


Impact statements
Khat consumption is a growing public health and social challenge with profound consequences. This policy brief urges immediate action to safeguard individuals, families and communities from the harmful effects of excessive khat use by empowering policymakers to transform existing evidence into practical, actionable recommendations. Furthermore, it raises awareness on the social, economic, psychological and health impact of excess khat use, informs evidence-based decision-making and effective implementation into legislation. It also highlights the consideration of legal restrictions on khat use, especially in vulnerable populations, including children, individuals with mental disorders, pregnant women and settings such as hospitals and schools. The findings offer new insight into the consequences of excessive khat consumption and inform decisive policy action to guide strategies mitigating its harmful effects.
Background
The scope of the problem
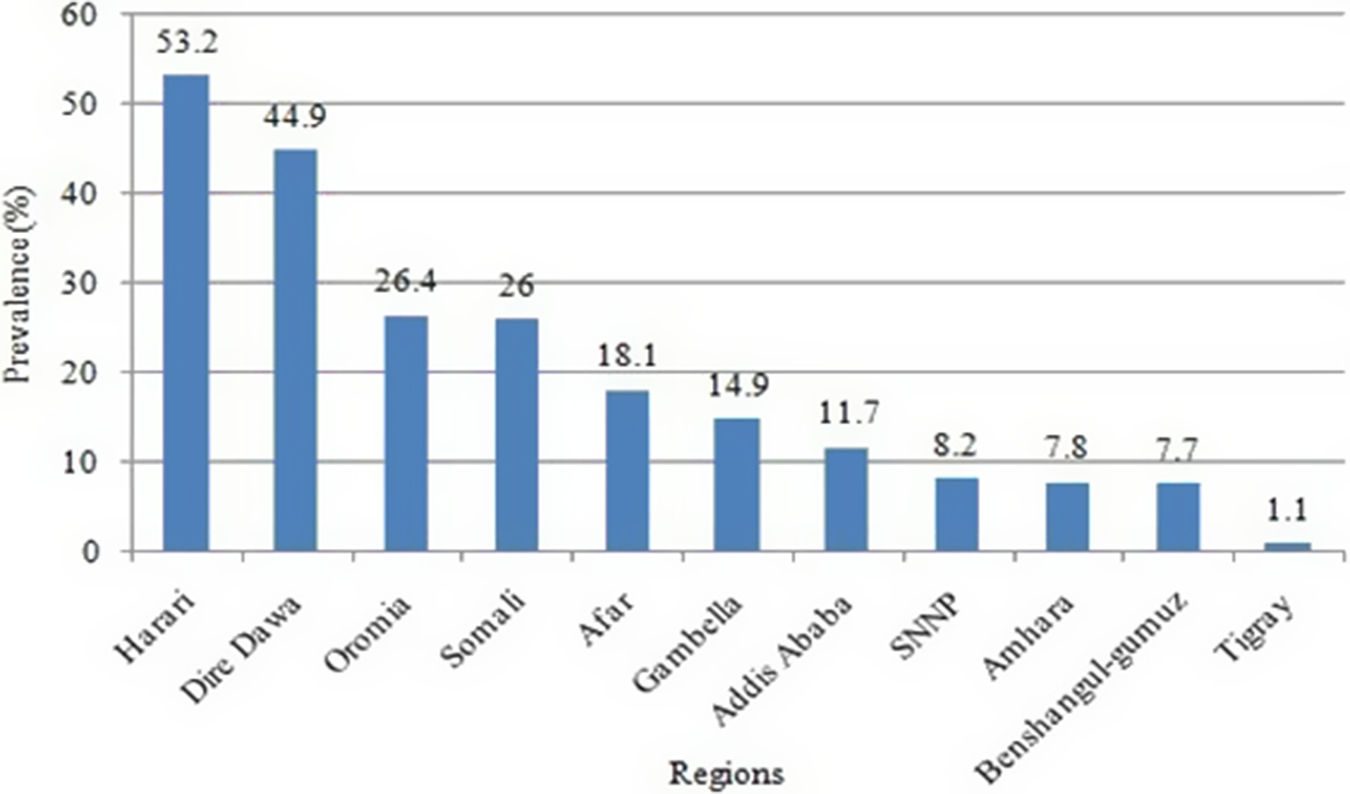
Khat is a stimulant grown and used mostly in East Africa and the Arabian Peninsula (Ahmed et al., Reference Ahmed, Minami and Rasmussen2020). About 10 million people worldwide chew khat daily (Atnafie et al., Reference Atnafie, Muluneh, Getahun, Woredekal and Kahaliw2020). The burden of substance use is dramatically increasing in Africa among young adults, which has a detrimental impact on the economy, healthcare system and society (Ahmed et al., Reference Ahmed, Minami and Rasmussen2020; Akalu et al., Reference Akalu, Baraki, Wolde, Lakew and Gonete2020). In Ethiopia, the incidence of khat use can be related to cultural context, such as the normalization of khat chewing within communities, its accessibility and its economic importance as a cash crop (Haile and Lakew, Reference Haile and Lakew2015). A study done in 2011 showed that the overall khat chewing prevalence was 15.3% with regional variation, with disparities, the highest burden of khat use in Harari and the lowest in Tigray (see Figure 1) (Haile and Lakew, Reference Haile and Lakew2015; Atnafie et al., Reference Atnafie, Muluneh, Getahun, Woredekal and Kahaliw2020). A study assessing the epidemiologic burden of khat chewing in Ethiopia showed a pooled prevalence of 19.55% for current use and 26.14% lifetime use (Ayano et al., Reference Ayano, Ayalew, Bedaso and Duko2024). The current use was significantly higher among men (23.72%) compared to women (8.45%), while lifetime use was 29.8% for men and 13.02% for women. Furthermore, a systematic review on khat use among pregnant women in Ethiopia showed a pooled prevalence of 26.6%, highlighting a critical public health concern on khat (Wogayehu et al., Reference Wogayehu, Demissie, Wolka, Alemayehu and Daka2023).
