



Impact statements
The present review brings together global evidence showing that climate change is not only an environmental threat but also a growing driver of suicide risk. Across diverse countries and populations, the findings demonstrate that higher temperatures, heatwaves, air pollution and extreme weather events such as floods and droughts are consistently linked to increases in suicidal behaviour, particularly fatal suicide. As these climate stressors become more frequent and intense, their influence on population mental health is likely to increase further. The results show that climate-related suicide risk is not uniform across society. Older adults, people with pre-existing mental health conditions, pregnant women and individuals exposed to severe environmental stress appear especially vulnerable. Seasonal and temperature-related effects are also evident, highlighting how changes in daily living conditions can affect psychological stability and crisis risk. The review also exposes a major equity concern. Most of the existing evidence comes from high-income countries, even though many of the most severe climate shocks occur in LAMICs, where social protection systems and mental health services are often weakest. This imbalance means that the people who are likely to be most affected by climate-related distress and suicide risk are also those least represented in the scientific literature. Importantly, the review supports concrete actions that can be implemented now. These include linking heat and air-quality warning systems with mental health services, establishing cooling centres during extreme heat and integrating mental health and electronic mental health support (eMHPSS) into disaster preparedness and response. Such measures have the potential to reduce psychological distress and prevent loss of life during climate-related emergencies. By clearly demonstrating that climate change is a direct suicide-prevention issue, this paper strengthens the case for embedding mental health protection within climate adaptation, public health policy and disaster risk-reduction strategies worldwide.
Introduction
Climate change represents one of the most significant challenges of our era, with substantial potential impacts on human beings (Rocha et al., Reference Rocha, Oliveira, Viana and Ribeiro2022). Climate change refers to long-term changes in local, global or regional temperatures and weather caused by human activity. (Shivanna, Reference Shivanna2022) Over the years, human life, flora and fauna have coexisted and developed within an environment that has experienced relatively stable climatic conditions, particularly in terms of temperature, humidity and solar radiation. Although there have been notable historical exceptions such as ice ages, medieval catastrophes and major natural disasters such as earthquakes and plagues, these events were either localized or occurred over extended periods, allowing some level of adaptation. As a result, the capacity of humans, plants and animals to adapt to sudden or extreme climatic changes, such as those driven by contemporary global warming, remains inherently limited. According to the results of the Lancet countdown in Europe, the impact of climate change on health is already clear throughout Europe. With the increase in frequent severe weather events, these impacts become increasingly evident, putting environmental conditions at risk from factors that cause the spread of infectious diseases and cause disruption of the water and food systems. (Romanello et al., Reference Romanello, van Daalen, Anto, Dasandi, Drummond, Hamilton, Jankin, Kendrovski, Lowe, Rocklöv, Schmoll, Semenza, Tonne and Nilsson2021) Climate change manifests itself in various forms, including acute weather events or natural disasters that occur over a few days, such as hurricanes, wildfires, floods and short-term heatwaves. It also includes subacute events that persist for months or a few years, such as droughts (Bell et al., Reference Bell, Brown, Conlon, Herring, Kunkel, Lawrimore, Luber, Schreck, Smith and Uejio2018). Furthermore, there are long-lasting changes that could extend until the end of the century, such as higher temperatures, extensive melting of glaciers, rising sea levels and the potential emergence of inhabitable physical environments due to permanent alterations (Global Change and Future Earth: The Geoscience Perspective – Google Books, n.d.). The World Health Organization (WHO) has put forward five key global research priorities to protect human health from the impact of climate change. These priorities include evaluating the risks involved, identifying the most effective interventions, providing guidance for health-promoting measures in other sectors, improving decision support systems and estimating the costs associated with protecting health from climate change (WHO, 2009).
The consequences of climate change have profound effects on individuals; people experience exposures and events that include mental health consequences that range from relatively mild stress symptoms to diagnosed psychiatric disorders. (Ebi et al., Reference Ebi, Balbus, Luber, Bole, Crimmins, Glass, Saha, Shimamoto, Trtanj and White-Newsome2018; Hayhoe et al., Reference Hayhoe, Wuebbles, Easterling, Fahey, Doherty, Kossin, Sweet, Vose and Wehner2018) For example, prolonged increases in average temperature have been associated with serious adverse outcomes, including higher rates of suicide, increased violence or aggression and poorer self-reported mental health. (Basu et al., Reference Basu, Gavin, Pearson, Ebisu and Malig2018; Burke et al., Reference Burke, González, Baylis, Heft-Neal, Baysan, Basu and Hsiang2018; Mullins and White, Reference Mullins and White2019) Extreme weather events are associated with increased frequency and duration, including heatwaves, storms, droughts, wildfires, heavy rainfall, floods, tropical storms and storm surges, and these combined or independent events are associated with post-traumatic stress disorder (PTSD), depression, mood disorders, anxiety and an increased risk of violence. (Vins et al., Reference Vins, Bell, Saha and Hess2015; Dodgen et al., Reference Dodgen, Donato, Kelly, Greca, Morganstein, Reser, Ruzek, Schweitzer, Shimamoto, Tart and Ursano2016) Extreme weather can also contribute to disturbing activities that people display outside to relieve stress. Also, such conditions lead people to stay inside, causing even more mental health problems for individuals (Dodgen et al., Reference Dodgen, Donato, Kelly, Greca, Morganstein, Reser, Ruzek, Schweitzer, Shimamoto, Tart and Ursano2016).
Despite growing evidence linking climate indicators such as rising temperatures, extreme weather events and air pollution to mental health problems, including suicidality, existing research remains fragmented. In the present review, suicidality is used as an umbrella term encompassing a spectrum of suicide-related outcomes, including suicidal ideation (thoughts of ending one’s life), suicide attempts (non-fatal, self-injurious behaviour with intent to die) and suicide completion (death by suicide). Most studies originate from high-income countries, while low- and middle-income countries (LAMICs) where climate stressors are often more severe remain underrepresented. Furthermore, prior studies vary widely in methodology, exposure measures and populations studied, limiting the comparability of findings. Few studies have synthesized these diverse results to provide a global perspective on how climate change influences suicide risk. Addressing this gap is essential to inform mental health policy, guide suicide prevention strategies and identify priorities for future research. Therefore, this review systematically examines the evidence on climate change and suicidality, highlighting global patterns, methodological challenges and critical gaps in knowledge.
Method
Study protocol and registration
The current systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (Page et al., Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl, Brennan, Chou, Glanville, Grimshaw, Hróbjartsson, Lalu, Li, Loder, Mayo-Wilson and McDonald2021a). (See Appendix).The protocol for this systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) with the registration number CRD42024539305.
Data collection and search strategy
We conducted a comprehensive literature search across five electronic databases and search engines: PubMed, Scopus, PsycINFO, Web of Science and Google Scholar. The search strategy combined terms for climate change with terms for suicidality, using Boolean operators and truncation to capture variations. For example, the PubMed search string was: (“climate change” OR “global warming” OR “temperature” OR “heatwave” OR “air pollution” OR “extreme weather” OR “flood” OR “drought”) AND (“suicide” OR “suicidal ideation” OR “suicide attempt” OR “self-harm” OR “self-injurious behavior”). The suicidality construct was operationalized broadly to include ideation, attempts and completed suicides, ensuring that studies addressing any stage of suicidality were captured. No restrictions were applied regarding study setting or population. Reference lists of included articles and relevant reviews were also manually screened to identify additional studies.
