


Homelessness is a complex multidimensional issue that impacts populations worldwide. Reference Carver, Ring, Miler and Parkes1 According to UN-Habitat, 2024, nearly 3 billion people live in inadequate housing, and approximately 330 million face homelessness. Reference Filipenco2 Homelessness often remains underrecognised particularly in low- and middle-income countries like India. In India, the problem of homelessness continues to be a significant concern. The Census of India 2011 defines a houseless household as ‘households who do not live in buildings or census houses but live in the open on roadside, pavements, in hume pipes, under flyovers and staircases, or in the open in places of worship, mandaps, railway platforms, etc.’. 3 As per the Census 2011, India has more than 1.7 million homeless people (0.14% of the total population), of whom 938 384 reside in urban areas. 3 Of these, homeless women account for almost 0.7 million of the population. However, non-governmental organisations estimate the number of homeless populations to be much higher. Reference Wilson and Sadi4
Large metropolitan cities in India, such as Delhi, Kolkata, Chennai and Mumbai, account for a higher number of homeless populations. The national capital of India, Delhi, has a population over 16 million, according to the 2011 Census data, and accounts for the highest rates of homelessness of any Indian city, at 46 724 people, representing approximately 1.28% of India’s homeless population. In Delhi, there are over 281 permanent and temporary shelters for the homeless, supported by a range of stakeholders that include civil society organisations, non-governmental organisations, the Delhi Development Authority, Municipal Corporation Delhi and Delhi Urban Shelter Improvement Board. 5,Reference Bhattacharya6
Despite the presence of such services, homeless individuals remain largely invisible and marginalised, facing persistent poverty, unemployment, lack of privacy and safety, exposure to violence, social exclusion, limited access to healthcare and chronic stress. Reference Singh, Koiri and Shukla7 Western literature report a higher rate of violence, poorer mental well-being and higher level of substance use among the homeless population compared with the general population. Reference Rhoades, Wenzel and Golinelli8,Reference Haile, Umer and Ayano9 Homeless women, in particular, experience complex vulnerabilities because of gender-based discrimination, inadequate legal protections and limited livelihood opportunities, especially in low- and middle-income countries.
Evidence suggests homelessness is associated with higher rate of psychiatric symptoms, as well as substance use and related disorders. Reference O’Campo, Nisenbaum and Crocker10 Systematic reviews indicate that 20–50% of this population have major depressive disorder or major depressive episodes, whereas 30–40% experience post-traumatic stress disorder. Reference Duke and Searby11 Up to one in five report moderate to high levels of suicidality. The rates of alcohol and other drug use disorders are higher in homeless women compared with women who are not homeless. Global literature reports the prevalence of substance use and disorder among homeless women ranges from 30 to 55%, and is often associated with reduced utilisation of healthcare services. Reference Guillén, Marín, Panadero and Vázquez12–Reference Adams, Parker, Jablonski, Kennedy, Tasker and Hunter14 Additionally, they face heightened vulnerability to a wide range of health and social risks. Reference O’Campo, Nisenbaum and Crocker10,Reference Duke and Searby11
In the Indian context, existing research has focused on specific subpopulations such as street children, runaway adolescents, homeless men or individuals with severe mental illnesses. Reference Bhat, Singh and Meena15–Reference Talukdar, Roy, Saha, Mitra and Detels18 Individual studies on homelessness have explored the living conditions, the reasons for homelessness and perceived experience of violence among homeless women. Reference Goel, Ghosh, Ojha and Shukla19,Reference Verma and Srivastava20 Thus it appears from the literature that homeless women represent an extremely vulnerable population where their daily lives are marked by insecurity, stigma, limited access to healthcare and exposure to various forms of physical and emotional abuse, which may act as a contributing factor to psychiatric illness and substance use. However, this has not been studied in India.
With this in mind, the present study aimed to assess the patterns and proportion of substance use among homeless women utilising services from urban shelter homes in Delhi. Additionally, the study has also evaluated the psychological well-being and quality of life, and their relation to substance use.
Method
Setting and participants
This exploratory cross-sectional observational study was conducted from December 2021 to March 2023, as part of a Doctor of Management (Addiction Psychiatry) dissertation. This study comprised homeless adult women residing in urban shelter homes located in Delhi, the capital city of India. The study was conducted across five urban shelter homes located in the South, South-East, Central and New Delhi Districts. These shelters are operated under the aegis of the Delhi Urban Shelter Improvement Board, Government of National Capital Territory of Delhi, and are managed by a non-profit organisation, the Society for Promotion of Youth and Masses (SPYM), New Delhi. The study followed the principles enshrined in the Declaration of Helsinki, with approval from the Institutional Ethics Committee (reference numbers: IECPG-691/25.11.2021 and RT-35/23.12.2021). All eligible participants were informed about the nature and purpose of the study. Informed consent was taken from willing participants before recruitment, and it was assured that personal information would be kept strictly confidential. Treatment options were discussed with homeless women who had psychiatric illnesses and were suffering from substance dependence. No incentive was provided to the participants for participating in the study.
