


Introduction
Globally, as well as in Norway, parents of children with CHD report higher levels of anxiety, depression, and other psychological distress compared to parents of children with other diseases. Reference Lawoko1,Reference Woolf-King, Anger, Arnold, Weiss and Teitel2 Such distress is particularly pronounced in parents of children with sustained cardiac impairment compared to parents of children with corrected defects. Reference Woolf-King, Anger, Arnold, Weiss and Teitel2–Reference Oftedal, Bekkhus, Haugen, Czajkowski and Kaasen4 Contributing factors may be attributed to frequent hospitalisations, feeding problems, medications, and constant monitoring. Reference Lumsden, Smith and Wittkowski5 At the same time, mothers of newborn infants with CHD have an increased incidence of postnatal symptoms of depression, which may potentially alter parents’ perception of the difficulty of events due to symptoms such as low energy, impaired concentration, and traumatic stress. Reference Woolf-King, Anger, Arnold, Weiss and Teitel2,Reference Oftedal, Bekkhus, Haugen, Czajkowski and Kaasen4,Reference Casaña-Granell, Lacomba-Trejo, Valero-Moreno, Prado-Gasco, Montoya-Castilla and Pérez-Marín6
The Pediatric Inventory for Parents measures parental stress related to having a child with chronic disease. Reference Braniecki, Kazak, Tercyak and Streisand7 The Pediatric Inventory for Parents was developed due to the lack of an instrument capable of measuring parents’ experiences both directly and indirectly related to their children’s health. These events encompass medical regimen demands, negotiating the healthcare environment, and illness-specific factors, such as pain, nausea, and discomfort, that may affect the family when a child is chronically ill. Reference Braniecki, Kazak, Tercyak and Streisand7
The European Neuroprotective Network strongly recommends using the Pediatric Inventory for Parents to measure disease-related stress among parents of children with CHD. Reference Lisanti, Vittner and Peterson8 It is one of the most utilised instruments for assessing parental stress and caregiver burden related to children with CHD. Reference Caris, Dempster and Wernovsky9–Reference Grootenhuis, Jantien Vrijmoet-Wiersma, Koopman, Ottenkamp and van Roozendaal16 However, psychometric properties of the Pediatric Inventory for Parents have not been tested in a sample of parents of infants with CHD. Reference Eagleson, McCombs, Gerlich, Justo, Kasparian and Bora10 Hence, the aim of the present study was to explore the psychometric and differential properties and evaluate its concurrent validity with measures of depression of mothers of infants with CHD in Norway.
Materials and methods
Setting
The Pediatric Inventory for Parents was used as an outcome measure in a controlled trial of parental psychological adaptation that compared two strategies for allocating medical information, supporting discharge preparations, and decision support. Reference Hjorth-Johansen, Børøsund and Moen17 The study was initiated at Oslo University Hospital in Norway between May 2021 and May 2023. Permission to translate was received from the developer of the original version of the Pediatric Inventory for Parents and translated into Norwegian language (Supplementary file 1).
Participants
Parents of infants with severe CHD were recruited after the initiation of initial treatment but before being transferred to their respective local hospitals for follow-up. The inclusion criteria were Norwegian-speaking parents of infants with CHD, aged less than three months, and having a gestational age at birth above 34 weeks. Data solely from the primary caregiver were analysed. In this context, the primary caregivers were mothers, as they typically take at least a six-month maternity leave in Norway.
Data collection
Outcome measures were collected digitally through mobile phones with downward scrolling.
Demographics
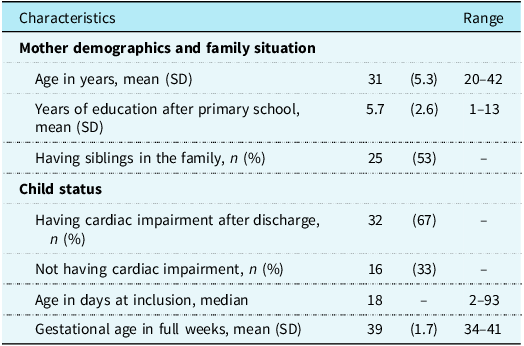
At baseline, demographic information was collected from the parents (Table 1). The first author abstracted diagnosis and treatment information from patient medical records from discharge to one month after discharge. To conduct the discriminant validity analysis, the researchers collaborated with a cardiologist to categorise the infants into two groups: (A) expected completion of treatment, or (B) still having significant cardiac impairment after discharge.