Eligibility criteria
Inclusion criteria
The inclusion criteria were: (1) peer-reviewed studies using quantitative data that examined the link between climate change and suicidality, (2) studies focusing on how climate indicators such as rising temperatures and extreme weather events influence the risk of suicide, (3) observational studies and randomized controlled trials and (4) studies published in English.
The exclusion criteria
Exclusion criteria were non-peer-reviewed studies, conference abstracts, editorials, reviews, studies not related to climate change and suicide rates, studies focused solely on mental health disorders without addressing suicide, qualitative studies without quantitative data and studies published in languages other than English. During screening, a small number of qualitative papers were identified; however, these were largely narrative in nature, discussing the general impact of climate change on mental health without providing empirical data, statistical testing or suicide-specific outcomes. The focus on quantitative studies was chosen to allow for the assessment of measurable associations between climate indicators and suicidality outcomes using effect size estimates and statistical parameters that could be meaningfully compared across studies. Mixed-methods studies were considered eligible only when the quantitative component could be clearly extracted and independently analysed; however, none met this criterion during full-text screening. While qualitative research provides valuable contextual and experiential insights, it was excluded because it does not permit quantitative synthesis of risk or exposure effects.
Study screening
The study screening process was carried out by two independent researchers (S.K.K and M.D.A), who reviewed the titles and abstracts of the identified articles for eligibility using the Rayyan AI platform (Ouzzani et al., Reference Ouzzani, Hammady, Fedorowicz and Elmagarmid2016), which helped streamline the screening process by allowing efficient sorting of articles based on predefined inclusion and exclusion criteria. They then performed a full-text screening based on these criteria. Subsequently, the lead author (D.R.A) performed a secondary screening to ensure that all studies met the inclusion criteria. Disagreements between the two screeners were minimal and were resolved through discussion with the lead author (D.R.A), ensuring consistency and accuracy in the study selection process.
Data extraction
Data extraction was conducted using a standardized form that captured key study characteristics, including the first author’s name, publication year, study country, study period, design, population, sample size, gender, age, climate change and suicide measurements, type of climate exposure and main findings. The detailed characteristics of the included studies are presented in Table 1.
Characteristics of the included studies, measurements of climate and suicide, types of climate exposure and main findings

Assessment of risk of bias
The risk of bias assessment was performed based on the included research design; we applied two different tools for the quality assessment of the included articles in the present review. We used the Mixed Methods Appraisal Tool (MMAT) (Hong et al., Reference Hong, Pluye, Fàbregues, Bartlett, Boardman F, Cargo, Dagenais, Gagnon, Griffiths, Nicolau, O’Cathain, Rousseau and Vedel2019) because there are studies with different designs and no exposure. We evaluated the research question, study design, sample size, data collection and statistical analysis using MMAT. We also used the ROBINS-E (risk of bias in nonrandomized studies of exposures) tool (Higgins et al., Reference Higgins, Morgan, Rooney, Taylor, Thayer, Silva, Lemeris, Akl, Bateson, Berkman, Glenn, Hróbjartsson, LaKind, McAleenan, Meerpohl, Nachman, Obbagy, O’Connor and Radke2024) because it is specifically designed to assess the risk of bias in nonrandomized observational studies that evaluate exposures rather than interventions. Observational studies often face unique challenges compared to randomized controlled trials (RCTs), such as confounding, selection bias and measurement errors.
Data synthesis and analysis
We performed a systematic narrative analysis, which allowed us to summarize and interpret the data while identifying patterns, trends and recurring themes in the relationship between climate variables and suicidality. A meta-analysis was not performed due to substantial heterogeneity in study designs, measurement approaches, populations, climate exposures and suicidality outcomes, which precluded meaningful pooling of effect sizes. Narrative synthesis was therefore deemed the most appropriate approach to integrate the findings across diverse methodologies and contexts.
Results
Study selection process
A total of 748 articles were identified through a comprehensive search, including PubMed, Scopus, PsycINFO, Web of Science and Google Scholar. After removing 343 duplicates, the remaining 405 articles underwent title and abstract screening, leading to the exclusion of 286 articles that did not meet the inclusion criteria for example, studies focusing on climate change and general mental health outcomes without reporting suicidality, or studies limited to physical health impacts. The full texts of the remaining 119 articles were reviewed, resulting in the exclusion of 76 articles due to ineligible criteria (49), assessment of psychosocial aspects without suicide (17), insufficient data (7) and narrative studies (3). Ultimately, 43 articles met the inclusion criteria and were included in the review, as presented in the PRISMA flow diagram (Figure 1).
PRISMA flowchart of the study selection.

Study characteristics
