


1. Introduction
Veterinarians are in high demand. Almost 96% of the 2023 graduating veterinary class in the United States had job opportunities or advanced education lined up 2 to 3 weeks before graduation (Doherty et al., Reference Doherty, McKay and Ouedraogo2024). Additionally, the US unemployment rate for veterinarians was only 0.5% (Doherty et al., Reference Doherty, McKay and Ouedraogo2024). Veterinary shortages have been indicated in the areas of non-specialist emergency care (Booth et al., Reference Booth, Rishniw and Kogan2021), low income and underserved communities (LaVallee et al., Reference LaVallee, Mueller and McCobb2017), rural communities (Villarroel et al., Reference Villarroel, McDonald, Walker, Kaiser, Dewell and Dewell2010a), and in the food animal veterinarian specialty (Tack et al., Reference Tack, McCool-Eye, Kizer, Dargatz and Turzillo2018). Of the new 2023 graduates, almost 74% indicated they were joining a companion animal practice (Doherty et al., Reference Doherty, McKay and Ouedraogo2024).
Animal and public health, including endemic and emerging disease surveillance, are critical roles of the rural practitioner as are farm and ranch success/livelihood. State and federal programs exist to incentivize rural veterinarians particularly in addressing their significant student debt loads from veterinary school. Representation and exposure to careers is critical in recruitment of any profession. With decreasing rural populations in some part due to the community features highlighted, there is a smaller student population to recruit from. This group has less opportunity to experience veterinary medicine as a career as rural practices close.
Rural human hospitals are facing similar struggles, in a review of the literature it was concluded that rural hospital closures resulted in negative economic outcomes, and increased time and distance required to access care and services (Mills et al., Reference Mills, Yeager, Unroe, Holmes and Blackburn2024). When the last medical doctor leaves a rural community people have issues facing time sensitive care and may face poorer outcomes for chronic and emergency conditions (Mills et al., Reference Mills, Yeager, Unroe, Holmes and Blackburn2024). Malone et al. (Reference Malone, Planey, Bozovich, Thompson and Holmes2022) found that hospital closure results in lower county-level income and reduced employment. For veterinarians the loss also impacts human health due to their role in zoonotic disease detection, rabies response, reportable disease surveillance and general one health coordination (Gibbs et al., Reference Gibbs2014).
Veterinarians face several decisions when choosing a practice to work for, become a partner in, or own. First, veterinarians choose which species of animals they want to focus on: small animal (companion), food animal, equine, or mixed species. Small-animal medicine typically includes pets such as cats and dogs. Food animal medicine includes the care and treatment of animals raised for food which often includes cattle, pigs, sheep, goats, and poultry. Large-animal practices often serve both food animal and equine clients. Mixed animal medicine implies a practice that sees both large animals and small animals.
Veterinarians may seek additional certifications, but they are not required to practice in most cases. Starting salaries for new graduates vary between sectors with companion animal exclusive and predominantFootnote 1 having the highest salaries, and equine and food animal predominant having lower (Doherty et al., Reference Doherty, McKay and Ouedraogo2024). However, nominal wages and real entry-level wages have grown over time in all segments (Doherty et al., Reference Doherty, McKay and Ouedraogo2024). Neill et al. (Reference Neill, Holcomb, Raper and Whitacre2019) also found that additional years of experience, hours worked per week, being male, and having a specialty certification increased income among veterinarians. They also found that veterinarians in a companion animal practice had higher salaries when compared to those in advanced education, equine, government, and mixed-animal practice type (Neill et al., Reference Neill, Holcomb, Raper and Whitacre2019). When veterinary density was increased in Neill et al.’s (Reference Neill, Holcomb, Raper and Whitacre2019) model veterinary income decreased.
Although small-, large-animal, and mixed-animal clinics may be present in both urban and rural communities, it is more likely for large-animal clinics to be present in rural areas. Therefore, once choosing which species of animal veterinarians want to focus on, individuals may choose practices based on regionality, practice structure, practice culture or a myriad of other professional and personal reasons. For example, telemedicine has been of increasing interest to the veterinary industry. Neill and Morgan (Reference Neill and Morgan2025) surprisingly found no statistically significant differences in adoption rates between rural and urban clinics. They did find that adoption rates of telemedicine were higher than teletriage, and rural practices were more likely to use remote patient monitoring daily.
Although previous studies have focused on why individual veterinarians choose to practice (Booth et al., Reference Booth, Rishniw and Kogan2021; Tack et al., Reference Tack, McCool-Eye, Kizer, Dargatz and Turzillo2018), that may not result in veterinary practice closure. Individuals can be replaced, and the loss of a veterinarian (although the loss may cause strain to the practice) may not result in clinic closure. In this analysis, we take a different approach from focusing on individual veterinarian movement by evaluating clinic closures. We believe this approach highlights a fundamental issue for communities, the loss of a business, and considers community factors that may correlate with veterinary practice closure. Our objectives are:
-
1. To determine the cross-sectional determinates of clinic closure.
-
2. Compare impacts across regionality and clinic type.
Our hypothesis is that despite amenity type attributes being a reason for individual veterinarians to choose to leave a practice, lack of amenities does not necessarily result in clinic closure.