The SPYM operates 15 shelter homes designated for families. Among them, five shelter homes operated by the SPYM were selected to make the sample heterogenous. A total of 284 women were registered in the five shelter homes. For this study, participants were recruited through purposive sampling. A formal sample size estimation was not performed. Based on literature research, we aimed for a sample size of at least 150 participants to give meaningful data for further analysis. This was primarily based on feasibility and time available for data collection for the dissertation. To achieve this sample size, a total of 164 homeless women were screened, and 152 of them met the study’s selection criteria and were included in the study.
Women aged between 18 and 50 years, meeting the Census 2011 definition of a homeless individual, currently residing in one of the urban shelter homes and providing informed consent, were included in the study. Individuals were excluded from the study if they were unable to communicate with the interviewer because of reasons such as disability, illness or intoxication at the time of data collection.
Procedure of the study
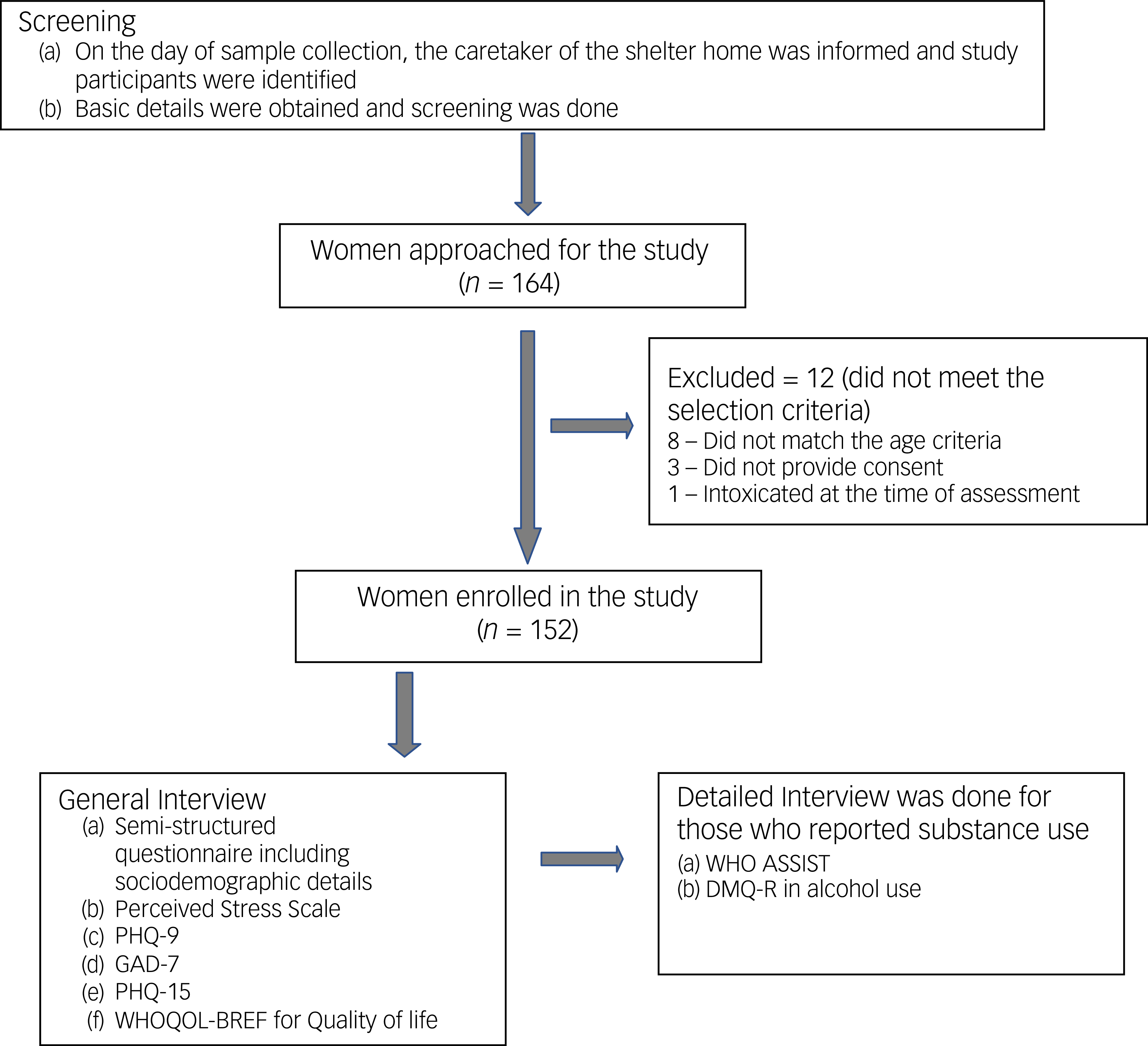
On the days of sample collection, the caretaker of the urban shelter home was informed to select homeless women for the survey. The caretakers selected participants based on their convenience and availability of women present in the shelter home, and informed them about the survey to be conducted. On the day of study, the staff/caretaker was informed and with the aid of the staff, the participants were approached. After screening the participants, informed consent was taken from those women who met the inclusion criteria and operational definitions as mentioned above. At any given time, approximately eight to ten women were present at a shelter home; however, it was not feasible to approach all of them on a single visit. Typically, two to three women were approached per visit, and based on the eligibility criteria, they were either included or excluded from the study. The total number of women approached was recorded, and those who declined participation were also documented as mentioned in Fig. 1.