Characteristics of mothers and their infants (N = 48)

Note: SD = standard deviation.
Measures
The Pediatric Inventory for Parents
The instrument comprises 42 items organised into 4 domains: (1) communication, (2) emotional functioning, (3) medical care, and (4) role function and asks parents to indicate how often an illness-related event has occurred in the past seven days using a 5-point Likert scale (1 = “Never” to 5 = “Very often”). Reference Braniecki, Kazak, Tercyak and Streisand7 ) Parents are then asked to report how difficult the event was, also on a 5-point Likert scale (1 = “Not at all” to 5 = “Extremely”). Subscale scores reflect the frequency of stressful events and the parents’ appraisal of the difficulty associated with these events. Scores for the domains within each subscale are divided into the following ranges: 9–45, 15–75, 8–40, and 5–50. In the original version of the Pediatric Inventory for Parents, a total score for the domains in the frequency subscale is summed to present the total frequency of stressful events. The same is done in the difficulty subscale. Each of these two subscales ranges from 42 to 210. In some studies, these subscale scores are summed to represent a total stress score ranging from 84 to 420. Reference Bishop, Gise, Donati, Shneider, Aylward and Cohen11 No clinical cut-offs have been established, but higher scores are associated with higher levels of disease-related stress. The instrument showed good scale reliability (0.80 to 0.88) for the domains included in the original version. Reference Braniecki, Kazak, Tercyak and Streisand7 Validity studies have demonstrated a significant correlation between the Pediatric Inventory for Parents and state anxiety and stress Reference Braniecki, Kazak, Tercyak and Streisand7 and depression. Reference Casaña-Granell, Lacomba-Trejo, Valero-Moreno, Prado-Gasco, Montoya-Castilla and Pérez-Marín6
Edinburgh Postnatal Depression Scale
The Edinburgh Postnatal Depression Scale is a 10-item self-rating scale developed to screen for postnatal depression. Reference Cox, Holden and Sagovsky18 Each statement has four possible responses, which are scored from 0 to 3, depending on the severity of the response. Higher scores indicate more severe depressive symptoms, with a maximum total score of 30. Reference Cox, Holden and Sagovsky18 The scale has been translated into Norwegian with good scale reliability (Cronbach’s alpha 0.89) and a cut-off score for major depression of ≥12. Reference Berle, Aarre, Mykletun, Dahl and Holsten19 The scale was included in the present study to measure concurrent validity due to the expectation that increased symptoms of depression may potentially alter parents’ perception of the difficulty of their situation. Reference Oftedal, Bekkhus, Haugen, Czajkowski and Kaasen4 In the current study sample, scale reliability estimated by Cronbach’s alpha was 0.93.
Statistics
Descriptive and correlation analyses were conducted using STATA version 18 and exploratory factor analysis, and scale reliability Cronbach’s alpha Reference Cronbach20 was assessed using IBM SPSS Statistics for Windows, Release 29. Three out of 50 questionnaires from mothers had less than 5% missing data, and a mean value for the remaining items was imputed as recommended. Reference Schulz and Grimes21 In 2 out of 50 questionnaires submitted, missing values were higher, and they were thus excluded from the analyses.
Due to the modest sample size, exploratory factor analysis was not applied to the full 42-item version of the Pediatric Inventory for parents but instead to each of the four domains separately. Exploratory factor analysis was applied only to the frequency domains because parents who had not experienced an item had their related difficulty item marked as missing, thereby reducing the sample size in these analyses. We regarded factor loadings below 0.50 to be questionable and thus omitted them from substantive evaluations in the current study. Furthermore, we omitted factor loadings below 0.40 from the analyses.
The Kayser–Meyer–Olkin test of each frequency domain at one month after discharge showed between 0.60 (role functioning) and 0.75 (emotional functioning), indicating a modest to moderate amount of shared variance and suitability for exploratory factor analysis.
Data were normally distributed; hence, we employed an independent samples t-test to analyse discriminant validity between mothers of infants with corrected CHD and sustained cardiac impairment. Concurrent validity between the difficulty subscale, the frequency subscale, and the Edinburgh Postnatal Depression Scale was analysed with Pearson`s correlation.
Results
Characteristics of mothers and infants
A total of 66% (48 of 73) of the participating mothers completed the Pediatric Inventory for Parents one month after discharge (Table 1). Their mean age was 31 years (standard deviation = 5.3), and their mean education level was approximately six years (SD = 2.6) after 10 years of primary school which equals to a completed bachelor’s degree. One-third of the infants had no cardiac impairment after discharge (Table 1).