The paper proceeds as follows: background and motivation, data/methods, results and discussion, and conclusion. We find that large-animal practices were more likely to experience closure when compared to small-animal practices, with the reverse being true for mixed-animal practices. Having a greater number of employees and being in a metro area both decreased the likelihood of closure.
2. Background & motivation
Veterinarians living and working in suburban areas have increased, while more veterinarians resided in rural areas than worked in rural areas. This implies that veterinarians who live in rural areas are not practicing in those areas and commute to urban or suburban communities (Doherty et al., Reference Doherty, McKay and Ouedraogo2024). This preference for non-rural practices can negatively impact the prevalence and success of rural veterinary clinics. Studying the time period of 1990–2010 Wang et al. (Reference Wang, Hennessy and Park2016) found that all else equal both male and female veterinarians tend to not locate in rural areas. Additionally, aversion to rural areas remained fixed over time for men, but strengthened among women (Wang et al., Reference Wang, Hennessy and Park2016).
The veterinary feed directive impacts how medically important antibiotics can be legally used for food producing animals requiring veterinarians to issue all VFD drugs within the context of a veterinarian–client–patient relationship (FDA, 2024). This increases the demand for food animal veterinarians resulting in additional efforts to identify shortage areas (Tack et al., Reference Tack, McCool-Eye, Kizer, Dargatz and Turzillo2018). Tack et al. (Reference Tack, McCool-Eye, Kizer, Dargatz and Turzillo2018) found 5 states with counties that were consistently identified as having a food animal veterinary shortage. The USDA also keeps track of veterinary shortages including private practice food animal medicine, private practice rural area food animal medicine, and public practices as part of the National Institute of Food and Agriculture Veterinary Medicine Loan Repayment Program (VMLRP) with only 5 states not having a qualified shortage (USDA, 2025a). The VMLRP helps qualified veterinarians offset a large portion of the debt incurred from veterinary school in return for their service in identified high priority veterinary shortage areas (USDA, 2025). Universities have made additional efforts to increase the number of food animal veterinarians through early admissions slots such as the University of Illinois food animal veterinarian early acceptance program, the University of Minnesota VetFAST Track program, and Iowa States PA-VEAP Program. Additionally, Texas Tech University has the admissions statement to “select students, primarily from Texas and New Mexico, who are committed to serving the veterinary, educational, and agricultural needs of rural and regional communities”, which reflects a desire to support rural veterinary medicine (Texas Tech, 2026). Additional efforts have been made to increase mentorship and strengthen food animal programs to attract students.
Previous studies have focused on understanding the choices made by veterinarians and veterinary students regarding practice location and type. Evaluating why veterinarians enter a rural practice, Villarroel et al. (Reference Villarroel, McDonald, Walker, Kaiser, Dewell and Dewell2010a) found that 60% of respondents ranked having relatives with a farm background being of high importance in their choice, and 48% ranked having a veterinary mentor who was a rural practitioner as important. Of lesser importance was being a member of 4-H or FFA (34%), being influenced by their parents (23%), and having read the stories of James HerriotFootnote 2 (23%).
In a Canadian study Hashizume et al. (Reference Hashizume, Woloschuk and Hecker2015) evaluated veterinary student perceptions over time and after having experienced a rural clinic experience. Hashizume et al. (Reference Hashizume, Woloschuk and Hecker2015) found that after rural clinical experience overall student’s attitude toward rural lifestyle, rural work–life balance, and interprofessional teamwork decreased. However, when comparing rural and urban students, rural students had higher rural lifestyle scores both at the beginning and at the end of the study (Hashizume et al., Reference Hashizume, Woloschuk and Hecker2015). This research points to the idea that increasing rural veterinarians may not be accomplished through exposure, but instead by recruiting and encouraging rural youth into veterinary medicine, or by improving rural practice workplace culture.
Villarroel et al. (Reference Villarroel, McDonald, Walker, Kaiser, Dewell and Dewell2010b) evaluated why US veterinarians chose and left rural practices. Factors that ranked high in choosing rural practices as a first job included practice atmosphere, location, caseload and variety, mentorship, quality of facilities and equipment, and potential for practice ownership. Family concerns, salary, benefits, emergency duty, insurance and time off were rated of high importance by less than half of respondents. For those who left a rural veterinary practice, the top 5 factors resulting in their departure were emergency duty, time off, salary, practice atmosphere, and family concerns (Villarroel et al., Reference Villarroel, McDonald, Walker, Kaiser, Dewell and Dewell2010b).
Rural and food animal are not synonymous, Schmitz et al. (Reference Schmitz, Vogt, Rupp, Brodersen, Abel, Wohlers and Marx2007) found that the veterinarians’ background mattered in choosing food animal. Growing up on a farm or ranch, owning livestock, and being an animal science major before entering veterinary school were all positive factors in choosing food animal. For veterinarians choosing rural practices, the most influential factors were a preference for the rural lifestyle, quality of schools, proximity to family, reasonable cost of living, and church/religious organizations (Schmitz et al., Reference Schmitz, Vogt, Rupp, Brodersen, Abel, Wohlers and Marx2007). Veterinarians choosing urban locations placed greater emphasis on reasonable cost of living, income, sufficient personal time away from work, employment of spouse, professional relationship opportunities, access to recreational activities, and access to cultural activities.