Flowchart depicting study procedure. DMQ-R, Drinking Motive Questionnaire-Revised; GAD-7, Generalised Anxiety Disorder-7; PHQ-9, Patient Health Questionnaire-9; PHQ-15, Patient Health Questionnaire-15; WHO ASSIST, World Health Organization Alcohol, Smoking and Substance Involvement Screening Test version 3; WHOQOL-BREF, World Health Organization Quality-of-Life Scale.

Fig. 1 Long description
The flowchart illustrates the study procedure for a research study on homeless women. The process begins with screening, where the caretaker of the shelter home is informed and participants are identified. Basic details are obtained, and screening is done. Women approached for the study total 164. Twelve women are excluded for not meeting the selection criteria: eight did not match the age criteria, three did not provide consent, and one was intoxicated at the time of assessment. Women enrolled in the study total 152. The next step involves a general interview using a semi-structured questionnaire that includes sociodemographic details, the Perceived Stress Scale, PHQ-9, GAD-7, PHQ-15, and WHOQOL-BREF for quality of life. A detailed interview is conducted for those who report substance use, utilizing the WHO ASSIST and DMQ-R in alcohol use.
Individuals who provided informed consent were enrolled in the study, and sociodemographic details were collected using a semi-structured questionnaire. A pilot test was conducted among ten homeless women to assess the feasibility of the study, and the data from these participants were excluded from the final analysis reported in this manuscript.
Study instruments
Semi-structured questionnaire
A semi-structured questionnaire was specifically designed for the study and used to gather information on the sociodemographic details of the participants, details of homelessness and violence.
For those who had a history of substance use or are current substance users – a separate semi-structured questionnaire was used to collect information regarding (a) pattern and frequency of substance use, (b) complications related substance use, (c) treatment-seeking, (d) barriers to treatment-seeking and (e) past abstinence attempts.
Perceived Stress Scale
The Perceived Stress Scale (PSS) is a self-reported scale assessing the degree to which individuals perceive situations in their lives as stressful, and was used to evaluate the psychological stress experienced over the past 4 weeks. This ten-item scale uses a five-point Likert response format ranging from 0 (never) to 4 (very often). The scale demonstrates acceptable internal consistency. The Hindi version of the scale was used in the study. Reference Pangtey, Basannar, Sethi and Banerjee21
Patient Health Questionnaire-9
The Patient Health Questionnaire-9 (PHQ-9) is a self-reported scale used to assess the severity of depressive symptoms. Each item is rated on a four-point Likert scale, reflecting the presence of symptoms over the past 2 weeks. The Hindi version of the scale was used in the study. Reference Kroenke, Spitzer and Williams22
Generalised Anxiety Disorder-7
The seven-item Generalised Anxiety Disorder-7 (GAD-7) is a self-report scale (Hindi version), used to assess the severity of generalised anxiety disorder. Responses were rated on a four-point Likert scale based on the frequency of symptoms over the past 2 weeks. It has shown good reliability and validity across diverse populations. Reference Spitzer, Kroenke, Williams and Löwe23
Patient Health Questionnaire-15
The self-reported scale Patient Health Questionnaire-15 (PHQ-15) was used to assess the severity of somatic symptoms across 15 common physical complaints. It uses a three-point Likert scale to rate symptom distress over the past 4 weeks. Reference Kroenke, Spitzer and Williams24
World Health Organization Quality-of-Life Scale
The World Health Organization Quality-of-Life Scale (WHOQOL-BREF) is a self-reported measure of quality of life. It uses a five-point Likert scale to evaluate physical health, psychological health, social relationships, environment and overall quality of life. Reference Garcia-Rea and LePage25
World Health Organization Alcohol, Smoking and Substance Involvement Screening Test – Version 3.0
The World Health Organization Alcohol, Smoking and Substance Involvement Screening Test (WHO ASSIST) Version 3.0 is an eight-item clinician administered tool that identifies hazardous or harmful use of substances like tobacco, alcohol, cannabis, opioids and others. It assesses lifetime and recent use, related problems, attempts to cut down and injecting behaviour. In this study, the Hindi version of WHO ASSIST was used to categorise participants into low-, moderate- or high-risk groups. 26
Drinking Motive Questionnaire-Revised
The Drinking Motive Questionnaire-Revised (DMQ-R) is a 20-item self-reported scale assessing reasons for alcohol use across four domains, including social, coping, enhancement and conformity. Items are rated on a five-point Likert scale and it has good internal consistency. Reference Fernandes-Jesus, Beccaria, Demant, Fleig, Menezes and Scholz27 The instrument was translated using standard forward translation procedures and reviewed by bilingual mental health professionals; however, formal psychometric validation could not be undertaken within the scope of the thesis.