The included studies came from a range of countries and regions. The United States contributed seven studies (Bakian et al., Reference Bakian, Huber, Coon, Gray, Wilson, McMahon and Renshaw2015b; Burke et al., Reference Burke, González, Baylis, Heft-Neal, Baysan, Basu and Hsiang2018; Bergmans et al., Reference Bergmans, Larson, Bennion, Mezuk, Wozniak, Steiner and Gronlund2021; Cheng et al., Reference Cheng, Plouffe, Nanos, Qamar, Fisman and Soucy2021; Rahman et al., Reference Rahman, Lorenzo, Ban-Weiss, Hasan, Azzouz, Eckel, Conti, Lurmann, Schlaerth, Johnston, Ko, Palinkas, Hurlburt, Silva, Gauderman, McConnell and Garcia2023; Freichel & O’Shea, Reference Freichel and O’Shea2023; Runkle et al., Reference Runkle, Sugg, Berry, Reed, Cowan, Wertis and Ryan2024), Italy five (Preti, Reference Preti1997; Reference Preti1998 ; Preti et al., Reference Preti, Lentini and Maugeri2007; Rocchi et al., Reference Rocchi, Sisti, Cascio and Preti2007; Di Nicola et al., Reference Di Nicola, Mazza, Panaccione, Moccia, Giuseppin, Marano, Grandinetti, Camardese, De Berardis, Pompili and Janiri2020; Aguglia et al., Reference Aguglia, Giacomini, Montagna, Amerio, Escelsior, Capello, Cutroneo, Ferretti, Scafidi, Costanza, Serafini and Amore2021) Turkey four (Doganay et al., Reference Doganay, Tevfik Sunter, Guz, Ozkan, Altintop, Kati, Colak, Aygun and Guven2003; Akkaya-Kalayci et al., Reference Akkaya-Kalayci, Vyssoki, Winkler, Willeit, Kapusta, Dorffner and Özlü-Erkilic2017; Asirdizer et al., Reference Asirdizer, Kartal, Etli, Tatlisumak, Gumus, Hekimoglu and Keskin2018; Kayipmaz et al., Reference Kayipmaz, San, Usul and Korkut2020), Australia three (Matthews et al., Reference Matthews, Longman, Berry, Passey, Bennett-Levy, Morgan, Pit, Rolfe and Bailie2019; Edwards et al., Reference Edwards, Taylor and Gray2023; Hertzog et al., Reference Hertzog, Charlson, Tschakert, Morgan, Norman, Pereira and Hanigan2024), Germany three (Müller et al., Reference Müller, Biermann, Renk, Reulbach, Ströbel, Kornhuber and Sperling2011; Schneider et al., Reference Schneider, Hampel, Ladwig, Baumert, Lukaschek, Peters and Breitner2020; Brailovskaia and Teismann, Reference Brailovskaia and Teismann2024), Finland two (Helama et al., Reference Helama, Holopainen and Partonen2013; Hiltunen et al., Reference Hiltunen, Haukka, Ruuhela, Suominen and Partonen2014), Canada two (Villeneuve et al., Reference Villeneuve, Huynh, Lavigne, Colman, Anisman, Peters and Rodríguez-Villamizar2023; Freichel & O’Shea, Reference Freichel and O’Shea2023) and the rest from other European, Asian and Latin American countries. Most of the included articles were retrospective in design, with a few exceptions where case-crossover (Bakian et al., Reference Bakian, Huber, Coon, Gray, Wilson, McMahon and Renshaw2015a; Lee et al., Reference Lee, Jung, Myung, Baek, Kang, Kim and Kim2019; Bergmans et al., Reference Bergmans, Larson, Bennion, Mezuk, Wozniak, Steiner and Gronlund2021; Rahman et al., Reference Rahman, Lorenzo, Ban-Weiss, Hasan, Azzouz, Eckel, Conti, Lurmann, Schlaerth, Johnston, Ko, Palinkas, Hurlburt, Silva, Gauderman, McConnell and Garcia2023; Villeneuve et al., Reference Villeneuve, Huynh, Lavigne, Colman, Anisman, Peters and Rodríguez-Villamizar2023; Lian et al., Reference Lian, Wang, Guo, Wan, Ye, Zhou, Han, Yu, Huang and Li2024; Runkle et al., Reference Runkle, Sugg, Berry, Reed, Cowan, Wertis and Ryan2024), cross-sectional (Matthews et al., Reference Matthews, Longman, Berry, Passey, Bennett-Levy, Morgan, Pit, Rolfe and Bailie2019; Di Nicola et al., Reference Di Nicola, Mazza, Panaccione, Moccia, Giuseppin, Marano, Grandinetti, Camardese, De Berardis, Pompili and Janiri2020; Miyazaki et al., Reference Miyazaki, Hino, Ito, Abe, Nomoto, Furuno, Takeuchi and Hishimoto2023; Ndetei et al., Reference Ndetei, Wasserman, Mutiso, Shanley, Musyimi, Nyamai, Munyua, Swahn, Weisz, Osborn, Bhui, Johnson, Pihkala, Memiah, Gilbert, Javed and Sourander2024), case control (Makris et al., Reference Makris, White, Reutfors, Ekselius, Andersen and Papadopoulos2021) and descriptive survey (Kayipmaz et al., Reference Kayipmaz, San, Usul and Korkut2020) designs were used. Although several included articles were published in 2024, the study periods and datasets they analysed covered years up to 2023, with durations ranging from a few months (Edwards et al., Reference Edwards, Taylor and Gray2023) to more than 50 years (Helama et al., Reference Helama, Holopainen and Partonen2013). Participants were exposed to a varying number of climate types, including extreme weather, high temperature, rainfall, air pollutants, flooding and humidity with suicidal behaviour ranging from mere ideation to complete/fatal suicide. The detailed characteristics of the included studies are presented in Table 1.
Participants
Studies covered a diverse population, with the general population being the group most frequently examined, followed by university students, employees, high school students, pregnant women, older adults (≥65 years), suicidal individuals, adolescents and those with mental illnesses such as bipolar disorder. Sample sizes varied widely, ranging from small cohorts of a few hundred participants to large-scale studies involving tens of thousands. Although some included more than 20,000 participants (Preti, Reference Preti1997; Preti et al., Reference Preti, Lentini and Maugeri2007; Rocchi et al., Reference Rocchi, Sisti, Cascio and Preti2007; Asirdizer et al., Reference Asirdizer, Kartal, Etli, Tatlisumak, Gumus, Hekimoglu and Keskin2018; Lee et al., Reference Lee, Jung, Myung, Baek, Kang, Kim and Kim2019; Bozsonyi et al., Reference Bozsonyi, Lester, Fulop, Zonda and Balint2020; Rahman et al., Reference Rahman, Lorenzo, Ban-Weiss, Hasan, Azzouz, Eckel, Conti, Lurmann, Schlaerth, Johnston, Ko, Palinkas, Hurlburt, Silva, Gauderman, McConnell and Garcia2023; Villeneuve et al., Reference Villeneuve, Huynh, Lavigne, Colman, Anisman, Peters and Rodríguez-Villamizar2023), the majority were limited to only 2000 (Deisenhammer et al., Reference Deisenhammer, Kemmler and Parson2003; Doganay et al., Reference Doganay, Tevfik Sunter, Guz, Ozkan, Altintop, Kati, Colak, Aygun and Guven2003; Müller et al., Reference Müller, Biermann, Renk, Reulbach, Ströbel, Kornhuber and Sperling2011; Bakian et al., Reference Bakian, Huber, Coon, Gray, Wilson, McMahon and Renshaw2015a; Fernández-Arteaga et al., Reference Fernández-Arteaga, Tovilla-Zárate, Fresán, González-Castro, Juárez-Rojop, López-Narváez and Hernández-Díaz2016; Akkaya-Kalayci et al., Reference Akkaya-Kalayci, Vyssoki, Winkler, Willeit, Kapusta, Dorffner and Özlü-Erkilic2017; Fernández-Niño et al., Reference Fernández-Niño, Astudillo-García, Rodríguez-Villamizar and Florez-Garcia2018; Matthews et al., Reference Matthews, Longman, Berry, Passey, Bennett-Levy, Morgan, Pit, Rolfe and Bailie2019; Koszewska et al., Reference Koszewska, Walawender, Baran, Zieliński and