Interestingly, many of the top reasons to join a rural practice, and top reasons to leave a rural practice overlap, perhaps demonstrating the individual perceptions of the challenges and benefits of rural veterinary medicine. Given the connection to food animal veterinary medicine and rural locations, the success of our rural practices is paramount to both human and animal health. Veterinarians ensure animals are healthy before entering the food supply and are often the first line of defense for zoonotic diseases such as rabies and brucellosis. Our approach at evaluating clinic closures, as opposed to individual veterinarian decisions, will contribute to the discussion of this issue.
3. Data and methods
Unlike previous studies that rely on survey data of individual veterinarians, our analysis provides an alternate perspective of the rural veterinarian shortage by focusing instead on veterinary practices and the regional and local characteristics of the communities they inhabit. We used a unique dataset of over 10 thousand veterinary practices across 17 states,Footnote 3 evaluating characteristics of each individual practice as well as sociodemographic attributes of each county. A map of the location of included practices is available in Figure 1.
Map of nonmetro and metropolitan practice locations.

Figure 1 Long description
A map of the United States showing the distribution of veterinary practice locations. The map highlights nonmetro practice locations with red dots and metropolitan practice locations with black dots. The map covers the entire continental United States, including Alaska and Hawaii. The distribution of practice locations varies across different regions, with a noticeable concentration of both nonmetro and metropolitan practices in certain areas. The map provides a visual representation of the demand and distribution of veterinarians across the country.
3.1. Identifying veterinary practices
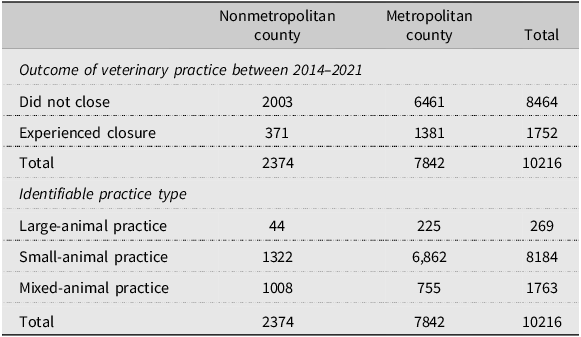
We used Data Axle longitudinal business establishment data to identify a cohort of veterinary practices that were open for business in 2014.Footnote 4 Table 1 indicates that, of the 11,677 practices in our sample, over 75% remained in business during the entire span of the analysis, with the remainder experiencing some form of business failure.Footnote 5 Establishments that were no longer operational as of 2021 were categorized as “closed,” serving as the outcome variable in our probit regression models. We also used the Data Axle data to gauge the size (i.e., number of employees) of each practice.
Veterinary practice failures by county type

Table 1 Long description
The table compares veterinary practice failures by county type between 2014 and 2021. It has two main sections: outcome of veterinary practice and identifiable practice type. The table has 4 rows and 3 columns. Column headers are Nonmetropolitan county, Metropolitan county, and Total. Row labels are Did not close, Experienced closure, Total, Large-animal practice, Small-animal practice, Mixed-animal practice, and Total. Row 1: Did not close, 2003, 6461, 8464. Row 2: Experienced closure, 371, 1381, 1752. Row 3: Total, 2374, 7842, 10216. Row 4: Large-animal practice, 44, 225, 269. Row 5: Small-animal practice, 1322, 6862, 8184. Row 6: Mixed-animal practice, 1008, 755, 1763. Row 7: Total, 2374, 7842, 10216.
Unfortunately, the Data Axle historical business database (Data Axle, 2022) does not include information specific to the veterinary industry, particularly regarding the type of veterinary practice. We employed undergraduate research assistants to use a combination of Google Maps, Yelp!, and other search engine tools, as well as contacting open clinics, to manually ascertain whether each establishment predominantly served small-animal, large-animal, or mixed-animal clientele.Footnote 6 Large and mixed-animal practices were clearly a minority (see Table 1), with large representing 29% and mixed-animal representing 19% of the total sample. However, large and mixed-animal practices combined account for over 56% of nonmetropolitan practices, suggesting the important role those veterinarians play in rural areas.