Statistical analysis
Data were organised and stored using Microsoft Excel spreadsheets. Descriptive statistics for continuous variables are presented as mean (s.d.) or median (interquartile range (IQR)), and categorical variables were summarised as frequencies and percentages. The Kolmogorov–Smirnov test was used to assess the normality of data distribution. Based on this, appropriate parametric or non-parametric tests were applied. For the purpose of comparison across variables, the total sample was divided into three groups: non-substance users (group 0); only tobacco use (group 1); and other substance users, i.e. who used alcohol or any other psychoactive substance besides tobacco (group 2). As the variables were non-normally distributed, a non-parametric test (Kruskal–Wallis test) was applied to compare the difference between these three groups. A p-value of <0.05 was considered statistically significant. Data were analysed using SPSS Statistics licensed version 29 (IBM Corp, Armonk, NY, USA).
Results
Of the 164 homeless women screened and approached, 152 met the inclusion criteria and were enrolled in the study (Fig. 1). The participation rate in the study was 92.7%. Twelve women were excluded: eight did not meet the age criteria, one was intoxicated at the time of assessment and three declined to provide consent. Thus, the final study sample comprised 152 homeless adult women.
Sociodemographic profile and details of homelessness
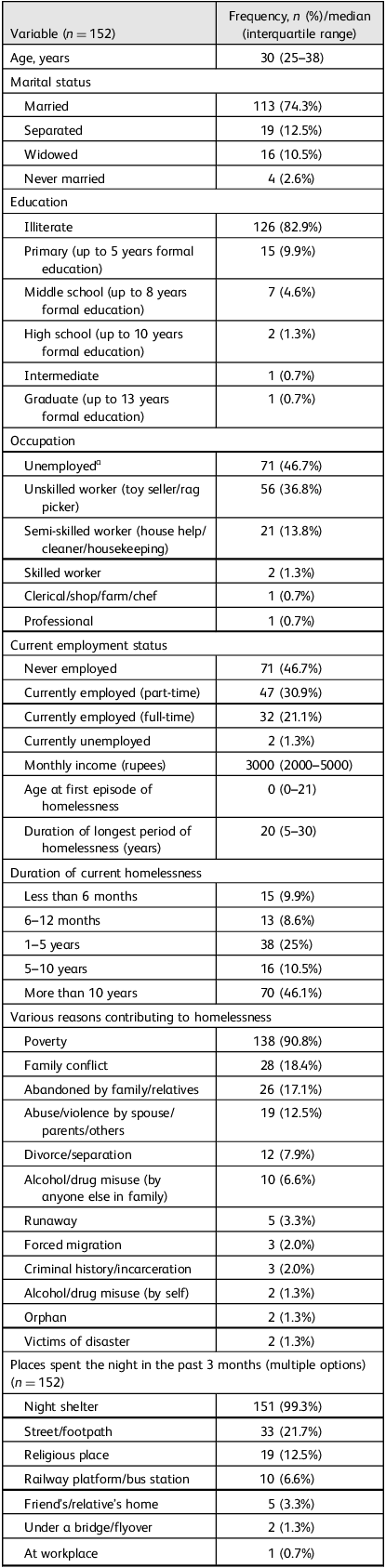
As shown in Table 1, the median age of participants was 30 (IQR: 25–38) years. Most of them were married (74.3%) and had no formal education (80%). The majority of them were homeless since birth, and nearly half of them reported homelessness (46.1%) for more than 10 years. Poverty was the most frequently cited reason for homelessness (90.8%), followed by family conflict (18.4%), abandonment (17.1%) and experiences of abuse or violence (12.5%). The majority (99.3%) had spent nights in night shelters in the past 3 months, and others also reported sleeping on streets, at religious places or transport hubs.
Sociodemographic variables and details of homelessness

Table 1 Long description
The table presents sociodemographic variables and details of homelessness among 152 participants. It includes data on age, marital status, education, occupation, current employment status, monthly income, age at first episode of homelessness, duration of longest period of homelessness, duration of current homelessness, various reasons contributing to homelessness, and places spent the night in the past 3 months. Key findings include a median age of 30 years, with most participants being married and having no formal education. Poverty is the most cited reason for homelessness, followed by family conflict and abandonment. The majority of participants have spent nights in night shelters.
a 36 participants were begging and 35 were homemakers.
Intimate partner violence
Out of 151 women who reported intimate partner violence, a significant number of homeless women reported emotional abuse (n = 92, 60.9%), physical violence (n = 90, 59.6%) and sexual violence (n = 63, 41.7%) from their intimate partners. Almost all of them reported suffering intimate partner violence more than three to four times or even more frequently (95.8%), compared with nearly four (5%) homeless women who reported experiencing it once or twice.
Other violence
Out of 152 homeless women, some of them reported verbal violence (n = 18, 11.8%), physical violence (n = 11, 7.2%) and sexual violence (n = 6, 3.9%) apart from their intimate partner, and reported the usual places of occurrence would be either shelter homes, workplaces or streets.