The prevalence of khat chewing in different regions of Ethiopia. Source: Haile and Lakew (Reference Haile and Lakew2015).

The use of khat is increasing dramatically in Ethiopia among the young population (Atnafie et al., Reference Atnafie, Muluneh, Getahun, Woredekal and Kahaliw2020). One-third of university students chew khat in Ethiopia (Mekuriaw et al., Reference Mekuriaw, Zegeye, Molla, Hussen, Yimer and Belayneh2020). College students use khat to get out of stressful social and academic burdens (Mekuriaw et al., Reference Mekuriaw, Zegeye, Molla, Hussen, Yimer and Belayneh2020). Khat has a significant impact on the young and productive population, which in turn can have an impact on the country’s economy in the long run (Akalu et al., Reference Akalu, Baraki, Wolde, Lakew and Gonete2020). Furthermore, khat use has also increased in women (Ahmed et al., Reference Ahmed, Minami and Rasmussen2020). The prevalence of khat chewing among pregnant women was 21.42% in the Horn of Africa and the Arabian Peninsula (Basa and Comiskey, Reference Basa and Comiskey2022).
Problematic khat use is associated with longer-term psychological, physical and social consequences (Ahmed et al., Reference Ahmed, Minami and Rasmussen2020). It is associated with decreased academic performance, with impacts of khat on concentration and motivation (Basker, Reference Basker2013). Driving under the influence of khat results in the impairment of drivers with high rates of traffic crashes and fatalities in Ethiopia, yet it remains under-researched compared to other substances like alcohol (Eckersley et al., Reference Eckersley, Salmon and Gebru2010). Ethiopian federal law forbids “driving under the influence of mind-affecting drugs.” Despite the presence of the law, the awareness and implementation of the law among traffic police officers are scarce (Eckersley et al., Reference Eckersley, Salmon and Gebru2010). Furthermore, the absence of screening technology that tests for khat consumption impedes routine screening and implementation (Eckersley et al., Reference Eckersley, Salmon and Gebru2010).
