


Introduction
Case example
A 25-year-old woman, Cassandra, is a second-generation immigrant from Haiti. Her general practitioner referred her to a psychologist after she reported complaints of feeling anxious, restless, and having difficulty concentrating. As the clinician attempts to build rapport by engaging in small talk, Cassandra informs her that she holds a university degree and currently works in the field of law for a large corporation. As Cassandra is speaking, she notices her clinician’s eyes widening. Seemingly surprised, the therapist exclaims, ‘Wow! You are so smart and well-spoken, even though you have immigrant parents’. Although Cassandra knows the clinician meant it as a compliment, her reaction implies that she did not expect her Black client to be a successful individual, and did not expect her to be able to engage in intelligent conversation.
The psychologist treating Cassandra has perpetrated a microaggression in session. The clinician, who is a White woman, assumes that Black people are not usually well-spoken and well-employed. This assumption also implies that the clinician believes racialized individuals are unlikely to succeed in comparison with their White counterparts. While a shocked facial expression and statements like ‘Wow! You are so smart and well-spoken’ may seem innocuous, it may emotionally and mentally trigger racially minoritized individuals. Consequently, it could negatively affect the therapeutic relationship. Notably, during therapy, Cassandra kept her guard up and did not share much because she feared being judged by her psychologist. She felt like she had to subscribe to the psychologist’s cultural norms and expectations to be accepted (Williams, Reference Williams2024; Williams et al., Reference Williams, Cenat, Caldwell, Osman, Gallo and Faber2024).
In the following sections, we provide Therapist Takeaways derived from our clinical expertise and the current literature. As this paper explores these takeaways, we encourage the reader to consider the function and maintaining contingencies of their behaviour. How might one’s own learned history contribute to the enactment and maintenance of microaggressions? While much of this paper’s focus is on racial microaggressions, microaggressions of all kinds may undermine the effectiveness of our therapeutic process and rapport. In this way, developing an understanding of microaggressions is an exercise in developing therapeutic tact rooted in principles of behaviourism.
Overview
Chester Pierce described microaggressions as ‘subtle and stunning’ daily racial offences and suggested therapeutic processes to address the detrimental effects that these acts had on the health and well-being of Black Americans (Pierce, Reference Pierce and Barbour1970). Pierce’s seminal description of the construct laid the foundation for Sue and colleagues (Reference Sue, Capodilupo, Torino, Bucceri, Holder, Nadal and Esquilin2007), who described racial microaggressions as ‘brief, everyday exchanges that send denigrating messages to people of colour because they belong to a racial minority group’ (Sue et al., Reference Sue, Capodilupo, Torino, Bucceri, Holder, Nadal and Esquilin2007; p. 273). Spanierman and colleagues (Reference Spanierman, Clark and Kim2021) classify microaggressions into four major categories: (a) pathologizing differences, (b) denigrating and pigeonholing, (c) excluding and rendering invisible, and (d) perpetuating colourblind attitudes, i.e., pretending differences do not exist; these also match empirical findings from those committing such behaviours (Kanter et al., Reference Kanter, Williams, Kuczynski, Corey, Parigoris, Carey, Manbeck, Wallace and Rosen2020b).
Since Sue and colleagues’ (Reference Sue, Capodilupo, Torino, Bucceri, Holder, Nadal and Esquilin2007) paper, additional types of microaggressions have been described across a spectrum of marginalized identities, such as those impacting sexual and gender minorities, sexist microaggressions, religious microaggressions, ableist microaggressions, and many others (e.g., Nadal et al., Reference Nadal, Whitman, Davis, Erazo and Davidoff2016).
While many explicit forms of discrimination are well established within academic literature (i.e., well-defined, recognized, and correlated), more implicit forms of discrimination such as microaggressions are less understood and often face harsh and unsubstantiated critiques. One such example, and in part, the inspiration for this paper, is the recent comments and critiques of Williams and colleagues (Reference Williams, Faber and Duniya2022), who pointed out that minimizing the concept of racial microaggressions only perpetuates racism in psychology. Although the primary aim of this paper is not to directly respond to such critiques (some of which will be specified later), this paper calls attention to common misconceptions about microaggressions, and provides the most recent scientific evidence to illustrate the occurrence, implications, clinical missteps, and reality behind these misconceptions. Moreover, the authors recognize that this paper does not cover all types of microaggressions, and most of this paper’s examples reflect racial microaggressions. This focus is reflective of our experience, expertise, and the literature. That said, the authors encourage readers to consider the wider applicability of this paper’s insights for microaggressions across the spectrum of marginalized identities. Finally, we clarify that such research is not an attempt to villainize those who have committed microaggressions, a common misconception in itself (e.g., Haidt, Reference Haidt2017), but an effort to enact change by deepening the understanding of how, when, and to what effect microaggressions are perpetuated, sustained, and harmful to clients who are part of marginalized communities.
Bias and prejudice are embedded in health policies and medical practices and often do permeate interactions with providers. Clinicians may hold false beliefs about people with marginalized identities and thereby unwittingly create an unwelcoming environment for these clients. Racial microaggressions, for example, can help explain patterns of under-utilization and premature termination among clients of colour (Anderson et al., Reference Anderson, Lett, Asabor, Hernandez, Nguemeni Tiako, Johnson, Montenegro, Rizzo, Latimore, Nunez-Smith and Boatright2022; Sue and Spanierman, Reference Sue and Spanierman2020; Williams, Reference Williams2020c). Notably, a recent study of Black Canadians found that over half (53.1%) reported having been treated unfairly when receiving care in a health care setting (Cénat et al., Reference Cénat, Hajizadeh, Dalexis, Ndengeyingoma, Guerrier and Kogan2022). This paper supports clinicians by offering accurate information so that they may skilfully and empathetically help clients experiencing microaggressions, and no longer accept microaggressions as a harmless, misunderstood, or dismissed phenomenon.
History of microaggressions
As briefly discussed, microaggressions scholarship has its roots in the early conceptual work of Chester Pierce. Pierce (Reference Pierce and Barbour1970) was the first to classify these subtle, everyday slights as offensive mechanisms – now known as microaggressions. Pierce’s work identified instances of microaggression and discussed their role in perpetuating racism, later inspiring exploration into concepts such as everyday racism and racial health disparities. Around the same time, Philomena Essed’s studies of ‘everyday racism’ provided a closely related framework illustrating how routine or mundane discriminatory acts accumulate to create hostile environments for marginalized individuals (Essed, Reference Essed1991). In the field of public health, David R. Williams advanced the study of subtle bias by developing the Everyday Discrimination Scale, a measure used to understand the health implications of microaggressions (Williams et al., Reference Williams, Yu, Jackson and Anderson1997). Building on these foundations, Daniel Solórzano integrated Critical Race Theory into microaggressions research in educational settings, focusing on how racial microaggressions affect the experiences and outcomes of students of colour (Solórzano, Reference Solórzano1998).
The concept gained broader visibility after Derald Wing Sue and his colleagues (Reference Sue, Capodilupo, Torino, Bucceri, Holder, Nadal and Esquilin2007) explicitly popularized the term ‘microaggressions’ in an American Psychologist article. Subsequent scholarship has since expanded both the theoretical and empirical understanding of microaggressions. For example, Nadal (Reference Nadal2011) explored how microaggressions affect sexual minorities and other marginalized communities, devising robust measurement tools to examine their mental health consequences (Nadal, Reference Nadal2011; Nadal, Reference Nadal2019). Similarly, Comas-Díaz (Reference Comas-Díaz, Alvarez, Liang and Neville2016) underscored the clinical relevance of microaggressions for people of colour (POC), emphasizing race-informed therapeutic approaches. More recent research by McGee (Reference McGee2016) has linked microaggressions to educational disparities, especially in science, technology, engineering, and mathematics (STEM) fields, and M. T. Williams has demonstrated the health-related impacts of racial microaggressions (e.g., Williams et al., Reference Williams, Kanter and Ching2018) and conducted pivotal work on the construct validity of the concept (Williams, Reference Williams2020b).
Terminology
In recent years, the term ‘microaggression’ has faced criticism founded primarily on the following misconceptions: (1) the term microaggression mischaracterized offenders as committing an aggressive act, and (2) microaggressions are not always ‘micro’. The first claim against its terminology is based upon the assumption that the perpetrators of racial microaggressions are presumed to be hostile and aggressive. However, this perspective centres Whiteness and perpetuates systemic oppression by neglecting the empirical evidence that microaggressions reflect aggressive tendencies (Botor and Tuliao, Reference Botor and Tuliao2024; Michaels et al., Reference Michaels, Gallagher, Crawford, Kanter and Williams2018; Williams, Reference Williams2021a), regardless of the perpetrator’s intent (Rini, Reference Rini2018). While the first claim is inaccurate, the latter is true. The term being composed of micro rather than macro, highlights the subtlety of the assault itself, allowing the aggression to be challenged, disregarded, and overlooked (Smith and Griffiths, Reference Smith and Griffiths2022). In an inconspicuous manner, this term emphasizes how these actions, independently and cumulatively, are a tool for reinforcing disparities in status and power (Harrell, Reference Harrell2000; Jones et al., Reference Jones, Peddie, Gilrane, King and Gray2016).
Understanding microaggressions through cognitive behavioural therapy principles
Williams (Reference Williams2021a) conceptualises microaggressive behaviours as responses to internal and external cues associated with prejudice and oppression that function to maintain unjust societal hierarchies (Williams, Reference Williams2020a; Williams, Reference Williams2020b). A cognitive behavioural account, derived from learning theory, helps to clarify how these behaviours develop and persist.
For instance, stereotypes reflect an over-generalization and bias towards a social group or identity (Sadavoy, Reference Sadavoy, Sadavoy and Zube2021). Prejudice (i.e., negative attitudes and hostility towards a group) arises from these stereotypes and is shaped and maintained through direct contingencies (i.e., respondent and operant learning histories) and verbally governed behaviour (Goodwyn, Reference Goodwyn, Sadavoy and Zube2022). Stereotypes are also legitimizing misconceptions that reinforce existing power structures which underlie microaggressive acts (Sidanius et al., Reference Sidanius, Pratto and Devereux1992; Williams et al., Reference Williams, Gooden, Davis, Hayes and Bryant2012). Oppression, more broadly, has been described as emerging from similar processes like respondent and operant contingencies, stimulus generalization, and derived relational responding (Critchfield et al., Reference Critchfield, Barnes-Holmes and Dougher2018; Matsuda et al., Reference Matsuda, Garcia, Catagnus and Brandt2020).