Substance use profile
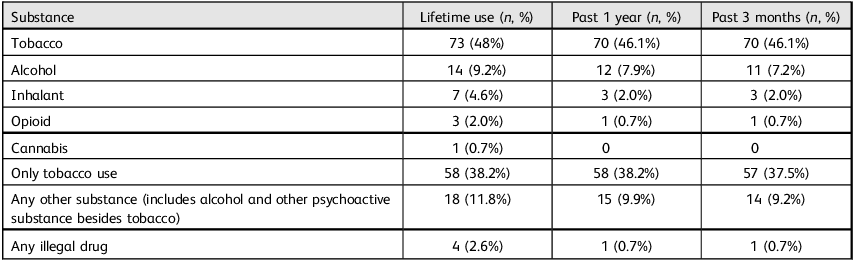
Among the 152 homeless women, tobacco was the most commonly used substance followed by alcohol, inhalants and opioids, in past 3 months. Table 2 depicts the pattern of substance use in homeless women (lifetime use, use in the past year, use in the past 3 months). None of the participants reported use of amphetamine, hallucinogen or sedative/hypnotics.
Substance use profile of the participants: use (n = 152)

Table 2 Long description
The table presents data on substance use among 152 homeless women, detailing lifetime use, past year use, and past 3 months use. The substances listed include tobacco, alcohol, inhalant, opioid, and cannabis. The table also categorizes only tobacco use, any other substance use, and any illegal drug use. Tobacco is the most commonly used substance, with 48 percent of participants reporting lifetime use, 46.1 percent in the past year, and 46.1 percent in the past 3 months. Alcohol follows, with 9.2 percent lifetime use, 7.9 percent in the past year, and 7.2 percent in the past 3 months. Inhalant use is reported by 4.6 percent lifetime, 2 percent in the past year, and 2 percent in the past 3 months. Opioid use is noted by 2 percent lifetime, 0.7 percent in the past year, and 0.7 percent in the past 3 months. Cannabis use is reported by 0.7 percent lifetime, with no use in the past year or past 3 months. Only tobacco use is reported by 38.2 percent lifetime, 38.2 percent in the past year, and 37.5 percent in the past 3 months. Any other substance use is reported by 11.8 percent lifetime, 9.9 percent in the past year, and 9.2 percent in the past 3 months. Any illegal drug use is reported by 2.6 percent lifetime, 0.7 percent in the past year, and 0.7 percent in the past 3 months.
Participants reporting substance use apart from tobacco included alcohol and other psychoactive substances, with 18 participants (11.8%) reporting lifetime use, 15 (9.9%) reporting use in the past year and 14 (9.2%) reporting use in the past 3 months.
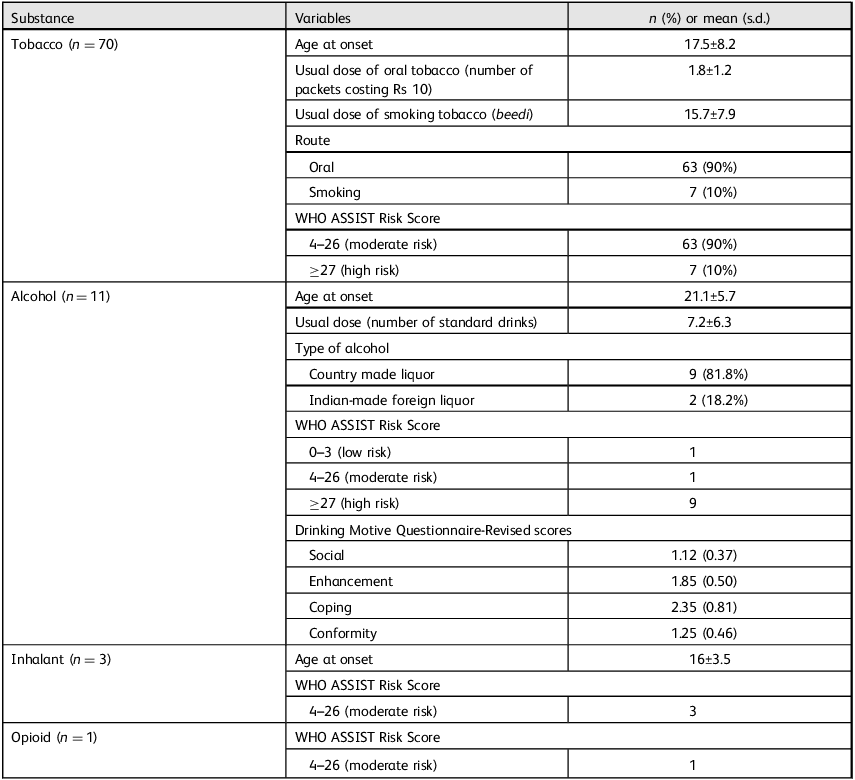
Assessment using the WHO ASSIST was conducted for participants who reported substance use in the past 3 months, as depicted in Table 3. Among homeless women who were using tobacco in the past 3 months (n = 70), the majority (90%) scored moderate risk in WHO ASSIST severity score. The mean age of initiation was 17.5 years, and most users (90%) used smokeless tobacco, averaging 1.8 packets per day. The rest (10%) smoked tobacco, consuming an average of 15.7 beedis per day.