Descriptive results
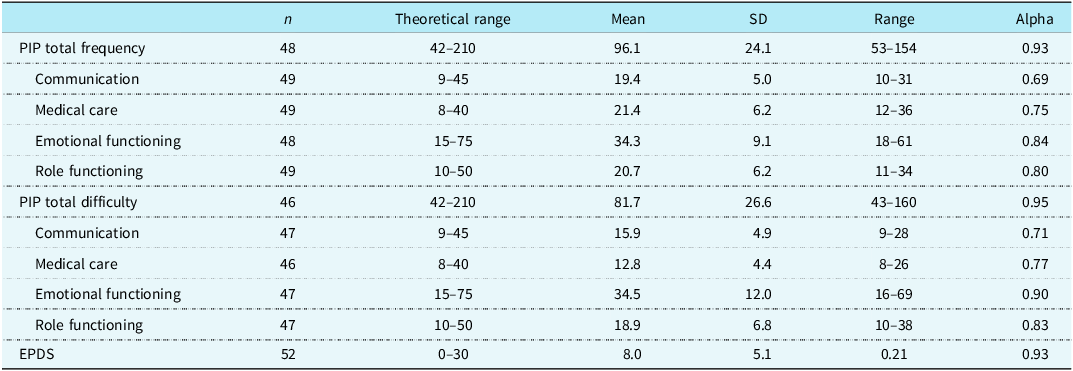
Cronbach’s alpha estimates were above 0.90 for both the frequency and difficulty total scores in Pediatric Inventory for Parents at one month after discharge (Table 2). Similarly, scale reliability was acceptable for all four domains (α =0.69 to 0.90).
Descriptive data for measures one month after discharge

Note: PIP = Pediatric Inventory for Parents. EPDS = Edinburgh Postnatal Depression Scale.
Psychometric properties of the frequency domains
Despite traditionally acceptable levels of Cronbach´s alpha as an estimate of scale reliability, the factor analysis of the different frequency domains revealed a substantial amount of multidimensionality. For the communication domain, three factors emerged: (1) differentiating between aspects of communication with doctors and nurses, (2) feelings of confusion, and (3) concerns related to family and friends. The first factor accounted for most of the shared variance (30.4%) (Table 3). Factor analysis of the emotional functioning domain revealed five factors, encompassing worries about the future, tensions related to the state of the child, concerns about the child’s pain and feelings, more generic symptoms of anxiety, and, lastly, a barely discernible factor driven by variance in thoughts related to other sick children (Table 3). Although factor analysis of the medical care domain revealed three factors, the first factor, accounting for 41% of the variance, was the most substantial, reflecting general distress related to the hospital situation. Reasonable thematic interpretations of the two subsequent factors were hard to find (Table 3). The factor analysis of the last domain, role functioning, also revealed three factors accounting for 69% of the variance (Table 3). The first factor, accounting for 34.4% of the variance, addressed concerns related to relationships with family and own needs. The second factor addressed the aspect of being away from familiar settings, while the third factor was extracted due to variance in items not related to each other (e.g., item 35: “Feeling uncertain about disciplining my child” and item 42: “Spending a great deal of time in unfamiliar settings”).
Explorative factor analysis of the Pediatric Inventory for Parents frequency domains

Note: Factor loadings from structure matrix (correlations), loadings below 0.40 omitted. KMO = Kayser–Meyer–Olkin; CI = confidence Interval.
Differential properties
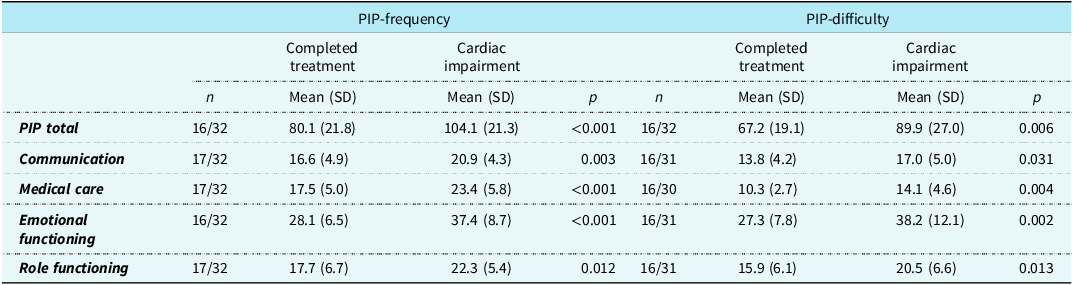
A comparison of the frequency and difficulty domains of the Pediatric Inventory for Parents between the severity groups yielded a significantly lower score among mothers of infants with completed treatment compared to mothers of infants with sustained cardiac impairment (Table 4).