Microaggressions can be communicated through verbal and non-verbal behaviours that communicate derogatory or negative identity-related slights, whether intentional or not (Sue and Spanierman, Reference Sue and Spanierman2020). They can manifest in various ways, ranging from neutral, negative, and positive statements about entire populations (e.g., gay men are sexual predators or have a talent for fashion) to subtle behaviours, such as clutching one’s purse when a Black person walks by, reflecting underlying biases. Other forms of microaggressions may include inaction (e.g., not speaking up when witnessing racial slurs made towards a person of colour, due to anxiety because it is ‘not their place’ to act), being unseen (e.g., the absence of disabled people in leading roles in movies or advertisements), and environmental assaults (e.g., public spaces that feature predominantly heteronormative couples) (Williams, Reference Williams2020b). Moreover, unique examples of microaggressions can occur in a therapeutic setting from therapist to client (e.g., ‘dressing down rank’ being when a therapist changes their appearance and behaviour, assuming it will help build rapport easier), and from client to therapist (e.g., a White client questioning a Black therapist’s education, training and experience; Bergkamp et al., Reference Bergkamp, Sloan, Krizizke, Lash, Trantel, Vaught, Fulmer, Waite, Martin, Scheiderer and Olson2023).
From a behavioural analytic perspective, microaggressions can be conceptualised as socially and culturally reinforced operant behaviours. Oppressive and prejudice behaviours may be shaped and maintained through direct contingencies (i.e., respondent and operant learning histories) and verbally governed rules (Goodwyn, Reference Goodwyn, Sadavoy and Zube2022). Matsuda and colleagues (Reference Matsuda, Garcia, Catagnus and Brandt2020) describe the emergence of oppressive behaviours through these contingencies and processes of stimulus generalization, and they outline alternative behavioural perspectives by connecting derived relational responding to the development of prejudice (see also Critchfield et al., Reference Critchfield, Barnes-Holmes and Dougher2018). In terms of microaggressions, these learned histories help explain when and why these behaviours occur. Williams (Reference Williams2021a) conceptualises microaggressive behaviours as responses to internal and external cues associated with prejudice and oppression, suggesting that microaggressions function to maintain unjust societal hierarchies (Williams, Reference Williams2020a; Williams, Reference Williams2020b). Consider how the examples provided above may serve to reinforce or punish microaggressions. Because of the deniable nature of racial microaggressions, they are sometimes minimized as simple cultural missteps or racial faux pas. Microaggressions, however, are not innocuous errors; rather, they reinforce pathological (false) stereotypes, discriminatory and exclusionary social norms, or communicate inferiority towards marginalized groups, regardless of whether this was the conscious intention of the offender (Osman et al., Reference Osman, Williams and Alftieh2024; Williams, Reference Williams2020a; Williams, Reference Williams2020b). These stereotypes reflect legitimizing misconceptions that reinforce existing power structures and underlie microaggressive acts (Sidanius et al., Reference Sidanius, Pratto and Devereux1992; Williams et al., Reference Williams, Gooden, Davis, Hayes and Bryant2012). This reinforcement of a power differential contributes heavily to the maintenance of microaggressions because it favours the in-group, and, in an effort to retain the extant power structure, socially punishes victims and observers when they challenge microaggressions.
Given their various manifestations, it is important to identify who primarily commits microaggressions. Microaggressions primarily occur from an offender, those possessing social privilege, to a target, those lacking the relevant social privilege (Bergkamp et al., Reference Bergkamp, Martin, Olson, Chin, Garcia and Blume2022a). Notably, the classification of directionality here avoids the commonplace classification based on identity labels (e.g., race, sexual orientation, etc). While these commonplace classifications may be contextually accurate, broadly speaking, classifying directionality in such a way is inaccurate as power and privilege are socially ascribed by historically dominant social groups (Bergkamp et al., Reference Bergkamp, Martin, Olson, Chin, Garcia and Blume2022a; Smedley and Smedley, Reference Smedley and Smedley2005).
Many perpetrators of microaggressions remain unaware of the subtle prejudice and resulting harm in their words and actions. It is therefore natural to question, how and why are microaggressions maintained? To answer this question, clinicians can look to descriptive terms like King’s (Reference King1991) concept of dysconsciousness, or to cognitive behavioural therapy (CBT) models (see Figure 1) for insight (Williams, Reference Williams2021a). King’s (Reference King1991) concept of dysconsciousness refers to a ‘habit of mind’, or acceptance and lack of critical judgement, of the existing status quo that justifies inequity. In other words, privileged agents are socially positioned to be unaware of their prejudice because these perceptions, attitudes, assumptions, and beliefs are perceived as a product of reality. The concept of dysconsciousness calls attention to the idea that these ‘habits of mind’ frequently go unchallenged by privileged agents.
The microaggression process model.

Microaggressions explained through cognitive behavioural therapy models
CBT model explanations lend well to building on the concept of dysconsciousness, as these models suggest that microaggressions, whether unconscious or conscious, are an assertion of dominance motivated by underlying bias and fears of relinquishing control. Both the Williams (Reference Williams2021a) CBT model and Sue and Spanierman (Reference Sue and Spanierman2020) propose that microaggressions stem from early socialization processes, beginning in childhood and persisting throughout adulthood, that create pathological stereotypes through a learned norm for the dominant group (e.g., being cisgender is the natural or default and is superior). As a consequence of this socialization, individuals of the dominant group develop biases and prejudices against non-normative identities (e.g., that educating youth on non-cisgender identities is dangerous, or that being intersex is a myth). When encountering people with marginalized identities, these underlying beliefs create unaddressed emotions (i.e., fear, anxiety), leading to maladaptive problem-solving to relieve the resulting anxiety. As such, individuals may consciously or implicitly feel the need to establish control over the interaction. Aggression increases feelings of power and temporarily relieves anxiety (Green, Reference Green1986). As a result, a perpetrator may undertake subtly aggressive comments or controlling actions to reaffirm their dominant social position. While conscious intentionality may vary, the underlying motivation is to reaffirm their social standing in the face of a threat.
The microaggression process model, based on the relationships described by Williams (Reference Williams2021a), elucidates this process, outlined in Figure 1.
The Deny, Distance, or Dismantle model
The Deny, Distance, or Dismantle (DDD) model by Knowles and colleagues (Reference Knowles, Lowery, Chow and Unzueta2014) provides insight into how members of dominant groups navigate the psychological challenges of recognizing systemic privilege. According to this framework, dominant social group people may use three strategies to cope with challenges to their privileged identity: (1) deny the existence of privilege to maintain a sense of meritocracy; (2) distance themselves from the dominant identity to avoid group-based guilt; (3) actively strive to dismantle systems of privilege. From a cognitive behavioural perspective, denial and distancing behaviours function to evade internal discomfort, social consequences and maintain existing verbal frames. Denial and distancing can perpetuate insensitivity and inaction regarding inequities, while dismantling privilege aligns with social accountability and fosters meaningful change. Furthermore, the DDD model highlights how meritocratic societal beliefs (i.e., the emphasis on internal attributions for success such as hard work, good grades, etc.) are threatened by alternative explanations for status and competency (e.g., systemic racism), and thus require dominant groups to re-evaluate attributions of self-competency.
We propose that this model may provide some explanations for the occurrence, sustainment, and resistance to microaggressions. For example, a tenured professor makes a microaggressive comment to an older graduate student about their age (e.g., ‘Wow! Starting a graduate degree at 50, that is unusual, are you sure you will be able to handle the workload?’). In this instance the professor’s microaggression reflects their belief that starting an academic career later in life is a disadvantage for the student. If challenged on this assumption, the professor may deny (e.g., ‘age has nothing to do with your success, it’s all about how hard you work’), or distance themselves (e.g., ‘age does not matter in academia, I have friends who started later than most students and they are still successful’) to protect their own self-worth. As we will discuss later, understanding maladaptive coping strategies for microaggressions that perpetuate harm allows CBT clinicians to better navigate guided discovery and conceptual integration for those perpetuating and experiencing microaggressions.
A Model of Integrating Awareness of a Privileged Social Identity
The Model of Integrating Awareness of a Privileged Social Identity (Bergkamp et al., Reference Bergkamp, Olson and Martin2022b; MIAPSI) takes a developmental approach to social privilege awareness. The model includes four developmental stages: (a) Critical Exposure; (b) Identity Threat; (c) Identity Protection; and (d) Reconciliation. Critical Exposure represents an irreversible accumulation of cognitive and comparative exposures that dismantle dysconsciousness, resulting in a new-found awareness of social privilege. Identity Threat occurs because of the perceived danger of social privilege, and a Critical Exposure’s propensity to undermine key experiences and concepts that constitute identity, such as accomplishments, morals and values. Naturally, individuals therefore experience cognitive and affective dissonance towards their role in oppression and the continued desire to benefit from privilege. Identity Protection therefore arises as a consequence of the complex experience of dissonance, and perpetuates a perceived need to protect one’s identity through strategies such as defence, dilution, and empty advocacy. Finally, Reconciliation is achieved through integrating the awareness of social privilege into one’s identity. Importantly, Bergkamp and colleagues have identified three factors that facilitate a movement towards Reconciliation: (a) interpersonal safety; (b) intrapersonal safety; and (c) cognitive scaffolding. If the individual can integrate their awareness of privilege, three core experiences are involved in this reconciliation: (a) acceptance; (b) integration; and (c) agent compassion to agent advocacy. For the purposes of this paper, we have chosen to exclude the summary of these factors and experiences and instead focus our conversation on how therapists can integrate knowledge from the MIAPSI into CBT practices in our Discussion section.