Substance use profile of the participants: variables

Table 3 Long description
The table presents the substance use profile of homeless women, detailing their use of tobacco, alcohol, inhalants, and opioids. For tobacco users (n=70), the mean age at onset is 17.5 years, with a usual dose of 1.8 packets of oral tobacco or 15.7 beedis for smokers. Most users (90%) are at moderate risk. For alcohol users (n=11), the mean age at onset is 21.1 years, with a usual dose of 7.2 standard drinks, predominantly consuming country-made liquor, and most (81.8%) are at high risk. Inhalant users (n=3) have a mean age at onset of 16 years, all at moderate risk. The single opioid user is also at moderate risk. The table includes variables such as age at onset, usual dose, route, type, and risk levels, with specific data for each substance.
Comparison of psychological well-being

Table 4 Long description
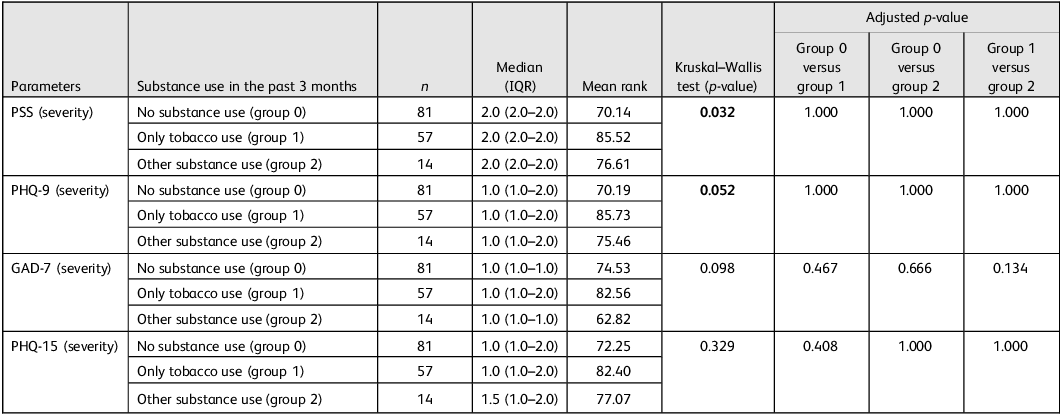
The table compares psychological well-being across different substance use groups, including no substance use, only tobacco use, and other substance use. It has five rows and eight columns. The columns are labeled Parameters, Substance use in the past 3 months, n, Median (IQR), Mean rank, Kruskal-Wallis test (p-value), and Adjusted p-value with sub-columns Group 0 versus group 1, Group 0 versus group 2, and Group 1 versus group 2. The rows are labeled PSS (severity), PHQ-9 (severity), GAD-7 (severity), and PHQ-15 (severity). The table shows the median (IQR), mean rank, and p-values for each group. A p-value of <0.05 was considered statistically significant and is represented in bold. Notable trends include significant p-values for PSS and PHQ-9 severity, indicating differences in psychological well-being among the groups.
IQR, interquartile range; PSS, Perceived Stress Scale; PHQ-9, Patient Health Questionnaire-9; GAD-7, Generalised Anxiety Disorder-7; PHQ-15, Patient Health Questionnaire-15. Bold text indicates statistical significance (p < 0.05).
Among the 11 homeless women who were using alcohol in the past 3 months, nine (81.8%) belonged to the high-risk group. The most commonly consumed was country-made liquor with an average of 7.2 standard drinks per day. Drinking motives assessed using the DMQ-R showed the highest mean score for coping 2.35 (s.d. 0.81), followed by enhancement 1.85 (s.d. 0.50), conformity 1.25 (s.d. 0.46) and social 1.12 (s.d. 0.37). Three participants reported inhalant use, and all of them were assessed to be at moderate risk as per the WHO ASSIST score. One participant reported opioid use at nearly 12 years of age, involving both prescription opioids and injected heroin, as well as sharing and reusing needles. Among 14 users of alcohol, inhalants or opioids in the past 3 months, nine (64.3%) reported physical symptoms (weakness and loss of appetite), and two (14.3%) were involved in illegal activities.
The majority of the participants expressed their desire to quit the substance. However, several challenges were reported, including craving and withdrawal, stress, peer pressure, substance availability and difficulty surviving on the street without the substance. Out of 71 participants who reported substance use in the past 3 months, only three (4.2%) had ever sought treatment.
Depression, anxiety and stress
Psychological well-being tools like the PSS were used for assessing perceived stress, the PHQ-9 for assessing depression, the PHQ-15 for assessing somatic symptoms and the GAD-7 for assessing anxiety; these was applied to all the participants, including those who were using substances.
More than 80% participants reported moderate to severe stress on the PSS. PHQ-9 results indicated that 5% had moderate to severe depression symptoms, 20.4% had mild depressive symptoms and 65.8% had minimal depressive symptoms. The PHQ-15 results showed that 5.9% of women had high severity of somatic symptoms, 9.9% had medium severity of somatic symptoms, around 60% had minimal somatic symptoms and 28.3% had low somatic symptoms. In the GAD-7 scale, 2% reported moderate to severe anxiety, 23% reported mild anxiety and 75% reported minimal anxiety.