3.2. Measuring quality-of-life and sociodemographic attributes
In addition to tracking clinic size and type, we also collected data regarding quality of life in the area surrounding each veterinary establishment. To measure access to shopping and retail, we used GIS to geolocate and set a 5-mile buffer zone around each clinic and tabulated the number of shopping outlets – full-service grocery stores, big-box supercenters, and retail businesses (excluding convenience stores and dollar stores) – that fell within each clinic’s 5-mile buffer zone. We used the same method to count the number of childcare establishments within 10 miles of each clinic, recognizing that childcare is a service that consumers are generally willing to drive further distances to access. Rather than measuring the per-capita number of childcare establishments, we measured annual change in childcare availability within 10 miles of each clinic to capture recent shifts in local resources that could affect workforce stability and family decision-making, particularly for practices experiencing turnover or considering new hires.Footnote 7
We used county-level high school achievement data (Reardon et al., Reference Reardon, Ho, Shear, Fahle, Kalogrides, Jang and Chavez2021) to ascertain the relative quality of the public education options near each clinic. Although “quality of life” is a complex, multifaceted concept, with numerous empirical manifestations (Dissart and Deller, Reference Dissart and Deller2000), this combination – shopping amenities, childcare availability, and school quality – provides a strong sense of the amenities that veterinarians might consider when deciding where to locate.
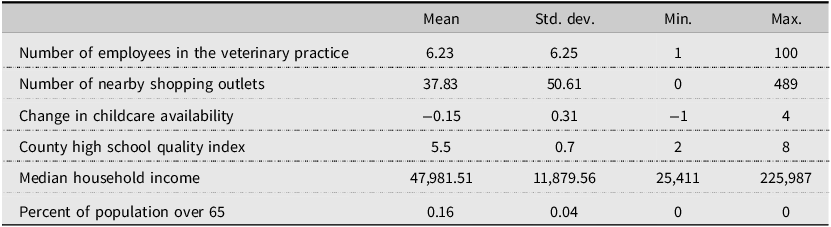
Finally, we added two variables that account for the sociodemographic heterogeneity in each county. First, median household income provides a sense of the ability (of each clinic’s prospective clientele) to pay for different veterinary services. We expected that counties with higher household incomes are able to afford more costly veterinary services, perhaps contributing to a lower likelihood of nearby clinics going out of business. We also controlled for the share of the county population over age 65, accounting for age-related differences in trends such as pet ownership (Bir et al., Reference Bir, Ortez, Olynk Widmar, Wolf, Hansen and Ouedraogo2020), and the increasing age of farmers (Census of Agriculture, 2022). Summary statistics of the quality of life and sociodemographic attributes are available in Table 2.
Descriptive statistics of veterinary practice information and county-level data n = 10,216
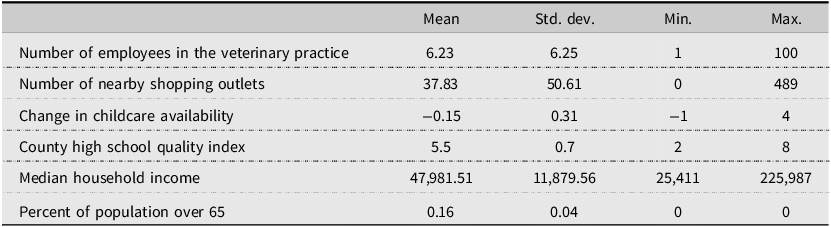
Table 2 Long description
The table presents descriptive statistics of veterinary practice information and county-level data. It includes six rows and five columns. The columns are labeled Mean, Std. dev., Min., and Max. The rows are labeled as follows: Number of employees in the veterinary practice, Number of nearby shopping outlets, Change in childcare availability, County high school quality index, Median household income, and Percent of population over 65. The values in each row are as follows: Row 1: Mean, 6.23; Std. dev., 6.25; Min., 1; Max., 100. Row 2: Mean, 37.83; Std. dev., 50.61; Min., 0; Max., 489. Row 3: Mean, -0.15; Std. dev., 0.31; Min., -1; Max., 4. Row 4: Mean, 5.5; Std. dev., 0.7; Min., 2; Max., 8. Row 5: Mean, 47,981.51; Std. dev., 11,879.56; Min., 25,411; Max., 225,987. Row 6: Mean, 0.16; Std. dev., 0.04; Min., 0; Max., 0.
To ensure that our results are not affected by excessive multicollinearity, we computed pairwise correlations and variance inflation factors (VIFs) for all model covariates. The correlation between median household income and school quality is moderate (ρ = 0.45 overall; ρ = 0.38 in nonmetropolitan counties), suggesting that the two are related but not strongly collinear. This indicates that while higher-income areas may tend to have better schools, a substantial portion of variation in school quality is not explained by income alone. All VIFs for substantive variables are below 2.1, indicating that multicollinearity is not a concern. These diagnostics support our decision to include both income and school quality as theoretically distinct predictors.Footnote 8
3.3. Empirical model
We used a binary probit model to estimate the relationship between practice attributes and local quality of life and socioeconomic characteristics and the likelihood of a veterinary practice “failing” (i.e., going out of business). We used the following equation:
 $Y_{ic}=\Phi \left(\beta _{0}+\beta _{1}P_{i}+\beta _{2}Q_{i}+\beta _{3}R_{c}+\epsilon _{ic}\right)$
$Y_{ic}=\Phi \left(\beta _{0}+\beta _{1}P_{i}+\beta _{2}Q_{i}+\beta _{3}R_{c}+\epsilon _{ic}\right)$
Where Y is the probability of failure for observation i in county c. Φ denotes the cumulative distribution function of the standard normal distribution. β 1, β 2, and β 3 are the coefficients to be estimated, representing the effects of the vectors of independent variables P, Q, and R respectively: P i is a vector of veterinary practice attributes, Q i is a vector of local quality-of-life attributes, and R c is a vector of regional (i.e., county-level) sociodemographic attributes. Finally, ϵ ic is the error term assumed to be normally distributed with mean 0 and constant variance.