Why it is important to study microaggressions
Studying microaggressions is important because these covert acts of discrimination reflect the pervasive and ubiquitous nature of discrimination in society that persist under the guise of benign interactions. Unlike overt forms of prejudice, microaggressions can be harder to recognize and address, yet they cumulatively harm the well-being, self-esteem, and mental health of those who experience them (Costa et al., Reference Costa, McDuffie, Brown, He, Ikner, Sabat and Miner2023; Williams, Reference Williams2020c). By examining microaggressions in various settings, practitioners and researchers can better understand how negative stereotypes and power imbalances coalesce to cause harm. Microaggressions are learned behaviours that may be unlearned through reflection and awareness. When committed by clinicians, microaggressions can be particularly harmful to vulnerable patients, who have shown courage seeking care. Clients with marginalized identities may find it difficult to respond to microaggressive remarks in clinical encounters due to self-doubt and power differentials (Constantine and Sue, Reference Constantine and Sue2007). These problems contribute to feelings of distance from the clinician, unwillingness to disclose sensitive information, and early termination from treatment. Thus, clients may be unable to overcome the condition for which they sought help due to undesirable clinician interactions. The degree of harm clinicians may cause in this manner is unknown and likely under-estimated (Chapman et al., Reference Chapman, Kaatz and Carnes2013; Constantine and Sue, Reference Constantine and Sue2007).
Ongoing research is needed to help to inform strategies and interventions aimed at creating bias-free environments, improving intergroup relations, and ultimately reducing the broader social inequalities that microaggressions both signal and reinforce for people with a spectrum of marginalized identities. A larger portion of research to date has focused on racial microaggressions, but we will also discuss other types of microaggression and microaggressions broadly where relevant literature exists.
Positionalities
Because an individual’s social, cultural, and personal background significantly influences their perspective and understanding of the world, positionality has become a crucial factor when publishing scholarly articles (American Psychological Association, 2023). Recognizing positionality helps promote self-awareness and ensures a more comprehensive and empathetic approach when engaging with diverse perspectives and experiences. As such, the authors provide their own positionalities with respect to this work.
The first author is a White, non-binary and gay; they are a doctoral student in Chicago; their current publications and research focus pertains to queerness, minority stress, and psychedelics. The second author is a doctoral student in clinical psychology at a university in Ontario, Canada, and a queer, Black, and Indigenous woman; she integrates an intersectional and trauma-informed approach to her clinical care and research on BIPOC mental health, racial trauma, and psychedelics. The third author is a master’s student in clinical psychology at Toronto Metropolitan University and a first-generation Syrian immigrant; his research is focused on advancing culturally aligned interventions and equitable access to mental health services using an intersectional framework. The fourth author is an adjunct professor and Black German woman, working in pharmaceutical development. The fifth author is a Chinese woman adoptee and an undergraduate student in psychology. The last author is a Canada Research Chair, a registered clinical psychologist, and an African American woman; she has published over 200 peer-reviewed articles, with a focus on trauma-related conditions and cultural differences, including articles about therapeutic best practices.
Purpose
Despite the vast research literature establishing microaggressions as a legitimate scientific construct, there remain pockets of misinformation and ignorance that continue to propagate misconceptions about this important problem. Without correct information, people with marginalized identities are harmed when their experiences of microaggressions are unseen, misunderstood, or dismissed. This is especially important in the therapeutic context, where clinicians need to be able to skilfully and empathetically assist clients in managing these stressful experiences.
Common misconceptions
Below we deconstruct the most common misconceptions about microaggressions. We begin by stating the misconception, and also describe where it originated, and why it is harmful. We then explain why people continue to believe the misconception, including the social biases that reinforce and perpetuate it. This is followed by facts and the scientific evidence debunking the misconception. Lastly, we have included a brief takeaway for therapists to consider.
The construct of microaggressions is not scientifically valid
The misconception
This misconception originated in 2017, when Scott Lilienfeld published an influential paper in an important journal that implied the construct of microaggressions was not scientifically valid, important, or useful. He wrote that the concept ‘is far too underdeveloped on the conceptual and methodological fronts to warrant real-world application’. His notions were picked up and quickly disseminated by the media, with headlines such as, ‘Don’t go for woke: microaggressions are unscientific’ and ‘Psychology Professor: little scientific evidence microaggressions are even a thing’ (e.g., Hardiman, Reference Hardiman2017; Maranto, Reference Maranto2020). Some scholars have agreed with this, for example, Haidt (Reference Haidt2017) echoed these sentiments, stating: ‘Empirical evidence supporting the utility and validity of the microaggression concept is minimal at best’. Cantu and Jussim (Reference Cantu and Jussim2021) also rallied against the construct, stating that microaggression research is not ‘rigorous science’ (p. 225). These misconceptions are problematic because those who experience microaggressions might be wrongly told that these covert slights are not real or are unscientific, thereby invalidating their experience. In a clinical setting, this misconception can permeate throughout the therapeutic journey to impact whether microaggressions are recognized, prevented, responded to, and repaired in clinical interactions.
Why do people believe this misconception? What does this imply?
It is our opinion that Lilienfeld tried to understand racial microaggressions through his own personal lens, one shaped by the racist political and scientific discourse of the times. While critique is central to academic rigor, Lilienfeld’s theories reflect a lack of critical reflection and understanding of microaggressions, as discussed in Williams (Reference Williams2020b). At the very least, and based on our past and current understanding of the literature (e.g., Nadal et al., Reference Nadal, Davidoff, Davis and Wong2015; Costa et al., Reference Costa, McDuffie, Brown, He, Ikner, Sabat and Miner2023), Lilienfeld’s critiques lack the support to justify calling for a ‘moratorium on microaggression training’ (p. 167). We believe that such critiques serve more to discredit microaggression research than to respond to the gaps in the literature. Intentional or not, these claims unjustly reinforce the deniability of microaggressions and the unscientific rhetoric that justifies racism.
The facts
Despite the immediate media attention and support for Lilienfeld (Reference Lilienfeld2017), several experts (e.g., Sue, Reference Sue2017; Williams, Reference Williams2020b) have published counter literature discrediting these claims. There is a robust body of scientific literature on ‘everyday racism’ and ‘microaggressions’ (over 15,000 scholarly publications to date). In a paper published in the same journal where Lilienfeld’s original publication appeared, Williams (Reference Williams2020b) addressed all of his arguments against the validity of the construct, which remains unopposed. Furthermore, they also debunk several false claims about microaggressions, including their scientific basis, their ability to be validly measured, and their adverse impacts on mental health. Williams (Reference Williams2021b) also guest-edited a special issue on microaggressions in that same journal which helped solidify the concept further. Many studies of microaggressions are large quantitative studies with national samples (e.g., Williams, Reference Williams2021a). Furthermore, other researchers (e.g., Hodson, Reference Hodson2021) have, and continue to, publish credible and empirically supported research that directly contradicts criticisms that microaggressions are not scientifically valid.
Therapist takeaway: When clients raise the issue of microaggressions in session, therapists can assure them this is a real issue that has been the subject of much study, and they are right to raise it as an important topic for discussion. In this case, helping the client recognize ‘jumping to conclusions’ as a type of automatic thought and engaging in hypothesis testing can be validating and helpful for targeting rule-governed behaviour associated with experiences of oppression.
There is no agreement between or within marginalized groups as to if something is actually a microaggression, which compromises its validity – it is all subjective
The misconception
There is a misperception that microaggressions are invalid because minoritized groups cannot agree between, or amongst themselves, on what is, or is not microaggressive. Lilienfeld (Reference Lilienfeld2017) stated that ‘there are no interrater reliability data on whether recipients of microaggressions agree on which individuals are engaging in subtle prejudice’ (p. 159). Other scholars have echoed these same concerns, with Cantu and Jussim (Reference Cantu and Jussim2021) arguing that there is ‘no valid basis for labelling a vast majority of alleged microaggressions as such’ (p. 225). Lilienfeld went on to claim that proponents maintain ‘microaggressions are in the eye of the beholder’ (p. 141).
Why do people believe this misconception? What does this imply?
Some have argued that microaggressions are best established by the target’s subjective feelings about an interaction. When someone commits a microaggression, those who question their culpability are often committing a second microaggression by attempting to justify or deny it (Williams et al., Reference Williams, Skinta and Martin-Willett2021b). These attempts to justify or deny culpability often come in the form of gaslighting (i.e., manipulating others into doubting their experience or reality; Johnson et al., Reference Johnson, Nadal, Sissoko and King2021). As such, people are advised not to get defensive when confronted with the possibility of having committed a microaggression so that they do not add insult to injury (Williams, Reference Williams2020a). As such, one might conclude that this means the victim is always right, and therefore can label anything a microaggression if they feel like it, which makes the concept feel too ripe for abuse by those who do not know how to tell who is correct. If microaggressions are viewed as purely an invention of a disgruntled group, they may not be considered legitimate, causing intergroup hostility. In a clinical setting this could imply microaggressions and discrimination reported by clients are not valid, thereby undermining their lived experience.
The facts
The subjective experience of a microaggression is certainly of paramount importance to a CBT clinician. Subjectivity, or how we interpret our reality, is shaped by personal experience and context; therefore, a microaggression naturally differs from person to person. Like most psychological constructs in therapy, subjectivity is the focus of inquiry rather than the determinant of validity. Even so, research shows there actually is general agreement (a significant positive correlation) between White people, Black people, other people of colour, and diversity experts as to what behaviour is racially microaggressive (Michaels et al., Reference Michaels, Gallagher, Crawford, Kanter and Williams2018; Williams et al., Reference Williams, Ching and Gallo2021a). Thus, microaggressions can be understood as objectively identifiable patterns of deniable acts of prejudice. One can recognize microaggressions by their alignment with stereotypes or their exclusionary nature.
Therapist takeaway: When discussing microaggressions with clients, therapists may feel the urge to challenge the objectivity of microaggressions. Instead, therapists can validate the client’s experience and assure them that microaggressions are real events with a measurable impact. Therapists should reflect upon any urges to question the objectivity of others’ experiences of microaggressions. For example, invalidating a microaggressive experience may reflect biased beliefs and habits of over-generalizing or magnification/minimization.