Quality of life
Overall quality of life varied, with median scores across the WHOQOL-BREF domains of 50 (IQR: 44–56) for physical health, 50 (IQR: 38–63) for psychological, 31 (IQR: 25–56) for social relationships and 44 (IQR: 38–56) for environmental health.
Comparison of psychological well-being across homeless women who had and had not used substances in the past 3 months
For the purpose of comparison across these variables, the total sample was divided into three groups based on the past 3 months: no substance use (group 0, n = 81); only tobacco use (group 1, n = 57); and other substance use, i.e. who used alcohol or any other psychoactive substance besides tobacco (group 2, n = 14).
As shown in Table 4, among homeless women, those with no substance use had lower median severity scores on the PHQ-9, PSS and PHQ-15 than women using tobacco or other substances. The overall Kruskal–Wallis test suggested differences for the PSS and PHQ-9, but pairwise comparison did not remain statistically significant after Holm–Bonferroni correction.
Barriers to help-seeking behaviour
Among homeless women who reported any substance use in the past three months (n = 71), the most frequent barrier to help-seeking was inadequate knowledge about available services (n = 57, 80.2%), followed by a perceived absence of problems (n = 17, 23.9%), disbelief in treatment (n = 4, 5.6%) and cost-related barriers (n = 1, 1.4%).
For general healthcare services (n = 140), the most cited barriers were cost (n = 114, 81.4%) and distance to healthcare facilities (n = 111, 79.3%), highlighting the financial and logistical challenges faced by this population. Additionally, past negative experiences with health services were reported by half of the participants (n = 71, 50.7%); fewer participants mentioned lack of expertise (n = 24, 17.1%) or gender-related concerns (n = 1, 0.7%) as barriers.
In the context of reproductive health (n = 101), nearly half of the women (n = 49, 48.5%) reported lack of knowledge as a key reason for not seeking care. Other barriers included normalising reproductive problems (n = 13, 12.9%), apprehension about treatment facilities (n = 2, 1.9%) and issues such as being unable to take leave from work, lack of transportation and financial constraints, each reported by 1% of participants.
Discussion
This cross-sectional observational study is the first comprehensive study conducted in India that has explored the patterns and proportion of substance use among homeless women, as well as their mental well-being and quality of life, using structured tools, among those residing in the urban shelter homes in Delhi, India.
We found that a high percentage of homeless women are using tobacco and alcohol in a high-risk pattern. The rates are much higher than those reported in the general population in large epidemiological surveys from India; namely, the Magnitude of Substance Use Survey 2019, National Family Health Survey-5, National Mental Health Survey-1 and Global Adult Tobacco Survey-2. Reference Ambekar, Agrawal, Rao, Mishra, Khandelwal and Chadda28–31 A higher rate of use among homeless people could be attributed to the easy availability of the substance in the community or an easy adaptation to the high level of stress one undergoes while living in shelter homes. This is also evident from the fact that more than 83% women from our study population reported moderate to high stress. Previous studies from other countries also report higher rates of substance use, such as alcohol, tobacco and other drugs, among homeless people. Reference Johnson and Fendrich32 Often, the substance use could also be because of the network of people they engage with when working, or the connections they make or their partners using substances. Studies have shown that such networks or social influences may exert pressure on women, which can lead to the initiation and maintenance of substance use. Reference Tucker, D’Amico, Wenzel, Golinelli, Elliott and Williamson33,Reference Manuel, McCrady, Epstein, Cook and Tonigan34 These personal networks may include abusive sexual partners, which can often lead to substance use just to deal with the emotional distress related to trauma. It is often noted that intimate partner violence is an important predictor for substance use in homeless women. Reference Salomon, Bassuk and Huntington35 Our study reports a higher prevalence of intimate partner violence. These findings suggest the need for tailored approaches and focused research in this marginalised population.
A quarter of the participants reported clinically relevant symptoms of depression and anxiety, and more than 80% reported moderate-to-high levels of perceived stress, indicating a substantial mental health burden in this population. Studies conducted elsewhere also reflect a higher prevalence of psychiatric symptoms among homeless women, with global data indicating that 20–50% of homeless women experience major depression. Reference Chambers, Chiu, Scott, Tolomiczenko, Redelmeier and Levinson36–Reference Goodman, Smyth and Banyard38 As per the National Mental Health Survey-1 (NMHS-1) 2015–16, the current prevalence of mental morbidity in women in the general population was nearly 7.5%, which is more or less similar to the current study findings (5% reported moderate to severe depression, 2% reported moderate anxiety and 23% reported mild anxiety). Reference Gururaj, Varghese, Benegal, Rao, Pathak and Singh30 Although studies conducted elsewhere reported a higher prevalence of psychiatric symptoms, we found that an overwhelming population of women reported significant stress. Some of the factors that could have attributed to these findings would be lack of insight into their mental health problems, internalising the trauma or fear of labelling.