Ustrnul2019; Di Nicola et al., Reference Di Nicola, Mazza, Panaccione, Moccia, Giuseppin, Marano, Grandinetti, Camardese, De Berardis, Pompili and Janiri2020; Makris et al., Reference Makris, White, Reutfors, Ekselius, Andersen and Papadopoulos2021; Aguglia et al., Reference Aguglia, Giacomini, Montagna, Amerio, Escelsior, Capello, Cutroneo, Ferretti, Scafidi, Costanza, Serafini and Amore2021). Most subjects were between 35 and 65 years of age with only a few exceptions in which populations of under-aged (15–25) (Akkaya-Kalayci et al., Reference Akkaya-Kalayci, Vyssoki, Winkler, Willeit, Kapusta, Dorffner and Özlü-Erkilic2017) or over-aged (Lee et al., Reference Lee, Jung, Myung, Baek, Kang, Kim and Kim2019; Koszewska et al., Reference Koszewska, Walawender, Baran, Zieliński and Ustrnul2019; Schneider et al., Reference Schneider, Hampel, Ladwig, Baumert, Lukaschek, Peters and Breitner2020) populations were exclusively targeted. Females outnumbered males in some studies (Doganay et al., Reference Doganay, Tevfik Sunter, Guz, Ozkan, Altintop, Kati, Colak, Aygun and Guven2003; Akkaya-Kalayci et al., Reference Akkaya-Kalayci, Vyssoki, Winkler, Willeit, Kapusta, Dorffner and Özlü-Erkilic2017; Matthews et al., Reference Matthews, Longman, Berry, Passey, Bennett-Levy, Morgan, Pit, Rolfe and Bailie2019; Di Nicola et al., Reference Di Nicola, Mazza, Panaccione, Moccia, Giuseppin, Marano, Grandinetti, Camardese, De Berardis, Pompili and Janiri2020; Bauer et al., Reference Bauer, Glenn, Achtyes, Alda, Agaoglu, Altınbaş, Andreassen, Angelopoulos, Ardau, Vares, Aydin, Ayhan, Baethge, Bauer, Baune, Balaban, Becerra-Palars, Behere, Behere, Belete, Belete, Belizario, Bellivier, Belmaker, Benedetti, Berk, Bersudsky, Bicakci, Birabwa-Oketcho, Bjella, Brady, Cabrera, Cappucciati, Castro, Chen, Cheung, Chiesa, Crowe, Cuomo, Dallaspezia, del Zompo, Desai, Dodd, Donix, Etain, Fagiolini, Fellendorf, Ferensztajn-Rochowiak, Fiedorowicz, Fountoulakis, Frye, Geoffroy, Gonzalez-Pinto, Gottlieb, Grof, Haarman, Harima, Hasse-Sousa, Henry, Høffding, Houenou, Imbesi, Isometsä, Ivkovic, Janno, Johnsen, Kapczinski, Karakatsoulis, Kardell, Kessing, Kim, König, Kot, Koval, Kunz, Lafer, Landén, Larsen, Lenger, Lewitzka, Licht, Lopez-Jaramillo, MacKenzie, Madsen, Madsen, Mahadevan, Mahardika, Manchia, Marsh, Martinez-Cengotitabengoa, Martiny, Mashima, McLoughlin, Meesters, Melle, Meza-Urzúa, Ming, Monteith, Moorthy, Morken, Mosca, Mozzhegorov, Munoz, Mythri, Nacef, Nadella, Nakanotani, Nielsen, O‘Donovan, Omrani, Osher, Ouali, Pantovic-Stefanovic, Pariwatcharakul, Petite, Pfennig, Ruiz, Pilhatsch, Pinna, Pompili, Porter, Quiroz, Rabelo-da-Ponte, Ramesar, Rasgon, Ratta-apha, Ratzenhofer, Redahan, Reddy, Reif, Reininghaus, Richards, Ritter, Rybakowski, Sathyaputri, Scippa, Simhandl, Severus, Smith, Smith, Stackhouse, Stein, Stilwell, Strejilevich, Su, Subramaniam, Sulaiman, Suominen, Tanra, Tatebayashi, Teh, Tondo, Torrent, Tuinstra, Uchida, Vaaler, Veeh, Vieta, Viswanath, Yoldi-Negrete, Yalcinkaya, Young, Zgueb and Whybrow2021a; Aguglia et al., Reference Aguglia, Giacomini, Montagna, Amerio, Escelsior, Capello, Cutroneo, Ferretti, Scafidi, Costanza, Serafini and Amore2021), leaving male predominance in the majority of the remaining studies (Deisenhammer et al., Reference Deisenhammer, Kemmler and Parson2003; Oravecz et al., Reference Oravecz, Sisti, Rocchi and Preti2007; Preti et al., Reference Preti, Lentini and Maugeri2007; Müller et al., Reference Müller, Biermann, Renk, Reulbach, Ströbel, Kornhuber and Sperling2011; Hiltunen et al., Reference Hiltunen, Haukka, Ruuhela, Suominen and Partonen2014; Bakian et al., Reference Bakian, Huber, Coon, Gray, Wilson, McMahon and Renshaw2015a; Fernández-Arteaga et al., Reference Fernández-Arteaga, Tovilla-Zárate, Fresán, González-Castro, Juárez-Rojop, López-Narváez and Hernández-Díaz2016; Asirdizer et al., Reference Asirdizer, Kartal, Etli, Tatlisumak, Gumus, Hekimoglu and Keskin2018; Fernández-Niño et al., Reference Fernández-Niño, Astudillo-García, Rodríguez-Villamizar and Florez-Garcia2018; Koszewska et al., Reference Koszewska, Walawender, Baran, Zieliński and Ustrnul2019; Lee et al., Reference Lee, Jung, Myung, Baek, Kang, Kim and Kim2019; Bozsonyi et al., Reference Bozsonyi, Lester, Fulop, Zonda and Balint2020; Kayipmaz et al., Reference Kayipmaz, San, Usul and Korkut2020; Schneider et al., Reference Schneider, Hampel, Ladwig, Baumert, Lukaschek, Peters and Breitner2020; Makris et al., Reference Makris, White, Reutfors, Ekselius, Andersen and Papadopoulos2021; Edwards et al., Reference Edwards, Taylor and Gray2023). Table 1.
Measurement of climate exposure and suicidality
The included studies employed diverse methods to measure both climate exposures and suicide outcomes, with most relying on retrospective statistical records. Climate data were largely based on core meteorological variables such as temperature anomalies, seasonal changes, precipitation, humidity, wind speed and daily sunshine duration. Several studies specifically examined air pollution (e.g., PM2.5, NO₂, O₃, SO₂) and its association with suicidality, while others assessed solar insolation and extreme weather events such as heatwaves, floods and droughts. A smaller number used specialized instruments, including the Climate Change Stress and Impairment Scale (CC-DIS) and the METEO-Q, to capture climate-related distress and sensitivity. Suicide outcomes were primarily measured using medical records, national suicide registries and hospital databases, often aligned with classifications from the Diagnostic and Statistical Manual of Mental Disorders (DSM). In addition, several studies employed validated psychometric scales, such as the Suicide Ideation and Behavior Scale (SIBS) and the Implicit Self-Harm Association Test (IAT), to assess suicidal ideation and related behaviours. Reported outcomes included suicidal thoughts, attempts, self-harm, severity of attempts and distinctions between violent and non-violent methods. Some studies also focused on specific populations (e.g., students, employees, pregnant individuals or suicide attempters) to examine subgroup differences in climate-related suicide risk. Overall, most studies combined quantitative climate data with registry-based or self-reported measures of suicidality to explore this relationship (see Table 1 for details).