Microaggressions cannot be considered accurate based on the interpretation of the victim unless someone else (e.g., a straight, able-bodied White male) can verify it
The misconception
The following claim was first made by Lilienfeld (Reference Lilienfeld2017) whereby he stated ‘Mono-source bias, specifically the exclusive reliance on self-report in microaggression research, is a serious limitation’ (p. 158). Here Lilienfeld claims that because research on microaggressions up until that point (i.e., 2017) had relied on solely self-report methodologies, it therefore lacked critical multiplism (Shadish, Reference Shadish1993), or more specifically, multiple operationalism, an approach that operationalizes constructs (i.e., creating procedures, measures, processes) in multiple ways, theoretically allowing researchers to obtain a more complete picture of the desired phenomenon (Carpentras, Reference Carpentras2024; Lilienfeld, Reference Lilienfeld2017). The lack of methodological diversity, and presence of mono-source bias, according to Lilienfeld (Reference Lilienfeld2017), therefore ‘renders it difficult or impossible to evaluate the extent to which MRP [the microaggression research program] findings are robust across different informants’ (p. 152). Critiquing the construct validity of microaggressions on such grounds perpetuates the idea that marginalized victims provide unreliable reports of their experiences.
Why do people believe this misconception? What does this imply?
The idea that microaggressions cannot be considered valid based solely on the report of the individual experiencing them reflects a broader scepticism toward marginalized perspectives rather than a genuine need for more rigorous methodologies. Psychological constructs such as self-esteem have long been developed using self-report measures alone (Akagi and Gooding, Reference Akagi and Gooding2021; Rosenberg, Reference Rosenberg1965), yet similar standards are not always applied when assessing the experiences of marginalized groups. Some critiques argue that research on microaggressions relies on ‘highly selected samples’ and advocate for the inclusion of those who commit microaggressions in such studies (Lilienfeld, Reference Lilienfeld2017; p. 149). This perspective carries significant implications: it reinforces the idea that individuals from marginalized groups cannot be trusted to reliably identify their own experiences of discrimination unless validated by others – typically those who hold more social power. As a result, the burden of proof shifts away from the people most affected and towards those least likely to recognize the impact of microaggressions, further entrenching doubt and disbelief in the experiences of minoritized groups.
The facts
The assertion that microaggressions cannot be accurately or comprehensively studied using self-reports from victims is inaccurate (Williams, Reference Williams2020b). There are several validated self-report measures of microaggressions with good psychometric properties, that are used frequently (Osman et al., Reference Osman, Williams and Alftieh2024), including the Racial Microaggressions Scale (RMS; Torres-Harding et al., Reference Torres-Harding, Andrade and Romero Diaz2012) and the Racial and Ethnic Microaggressions Scale (REMS; Nadal, Reference Nadal2011), the Gender Identity and Expression Microaggressions in Therapy Scale (GIEMTS; Velez et al., Reference Velez, Scheer, Adames, Cavic and Breslow2024), the Sexual Orientation Microaggressions Scale (SOMS; Nadal, Reference Nadal2019), and the Ableist Microaggressions Scale (Conover et al., Reference Conover, Israel and Nylund-Gibson2017). However, both potential perpetrators and targets can accurately appraise microaggressions and censor their language when presented with vignettes of ableist and racist microaggressions, and most people agree on what constitutes a microaggression (Conover et al., Reference Conover, Acosta and Bokoch2021; Michaels et al., Reference Michaels, Gallagher, Crawford, Kanter and Williams2018; Williams, Reference Williams2020b). Furthermore, racialized, queer, and persons with disabilities understand their respective forms of prejudice better than their non-marginalized counterparts (Banaji et al., Reference Banaji, Fiske and Massey2021; Conover et al., Reference Conover, Acosta and Bokoch2021). Therefore, advocating for the inclusion of non-minoritized perspectives to ‘increase construct validity’ is unnecessary and biased. In fact, the drive to do so can be easily conceptualised as a means of identity protection (e.g., denial and gaslighting) as explained through the MIAPSI (Bergkamp et al., Reference Bergkamp, Olson and Martin2022b). It is much easier for offenders to soothe dissonance by countering and trivializing the target’s experience, than to confront said dissonance. What extra insight do these non-minoritized groups add to confirming or denying the existence of microaggressions?
Therapist takeaway: Trust your clients’ reports of microaggressions as valid expressions of their lived experience – minimizing or requiring external ‘verification’ reinforces systemic invalidation. Requiring external verification for any form of harm is inconsistent with clinical best practice. Empirical research supports the reliability of self-reports among marginalized groups, who often have deeper insight into the dynamics of discrimination than their non-marginalized counterparts.
Microaggressions are simply a product of Critical Race Theory
The misconception
A common misconception is that microaggressions are purely a product of Critical Race Theory (CRT) and that they lack empirical grounding or historical development independent of CRT. Reducing microaggressions to a ‘CRT creation’ misses both the broader scholarly lineage and the robust body of interdisciplinary empirical evidence supporting the validity and impact of this slippery form of discrimination. Moreover, co-opting terms to fit oppressive narratives is not unique to CRT. Terms such as using neurotic to describe LGBTQ+ people, ‘my body, my choice’ to justify anti-masking, or more recently using DEI (diversity, equity and inclusion) as a catch-all pejorative for ‘wokeness’. As a result, when people try to discuss the problem of microaggressions their concerns may be (mis)branded as poorly understood CRT and villainized.
Why do people believe this misconception? What does this imply?
There is a belief that microaggression science reinforces a CRT narrative about social reality, which concerns CRT opponents in a context where CRT has become increasingly maligned and politicized. Perceived as an erroneous and dangerous framework, in the United States bills were introduced in several Republican-controlled legislatures to restrict teaching about CRT. Opponents of racism education misrepresent CRT as advancing notions such as that all White people are ‘instinctively White supremacists’ and ‘oppressors’ (e.g., Thiessen, Reference Thiessen2021). In September 2020, conservative lawmakers and activists started using the term CRT as ‘a catchall phrase for nearly any examination of systemic racism’, which problematically conflates these conceptually distinct constructs. Notably, Solórzano (Reference Solórzano1998) and colleagues (Solórzano et al., Reference Solórzano, Ceja and Yosso2000, Reference Solórzano, Pérez Huber and Huber-Verjan2020) wrote a number of papers using CRT to help understand and explain the concept of racial microaggressions, which may also have played a role in tying these concepts together. Negative public reactions to CRT often result in the important concept of microaggressions being a secondary casualty.
The facts
CRT is not a ‘movement’, nor does it make policy prescriptions; rather, it is a way of looking at the world whereby racism and disparate racial outcomes are the result of complex and often subtle social and institutional forces, rather than intentional malice by individuals. The concept of microaggressions did not evolve out of CRT: microaggressions were coined before 1970, whereas CRT did not start to form until the mid-1970s (e.g., Solórzano et al., Reference Solórzano, Ceja and Yosso2000). However, microaggressions can help explain the mechanisms by which social systems uphold disparities, although an important distinction involves them occurring at an individual level.
Therapist takeaway: Therapists should understand that microaggressions are not political rhetoric or ideological products of CRT – they are empirically documented experiences with real psychological consequences. Dismissing them as CRT-related undermines clients’ valid concerns and risks empathic failure. Co-opting terminology like ‘CRT’ may be a cue for therapists to reflect on the learned associations clients and themselves have made to these terms.
People of colour complain about microaggressions because they are high in negative emotionality/affectivity (e.g., neurotic)
The misconception
The myth that people of colour complain about microaggressions because they are neurotic perpetuates stereotypes about emotional instability based on race. This misconception assumes that people of colour are inherently prone to negative emotionality or over-reaction, disregarding the real social and psychological impacts of experiencing discrimination. Research on race-based rejection sensitivity (RBRS) reveals that individuals who are sensitive to racial rejection are more likely to perceive racism and negativity, even in ambiguous situations (Lilienfeld, Reference Lilienfeld2017).
Why do people believe this misconception? What does this imply?
This misconception often stems from historical biases that associate people of colour with emotional or psychological vulnerability, overshadowing the real socio-cultural factors contributing to their emotional responses. Historically, people of colour have been unjustly associated with being emotional unstable and overly sensitive (e.g., African Americans are often stereotyped as intellectually inferior or angry) (Steele and Aronson, Reference Steele and Aronson1995). This aligns with the idea that their complaints about microaggressions are simply a result of heightened emotionality or neuroticism, not deserving of any special consideration or empathy. In the clinical setting, when therapists endorse their own values and cultural worldview while devaluing and pathologizing the cultural values of their marginalized client, this can make clients feel unsafe in therapy. This could be a therapist rushing a client through a difficult race-based experience, saying ‘I’m really sorry you experienced that, let’s discuss it when we meet again’, then proceeding to discharge the client without notice. These interactions disregard the psychological impact of the client’s race-based experiences and imply clients of colour are undeserving.
The facts
By labelling the emotional responses of people of colour to microaggressions as neurotic, the misconception dismisses the legitimate nature of their experiences. This frames their reactions as personal flaws rather than valid responses to systemic bias and marginalization. Research on race-based rejection sensitivity fails to consider the broader context of marginalization that people of colour face regularly. Moreover, people of colour are often reluctant to speak up about microaggressions due to the risk of being labelled as ‘neurotic’ (Lilienfeld, Reference Lilienfeld2017), as the misconception suggests (Williams, Reference Williams2020b). The idea that they complain about microaggressions because they are high in negative emotionality is false, as research demonstrates that microaggressions do, in fact, have negative mental health consequences (Costa et al., Reference Costa, McDuffie, Brown, He, Ikner, Sabat and Miner2023; Williams, Reference Williams2020b). These emotional responses should be considered legitimate reactions to ongoing systemic bias, rather than a reflection of inherent neuroticism. Furthermore, one study investigating this issue found that it was White people who scored higher on measures of negative affectivity, not people of colour (Williams et al., Reference Williams, Kanter and Ching2018).
Therapist takeaway: Do not pathologize clients of colour for expressing distress about microaggressions – these emotional responses are valid reactions to real experiences of marginalization, not signs of neuroticism. Assuming otherwise perpetuates racial stereotypes and undermines trust in the therapeutic relationship. Culturally competent care requires honouring the emotional truth of clients’ racialized experiences and responding with empathy, not dismissal.