Overall, the findings suggest that screening, timely awareness of mental health problems and stress management in shelter homes should be incorporated in a structured way. On the other hand, the findings also imply that having a good social network and having shelter home where once could reside and discuss about their problems with other residents could mitigate some of the distress. Studies have reported that a positive social network and social support are linked to a decrease in psychological symptoms and greater engagement in mental health services. Reference Maulik, Eaton and Bradshaw39
It is worthwhile to note that the majority of the study participants were homeless since birth, which suggests that unstable housing can be associated with vulnerabilities like substance use and psychiatric illness, such as stress, anxiety and depression, thus indicating the need for appropriate mental health and addiction treatment services. Various factors, such as abuse or violence, chronic stress, lack of social support and social exclusion, can lead to stress, anxiety or depressive symptoms. A lack of support, compounded by poverty, can further undermine healthy coping mechanisms. The overall quality of life of the participants was poor, with scores being lowest in the social and environmental domains compared with the physical and psychological health domains, potentially because of a lack of social support, chronic substance use, mental health conditions and homelessness. Reference Gadermann, Hubley, Russell, Thomson, Norena and Rossa-Roccor40,Reference Konrady and Talarska41 Hence, a comprehensive approach and integrated care are required to address the quality of life and mental health problems.
The study also reports certain barriers to help-seeking behaviour in terms of healthcare services, reproductive health and substance use treatment. Overall, the most common barriers cited were lack of knowledge, financial and logistical constraints, followed by past negative experiences, low perceived need and disbelief in treatment. The majority of the homeless women in the study were illiterate, which could hinder their knowledge of help-seeking behaviour. At the same time, poverty, which was cited as the most common reason for homelessness in the study, would have been a contributing factor to not seeking help. Other reasons could include discrimination, stigma or a fear of negative experiences, which may have discouraged them from seeking further help. Studies conducted elsewhere also reported similar reasons in addition to psychiatric illness, which hindered their help-seeking behaviour. Reference Upshur, Jenkins, Weinreb, Gelberg and Orvek42–Reference Gelberg, Browner, Lejano and Arangua45
It is important to note that the population of interest in our study was residing in shelter homes, a condition that may serve as a protective factor compared with those who were living on the streets. Evidence suggests that shelter homes can ease the stress of housing, protect against violence and enhance mental health outcome. Reference Yakubovich, Bartsch, Metheny, Gesink and O’Campo46 Homeless women who do not have any shelter home or transitional housing may even face worse outcome in terms of substance use and psychological symptoms. Studies have reported women living on the streets are at greater risk for poorer physical and mental health, as well as substance use, compared with those who are residing in shelter homes. Reference Leake and Lillian47,Reference Richards and Kuhn48
Although the problems remain multi-layered, they need to be addressed. Some possible interventions that could ameliorate the situation are providing basic education, engaging homeless women with small organisations for employment, providing education and awareness regarding general health, reproductive health, pre-pregnancy counselling, educating about early signs of mental illness, availability of general healthcare services and substance use treatment in the shelter homes. One-stop integrated models for women who use drugs have been found to be effective in providing comprehensive harm reduction services in the Indian context. Reference Rao49 Such centres should be further scaled up with the provision of treatment for common mental and physical illnesses, as well as linkages to social welfare schemes, in addition to comprehensive harm reduction measures.
The current study has some limitations. As this study was limited to urban shelter homes in Delhi, its findings may not accurately represent the general population, which could affect the generalisability of the results. The use of convenience sampling may have introduced selection bias. Reliance on self-reported data may have led to underreporting, especially of sensitive issues like mental health and substance use. Logistical constraints in shelter settings, such as limited privacy and time, may have influenced the quality of responses.
To conclude, this study highlights the significant burden and underreporting of mental health issues and substance use among homeless women residing in shelter homes. The study emphasises the need for integrated, gender-sensitive and context-specific interventions targeting the complex interplay between homelessness, mental health and substance use. Future research should explore trauma-informed care, housing interventions and early prevention strategies, which are crucial for designing effective, gender-sensitive support systems.
Data availability
The data-sets generated during the current study area available from the corresponding author, A. Agrawal, on reasonable request.
Acknowledgements
We sincerely thank Dr Rajesh Kumar, Executive Director of the Society for Promotion of Youth and Masses (SPYM), for his invaluable leadership and support in managing shelter homes in Delhi, India.
Author contributions
P. Saha contributed to study conceptualisation, data curation, methodology, software, formal analysis, validation and visualisation, writing the original draft, and reviewing and editing the manuscript. A. Ambekar contributed to study conceptualisation, methodology, resources, supervision, data curation, validation and visualisation, and reviewing and editing the manuscript. S.S. contributed to study supervision, validation and visualisation, and reviewing and editing the manuscript. P. Sevda and A.P. reviewed and edited the manuscript. A. Agrawal contributed to study conceptualisation, project administration, methodology, resources, data curation, supervision, validation and visualisation, and reviewing and editing the manuscript.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.

 Open access
Open access
eLetters
No eLetters have been published for this article.