Globally, there are no uniform international regulations on khat use. While khat use and accessibility are controlled by the government of some countries including Europe, Canada, the United Kingdom and the United States, others countries lack any formal regulatory measures (Klein et al., Reference Klein, Beckerleg and Hailu2009; El-Menyar et al., Reference El-Menyar, Mekkodathil, Al-Thani and Al-Motarreb2015). In Ethiopia, there is limited restriction on khat; however, in the Amhara region, the regional government imposed a policy and increased taxation (Akalu et al., Reference Akalu, Baraki, Wolde, Lakew and Gonete2020). The Ethiopian economy is highly dependent on khat production and export. Despite this, Ethiopian law neither explicitly allows nor prohibits the cultivation, consumption or sale of khat (Cochrane and O’Regan, Reference Cochrane and O’regan2016). In Ethiopia, in recognition of the burden of khat use in the country, the Ministry of Health has established a national task force that advises the khat-regulating legislation through evidence generation, policy guidance, advocacy and awareness creation (Ababor et al., Reference Ababor, Kebede, Getachew, Bogale, Solomon, Mideksa, Ararso, Zeru, Wolde and Dagne2022). There is still a lot that needs to be done in advocacy and policy about this critical issue. In addition, there is a need for international collaboration that involves governments, international organizations and relevant stakeholders, which is important to tackle this public health concern.
Impact of khat use on physical health, mental health and social well-being
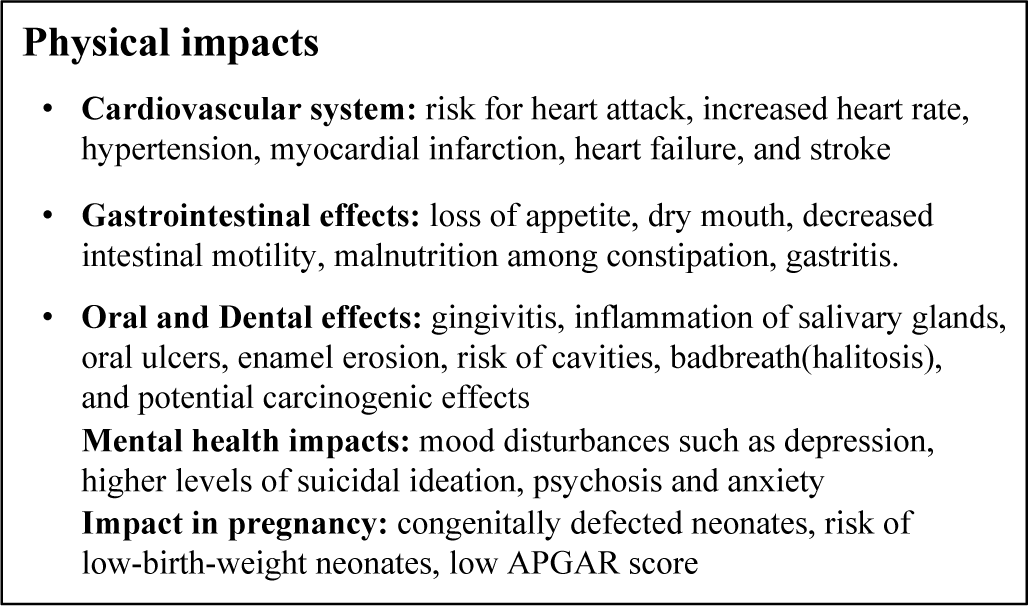
Khat use is associated with physical and mental health disorders and social consequences (Ahmed et al., Reference Ahmed, Minami and Rasmussen2020). The impacts associated with khat use are discussed as listed below (see Figure 2).