Experiencing microaggressions is not harmful because they are small and subtle
The misconception
The belief that microaggressions are not harmful often stems from their subtle nature, leading many to dismiss them as insignificant. Because microaggressions are perceived as minor, some argue that any harm associated with them must be caused by other factors, rather than the microaggressions themselves. Critics have pointed out that much of the existing research establishes correlations rather than direct causation, leading to scepticism about whether microaggressions are a definitive cause of negative mental and physical health outcomes. However, these arguments downplay the impact of microaggressions by shifting the focus away from their harm and attributing negative effects to other unidentified variables. This line of reasoning ultimately minimizes the lived experiences of those affected, reinforcing the notion that microaggressions are too minor to warrant concern.
Why do people believe this? What does this imply?
Microaggressions are often ambiguous, which can make it challenging to determine whether they have occurred (Lilienfeld, Reference Lilienfeld2017). As a result, identifying microaggressions becomes difficult, especially when alternative explanations seem plausible (Sue et al., Reference Sue, Capodilupo, Torino, Bucceri, Holder, Nadal and Esquilin2007). For those of the dominant social group, this can be especially difficult as recognizing microaggressions may elicit fears of realizing one’s complicity in oppression (Constantine and Sue, Reference Constantine and Sue2007). These fears and lack of first-hand experience of microaggressions make it difficult to grasp how these seemingly minor slights accumulate and lead to significant distress. Furthermore, individuals from the dominant social group may struggle to identify and understand microaggressions, as they are often unaware of how their identity represents the social ideal or norm. As such, they may not recognize these microaggressions as prejudicial, or see the need to identify them, as their personal safety and well-being are not threatened by microaggressions (Williams, Reference Williams2020b). Therapists can minimize microaggressions and endorse stereotypes of people from a given country, a homogenous group, by saying, ‘I have an immigrant friend, they’ve taught me about your culture and lived experience’. Statements such as this might appear too minor for a therapist to warrant concern; however, they minimize the lived experiences of newcomers.
The facts
Research has consistently shown that microaggressions are associated with many adverse mental health consequences, including stress, anxiety, depression, symptoms of post-traumatic stress disorder, low self-esteem, obsessive-compulsive disorder, substance use, alcohol abuse, severe psychological distress, reduced self-efficacy, and suicide (Williams, Reference Williams2020b). This includes not just correlational studies but prospective studies as well (Williams, Reference Williams2020c). Furthermore, a meta-analysis by Costa and colleagues (Reference Costa, McDuffie, Brown, He, Ikner, Sabat and Miner2023) shows that microaggressions are generally detrimental to individuals. Specifically, the analysis revealed that experiences of microaggressions predicted a decrease in psychological well-being, physical health and job outcomes.
Therapist takeaway: Despite their seemingly subtle nature, microaggressions leave lasting impressions and should not be dismissed or minimized. What may seem subtle or insignificant to one person can be deeply invalidating or even retraumatizing to a client. Therapists must recognize and address microaggressions as legitimate sources of distress, not just incidental remarks to be overlooked.
Microaggressions are not aggressive because they are largely unintentional
The misconception
Some have argued that microaggressions cannot be considered aggressive unless there is clear intent behind them, suggesting that there is no evidence linking microaggressions to aggression or prejudice in those who commit them (Lilienfeld, Reference Lilienfeld2017; p. 161). However, this perspective reflects a narrow understanding of the ways aggression can manifest and assumes that microaggressions are always unintentional. Such an approach dismisses the lived experiences of those who experience microaggressions, reinforcing dominant definitions of aggression while overlooking the perspectives of those directly affected.
Why do people believe this? What does this imply?
Many believe that microaggressions do not qualify as aggression because aggression is often defined as an intentional act meant to cause harm to someone who does not wish to be harmed (Allen and Anderson, Reference Allen, Anderson and Sturmey2017). This definition implies that aggression must be both deliberate and malicious. As microaggressions are typically described as subtle and unintentional, some argue that there is no clear link between microaggressions and aggression (Lilienfeld, Reference Lilienfeld2017). Additionally, the narrow definition of aggression often leads to confusion between aggression and overt violence. Bushman and Huesmann (Reference Bushman, Huesmann, Fiske, Gilbert and Lindzey2010) define violence as an act that results in extreme physical harm, categorizing violence as a subset of aggression (Allen and Anderson, Reference Allen, Anderson and Sturmey2017). Because violence represents only a small category of aggressive behaviours, the two concepts are not synonymous. This conflation of aggression with violence reinforces the perception that microaggressions cannot be considered aggressive simply because they do not typically involve physical harm.
The facts
While some scholars argue that microaggressions are not a form of aggression due to the absence of malicious intent, the assumption that microaggressions are always unintentional is not true. Microaggressions, although subtle, are a form of biased-motivated behaviour (Botor et al., Reference Botor, Tuliao, Felipe, Awua and Babcock2024). Research indicates that racism involves a range of multi-faceted behaviours enacted by the dominant group and imposed on subordinate groups (Williams, Reference Williams2020b). As microaggressions are a form of racism, this tells us that they are not isolated events but rather reflect an underlying ideological social system which is itself a form of violence. Additionally, Williams (Reference Williams2021a) found that aggressive anger was closely linked to all four types of microaggressions: negative/hostile attitudes, colourblindness, objectifying, and avoidance. These data indicate that microaggressions are intentional acts of dominance, driven by biases, and thus constitute a distinct form of subtle relational aggression (Williams, Reference Williams2021a). Given this understanding of how microaggressions are typically manifested, assuming that they are largely unintentional may lead victims to overlook the potential aggressive tendencies of offenders.
Therapist takeaway: First and foremost, therapists should contextualize the existence of microaggressions as a form of prejudice enacted by dominant social groups and driven by underlying biases. While therapists should challenge cognitive distortions, they should be cautious not to challenge the validity of the distress felt by clients. If therapists make excuses for offenders (e.g., ‘do we really know they meant that to be hurtful?’), they may be inadvertently putting clients at risk of future acts of aggression by lowering their ability to identify realistic risk.
Microaggressions are not an indication of racism or any other form of prejudice
The misconception
The claim that ‘there is no research evidence that microaggressions correlate with indices of … prejudice in deliverers’ (Lilienfeld, Reference Lilienfeld2017) was not entirely accurate, as scholars of colour had long documented how racial microaggressions align with racial stereotypes and reflect patterns of unfair treatment. A call for quantitative research examining whether a tendency to microaggress correlates with discriminatory beliefs was reasonable at the time, as no such studies had yet been conducted. However, the assumption that no such connection would be found contradicted the perspectives of scholars who had studied these issues extensively. This scepticism overlooked decades of work detailing the links between microaggressions, implicit biases, and structural inequalities.
Why do people believe this? What does this imply?
Many who consider themselves fair and unbiased people were surprised and dismayed to learn that many common microaggressions were behaviours that they routinely engaged in (e.g., Fisher et al., Reference Fisher, Moore, Simmons and Allen2017; Michaels et al., Reference Michaels, Gallagher, Crawford, Kanter and Williams2018). Because they did not consider themselves prejudiced, they found it easier to dismiss racial microaggressions as unrelated to racism, reinforcing their belief that they were not racist. This myth excuses microaggressions by saying they are not a form of prejudice, creating a lack of accountability for perpetrators. This problem is propagated by researchers who have their own agenda and misrepresent the state of the science. For example, a recent paper by Jussim and Honeycut (Reference Jussim and Honeycutt2024) wrongly states that ‘there is no evidence … that racism causes microaggressions’.
The facts
Research has firmly linked microaggressions and prejudice. Multiple studies have found that the propensity to commit racial microaggressions (showing negative attitudes, colourblind statements, objectification, and avoidance) is correlated to many indicators of racism, including symbolic racism, colourblind racial attitudes, modern racism, and negative feelings towards people of colour (Kanter et al., Reference Kanter, Williams, Kuczynski, Manbeck, Debreaux and Rosen2017; Kanter et al., Reference Kanter, Williams, Kuczynski, Corey, Parigoris, Carey, Manbeck, Wallace and Rosen2020b; Neville et al., Reference Neville, Awad, Brooks, Flores and Bluemel2013; Williams et al., Reference Williams, Kanter, Peña, Ching and Oshin2020). In other words, people who are more racist commit more racial microaggressions. Additionally, affinity towards outgroup members (allophilia), which is negatively correlated to racism, was also negatively correlated to the tendency to commit racial microaggressions (Williams and Sharif, Reference Williams and Sharif2021). Another study found that the propensity to commit microaggressions based on sexual orientation (microinvalidations, assumption of pathology, heterosexist language, enforcement of binary gender roles) was higher among people with more negative prejudice towards lesbians and gay men (Botor et al., Reference Botor, Tuliao, Felipe, Awua and Babcock2024). As such, microaggressions are clearly a result of bias.
Therapist takeaway: Microaggressions are not simply accidental or harmless misunderstandings – they reflect underlying biases, whether conscious or not. Therapists must recognize that committing a microaggression often signals internalized prejudice, and failing to acknowledge this risks perpetuating harm in the therapeutic relationship. Awareness and accountability are essential for creating a safe, respectful space for all clients.
People of colour cannot commit racial microaggressions
The misconception
Another misconception is that people of colour (POC) cannot commit racial microaggressions and that only White people can commit racial microaggressions against POC. This misconception is based on inaccurate assumptions, being that (1) all POC experience monolithic oppression, and (2) POC are unable to commit oppression (Williams, Reference Williams2020b). Thus, this perspective does not account for the nuances of an individual’s power in society, which is based on the intersectional factors of identity (e.g., the institutional power of a Black woman in comparison with a man of colour). Misunderstanding occurs when individuals equate racial microaggressions to an action committed by solely White individuals.
Why do people believe this? What does this imply?
While some maintain the belief that only White people can commit racial microaggressions, this perspective does not recognize that White supremacy can be upheld by individuals regardless of race (Spanierman et al., Reference Spanierman, Clark and Kim2021). In other words, racial microaggressions are not a White versus BIPOC (Black, Indigenous, and people of colour) issue but rather interpersonal harm from one person (perpetrator) to a BIPOC individual (target). Racial microaggressions are just one example of the many mechanisms that uphold systemic oppression. Given that these subtle yet detrimental harms are committed repetitively, they become prevalent throughout society and normalized as an experience amongst POC. Whether conscious or unconscious, individuals internalize this oppression and can subsequently enact harm on themselves and other POC (e.g., believing negative stereotypes or derogatory statements about one’s in-group). This oppression cycle permits POC to become the perpetrator and invalidate POC experiences of racial microaggressions. Thus, POC can experience racial microaggressions from their in-group and/or the dominant group in society. In the clinical setting, therapists with a marginalized identity may reject perpetuating microaggressions about another marginalized group implying they are unable to commit oppression despite the power differentials in a therapeutic setting.