The outcome of risk of bias assessments
Quality assessment using MMAT (Nha HONG et al., n.d.) of 17 studies (Bakian et al., Reference Bakian, Huber, Coon, Gray, Wilson, McMahon and Renshaw2015a; Burke et al., Reference Burke, González, Baylis, Heft-Neal, Baysan, Basu and Hsiang2018; Matthews et al., Reference Matthews, Longman, Berry, Passey, Bennett-Levy, Morgan, Pit, Rolfe and Bailie2019; Lee et al., Reference Lee, Jung, Myung, Baek, Kang, Kim and Kim2019; Kayipmaz et al., Reference Kayipmaz, San, Usul and Korkut2020; Di Nicola et al., Reference Di Nicola, Mazza, Panaccione, Moccia, Giuseppin, Marano, Grandinetti, Camardese, De Berardis, Pompili and Janiri2020; Makris et al., Reference Makris, White, Reutfors, Ekselius, Andersen and Papadopoulos2021; Bergmans et al., Reference Bergmans, Larson, Bennion, Mezuk, Wozniak, Steiner and Gronlund2021; Jenwitheesuk et al., Reference Jenwitheesuk, Virasiri, Jenwitheesuk, Peansukwech, Arunpongpaisal and Nampathong2022; Miyazaki et al., Reference Miyazaki, Hino, Ito, Abe, Nomoto, Furuno, Takeuchi and Hishimoto2023; Rahman et al., Reference Rahman, Lorenzo, Ban-Weiss, Hasan, Azzouz, Eckel, Conti, Lurmann, Schlaerth, Johnston, Ko, Palinkas, Hurlburt, Silva, Gauderman, McConnell and Garcia2023; Villeneuve et al., Reference Villeneuve, Huynh, Lavigne, Colman, Anisman, Peters and Rodríguez-Villamizar2023; Brailovskaia and Teismann, Reference Brailovskaia and Teismann2024; Hertzog et al., Reference Hertzog, Charlson, Tschakert, Morgan, Norman, Pereira and Hanigan2024; Lian et al., Reference Lian, Wang, Guo, Wan, Ye, Zhou, Han, Yu, Huang and Li2024; Ndetei et al., Reference Ndetei, Wasserman, Mutiso, Shanley, Musyimi, Nyamai, Munyua, Swahn, Weisz, Osborn, Bhui, Johnson, Pihkala, Memiah, Gilbert, Javed and Sourander2024; Runkle et al., Reference Runkle, Sugg, Berry, Reed, Cowan, Wertis and Ryan2024) showed that most of the studies had clear research questions and used data well suited to address those questions. Sample strategies were generally appropriate for the research objectives and, in most cases, the samples appeared to represent the target population. The measurements used in the studies were relevant and appropriate, and the statistical analyses were suitable to answer the research questions. On the contrary, when it came to assessing the risk of non-response bias, none of the studies provided enough information to determine this, resulting in all studies being marked as ‘Cannot tell’ for this criterion. The outcome of the MMAT quality assessment is shown in Table 2.
Outcome of quality assessment using the Mixed Methods Appraisal Tool (MMAT)

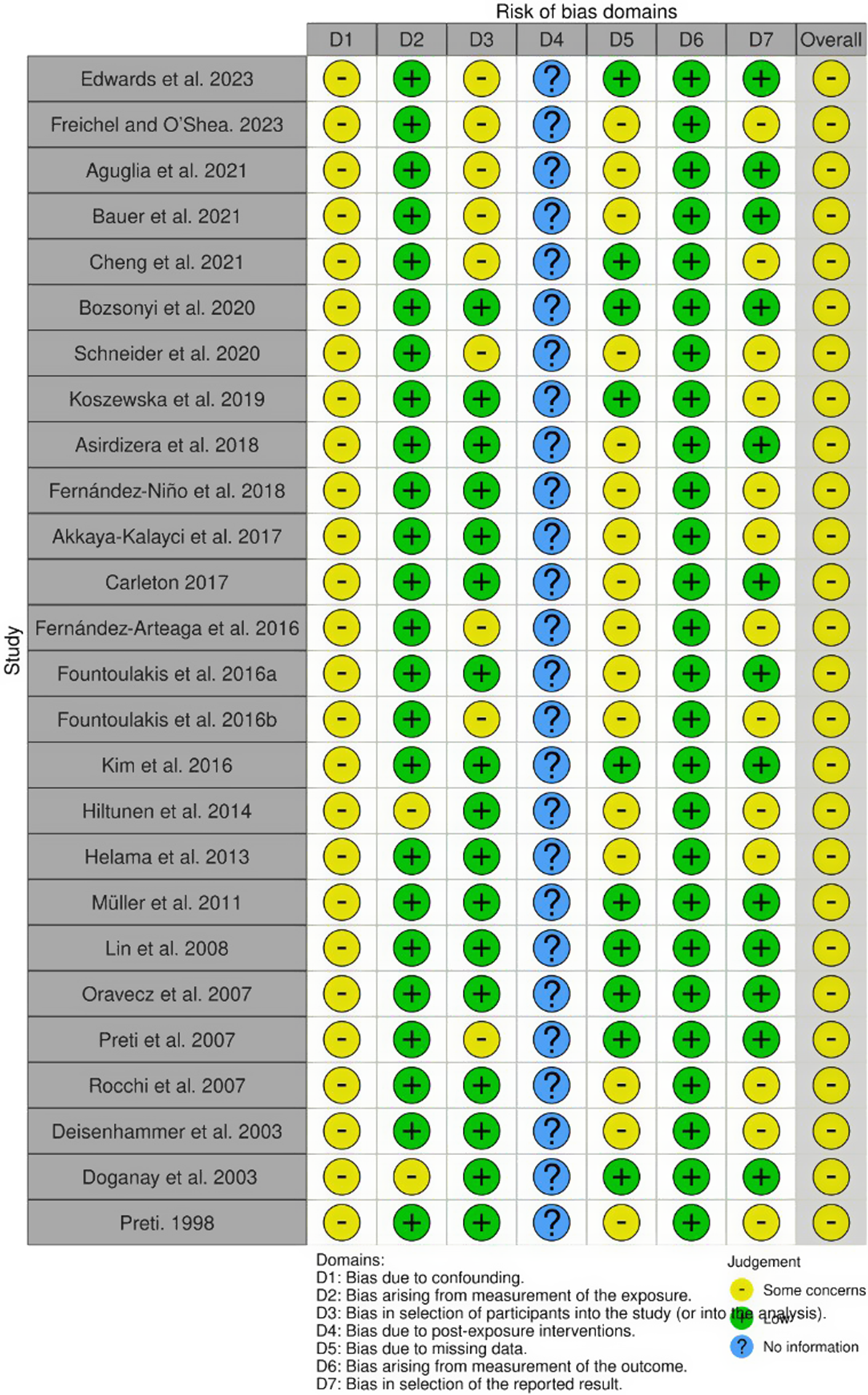
The quality assessment using ROBINS-E (Higgins et al., Reference Higgins, Morgan, Rooney, Taylor, Thayer, Silva, Lemeris, Akl, Bateson, Berkman, Glenn, Hróbjartsson, LaKind, McAleenan, Meerpohl, Nachman, Obbagy, O’Connor and Radke2024) of 26 studies (Preti, Reference Preti1997; Deisenhammer et al., Reference Deisenhammer, Kemmler and Parson2003; Doganay et al., Reference Doganay, Tevfik Sunter, Guz, Ozkan, Altintop, Kati, Colak, Aygun and Guven2003; Oravecz et al., Reference Oravecz, Sisti, Rocchi and Preti2007; Preti et al., Reference Preti, Lentini and Maugeri2007; Rocchi et al., Reference Rocchi, Sisti, Cascio and Preti2007; Lin et al., Reference Lin, Chen, Xirasagar and Lee2008; Müller et al., Reference Müller, Biermann, Renk, Reulbach, Ströbel, Kornhuber and Sperling2011; Helama et al., Reference Helama, Holopainen and Partonen2013; Hiltunen et al., Reference Hiltunen, Haukka, Ruuhela, Suominen and Partonen2014; Kim et al., Reference Kim, Kim, Honda, Guo, Chen, Woo and Ebi2016; Fernández-Arteaga et al., Reference Fernández-Arteaga, Tovilla-Zárate, Fresán, González-Castro, Juárez-Rojop, López-Narváez and Hernández-Díaz2016a; Fountoulakis, Chatzikosta, et al., Reference Fountoulakis, Chatzikosta, Pastiadis, Zanis, Kawohl, Kerkhof, Navickas, Höschl, Lecic-Tosevski, Sorel, Rancans, Palova, Juckel, Isacsson, Jagodic, Botezat-Antonescu, Rybakowski, Azorin, Cookson, Waddington, Pregelj, Demyttenaere, Hranov, Stevovic, Pezawas, Adida, Figuera, Jakovljević, Vichi, Perugi, Andreassen, Vukovic, Mavrogiorgou, Varnik, Dome, Winkler, Salokangas, From, Danileviciute, Gonda, Rihmer, Forsman, Grady, Hyphantis, Dieset, Soendergaard, Pompili