Impact of khat use on physical health, mental health and social well-being (Ahmed et al., Reference Ahmed, Minami and Rasmussen2020; Khatib et al., Reference Khatib, Jarrar, Bizrah and Checinski2013; Magdum, Reference Magdum2011; Atnafie et al., Reference Atnafie, Muluneh, Getahun, Woredekal and Kahaliw2020; Masood and Al-Mansoob, Reference Masood and Al-Mansoob2015; Bayih et al., Reference Bayih, Belay, Ayalew, Tassew, Chanie, Feleke, Asnakew, Legas, Belete and Mekie2021b).

Physical health
The physical consequences of khat use are significant and can impact various bodily systems. The sympathetic nervous system significantly increases the risk for cardiovascular complications, including increased heart rate and blood pressure, hypertension, myocardial infarction, heart failure and stroke (Ahmed et al., Reference Ahmed, Minami and Rasmussen2020; Akalu et al., Reference Akalu, Baraki, Wolde, Lakew and Gonete2020; Mega and Dabe, Reference Mega and Dabe2017). Acute gastrointestinal effects range from acute symptoms, such as loss of appetite, dry mouth and decreased intestinal motility leading to constipation, to long-term issues, such as malnutrition among habitual users and constipation. Prolonged use may also lead to delayed gastric emptying, increased risk of gastritis and esophagitis, as well as potential precancerous conditions such as Barrett’s esophagus (Magdum, Reference Magdum2011; Khatib et al., Reference Khatib, Jarrar, Bizrah and Checinski2013; Ahmed et al., Reference Ahmed, Minami and Rasmussen2020). In addition, periodontal effects of khat use include gingivitis, inflammation of salivary glands, oral ulcers, enamel erosion, risk of cavities, bad breath (halitosis) and potential carcinogenic effects (Ahmed et al., Reference Ahmed, Minami and Rasmussen2020; Akalu et al., Reference Akalu, Baraki, Wolde, Lakew and Gonete2020; Basker, Reference Basker2013).
Mental health impacts
The mental health impacts of khat use are directly related to the severity of khat dependence, the frequency and intensity of its use (Atnafie et al., Reference Atnafie, Muluneh, Getahun, Woredekal and Kahaliw2020). Problematic khat use is associated with mood disturbances, including symptoms of depression, higher levels of suicidal ideation and anxiety. The use of khat can result in psychosis in vulnerable populations, such as those with preexisting psychosis, family history of psychosis, large and prolonged use and early onset of khat use. The prolonged and increased quantity has been associated with cognitive deficits, such as impairments in cognitive flexibility, working memory and difficulties in tasks requiring inhibitory control and decision-making (Magdum, Reference Magdum2011; Ahmed et al., Reference Ahmed, Minami and Rasmussen2020 Reference Ahmed, Ruiz, Cohen Kadosh, Patton and Resurrección2021).
Social impacts
Prolonged khat use can result in social isolation, which can strain family and friendship social interaction because of the prioritization of khat use over relationships and responsibilities. The neglect can result in conflicts in the family. Furthermore, it can have a significant economic impact because users spend money on khat use and neglect essential personal and family needs. In regions of the khat belt, khat is socially accepted and incorporated into social gatherings and religious praying. These can impede the efforts of abstinence (Ahmed et al., Reference Ahmed, Minami and Rasmussen2020). There is a high socioeconomic burden related to khat consumption, which includes spending money, that leads to financial constraints for individuals and extends to a social burden to families, women, children, the community and the country at large (Ababor et al., Reference Ababor, Kebede, Getachew, Bogale, Solomon, Mideksa, Ararso, Zeru, Wolde and Dagne2022).