The facts
Research indicates that people of colour have experienced racial microaggressions from other POC belonging to the same and/or a different ethnic group (Williams et al., Reference Williams, Ching and Gallo2021a). In addition to internalized racism, POC have been found to commit racial microaggressions as a way to move up the social hierarchy and acquire power, even if momentarily (González Vera et al., Reference González Vera, Domenech Rodríguez, Navarro Flores, Vázquez, San Miguel, Phan, Wong, Klimczak, Bera, Papa and Estrada2024). This lateral violence contributes to the subjugation of POC without the presence of a White person. Additionally, other marginalized groups such as LGBTQ + individuals can commit within-group microaggressions towards each other, particularly towards bisexual individuals (Bostwick and Hequembourg, Reference Bostwick and Hequembourg2014). Research findings signify the need to expand on racial microaggressions literature (e.g., Kanter et al., Reference Kanter, Williams, Kuczynski, Corey, Parigoris, Carey, Manbeck, Wallace and Rosen2020b; Spanierman et al., Reference Spanierman, Clark and Kim2021) which predominantly investigates White populations as the perpetrators – without careful attention to the nuances of oppression, this trend may mislead individuals to believe that POC cannot enact such harms to themselves and other POC.
Therapist takeaway: Therapists can help clients understand that even those with the same marginalized identities can perpetrate harm due to internalized biases. People of colour can internalize and enact oppressive beliefs, including towards members of their own or other marginalized groups.
People of colour should not be educated about racial microaggressions as it will make them needlessly angry or emotional
The misconception
Some scholars have argued that framing microaggressions as a form of racism could be harmful to people of colour, as it may lead to increased anger, hostility, or psychological distress (Cantu and Jussim, Reference Cantu and Jussim2021; Haidt, Reference Haidt2017). By 2017, this scepticism intensified, with some suggesting that this framing might heighten individuals’ sensitivity to perceived slights, making them more likely to experience negative emotional reactions and view themselves as psychologically vulnerable (Lilienfeld, Reference Lilienfeld2017). Based on this reasoning, calls were made for a temporary halt on microaggression training programs and the distribution of publicly available microaggression lists commonly used in academic and corporate settings. As a result, many universities stopped providing information about microaggressions, fostering ignorance and stymieing educational efforts to reduce microaggressions (Williams, Reference Williams2020b).
Why do people believe this? What does this imply?
Stereotypes about many marginalized groups include that they are hostile or angry (e.g., Williams et al., Reference Williams, Skinta and Martin-Willett2021b). One way to turn people against each other is to instil fear in them about the malicious intentions of the other group. For example, White people know at some level that POC have been mistreated for a very long time and have fears about what POC might do when they decide enough is enough (e.g., Martin and Lakins, Reference Martin and Lakins2022). So, naturally, White people may fear that admitting to the existence of everyday, unconscious mistreatment of POC, and other identities for that matter, may make them even more angry, leading them to seek revenge. Reacting to this fear, such White people shift the blame and act as if they are doing POC a favour by protecting them. In reality, this is more indicative of White emotional fragility than that of POC. Calling for a moratorium on microaggression education because it may inadvertently hurt POC is equivalent to hiding the rules to Monopoly because you don’t want the players to argue. Denying education as a means of ‘protecting’ marginalized groups is a textbook example of oppressor groups controlling marginalized groups (Litwack, Reference Litwack1998), because keeping them ignorant makes them easier to control.
The facts
Research shows that in placebo-controlled trials educating students about racial microaggressions reduces racism and improves ethnic identity, which makes students of colour stronger not weaker, and students (both Black and White) positively rate the training experience (Williams et al., Reference Williams, Kanter, Peña, Ching and Oshin2020). Furthermore, those who have the tools to confront racism often feel a sense of increased self-efficacy (Gay et al., Reference Gay, Burnett-Bowie and Bromberg2024). The opposite is true when people lack the tools for confronting microaggressions. When POC remain silent in the face of prejudice, they often ruminate and report negative self-evaluations and a fatalistic attitude about racism (Shelton et al., Reference Shelton, Richeson, Salvatore, Hill, Levin and van Laar2006; Williams and Williams-Morris, Reference Williams and Williams-Morris2000). Lastly, microaggression education has been shown to benefit both POC and White targets, allies and by-standers (Fisher et al., Reference Fisher, Moore, Simmons and Allen2017; Sue et al., Reference Sue, Alsaidi, Awad, Glaeser, Calle and Mendez2019; Williams et al., Reference Williams, Kanter, Peña, Ching and Oshin2020). While there are several theorized benefits, a particularly relevant one is the potential for building an understanding of the differentiation between intent and harmful impact (Sue et al., Reference Sue, Alsaidi, Awad, Glaeser, Calle and Mendez2019).
Therapist takeaway: Withholding education about microaggressions out of fear will upset clients of colour, and is both patronizing and harmful. Empowering clients with knowledge about the realities of racism can enhance their self-efficacy, validate their experiences, and support healing. Therapists should trust that clients are resilient and capable of engaging critically with difficult truths – education is a tool for liberation, not a threat to emotional stability.
Clinicians should not be educated about microaggressions
The misconception
The aforementioned statement on prohibiting education on microaggressions extends to the training of clinicians. Critics have posited that such education is not necessary due to microaggressions research being unscientific (i.e., ‘lack of base rates’), inaccurate, and parallel to ‘mind reading’ (i.e., a cognitive distortion). Other scholars who also share this perspective assert that measures assessing microaggressions are fatuous and based on ‘premature conclusions’ that the alleged aggressor has intended an underlying, negative response (Cantu and Jussim, Reference Cantu and Jussim2021; Lilienfeld, Reference Lilienfeld2017). Therefore, asserting that a statement is a microaggression requires making assumptions that cannot be determined through a rigorous, scientific process. Thus, this myth focuses on an individual’s interpretation of the statement, rather than the delivery (or intent) of the message. These notions caused several clinical training programs to stop teaching therapists about microaggressions and other forms of bias.
Why do people believe this? What does this imply?
Censoring education is one of many tools for upholding systemic barriers for minoritized populations. Systemic barriers are perpetuated by implicit biases rooted in fears of dominant groups losing power (Williams, Reference Williams2020b). When implicit biases exist within systems that develop and provide education, gaps in understanding persist. In the case of clinicians, this prohibition would be unethical as this creates a gap in understanding of minoritized clients; clinicians lacking the skills to process client experiences of microaggressions would in turn exacerbate mental health disparities. The lack of education will contribute to the perpetuation of biased and insensitive beliefs and behaviours by clinicians, and the internalization of such by minoritized clinicians, promoting interpersonal conflicts between clinicians and clients (González Vera et al., Reference González Vera, Domenech Rodríguez, Navarro Flores, Vázquez, San Miguel, Phan, Wong, Klimczak, Bera, Papa and Estrada2024). Consequently, minoritized clients and clinicians are invalidated or misunderstood by not having a label or words to describe their lived experiences. This denial through lack of proper training also plays a role in diminished well-being for POC (González Vera et al., Reference González Vera, Domenech Rodríguez, Navarro Flores, Vázquez, San Miguel, Phan, Wong, Klimczak, Bera, Papa and Estrada2024) and medical racism (e.g., inaccurate diagnosis; denial of medical care; symptoms overlooked and disregarded; Hall and Fields, Reference Hall and Fields2015), creating barriers to clinical care (Walls et al., Reference Walls, Gonzalez, Gladney and Onello2015).
The facts
Clinicians should be educated about microaggressions as they can unintentionally cause harm without this knowledge. Microaggressions have a detrimental impact on those who experience them, and as clinicians are dedicated to their clients’ well-being, the last thing they would want is to cause harm by dismissing their effects (Williams, Reference Williams2020a). A study by Owen and colleagues (Reference Owen, Tao, Imel, Wampold and Rodolfa2014b), however, found that 53% of multi-ethnic clients reported experiencing racial microaggressions from their therapist. In a recent study of 288 Black, Indigenous, and women of colour clients, 89% reported experiencing racial and gender microaggressions in therapy, with therapists’ avoidance of discussing racial microaggressions being the most frequent racial microaggression experienced by clients (DeBlaere et al., Reference DeBlaere, Zelaya, Dean, Chadwick, Davis, Hook and Owen2023). Additionally, racial microaggressions negatively predicted the therapist’s cultural humility, working alliance, and positive therapy outcomes (DeBlaere et al., Reference DeBlaere, Zelaya, Dean, Chadwick, Davis, Hook and Owen2023). By understanding microaggressions, clinicians can avoid committing them, better empathize with their clients’ experiences, provide targeted support, and feel empowered to engage in psychoeducation (Comas-Díaz, Reference Comas-Díaz, Alvarez, Liang and Neville2016; Pérez Huber and Solórzano, Reference Pérez Huber and Solórzano2018). Training clinicians about microaggressions can improve clinical care, client experience, and clinician confidence (Azman et al., Reference Azman, Zhou and Shorey2023; Kanter et al., Reference Kanter, Rosen, Manbeck, Branstetter, Kuczynski, Corey, Maitland and Williams2020a).
Therapist takeaway: Clinicians must be educated about microaggressions to avoid unintentionally harming clients. To competently address the impact of subtle discrimination in therapy, clinicians must be able to recognize, educate and address microaggressions. Dismissing microaggression training undermines cultural humility, weakens the therapeutic alliance, and perpetuates mental health disparities. Ethical, effective care requires understanding how bias shows up, even unintentionally, and how to repair and respond when it does.
Microaggressions are just an American problem because people are so much more bigoted there
The misconception
Despite world-wide recognition of prejudice and an increased interest in studying its various forms, phenomena such as microaggressions are frequently viewed as an ‘American problem’ (e.g., Avery, Reference Avery2020). This misconception, in part, stems from the steadily growing number of American researchers openly discussing and publishing on the topic, as well as the newfound attention from American news outlets as contentious debates on Critical Race Theory and civil rights continue. Public incidents like the murder of George Floyd have also intensified conversations around these topics as they emerge from the American media.