We added a series of categorical dummy variables to account for state-level differences, such as varying agricultural needs and diverse regulatory environments. Additionally, we conducted a secondary model iteration, using only those veterinary practices situated in nonmetropolitan counties. This approach allowed us to disentangle the factors influencing closures in rural veterinary practices, comparing both sets of results, both in terms of magnitude and statistical significance.
It is important to clarify that our methodology tells a descriptive story rather than a causal one. The term “determinants” does not refer to the factors that cause veterinary practices to close. Rather, our analysis focuses on identifying the factors that are associated with the closure of veterinary business establishments. Future research may employ a quasi-experimental design to estimate the causal impact of veterinary practice closures. However, as this phenomenon is underexplored by applied economists, this research is nonetheless valuable to shed light on the contours of the rural veterinary shortage.
3.4. Robustness: Survival analysis
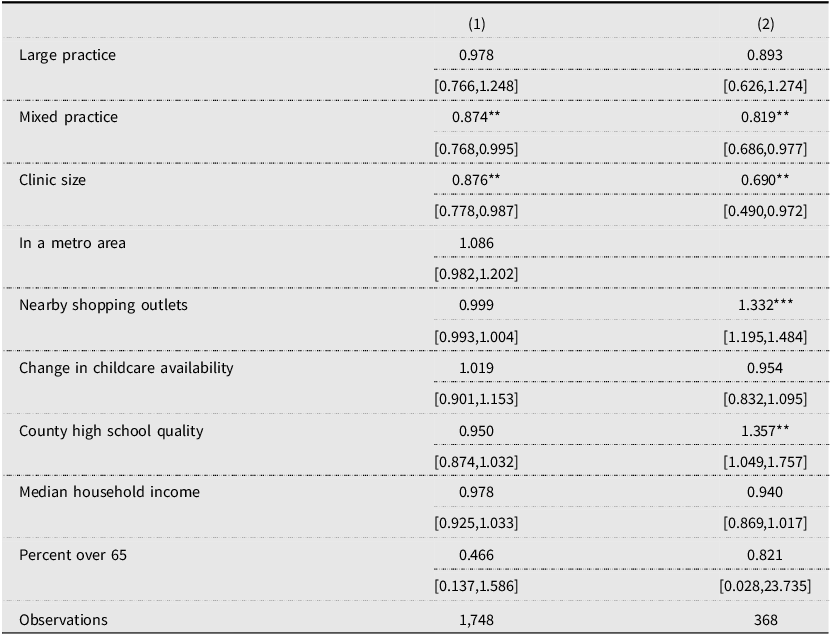
As a robustness check consistent with the cohort design (all practices open in 2014), we estimate Cox proportional hazards models with time‑to‑event defined from 2014 to closure and censoring in 2021. The covariate set mirrors the probit specification (practice type, clinic size, metro status, retail access, childcare change, school quality, income, and percent over age 65), and we stratify baseline hazards by state with robust clustered standard errors. The survival results corroborate our principal inferences – mixed‑animal practices and larger clinics have significantly lower hazards of closure – while differences for certain amenity variables in the rural subset reflect the distinct estimand (hazard vs. cumulative closure probability) and the smaller number of events used by partial likelihood. Full hazard ratios and confidence intervals are reported in Appendix Table A.