Impact of khat use on pregnant women
Khat use during pregnancy can lead to the disruption of the fetal neural tube development, undifferentiating brain vesicles, causing incomplete closure of the brain flexure, low birth weight and low Apgar scores (Bayih et al., Reference Bayih, Ayalew, Tadege, Mekie, Kiros, Alemu, Alemnew, Getacher, Belay, Birhane and Alemu2021a). Furthermore, it can have negative impacts on the pregnancy, such as breech presentation, anemia, premature rupture of the membrane, postpartum hemorrhage, perineal tears, intrauterine fetal death (Masood and Al-Mansoob, Reference Masood and Al-Mansoob2015), depression, loss of appetite, anemia, sleep disturbance and memory impairment (Basa and Comiskey, Reference Basa and Comiskey2022). The use of khat during pregnancy increases the risk of congenitally defective neonates and risk of low birth weight neonates, low APGAR score, which is due to the sympathomimetic activity of cathinone that is responsible for its vasoconstrictive effects, leading to complications of pregnancy and birth outcome (Bayih et al., Reference Bayih, Belay, Ayalew, Tassew, Chanie, Feleke, Asnakew, Legas, Belete and Mekie2021b).
Analysis
Key debates of existing research and current policies
There are several controversies attached to khat use, such as health implications, legal status and socioeconomic effects. Even though the health and mental health impacts are prominent and noticeable, some individuals argue that the prohibition of khat use can help manage health risks and control the market, but the prohibition can enhance illicit trade and loss of cultural heritage (Ababor et al., Reference Ababor, Kebede, Getachew, Bogale, Solomon, Mideksa, Ararso, Zeru, Wolde and Dagne2022). Most of them also argue that khat is a source of income for Ethiopia and farmers because the economic benefits outweigh the financial strains (Lamina, Reference Lamina2010; Ababor et al., Reference Ababor, Kebede, Getachew, Bogale, Solomon, Mideksa, Ararso, Zeru, Wolde and Dagne2022). There is an inconsistency that leads to debates about its categorization of khat as an illicit drug (Lamina, Reference Lamina2010). The presence of controversy on the existing evidence on the dependency, mental and health impacts of khat can contribute to diversified views on the khat’s safety and being assigned as an illicit drug (Lamina, Reference Lamina2010; McGonigle, Reference McGonigle2013).
The WHO Expert Committee on Drug Dependence has reviewed khat under the 1971 Convention and norephedrine, which is controlled under the 1988 Convention. The committee concluded that khat has a low potential for abuse and dependence (Organization, Reference Organization2006). Consequently, the committees did not recommend scheduling khat under international drug treaties, although they recognized the health risk associated with excess use (Organization, Reference Organization2006). So, there is no global regulation but rather regional-level legislation or regulations, which have created variation in the policy in many countries in the world. There is a wide variation in legal regulation among different countries, which has led to strains in the implementation of control of khat use and raises questions and concerns about the unified effectiveness of bans (Griffiths et al., Reference Griffiths, Lopez, Sedefov, Gallegos, Hughes, Noor and Royuela2010). In some countries, such as the United States, Canada, Denmark, France, Germany, Italy, Norway, Spain, Sweden, Saudi Arabia, Rwanda, Tanzania, the Netherlands, the United Kingdom, Australia and South Africa, khat is prohibited as a controlled substance (Klein et al., Reference Klein, Beckerleg and Hailu2009; El-Menyar et al., Reference El-Menyar, Mekkodathil, Al-Thani and Al-Motarreb2015; Ahmed et al., Reference Ahmed, Minami and Rasmussen2020). In Australia, imports are banned, and no personal use is permitted. There is variation in the regulation within states for use and cultivation; it is illegal in Queensland but varies in other states (Douglas and Pedder, Reference Douglas and Pedder2010). In other countries like Ethiopia, Somalia, Djibouti, Kenya, Uganda and Yemen, there is no sort of legal regulation (Klein et al., Reference Klein, Beckerleg and Hailu2009; El-Menyar et al., Reference El-Menyar, Mekkodathil, Al-Thani and Al-Motarreb2015; Ahmed et al., Reference Ahmed, Minami and Rasmussen2020).