Why do people believe this misconception? What does this imply?
The history and impact of racism continue to be a central issue that has been widely discussed since America’s inception. While microaggressions are not exclusive to acts of racism, they are rooted in Black American researchers’ endeavour to identify and study the subtle, everyday acts of racism experienced by Black Americans. As expected, the USA has therefore done most of the research in this area, and strong social values around freedom of speech, have allowed researchers to be more open with national problems like racism. Researchers routinely collect data on marginalized identities through governmental systems (e.g., US Census, DMV, criminal justice), health systems, and large-scale research initiatives (e.g., Project Implicit) which makes it easier to crunch the numbers and identify more subtle and nuanced forms of prejudice. At face value, the abundance of research from American scholars, and conversely the scarcity of research from international scholars, may mistakenly be viewed as an indication that microaggressions are an American issue. However, this perspective ignores the existence of such prejudice, and the cultural and societal nuances that explain what is and is not emphasized in academic research in other countries.
The facts
Microaggressions are a problem in Canada (Cénat et al., Reference Cénat, Hajizadeh, Dalexis, Ndengeyingoma, Guerrier and Kogan2022), Europe (Guardamagna et al., Reference Guardamagna, Hampton, Roccia and Sredanovic2024; Nyul et al., Reference Nyul, Kende, Pántya, Váradi, Braverman, Hushegyi and Hopkins2025), and everywhere else in the world (e.g., China: Kwok and Kwok, Reference Kwok and Kwok2022; Germany: Aikins et al., Reference Aikins, Bremberger, Aikins, Gyamerah and Yıldırım-Caliman2021; India: Bakshi, Reference Bakshi2023; Israel: Breski and Lavie-Ajayi, Reference Breski and Lavie-Ajayi2023). While the rates and content of microaggressions varies between countries, these differences are impacted by differing perceptions of microaggressions. For example, Sims and colleagues (Reference Sims, Kan and Lechien2023) reported differences in the recognition of discriminatory experiences as microaggressive between US and European participants. Sims and colleagues (Reference Sims, Kan and Lechien2023) posit that these differences are likely explained by differing social systems and a tendency for Europeans to be more reticent in their language. European participants may not label events as microaggressive because they do not relate to certain facets of identity, such as race; therefore, these events are likely to be labelled as a different form of interaction. Wherever individuals are socialized into ruling classes with privileged identities one is likely to find microaggressions. Regardless of these differences, it is clear that subtle everyday forms of prejudice, whether recognized as microaggressions or not, exist and cause harm both outside and inside the US.
Therapist takeaway: Microaggressions are not unique to the United States – they occur wherever social hierarchies and dominant group norms exist, including in Canada, Europe, and beyond. Therapists practising outside the USA must not dismiss microaggressions as an ‘American issue’, but instead recognize how these subtle harms manifest within their own cultural contexts. Addressing them is essential to providing culturally responsive and trauma-informed care globally.
Discussion
Now that we have addressed many of the misconceptions that aim to discredit microaggressions (Table 1), it is important to recalibrate our discussion on the future. What can we do as clinicians, researchers, students, and people with this knowledge? And what considerations should be made for patients or clients experiencing microaggressions? In this section, we will discuss how the DDD and MIAPSI models, described in the Introduction, can provide insight for CBT clinicians confronting microaggressions, and then present some clinical considerations inspired by these models, concepts, and misconceptions.
Microaggression misconceptions and evidence

Cultural humility
Cultural humility is a continuous process of reflecting on one’s own culture while seeking to understand others, recognizing and unlearning biases, adjusting power imbalances, and contributing to partnerships that are mutually beneficial and unoppressive (Cleaver et al., Reference Cleaver, Carvajal and Sheppard2016). Mental health clinicians must be especially attuned to experiences of prejudice and consider cultural factors that impact effective professional practices. The process of challenging unhelpful thoughts and behaviours is core to CBT (Beck and Haigh, Reference Beck and Haigh2014). Self-reflection around beliefs, thoughts and behaviours that contribute to, or stem from, these biased misconceptions is a practice of cultural humility. With this knowledge, CBT clinicians may tactfully utilize cognitive behavioural techniques to address maladaptive behaviour, thus engaging in cognitive restructuring that promotes equity. Competence means recognizing social identity and its influence on the therapeutic process, such as the ability to develop rapport, to develop a working alliance, and overall, to be culturally empathetic. Cultural humility reflects a way of being wherein clinicians maintain an other-oriented perspective that involves respect, lack of superiority, and attunement to clients’ cultural heritage (Hook et al., Reference Hook, Davis, Owen, Worthington and Utsey2013). Without a knowledge of, and an openness to explore inequities, clinicians may inadvertently reinforce biased or distorted beliefs. It behoves clinicians to enact this other-oriented, unselfish, and humble perspective, which may ultimately assist patients in reaching their therapeutic goals (Owen et al., Reference Owen, Jordan, Turner, Davis, Hook and Leach2014a).
Clinical considerations for CBT clinicians
Part of developing cultural humility is integrating concepts that consider minoritized perspectives and reflect on the interconnectedness of power, oppression, and suffering. Indeed, research has shown that a lack of perspective-taking is one predictor for generalized prejudice (Levin et al., Reference Levin, Luoma, Vilardaga, Lillis, Nobles and Hayes2016). Third-wave CBT modalities such as acceptance and commitment therapy that utilize perspective-taking show promise for confronting racism (Matsuda et al., Reference Matsuda, Garcia, Catagnus and Brandt2020). Clinicians, for themselves and for their clients, can use perspective to practise cultural humility. In the following section, we will describe how, through considering the common misconceptions, we can implement a variety of CBT interventions to deal with microaggressions.
Models like the DDD model and MIAPSI highlight the socialized nature of prejudice. Similarly, behavioural-analytic perspectives express the learned nature of prejudice through concepts of respondent and operant conditioning, derived relational responding, and stimulus generalization (Goodwyn, Reference Goodwyn, Sadavoy and Zube2022; Matsuda et al., Reference Matsuda, Garcia, Catagnus and Brandt2020). Clinicians should consider how the models (e.g., MIAPSI; Bergkamp et al., Reference Bergkamp, Olson and Martin2022b) describe tendencies for awareness of privilege to result in defensive and protective responses from offenders. From a cognitive behavioural perspective, defensiveness is a response to negative internal emotional states. Functionally, when beliefs (e.g., verbal rules such as ‘I am not racist’) are challenged, individuals may experience negative affect; and therefore, attempt to avoid these emotions through maladaptive behaviour (Matsuda et al., Reference Matsuda, Garcia, Catagnus and Brandt2020). Misconceptions inaccurately rationalize maladaptive behaviour; therefore, facilitating avoidance. Moreover, the verbal rules that govern prejudicial behaviour, like most mental health problems, serve to restrict individuals from pursuing what they value, underpinning the benefit of addressing microaggressions for victims and for offenders as well.
With this understanding, we suggest CBT clinicians consider the influence of these misconceptions on the therapeutic alliance, case conceptualisations, and cognitive restructuring in therapy.
Therapeutic relationship and alliance
The therapeutic relationship and alliance are vital to ensuring positive client outcomes to therapy. The basic tenets of a strong therapeutic alliance include active listening, empathy, collaboration, reliability, validation, and flexibility. In the case that a therapist-perpetrated microaggression occurs, this serves as in vivo material for case conceptualisation or alliance repair. For example, a racialized client describes an experience of racism that occurred in the week prior to session, where they were followed around a store by security while they were shopping. The therapist immediately responds with, ‘Are you sure that you are not overthinking things or being too sensitive?’. The client then appears to shut down, and the therapist overlooks the client’s disposition as related to a racially insensitive (and harmful) comment. Far too often and aided by the various misconceptions outlined in this paper, clinicians fail to recognize the impact of racial microaggressions, and the therapeutic rupture that comes with invalidating them. Whether alone or in the context of supervision, the CBT therapist must reflect and consider the ABC’s they profess (see Table 2).
Example of a therapist’s self-reflective functional analysis

Following the simplistic functional analysis of the therapist’s behaviour, it is evident how such experiences threaten the therapeutic alliance. The therapist is inadvertently positively punishing open disclosures of microaggressions, which may be contributing to the clients suffering. Understanding this, therapists should reflect and adapt their behaviour to respond in more equitable and efficacious ways (see Table 3).
Ideal outcome self-reflective functional analysis

Practising this self-reflection and analysis, importantly, provides clinicians with a greater understanding of their own behaviour and its influence on clients. While mistakes are inevitable, repairing and recognizing ruptures to the therapeutic alliance become easier with this awareness.
In addition to avoiding mistakes that threaten the therapeutic alliance, therapists may use experiences like these as exposure material. Using therapist perpetuated, or past microaggressions, for exposures utilizes established CBT techniques that benefit the client, and:
-
(1) Allow for the therapist to take accountability for their role in the therapeutic rupture and/or oppression.
-
(2) Help the client confront everyday microaggressions.
-
(3) Create a collaborative opportunity for developing cultural competence while strengthening the therapeutic relationship.
Race is one of the most challenging and stigmatized identities to navigate. White clinicians may struggle to face their own role in oppression head-on. However, this resistance can be amenable to change through reflection and awareness. Clinicians would serve to benefit from recognizing and processing fears of appearing racist (i.e., taking a ‘colourblind’, passive approach and ignoring differences), fears of recognizing personal bias (i.e., the racial biases, prejudices, and stereotypes that impact interpersonal relationships), fears of confronting their own privilege (i.e., conversations about White privilege require the acknowledgement that White individuals have benefited from racism), and the fear of taking accountability (i.e., confronting and dismantling White privilege may lead to a shift in status, social circles, socioeconomic opportunities, etc.; Sue et al., Reference Sue, Capodilupo, Torino, Bucceri, Holder, Nadal and Esquilin2007; Sue and Spanierman, Reference Sue and Spanierman2020). Albeit challenging, clinicians’ awareness and ability to discuss microaggressions are linked to positive therapy outcomes (DeBlaere et al., Reference DeBlaere, Zelaya, Dean, Chadwick, Davis, Hook and Owen2023). Thus, it is the ethical responsibility of clinicians to take an active anti-oppressive approach to care by creating space for discussing microaggressions, including addressing their own biases, and detecting microaggressions when they occur in therapy, minimizing the risk of harm (Nadal et al., Reference Nadal, Griffin, Wong, Hamit and Rasmus2014; Owen et al., Reference Owen, Drinane, Tao, DasGupta, Zhang and Adelson2018).