and Bech2016; Fountoulakis, Savopoulos, et al., Reference Fountoulakis, Savopoulos, Zannis, Apostolopoulou, Fountoukidis, Kakaletsis, Kanellos, Dimellis, Hyphantis, Tsikerdekis, Pompili and Hatzitolios2016a; Akkaya-Kalayci et al., Reference Akkaya-Kalayci, Vyssoki, Winkler, Willeit, Kapusta, Dorffner and Özlü-Erkilic2017; Carleton, Reference Carleton2017; Asirdizer et al., Reference Asirdizer, Kartal, Etli, Tatlisumak, Gumus, Hekimoglu and Keskin2018; Fernández-Niño et al., Reference Fernández-Niño, Astudillo-García, Rodríguez-Villamizar and Florez-Garcia2018; Koszewska et al., Reference Koszewska, Walawender, Baran, Zieliński and Ustrnul2019; Bozsonyi et al., Reference Bozsonyi, Lester, Fulop, Zonda and Balint2020; Schneider et al., Reference Schneider, Hampel, Ladwig, Baumert, Lukaschek, Peters and Breitner2020; Aguglia et al., Reference Aguglia, Giacomini, Montagna, Amerio, Escelsior, Capello, Cutroneo, Ferretti, Scafidi, Costanza, Serafini and Amore2021; Bauer et al., Reference Bauer, Glenn, Achtyes, Alda, Agaoglu, Altınbaş, Andreassen, Angelopoulos, Ardau, Vares, Aydin, Ayhan, Baethge, Bauer, Baune, Balaban, Becerra-Palars, Behere, Behere, Belete, Belete, Belizario, Bellivier, Belmaker, Benedetti, Berk, Bersudsky, Bicakci, Birabwa-Oketcho, Bjella, Brady, Cabrera, Cappucciati, Castro, Chen, Cheung, Chiesa, Crowe, Cuomo, Dallaspezia, del Zompo, Desai, Dodd, Donix, Etain, Fagiolini, Fellendorf, Ferensztajn-Rochowiak, Fiedorowicz, Fountoulakis, Frye, Geoffroy, Gonzalez-Pinto, Gottlieb, Grof, Haarman, Harima, Hasse-Sousa, Henry, Høffding, Houenou, Imbesi, Isometsä, Ivkovic, Janno, Johnsen, Kapczinski, Karakatsoulis, Kardell, Kessing, Kim, König, Kot, Koval, Kunz, Lafer, Landén, Larsen, Lenger, Lewitzka, Licht, Lopez-Jaramillo, MacKenzie, Madsen, Madsen, Mahadevan, Mahardika, Manchia, Marsh, Martinez-Cengotitabengoa, Martiny, Mashima, McLoughlin, Meesters, Melle, Meza-Urzúa, Ming, Monteith, Moorthy, Morken, Mosca, Mozzhegorov, Munoz, Mythri, Nacef, Nadella, Nakanotani, Nielsen, O‘Donovan, Omrani, Osher, Ouali, Pantovic-Stefanovic, Pariwatcharakul, Petite, Pfennig, Ruiz, Pilhatsch, Pinna, Pompili, Porter, Quiroz, Rabelo-da-Ponte, Ramesar, Rasgon, Ratta-apha, Ratzenhofer, Redahan, Reddy, Reif, Reininghaus, Richards, Ritter, Rybakowski, Sathyaputri, Scippa, Simhandl, Severus, Smith, Smith, Stackhouse, Stein, Stilwell, Strejilevich, Su, Subramaniam, Sulaiman, Suominen, Tanra, Tatebayashi, Teh, Tondo, Torrent, Tuinstra, Uchida, Vaaler, Veeh, Vieta, Viswanath, Yoldi-Negrete, Yalcinkaya, Young, Zgueb and Whybrow2021a; Cheng et al., Reference Cheng, Plouffe, Nanos, Qamar, Fisman and Soucy2021; Freichel & O’Shea, Reference Freichel and O’Shea2023; Edwards et al., Reference Edwards, Taylor and Gray2023) showed that all the studies had ‘Some concerns’ in Domain 1, which relates to bias due to confounding. Domains 2 and 6, covering bias arising from exposure measurement and bias arising from measurement of the outcome, were generally rated ‘low’ risk. Domain 3, which examines bias in the selection of participants in the study, and Domain 5, which addresses bias due to missing data, showed mixed ratings, with several studies indicating ‘Some concerns’. Domain 4, which addressed bias due to post-exposure interventions, had insufficient information. Overall, the studies predominantly fell under the category ‘Some concerns’, indicating a moderate risk of bias in general. The outcome of the ROBINS-E quality assessment is illustrated in Figures 2 and 3.
ROBINS-E assessment of individual studies across domains. Most studies showed ‘Some concerns’ in Domain 1 (bias due to confounding). Domains 2 and 6 (bias in exposure measurement and outcome measurement) were generally rated ‘low’ risk. Domains 3 (bias in selection of participants) and 5 (bias due to missing data) showed mixed ratings, while Domain 4 (bias due to post-exposure interventions) often lacked sufficient information.

Summary of ROBINS-E quality assessment across all included studies. The majority of studies fell under the category of ‘Some concerns’, reflecting a moderate overall risk of bias.