In the past, there was resistance to the effective implementation of the khat ban because it is important to have socially and culturally tailored regulation rather than an outright ban (Klein et al., Reference Klein, Beckerleg and Hailu2009). There is a need to include legally restricting khat use in vulnerable populations like children, individuals with mental disorders and pregnant women, and settings such as hospitals and schools (Klein et al., Reference Klein, Beckerleg and Hailu2009). Researchers suggest that the direct banning of khat use abruptly can be difficult to accept, so collaborative efforts from government and international organizations with regulation and harm-reduction measures are urgently needed (Odenwald et al., Reference Odenwald, Warfa, Bhui and Elbert2010). Prohibition in other countries has, in the past, led to enhanced black market and cross-border smuggling, increased the prices, boosted the khat economy and (Cochrane and O’Regan, Reference Cochrane and O’regan2016) increased crime (Anderson and Carrier, Reference Anderson and Carrier2009).
In Ethiopia, the regulation of khat use is considered a more preferred/effective intervention rather than an outright ban. A qualitative study in Jimma, Ethiopia, conducted among 102 khat-chewing participants revealed that those who had agreed upon neither laissez-faire nor total prohibition were viewed as effective. Instead, participants suggested the system that includes empowering khat users with awareness and controlling problematic use, managing supply and restricting the use based on place and age in restricting khat use (Olani, Reference Olani2025). In addition, another study exploring the perception of key stakeholders toward khat use involved key stakeholders including individuals with lived experience, the Ministry of Justice, the Ministry of Women and Social Affairs, the Ministry of Health and health facilities with addiction treatment centers – emphasized on the importance of prevention, treatment or care for individuals with problematic use, law regulation and harm reduction rather than banning (Habtamu et al., Reference Habtamu, Teferra and Mihretu2023). Furthermore, the study suggests that excessive khat can negatively impact health and undermine that can have impacts on human rights, especially youth, families and vulnerable populations, affecting access to health education and family well-being, strongly justifying the call for comprehensive regulation and targeted interventions (Jemaneh, Reference Jemaneh2012). The Ethiopian economy is highly dependent on khat production and export. Despite this, Ethiopian law neither explicitly allows nor prohibits the cultivation, consumption or sale of khat (Cochrane and O’Regan, Reference Cochrane and O’regan2016). There is conflicting evidence on the mental health impacts of khat use due to the limitations of studies eliciting causal relationships, potential confounders and biases (Olani et al., Reference Olani, Gerbaba, Getnet, Soboka and Decorte2023). But there is still existing evidence that shows the risk of excessive use affecting the vulnerable population, with many health impacts. There is a need for future studies on these gaps in the literature with prospective designs, standardized and valid measures of khat use and addressing types of mental health disorders (Griffiths et al., Reference Griffiths, Lopez, Sedefov, Gallegos, Hughes, Noor and Royuela2010; Olani et al., Reference Olani, Gerbaba, Getnet, Soboka and Decorte2023).
Proposed policies
This policy proposes to enforce the importance of education campaigns aimed at awareness creation on the impact of khat use, the role of research in generating strong evidence-based insight and to consider legally restricting availability and khat use in vulnerable populations, including children under 18 years, individuals with mental disorders, pregnant women, as well as settings such as hospitals and schools by relevant government authorities like the Ethiopian Revenue and Customs Authority, Ethiopian Food and Drug Authority, Ministry of Trade and Regional Integration, traffic police, the Ministry of Health, the Ministry of Education and researchers. It also wants to target the approaches of awareness, prevention, harm reduction, managing supply and restricting the use in place and age. Furthermore, it also recommends multilevel recommendations that target education, policy measures related to regulation and screening that are culturally tailored.
Policy recommendations
To the Ministry of Health
Education (Ahmed et al., Reference Ahmed, Minami and Rasmussen2020)
-
• Create awareness among khat users and healthcare providers about the potential harms and dependence.
-
• Public education campaigns that raise awareness about the potential harms of khat use.
-
• To prepare educational material for educational campaigns with culturally tailored approaches that consider community norms and values.
-
• To engage religious leaders in awareness campaigns and prevention strategies.
Other recommendation
-
• To develop testing technologies that screen the consumption of drivers for traffic police.