Case conceptualisations
Case conceptualisations are a core element for developing therapeutic interventions. Of particular importance for conceptualising problems around microaggressions is integrating elements of power and oppression into your formulation. While there are some behavioural-analytic explanations of racism (see also Arhin and Thyer, Reference Arhin, Thyer and Chin2004; Matsuda et al., Reference Matsuda, Garcia, Catagnus and Brandt2020), adapting case conceptualisations to incorporate microaggressions may bolster culturally competent care. Power and oppression are environmental contexts that shape the learning of those oppressed and their oppressors (Goodwyn, Reference Goodwyn, Sadavoy and Zube2022). Microaggressions are one of many behaviours that maintain these environments. For example, chronic exposure to microaggressions may lead to core beliefs like ‘all White people are unsafe’ or behaviours such as social isolation.
With this understanding, we suggest that incorporating variables of power and oppression into CBT conceptualisations serve to:
-
(1) Allow for a deeper understanding of the contingencies that lead to marginalized suffering.
-
(2) Provide more opportunities and ideas for CBT interventions.
-
(3) Empower minoritized clients through validation and culturally competent care.
One such example of incorporating power and oppression into CBT conceptualisations is understanding covert instances of oppression that reinforce rigid core beliefs around traditional masculinity. For example, some Black men’s adherence to traditional masculinity norms (e.g., restrictive emotionality, toughness) may be culturally contingent upon systems of oppression that reinforce rigid expectations for what a man ‘should be’. Chronic exposure to racial microaggressions (e.g., invalidation and tone policing like ‘You are over-reacting’) can further anchor these beliefs by reinforcing society’s aversiveness to Black men’s emotions. While traditional masculinity is not inherently maladaptive, and in some cases can act as a protective factor for Black men who face barriers to seeking mental health support (e.g., Colemane-Kirumba et al., Reference Coleman-Kirumba, Cornish, Horton and Alvarez2023), recognizing experiences of microaggressions may provide insight into over adherence to masculine beliefs that contribute to a client’s struggles (e.g., emotional suppression).
Cognitive restructuring
Cognitive restructuring refers to the process of identifying, challenging and reframing maladaptive thoughts (Beck, Reference Beck2011). Cognitive restructuring can be useful for:
-
(1) Targeting maladaptive therapist-held schemas and beliefs about microaggressions
-
(2) Reframing client appraisals of microaggressions.
In both instances, it is important to avoid invalidating the client’s experience of the microaggression and their broader experience of oppression. The goal of these practices is not to challenge the existence of racism or microaggressions. Rather, clinicians should target automatic thoughts that are unhelpful or counter-productive to processing and coping with experiences of oppression. Additionally, therapeutic spaces are client-centred; therefore, targeting one’s own (i.e., therapist-held) beliefs should be done as a reflective process outside of therapy, unless the practice is intentional and directly in the client’s benefit.
Debunked misconceptions of microaggressions are perhaps the most relevant for targeting maladaptive therapist-held schema or stereotypes. The accumulation and reinforcement of biased perceptions around marginalized people can form negatively biased schemas or core beliefs that perpetuate oppression. CBT strategies such as Socratic questioning, recognizing cognitive distortions, evidence testing, and reattribution may be used to target maladaptive beliefs held by therapists and other offenders of microaggressions.
For example, a therapist may initially question the validity of a microaggression and assume these complaints are reflective of neuroticism. Through the clinician’s newfound understanding that (a) historically, neuroticism has been used to dismiss marginalized experiences of oppression, and (b) that microaggressions have real and meaningful negative impacts on mental health, the therapist can use this evidence to challenge their own initial thoughts and feelings. With continued effort, clinicians can recognize their own patterns of defensiveness and effectively manage countertransference, so they respond in a more empathetic and effective way for the client.
As briefly mentioned, victims of microaggressions may also benefit from cognitive restructuring. Through these strategies, CBT clinicians can help clients identify the automatic thoughts and core beliefs that contribute to their suffering in the face of oppression. For example, a client who regularly experiences microaggressions at work may begin to associate daily acts of prejudice with negative core beliefs like, ‘I am unlovable’. A traditional CBT clinician’s guide takes the client through a cognitive restructuring process that incorporates reframing unhelpful thoughts and providing explanations for pervasive misconceptions that change how the client views these thoughts: ‘Is it possible the microaggression you experienced is not about you, but perhaps caused by wrong thinking in the other person?’. However, cognitive restructuring poses risks in the therapeutic process if used to challenge the reality and impact of a discriminatory experience. Therefore, it is important to avoid invalidating the client’s experiences of microaggressions.
Additionally, one alternative, but related, method for clients possessing marginalized identities is to use acceptance and commitment therapy (ACT), or other contextual behavioural approaches that do not require challenging a thought (Matsuda et al., Reference Matsuda, Garcia, Catagnus and Brandt2020). Drawing from ACT modalities, clients can learn cognitive diffusion, the process of altering how one relates and responds to unhelpful thoughts, which emphasizes observation and values-based action (Payne, Reference Payne2022).
Recently, our laboratory started a social media campaign called STOP Bad Therapy to draw attention to the harm that this misinformation has caused in clinical care. We have included some example graphics from our campaign to illustrate our educational material about how microaggressions might show up in CBT (see Figure 2).
STOP Bad Therapy campaign graphics.

Each graphic depicts a clinician (male) inadequately addressing a microaggression (with a misconception), and the client (female) responding (with the truth).
Conclusion
Prejudice presents itself in several forms, from blatant acts of violence to the more hidden everyday slights known as microaggressions. The subtle yet pervasive nature of microaggressions contributes to the detrimental impacts on physical and mental well-being for minoritized and stigmatized people globally (Smith and Griffiths, Reference Smith and Griffiths2022). The everyday experience of microaggressions is aptly described by the common idiom: ‘death by a thousand cuts’, differing only through the offenders, and more insidiously, researchers’ failure to recognize that they are indeed harmful, and not simply a cultural or social faux pas.
Given the supporting evidence, correcting misconceptions about microaggressions is crucial to ensuring that no further harm, whether it be invalidation, is committed towards minoritized clients and clinicians. As an important public health issue, investigating microaggressions and their impacts is an ethical responsibility for researchers, which will aid clinicians in better-serving all clients and minimizing mental health disparities (DeBlaere et al., Reference DeBlaere, Zelaya, Dean, Chadwick, Davis, Hook and Owen2023; Nadal et al., Reference Nadal, Griffin, Wong, Hamit and Rasmus2014; Owen et al., Reference Owen, Drinane, Tao, DasGupta, Zhang and Adelson2018). Despite the often politically charged nature of microaggressions, our goal as researchers, clinicians, and educators remains the same, to provide clinicians with correct information so that they may skilfully and empathetically help clients experiencing microaggressions; and to no longer accept microaggressions as an unseen, misunderstood, or dismissed phenomenon.
Key practice points
-
(1) Microaggressions are common and harmful for those with minoritized identities.
-
(2) Competent clinicians must understand the true nature of microaggressions and not dismiss their importance.
-
(3) Many misconceptions persist due to bigoted ideas promoted by scholars and others who are threatened by the principles of social justice and equality.
-
(4) All clinicians need to learn how to address microaggressions responsibly in therapeutic encounters.
Data availability statement
Data availability is not applicable to this article as no new data were created or analysed in this study.
Acknowledgements
The authors would like to thank the following people for their input and assistance: Sophia Gran-Ruaz, Dana Strauss, Manzar Zare, and Simranjeet Saini.
Author contributions
Kellen Saxberg: Writing - original draft (lead), Writing - review & editing (lead); Myriah MacIntyre: Methodology (supporting), Project administration (supporting), Writing - original draft (supporting), Writing - review & editing (supporting); Ahmad Alftieh: Writing - original draft (supporting); Sonya Faber: Project administration (lead), Writing - original draft (supporting), Writing - review & editing (supporting); Gloria Lamontagne: Writing - original draft (supporting); Monnica Williams: Funding acquisition (lead), Methodology (lead), Project administration (supporting), Writing - original draft (equal), Writing - review & editing (equal).
Financial support
This research was undertaken, in part, thanks to funding from the Canada Research Chairs Program, Canadian Institutes of Health Research (CIHR) award number: CRC-2024-00171 (PI: M. Williams).
Competing interests
The author S.F. is an employee of Angelini Pharma and a partner in the company Bioville GmbH, neither of which have any competing interests, nor have influenced the content. The other authors report no competing interests.
Ethical standards
All authors adhered to the Ethical Principles of Psychologists and Code of Conduct as set out by the BABCP and BPS. No ethical approval was needed for this paper.


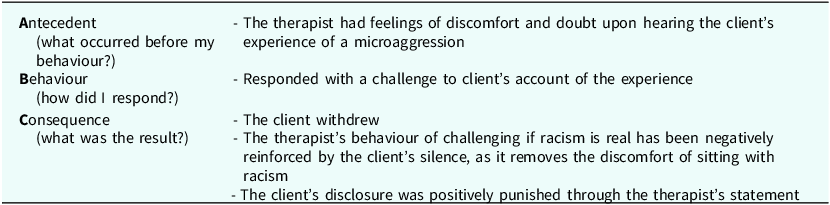
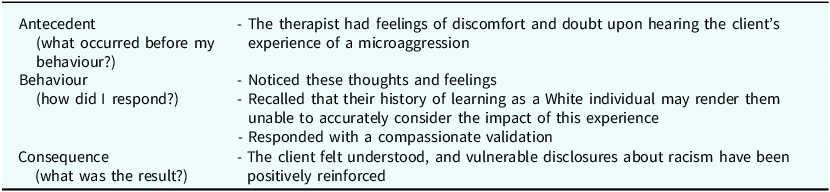


 Open access
Open access
Comments
No Comments have been published for this article.