The Pediatric Inventory for Parents’ scores between severity groups one month after discharge

Note: Mean values from independent samples t-test (two-tailed). PIP = Pediatric Inventory for Parents.
Relationships between Pediatric Inventory for Parents and Edinburgh Postnatal Depression Scale
In assessing parental stress for comparison with depression, both frequency and difficulty scores were used. The correlation between the total scores for the difficulty and the frequency subscale and the Edinburgh Postnatal Depression Scale was moderate (r = 0.56 and 0.63, p < 0.001). The emotional domain had the highest correlation with the Edinburgh Postnatal Depression Scale, and the frequency of medical care domain had the lowest (Supplementary file 2).
Discussion
This paper describes the psychometric properties and evaluation of the Norwegian version of the Pediatric Inventory for Parents for an infant population with CHD. Findings of the study were twofold. First, there is reason to suspect some psychometric challenges with implications for valid interpretations of the domain scores of the frequency subscale. Second, the Norwegian version was able to discriminate stress levels between mothers of infants with completed treatment and mothers of infants with sustained cardiac impairment, and the scores were significantly correlated with symptoms of depression, as expected.
Psychometric properties
The Norwegian version of the Pediatric Inventory for Parents demonstrated acceptable scale reliability within each of the four domains, as indicated by Cronbach´s alpha. Exploratory factor analysis revealed that each domain in the frequency subscale contained several sub-aspects. Although the covariance of items within the frequency domains was distributed among different factors, many items cross-loaded with several other factors within their domain. This means that the factor analysis did not disclose clear and distinct sub-aspects within the domains but rather a diversity of different themes addressed by the items within each domain.
Many studies employing the Pediatric Inventory for Parents have described the scale reliability of the frequency and difficulty total scales as excellent, with a Cronbach’s alpha above 0.90. Reference Braniecki, Kazak, Tercyak and Streisand7,Reference Khanjari, Tehrani, Panahi and Saidee22–Reference Vrijmoet-Wiersma, Hoekstra-Weebers and Margreet de Peinder24 However, Cronbach’s alpha is not applicable to multidimensional total scores and is influenced by the number of items in a scale and their average covariance. Reference Cronbach20 Therefore, it does not necessarily indicate internal consistency or one-dimensionality. Other studies have indicated that the four sub-domains of the Pediatric Inventory for Parents do not satisfy basic psychometric properties, Reference Casaña-Granell, Lacomba-Trejo, Valero-Moreno, Prado-Gasco, Montoya-Castilla and Pérez-Marín6 a claim supported by our study. At the same time, it is suggested that a one-factor model representing the total scales may be preferred. Reference Vrijmoet-Wiersma, Hoekstra-Weebers and Margreet de Peinder24
Relevance of items to the infant population
Items with a lack of relevance to infants with CHD were identified in all domains. In the communication domain, item 32, “Speaking to my child about his/her illness,” had no factor loadings above 0.3.
Within the emotional functioning domain, “Difficulty sleeping” (item 1) did not share variance with any other aspects. This might relate to feeding demands during the night in the specific infant population, rather than solely emotional distress. This may result in higher scores of emotional distress among parents of infants compared to parents of other age groups. Nevertheless, it may also reflect a more general parental experience of sleep disturbance in infancy. The second item with poor loadings was “Thoughts of other sick children” (item 31). This may reflect positive thinking, which is often used as a coping strategy in the early phase after surgery and hospital discharge among parents of infants with CHD. Reference Lumsden, Smith and Wittkowski5
In the medical care domain, the item “Making decisions about medical care or medicines” (item 18) was correlated above 0.5 with only one item. This may indicate that parents of infants with severe CHD rarely make decisions regarding treatment due to the medical complexity and vulnerability in early infancy. In addition, “Helping my child with his/her personal hygiene needs” (item 23) had a negative factor loading. This is probably due to the high frequency related to taking care of a newborn infant, such as diaper changes, in contrast to the rest of the items in this domain, which are related to medical care.