Main findings
Distribution of climate indictors and suicidality outcomes
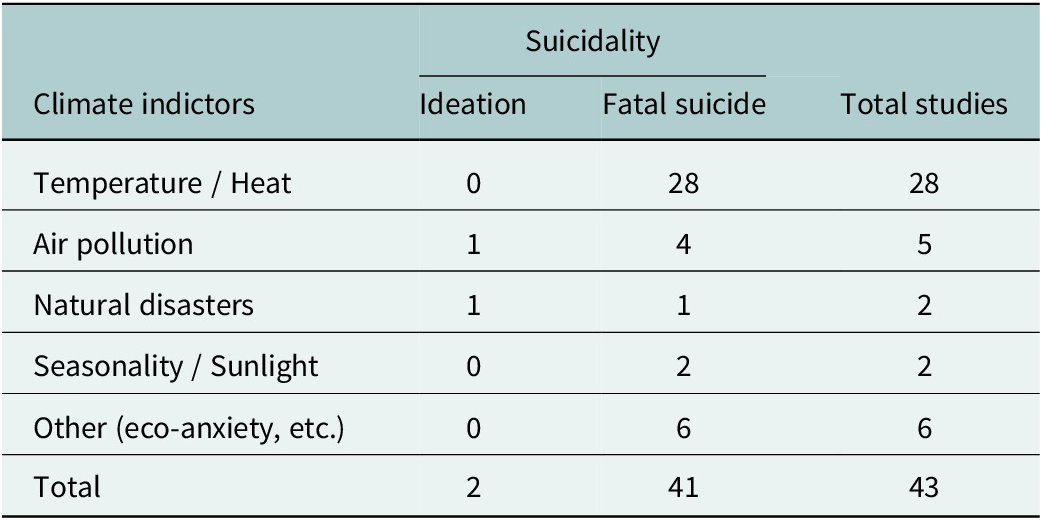
To illustrate how climate indicators and suicidality outcomes align across literature, Table 3 summarizes the distribution of the 43 included studies. The majority examined temperature or heat as the main indicator (28 studies), followed by air pollution (5 studies), natural disasters such as floods or droughts (2 studies), and seasonality or solar-related variables (2 studies). Six studies focused on other indicators, such as eco-anxiety, altitude, foehn wind or aeroallergens. Regarding suicidality outcomes, 41 studies investigated fatal suicide, while only 2 assessed suicidal ideation, reflecting the spectrum of suicide outcomes from thoughts to fatal acts. These two suicidal ideation studies, conducted among students and adolescents, reported significant associations between climate-related stressors and suicidal thoughts but were limited to specific populations. This imbalance highlights the dominance of mortality-focused research and the lack of attention to earlier stages of suicidality.
Distribution of climate indicators and suicidality outcomes across included studies (n = 43)

Geographic distribution and climate factors in suicide risk
Although LAMICs cover a large portion of the global population, there are relatively few studies that examine the connection between climate change and suicidality in these regions. Most of the research on suicidality linked to climate change has been conducted in European countries (Aguglia et al., Reference Aguglia, Giacomini, Montagna, Amerio, Escelsior, Capello, Cutroneo, Ferretti, Scafidi, Costanza, Serafini and Amore2021; Akkaya-Kalayci et al., Reference Akkaya-Kalayci, Vyssoki, Winkler, Willeit, Kapusta, Dorffner and Özlü-Erkilic2017a; Asirdizer et al., Reference Asirdizer, Kartal, Etli, Tatlisumak, Gumus, Hekimoglu and Keskin2018; Bozsonyi et al., Reference Bozsonyi, Lester, Fulop, Zonda and Balint2020; Brailovskaia and Teismann, Reference Brailovskaia and Teismann2024; Di Nicola et al., Reference Di Nicola, Mazza, Panaccione, Moccia, Giuseppin, Marano, Grandinetti, Camardese, De Berardis, Pompili and Janiri2020a; Doganay et al., Reference Doganay, Tevfik Sunter, Guz, Ozkan, Altintop, Kati, Colak, Aygun and Guven2003; Helama et al., Reference Helama, Holopainen and Partonen2013; Kayipmaz et al., Reference Kayipmaz, San, Usul and Korkut2020; Müller et al., Reference Müller, Biermann, Renk, Reulbach, Ströbel, Kornhuber and Sperling2011; Oravecz et al., Reference Oravecz, Sisti, Rocchi and Preti2007; Preti, Reference Preti1997, 1998a; Preti et al., Reference Preti, Lentini and Maugeri2007; Schneider et al., Reference Schneider, Hampel, Ladwig, Baumert, Lukaschek, Peters and Breitner2020), USA (Bergmans et al., Reference Bergmans, Larson, Bennion, Mezuk, Wozniak, Steiner and Gronlund2021; Rahman et al., Reference Rahman, Lorenzo, Ban-Weiss, Hasan, Azzouz, Eckel, Conti, Lurmann, Schlaerth, Johnston, Ko, Palinkas, Hurlburt, Silva, Gauderman, McConnell and Garcia2023; Freichel & O’Shea, Reference Freichel and O’Shea2023; Runkle et al., Reference Runkle, Sugg, Berry, Reed, Cowan, Wertis and Ryan2024), Australia (Matthews et al., Reference Matthews, Longman, Berry, Passey, Bennett-Levy, Morgan, Pit, Rolfe and Bailie2019; Edwards et al., Reference Edwards, Taylor and Gray2023; Hertzog et al., Reference Hertzog, Charlson, Tschakert, Morgan, Norman, Pereira and Hanigan2024) and Canada (Villeneuve et al., Reference Villeneuve, Huynh, Lavigne, Colman, Anisman, Peters and Rodríguez-Villamizar2023; Freichel & O’Shea, Reference Freichel and O’Shea2023). The sociocultural and environmental contexts, as well as resource availability in LAMICs, differ significantly from those of developed European nations. Therefore, there is a pressing need for more regional research to develop remediation strategies specific to these areas.
Temperature and heat exposure and suicide
Temperature and heat anomalies were among the most strongly linked climate factors to suicidality. Multiple studies found that higher temperatures significantly increased suicide mortality, particularly in older adults and men (Preti et al., Reference Preti, Lentini and Maugeri2007; Cheng et al., Reference Cheng, Plouffe, Nanos, Qamar, Fisman and Soucy2021; Hertzog et al., Reference Hertzog, Charlson, Tschakert, Morgan, Norman, Pereira and Hanigan2024). In Australia, 55-year-old men and older showed the highest vulnerability to heat-related suicides, while studies in the United States, Canada and Germany reported that each 1 ° C increase in temperature was associated with a rise in suicide rates (Burke et al., Reference Burke, González, Baylis, Heft-Neal, Baysan, Basu and Hsiang2018; Schneider et al., Reference Schneider, Hampel, Ladwig, Baumert, Lukaschek, Peters and Breitner2020; Cheng et al., Reference Cheng, Plouffe, Nanos, Qamar, Fisman and Soucy2021; Hertzog et al., Reference Hertzog, Charlson, Tschakert, Morgan, Norman, Pereira and Hanigan2024). Furthermore, Bozsonyi et al. (Reference Bozsonyi, Lester, Fulop, Zonda and Balint2020)) in Hungary found a strong positive correlation between suicide rates, high ambient temperatures and duration of sunshine. Kayipmaz et al. (Reference Kayipmaz, San, Usul and Korkut2020)) in Turkey reported that an increase in minimum temperature on the day of application was correlated with a rise in suicides. Similarly, in Mexico, rain and high temperatures were significantly associated with suicide risk in which a 1 ° C increase in monthly temperature led to a 2.1% increase in suicide rates, while in the United States, the increase was 0.7% (Fernández-Arteaga et al., Reference Fernández-Arteaga, Tovilla-Zárate, Fresán, González-Castro, Juárez-Rojop, López-Narváez and Hernández-Díaz2016; Burke et al., Reference Burke, González, Baylis, Heft-Neal, Baysan, Basu and Hsiang2018).