4. Results and discussion
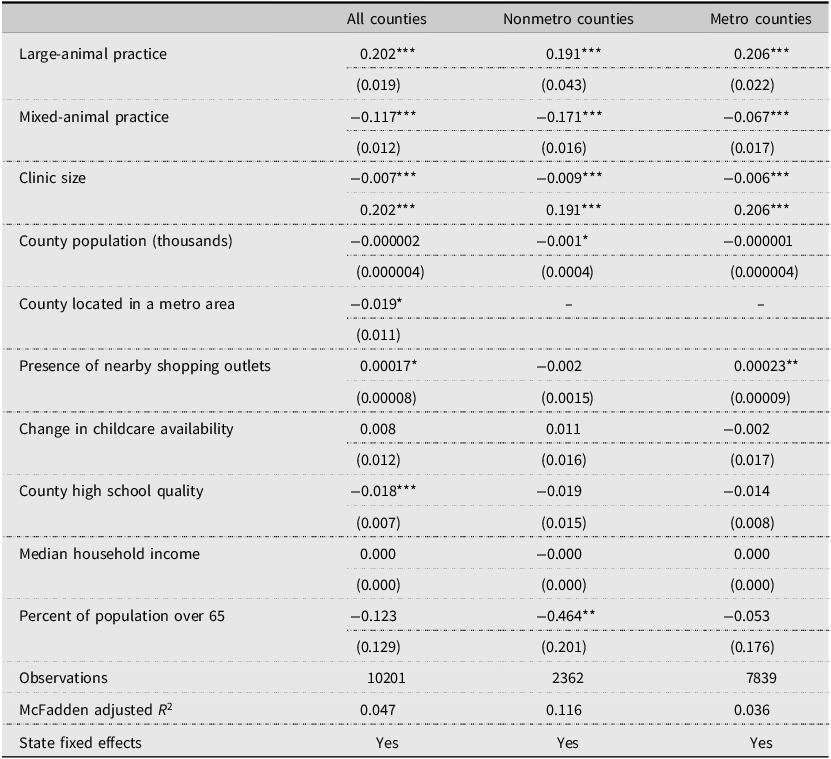
The results of our probit model are presented in Table 3.Footnote 9 Looking first at the all-counties model (first column), it is evident that, relative to those serving small animals, veterinary establishments that primarily serve large animals had a statistically significant association with experiencing closure. Conversely, we observed a negative correlation between “mixed” (i.e., both large and small) service and failure, although the strength of this correlation was slightly weaker. Turning to the second model – which only included practices outside of metropolitan areas – we observed similar results with regards to practice type. Large-animal practices in rural areas were more likely to close, while rural clinics serving both large and small animals had a statistically higher survival rate. The third model reports results for metro counties only and mirrors the pooled model for the coefficient for large-animal practices (albeit with a much lower goodness of fit).Footnote 10
Probit results of veterinary practice closure
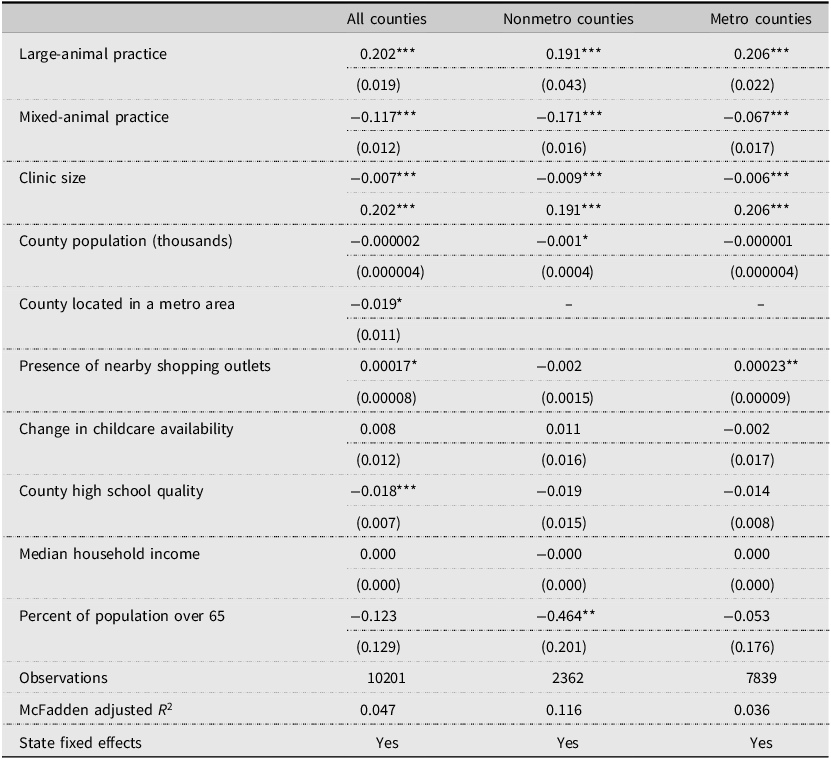
Table 3 Long description
The table presents probit results of veterinary practice closure across all counties, nonmetro counties, and metro counties. It has 14 rows and 3 columns. The columns are labeled 'All counties', 'Nonmetro counties', and 'Metro counties'. The rows include various factors such as large-animal practice, mixed-animal practice, clinic size, county population, county located in a metro area, presence of nearby shopping outlets, change in childcare availability, county high school quality, median household income, percent of population over 65, observations, McFadden adjusted R-squared, and state fixed effects. Each cell contains numerical values representing the coefficients and standard errors for each factor. Notable trends include the positive association of large-animal practice with closure in all county types and the negative association of mixed-animal practice with closure. The presence of nearby shopping outlets shows a slight positive correlation in metro counties, while the percent of population over 65 has a significant negative correlation in nonmetro counties.
Single, double, and triple asterisks (*, **, ***) indicate statistical significance at the 10%, 5%, and 1% level.
Note: results are reported as marginal effects.
We can only hypothesis as to why having a mixed-animal practice results in a lower probability of closure without additional research. Demand for veterinarians and demand for veterinary services do not necessarily correlate, and much of the literature examining these topics is now nearly two decades old. In addition, demand for veterinarians is most often evaluated at a national level, which may not accurately reflect local, state, or regional workforce needs. Several workforce assessments rely heavily on survey responses from professional veterinary organization members, whose membership is disproportionately composed of companion animal practitioners. As a result, the perspectives and service needs associated with food animal practice may be underrepresented in national workforce analyses. Furthermore, many workforce and economic datasets used to evaluate veterinary demand are not publicly available, limiting independent analysis and comprehensive evaluation of veterinary service demands.