In the last domain, regarding role functioning, “Being unable to go to work/job” (Item 5) did not share variance with any items. This may be due to the 49 weeks of paid parental leave offered in Norway. In addition, “Feeling uncertain about disciplining my child” (item 35) stood out as a single factor. This finding may be attributable to the cultural context in Norway, where the prevailing approach to child-rearing places strong emphasis on positive parenting and minimal use of discipline, particularly in early childhood development. 25
Most studies of the Pediatric Inventory for Parents have thus far employed data from heterogenic patient groups with children from 0 to 18 years of age. It has been pointed out that the Pediatric Inventory for Parents may perform differently among different age groups. Reference Vrijmoet-Wiersma, Hoekstra-Weebers and Margreet de Peinder24 This is in line with our findings for the frequency subscale, which showed which items might fit poorly with the infant population. Our findings underline the need for further factor analysis among a larger group of parents to infants to define a version more appropriate for them.
One advantage of the Pediatric Inventory for Parents is that parents may choose “never experienced” and thereby eliminate some parts of the problem. But, at the same time, an item like “Difficulty sleeping” may increase the score but not necessarily correspond with increased emotional distress. In addition, the item “Helping my child with his/her personal hygiene needs” may have an opposite effect on the stress score in different age groups. Hence, when comparing results from parents of older children with parents of infants, such interpretations should be considered.
Differential and convergent properties
Although some items in the Pediatric Inventory for Parents may lack relevance for infants, it differentiated parental stress between different groups of CHD severity. A high correlation between the difficulty and the frequency of events indicates that the increased need for medical care for infants with cardiac impairment may lead to naturally increased disease-related stress. This is also in line with other studies comparing severity and stress. Reference Caris, Dempster and Wernovsky9,Reference Choi and Lee12,Reference Kaugars, Shields and Brosig14 This verifies that our translation may have a good discriminant validity for infants with CHD.
In the present study, we found that both the frequency and difficulty of stress-related events were moderately—but significantly—correlated with symptoms of depression. This indicates that the level of depression may have an impact on how disease-related events are experienced and managed, a finding corresponding with other studies of this population. Reference Oftedal, Bekkhus, Haugen, Czajkowski and Kaasen4,Reference Lefkowitz, Baxt and Evans26
Limitations
This study had several limitations. First, our study sample only included mothers of infants with CHD who were under six months of age. However, the homogeneity of participants regarding the infants’ diagnosis, age, and time since hospital admission can also be viewed as an advantage due to the findings concerning the sensitivity of the Pediatric Inventory for Parents with respect to the severity of the disease and age groups. Second, our small sample size of 48 mothers makes reliable estimates of psychometric properties uncertain. In addition, it was not possible to apply factor analysis to the total number of items. Third, in our study, the questions related to the difficulty subscale had too many missing items to apply factor analysis, as responses to the items of difficulty were marked as missing if the corresponding event was not experienced.
Despite these challenges, the domains in the frequency and difficulty effectively discriminated between CHD severity groups and were moderately correlated with depression.
Implications for practice
The current evaluation of the Norwegian version of the Pediatric Inventory for Parents for mothers of infants with CHD indicates that several items may lack relevance for infants. In addition, each domain in the frequency subscale encompasses multiple aspects. The Norwegian version of the Pediatric Inventory for Parents could be a valuable instrument for assessing parental stress in mothers of infants with CHD in clinical practice. However, for research purposes, it is important to recognize that the domains of the frequency subscale are not unidimensional. Further validation and psychometric assessment in larger populations of parents of infants would be beneficial for further defining an instrument specifically adapted to infants. If the original version is used in mixed populations, lack of relevance of some items to infants should be accounted for.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951126113791.
Acknowledgements
The authors thank all participating parents as well as Eli Våbenø, Henrik Holmstrøm, Britt Fredriksen, and Kristine Hjorth-Gulbrandsen for important contributions during translation (Supplementary file 1).
Financial support
This work was partly supported by the Research Foundation of the Norwegian Association for Children with Congenital Heart Disease (grant number 119).
Competing interests
The authors declare none.
Ethical standard
The study was approved by the Regional Committee for Medical and Health Research Ethics, Southeast, Norway (2019/1271), and the Hospital’s Privacy Protection and Data Security Committee (19/23041). The controlled trial was registered in ClinicalTrials.gov (NCT04315610). Both parents of each child provided written, informed consent.




 Open access
Open access