected, but only if the neonatal ICU is within the same electronic medical record system. Dealing with two medical records that need to be connected or linked is not always straightforward and depends on the electronic medical record setup of each individual hospital system. If a patient is born at a different hospital and then transferred, loss of access to maternal data is almost certain. We found that impaired foetal environment data were missing in more than 10% of patients. Maternal smoking, for example, was missing in >50% of records and thus was not used for data analysis but is known to be an important contributor to impaired foetal environment and therefore likely would have had a significant impact on our data. Reference Savla, Putt and Huang6 The Cardiovascular Round Table of the European Society of Cardiology held a workshop among international experts in cardiovascular clinical research and health informatics to explore how electronic medical record could advance cardiovascular clinical research. Reference Cowie, Blomster and Curtis13 Cowie et al. summarised their findings, and while acknowledging multiple limitations regarding electronic medical record in research, they don’t report on challenges associated with linking mother and baby records. It may be that European national health systems provide an improved infrastructure over private healthcare in the United States. However, the consistent ability to retrieve maternal, perinatal, and neonatal data would facilitate powerful research opportunities. Reference Cowie, Blomster and Curtis13 Chaudhry et al. have previously discussed the need for the creation impaired foetal environment a specific database for neonates with CHD, acknowledging both—the data gaps that occur in neonatal databases regarding cardiac and surgical specific data and those that occur in cardiac/surgical databases regarding maternal, prenatal, and perinatal data. Reference Chaudhry, Ball and Hamrick14 Without a centralised database that includes all levels of this data, abstracted by skilled neonatal AND cardiac champions, we will continue to miss opportunities for important clinical advances.
Factors that were clearly associated with increased missingness were prematurity, post-natal cardiac diagnosis, older age at surgery, lower STAT category, and biventricular circulation. Premature infants might have been born without much warning and thus without complete maternal work up. For example, gestational diabetes is commonly first tested for between 24 and 28 weeks gestation, and therefore, mothers who deliver prior to this point may not have a “diagnosis” of gestational diabetes even if they do have an impaired glucose tolerance environment. Antenatal diagnosis also leads to higher likelihood of delivery at a high-risk obstetric hospital with early transfer to the receiving paediatric critical care consortium centre. These patients were often already being followed by cardiology and therefore have more robust records even within the prenatal period. Older age at surgery, lower STAT category, and biventricular circulation were all associated with an increased degree of data gaps; these variables point towards less severe forms of CHD which may reflect lower rates of prenatal diagnosis and later transfer of neonates to the cardiac ICUs, leading to a lower likelihood of accompanying maternal data.
The extent of missingness of impaired foetal environment data is a serious limitation and was not anticipated in this study. It led to decreased power, and our negative results need to be assessed acknowledging this. The study per se was not powered for a certain effect size, and the enrolment was time limited. However, looking at the preterm single ventricle group, the absolute mortality difference in this study was 24.6% between neonates without impaired foetal environment and neonates with severe impaired foetal environment; this did not reach statistical significance given our small numbers (n = 23 in the no impaired foetal environment group and n = 15 in the significantly impaired foetal environment group). With a higher sample size (i.e., n = 42 in each group), this result would reach statistical significance with a power of 0.8 and a p-value < 0.05. It is important to state that despite the lack of statistical significance in this study, it would be wrong and potentially harmful, to deem impaired foetal environment as a non-important predictor. Further studies should focus on the preterm single ventricle group and aim for complete data and appropriate sample size.
The additional concern with missing data is non-randomness. For example, many Pediatric Cardiac Critical Care Consortium centres have associated high-risk delivery units with easily accessible maternal records. We performed several sensitivity analyses to demonstrate that missing data were most likely random. A second limitation is that the patient population was limited to those in a cardiac ICU. One must consider that the study population has an inherent selection bias: only neonates who survived to a CICU at a tertiary care centre were included. Neonates who were not referred because they were not deemed a surgical candidate, or whose families chose comfort care pathways were not included in our cohort, or those who suffered significant complications leading to mortality prior to transfer (e.g., a preterm neonate with hypoplastic left heart syndrome who developed necrotising enterocolitis and died during their neonatal intensive care nursery stay) were not included in our cohort. It is safe to assume that many of these babies had a component of impaired foetal environment and would have thus increased the effect of impaired foetal environment on this patient group. A third limitation in our study is that point evaluations for impaired foetal environment scoring may not appropriately reflect the relative magnitude of adversity attributed to an individual risk factor.
The evidence and the biological plausibility that impaired foetal environment impacts outcomes later in life in neonates with CHD is strong. What has started as an epidemiological observation over 3 decades ago—the Barker Hypothesis Reference Barker15 —has reached in depth molecular understanding; metabolic imprinting and epigenetic influences have been found in many conditions confirming their foetal origin. Reference Dyer and Rosenfeld16–Reference Monk, Mackay and Eggermann19 In this study, we identified the group of preterm infants with single ventricle physiology as the group that might be most vulnerable to an adverse impaired foetal environment.
Our findings underscore the need for improved data collection methods to accurately assess the impact of impaired foetal environment on neonatal CHD outcomes. Establishing integrated databases that link maternal, foetal, and neonatal records could enhance research capabilities. Future studies should focus on elucidating the mechanistic pathways through which impaired foetal environment affects neonatal outcomes and explores interventions aimed at mitigating these effects. Understanding the interplay between maternal health and neonatal CHD outcomes is crucial for developing comprehensive care strategies for this vulnerable population.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951126113225.
Acknowledgements
We would like to thank Erik Michelfelder from Hospital of Atlanta, Michele Frommelt from Children’s Hospital of Wisconsin, Carly Scahill from Children’s Hospital of Colorado, Jenn Winter from Children’s Hospital of Omaha, Jeffrey Alten from Cincinnati Children’s Hospital Medical Center, Asha Nair from Lucile Packard Children’s Hospital, Jenine Davilla from Medical City Dallas Hospital, Jason Buckley from the University of South Carolina, Mike Seed from Toronto Sick Kids, Laura Brasseale from the University of Alabama and Thor Thorsson from the University of Michigan for participation in data collection for this study.
Financial support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Competing interests
None.





 Open access
Open access