Several consistent themes nonetheless emerge that complicate evaluating demand for food animal veterinary services. Structural changes within the livestock industry have significantly influenced the nature of veterinary service demand. Consolidation of livestock operations and increasing herd sizes have shifted veterinary roles away from individual animal treatment toward herd-level health management, preventive medicine, and production consulting. As operations grow larger and more technologically advanced, producers increasingly rely on fewer veterinarians for population health strategies, biosecurity planning, antimicrobial stewardship, and performance optimization (National Research Council, 2013).
Research also highlights differences in veterinary service needs among livestock producer types. Small-scale and backyard livestock owners often have distinct veterinary service needs compared with large commercial operations. These producers frequently seek veterinary support but may face barriers to accessing veterinary care due to cost, limited availability of veterinarians, or lack of established veterinary–client–patient relationships (Pires et al., Reference Pires, Peterson, Baron, Adams, Martínez-López and Moore2019).
Large-animal practices often have inconsistent demand which may be impacted by seasonal variations and economic pressures (Graves et al., Reference Graves, Anderson and DeNovo2020). For example, calving and foaling season may be a particularly busy time, with decreased demand during other times of the year. Producers may be willing to pay for additional services if cattle prices are high, increasing the value of breeding stock, or less willing if times are bad. Having a mixed-animal practice may help smooth revenue throughout the year, improving the success rate of mixed-animal clinics. Although Ouedraogo et al. (Reference Ouedraogo, Bain, Hansen and Dutton2018) indicates gross revenue is higher for companion animal exclusive CAE practices, Ouedraogo et al. (Reference Ouedraogo, Lefebvre and Salois2022) admit that more research is needed to understand productivity differences between practice types.
In both the all-counties model, and the nonmetropolitan counties model we see that clinic size had a negative, albeit small, statistical association with closure. In other words, veterinary establishments with more personnel were, on average, slightly less likely to experience a business closure. In a study of 409 owners of mixed and companion animal practices Ouedraogo et al. (Reference Ouedraogo, Lefebvre and Salois2022) found that non-veterinarian staff increased revenue. For example, a 1 unit increase in total number of technician hours to support 1 hour of veterinarian work increased revenue by 20.5% with no change in productivity. Nonmedical staff hours increased revenue by 17% and productivity by 14.4%. Higher staff numbers, with veterinary technicians or other employees may decrease closure rates through increased revenue and productivity. This finding was further reinforced by our robustness check using a Cox survival model (see Table A in Appendix).
Clinics located within a metropolitan area were also less likely to close during the study period, although this relationship had only weak statistical significance. Interestingly, among all the amenities and “quality-of-life” variables in our model, only one was significant: we found a strong, negative association between the average quality of high schools in the county and the closure of veterinary establishments. This implies that perhaps the most important consideration veterinary practices face within our quality-of-life variables is the quality of education provided in their local educational institutions. This may be due to a preference of veterinarians and their staff to live in an area with better schools. However, this may also be a reflection of the community and possible clientele available.
Among the remaining locational characteristics in the rural county model, only two were statistically significant. The prevalence of nearby shopping outlets was associated with a higher likelihood of survival (i.e., lower odds of closure) among rural practices. This may be a more important consideration as grocery stores, big-box supercenters, and other essential retail businesses are less abundant in rural communities and their presence (or absence) is thus more deeply felt. Opportunities to complete other shopping needs may be a draw for other surrounding rural communities who do not have a veterinarian. The idea of “killing one bird with two stones” may apply when traveling to another town for services.
Additionally, a higher share of the county population over age 65 was also associated with lower odds of closure for rural veterinary practice. As nonmetropolitan counties are already, on average, older than metropolitan counties, the presence of a higher share of the population over age 65 – likely representing a more stable client base for veterinary services – has a more pronounced effect on the survival of rural veterinary practices is not surprising.
Interestingly, the childcare variable was not statistically significant in either model. Although multiple sources indicate that childcare is a major burden for veterinarians (Larkin, Reference Larkin2013; Singler, Reference Singler2023), especially the increasing number of female veterinarians, this did not result in clinic closure. Perhaps the clinics with the greatest issues have found alternative solutions to avoid closure. Larkin (Reference Larkin2018) discusses a Texas clinic that offers its own childcare services to employees. Additional research is needed to continue to separate the personal struggles of veterinarians which may impact their choice of practice type, and the actual closure of veterinary practices. Doherty et al. (Reference Doherty, McKay and Ouedraogo2024) suggest reducing employee turnover by promoting a healthy work environment with flexible hours and encouraging employees to use their sick and vacation leave amongst other suggestions. Considering these practices to improve employee moral beyond what the community itself provides may lead to stronger veterinary practices.