-
• Policies should take into account the culture and social norms associated with khat consumption in Ethiopia.
-
• To establish rehabilitation services for individuals with problematic khat and other substances.
-
• To initiate an international collaboration that involves governments, international organizations and relevant stakeholders that are important to tackle problematic khat use.
Policymakers (Klein and Metaal, Reference Klein and Metaal2010; Mihretu et al., Reference Mihretu, Teferra and Fekadu2017; Ahmed et al., Reference Ahmed, Minami and Rasmussen2020; Akalu et al., Reference Akalu, Baraki, Wolde, Lakew and Gonete2020; Ababor et al., Reference Ababor, Kebede, Getachew, Bogale, Solomon, Mideksa, Ararso, Zeru, Wolde and Dagne2022)
To government officials (Ethiopian Revenue and Customs Authority, Ethiopian Food and Drug Authority, Ministry of Trade and Regional Integration, and the traffic police)
-
• To regulate khat sale and distribution, such as restricting shop availability, age restrictions (allowing only above 18 years), increased taxation, requesting licenses for vendors and limits on the quantity that can be purchased to control its availability and reduce problematic use.
-
• To regulate access and availability of khat by restricting the time, place and status of individuals.
-
• To engage stakeholders, such as government officials, traffic police, health professionals and community leaders, about khat use and road safety
To the Ministry of Education
-
• To integrate mental health and substance education into the curriculum for students in educational institutions.
To Ethiopian Researchers (Ababor et al., Reference Ababor, Kebede, Getachew, Bogale, Solomon, Mideksa, Ararso, Zeru, Wolde and Dagne2022; Olani et al., Reference Olani, Gerbaba, Getnet, Soboka and Decorte2023)
-
• There is a need for future studies to fill the gaps in the literature, such as longitudinal and case–control studies, to understand the long-term impacts of khat.
Conclusion
About 10 million people worldwide chew khat daily. Chronic khat use is a public health problem associated with physical and psychological impacts, such as mental health disorders and social consequences. The use of khat is increasing dramatically in Ethiopia among the young population. Policymakers need to enforce education campaigns aimed at awareness creation on the impact of khat use. Furthermore, it is important to consider legally restricting the availability and khat use, especially in vulnerable populations like children under 18 years, individuals with mental disorders and pregnant women, as well as in settings such as hospitals and schools. This policy regulation in Ethiopia will play a role in improving public health with a healthier and more productive community.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10189.
Author contributions
S.A.T. contributed to the conceptualization. S.A. searched the literature and wrote the first draft of the manuscript. The original inquiry, policy analysis, report writing, manuscript drafting and manuscript revision were all organized by the authors. S.A.T., S.K., A.F. and C.K. evaluated the manuscript draft and made a sufficient contribution to the research preparation. The final manuscript was read and approved by all authors.
Financial support
No specific fund was secured for this study.
Competing interests
The authors declare none.

 Open access
Open access
Comments
Dear Editor-in-Chief,
On behalf of all coauthors, I’m writing to submit my article entitled “The Regulation and Control of Khat Use and Access in Ethiopia: Policy Brief.” for consideration for the reputable Journal of Cambridge Prisms: Global Mental Health. I can confirm that the attached manuscript is an original piece of work and that I am not submitting it to other journals for consideration.
The research describes the burden of Khat use is high and calls for the consideration of the issue in health policy. There is a need to address this public health concern in public health policy, practice, and implementation of interventions to reduce khat use and prevent the physical and mental health impacts. This policy brief highlights the scope of the problem, physical and mental health impacts, and debates related to khat use in Ethiopia, and gives a recommendation. The finding will new insight into the impacts of excessive use of khat and its implication for policymakers. Please send all correspondence regarding the publication of this article to email: alemayehuselam534@gmail.com. Attached is a copy of the manuscript.
Thank you for your consideration
Sincerely,
Selamawit Alemayehu (MD, Psychiatrist)