While our models identify several robust predictors of veterinary clinic closure, the models explain less variation in metro counties than in rural areas. The lower explanatory power of our models in metro counties suggests that additional or different factors – such as urban market dynamics, practice specialization, or workforce characteristics – may be important determinants of clinic closure in these contexts, and future research could explore these metro-specific influences in greater detail.
Perhaps surprisingly, community income level did not impact veterinary practice closure. One could believe that a more affluent area would demand more veterinary services and be better able to sustain a veterinary practice. Bir et al. (Reference Bir, Ortez, Olynk Widmar, Wolf, Hansen and Ouedraogo2020) did find that the likelihood of seeking veterinary care increased with income for dog owners but was insignificant among cat owners. Zhang et al. (Reference Zhang, House and Salois2024) also found that the probability of using veterinary services increased as income increased. Individual choices to pursue veterinary care can be complicated and may be mitigated through the use of payment plans, or other credit programs. Additional research regarding surviving clinics clientele makeup beyond just the community itself would be needed to further assess the impact of income.
5. Conclusion
Although the preferences of individual veterinarians matter for the overall health of the profession, community variables had a mixed effect on clinic closure in our evaluation. Mixed-and small-animal clinics had a decreased probability of closure when compared to large-animal practices, as well as clinics with larger staff numbers. These findings point more toward clinic business practices as important factors in clinic closure. Dodge et al. (Reference Dodge, Koontz and Hadrich2019) found that debt management was found to be a limiting factor in financial success for companion and mixed-animal practices. Further pointing to the need for more business analysis for future researchers, as well as business education for veterinary practice owners.
Despite childcare being a topic of discussion in the profession, childcare was not a statistically significant indicator of veterinary closure. Although lack of childcare may result in individual veterinarians leaving the area, perhaps these clinics were able to find other veterinarians to continue the practice. Alternatively, clinics who face these challenges may be finding creative solutions to retain veterinarians facing childcare constraints. Either way, continued discussions and solutions are needed to address this issue that, although lack of childcare may not be resulting in closures, is still harming the profession’s moral.
Overall, our results do not point toward any one solution for communities who are trying to support a veterinary clinic. Proximity to nearby shopping did decrease closure rates, so supporting businesses in general is likely to support veterinary clinics. Further qualitative research and financial analysis would help further explain why some veterinary clinics are successful and others are not.
Data availability statement
Upon request.
Acknowledgements
We would like to thank Bailey Cope and Jordyn Bertrem for their assistance in data verification.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors. Conceptualization, CB, AV, RB; Methodology, CB, AV; Formal Analysis, AV; Data Curation, CB, AV; Writing – Original Draft, CB, AV, RB, Writing – Review and Editing, CB, AV, RB; Supervision, CB, AV.
Competing interests
The authors declare none.
Appendix
Survival robustness: Cox hazard ratios
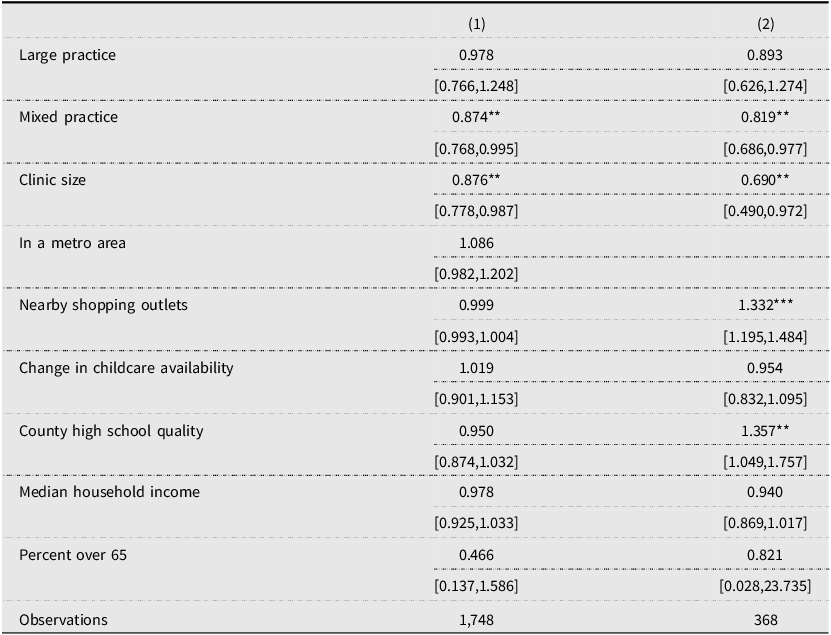
Table A Long description
The table presents hazard ratios for different factors affecting practice closure, with two columns labeled (1) and (2). Each row lists a factor such as practice type, clinic size, metro area status, nearby shopping outlets, change in childcare availability, county high school quality, median household income, and percent over 65. The table includes hazard ratios and confidence intervals for each factor. For example, the hazard ratio for large practice in column (1) is 0.978 with a confidence interval of [0.766, 1.248], and in column (2) it is 0.893 with a confidence interval of [0.626, 1.274]. The table has 1,748 observations in column (1) and 368 observations in column (2).


 Open access
Open access