In India, high temperatures increased suicides, particularly during the growing season, suggesting that economic hardship due to climate-related crop failures exacerbated the risk of suicide (Carleton, Reference Carleton2017). In particular, older adults (65+) in Sweden showed increased vulnerability to suicidal risk due to higher temperatures and increased sunshine, although these effects were not significant after adjustments (Makris et al., Reference Makris, White, Reutfors, Ekselius, Andersen and Papadopoulos2021). Furthermore Fountoulakis, Chatzikosta, et al. (Reference Fountoulakis, Chatzikosta, Pastiadis, Zanis, Kawohl, Kerkhof, Navickas, Höschl, Lecic-Tosevski, Sorel, Rancans, Palova, Juckel, Isacsson, Jagodic, Botezat-Antonescu, Rybakowski, Azorin, Cookson, Waddington, Pregelj, Demyttenaere, Hranov, Stevovic, Pezawas, Adida, Figuera, Jakovljević, Vichi, Perugi, Andreassen, Vukovic, Mavrogiorgou, Varnik, Dome, Winkler, Salokangas, From, Danileviciute, Gonda, Rihmer, Forsman, Grady, Hyphantis, Dieset, Soendergaard, Pompili and Bech2016) and Fountoulakis, Savopoulos, et al. (Reference Fountoulakis, Savopoulos, Zannis, Apostolopoulou, Fountoukidis, Kakaletsis, Kanellos, Dimellis, Hyphantis, Tsikerdekis, Pompili and Hatzitolios2016b) found that male suicide rates in Greece and throughout Europe were linked to minimum temperatures, with suicide attempts peaking during May to August and December to February. Particularly low temperatures accounted for 37.6% of male suicides and 28.1% of female suicides. Furthermore, the timing of heat exposure was critical. Studies in Germany, Italy and Austria found that high temperatures, low humidity and thunderstorms were significantly linked to higher suicide rates, men being more affected than women (Preti, Reference Preti1998; Deisenhammer et al., Reference Deisenhammer, Kemmler and Parson2003; Müller et al., Reference Müller, Biermann, Renk, Reulbach, Ströbel, Kornhuber and Sperling2011).
Air pollution and suicide
Exposure to air pollution was also a key factor contributing to suicidality. In Japan, elevated SO2 levels were strongly linked to higher suicide attempts, while NO (nitrogen oxide) levels showed an inverse relationship with suicidality (Miyazaki et al., Reference Miyazaki, Hino, Ito, Abe, Nomoto, Furuno, Takeuchi and Hishimoto2023). In Thailand, a 1 mg/m3 increase in PM2.5 dust led to a 63.5% increase in suicide risk, demonstrating the direct impact of poor air quality (Jenwitheesuk et al., Reference Jenwitheesuk, Virasiri, Jenwitheesuk, Peansukwech, Arunpongpaisal and Nampathong2022). Studies in Canada and the United States showed that exposure to fine particulate matter (PM2.5) and nitrogen dioxide (NO2) significantly increased suicide risks, particularly during seasonal transitions in spring and fall (Bakian et al., Reference Bakian, Huber, Coon, Gray, Wilson, McMahon and Renshaw2015b; Rahman et al., Reference Rahman, Lorenzo, Ban-Weiss, Hasan, Azzouz, Eckel, Conti, Lurmann, Schlaerth, Johnston, Ko, Palinkas, Hurlburt, Silva, Gauderman, McConnell and Garcia2023; Villeneuve et al., Reference Villeneuve, Huynh, Lavigne, Colman, Anisman, Peters and Rodríguez-Villamizar2023). Furthermore, Lian et al. (Reference Lian, Wang, Guo, Wan, Ye, Zhou, Han, Yu, Huang and Li2024)) in China found that short-term exposure to air pollution significantly increased suicide deaths, particularly in cities at the county level, accounting for up to 8.07% of excess suicide deaths. Similarly, in Italy, solar radiation (65%) and PM2.5 (32%) were positively correlated with suicide attempts, particularly among middle-aged males (Aguglia et al., Reference Aguglia, Giacomini, Montagna, Amerio, Escelsior, Capello, Cutroneo, Ferretti, Scafidi, Costanza, Serafini and Amore2021). While many studies confirmed the association between air pollution and suicide, some did not find significant links. In Colombia, no statistically significant association was found between air pollution and suicidality, suggesting potential geographical and demographic differences in susceptibility (Fernández-Niño et al., Reference Fernández-Niño, Astudillo-García, Rodríguez-Villamizar and Florez-Garcia2018).
Seasonality and suicide
Seasonal variations in temperature and exposure to sunlight were repeatedly linked to suicide rates. In studies from the United States, United Kingdom, Canada, Taiwan and Italy, suicidal ideation and attempts peaked during seasonal transitions, with spring and early summer showing the highest suicide rates (Preti, Reference Preti1997; Lin et al., Reference Lin, Chen, Xirasagar and Lee2008; Freichel & O’Shea, Reference Freichel and O’Shea2023c). Suicide rates were observed to peak in December, and implicit self-harm thoughts reaching their highest levels in February, suggesting a delayed psychological effect of reduced daylight exposure (Freichel & O’Shea, Reference Freichel and O’Shea2023c). Kim et al. (Reference Kim, Kim, Honda, Guo, Chen, Woo and Ebi2015) in South Korea, sJapan and Taiwan found a positive association between suicide rates and elevated ambient temperatures, including the duration of sunshine. Akkaya-Kalayci et al. (Reference Akkaya-Kalayci, Vyssoki, Winkler, Willeit, Kapusta, Dorffner and Özlü-Erkilic2017) in Turkey found that suicide attempts in youth were linked to seasonal changes, peaking in summer with short-term effects in men. Koszewska et al. (Reference Koszewska, Walawender, Baran, Zieliński and Ustrnul2019) in Poland found that the foehn wind was associated with increased suicide risks, particularly in summer and autumn. Furthermore, in Slovenia, the seasonality of suicide showed a stronger correlation among women (Oravecz et al., Reference Oravecz, Sisti, Rocchi and Preti2007). In Italy, suicide attempts peaked in spring, accounted for 40% in males and 39% in females, while in Taiwan, rising ambient temperatures from March to May were linked to higher violent suicide rates (Rocchi et al., Reference Rocchi, Sisti, Cascio and Preti2007; Lin et al., Reference Lin, Chen, Xirasagar and Lee2008). Furthermore, Helama et al. (Reference Helama, Holopainen and Partonen2013)) in Finland found that temperature variability accounted for more than 60% of the variance in suicide rates. However, a decline in suicide rates was observed despite ongoing warming.
Natural disasters and extreme climate events and suicide
Several studies linked natural disasters, such as wildfires, floods and droughts, to increased suicidal thoughts and behaviours. In Australia, floods were associated with a 7% increase in suicidal ideation, particularly among adolescents (Matthews et al., Reference Matthews, Longman, Berry, Passey, Bennett-Levy, Morgan, Pit, Rolfe and Bailie2019; Edwards et al., Reference Edwards, Taylor and Gray2023). Lee et al. (Reference Lee, Jung, Myung, Baek, Kang, Kim and Kim2019) in South Korea found that dust storms were associated with a higher risk of suicide, with stronger associations during prolonged storms. A study in Turkey found that altitude-related climate conditions contributed to higher suicide rates, particularly among women (Asirdizer et al., Reference Asirdizer, Kartal, Etli, Tatlisumak, Gumus, Hekimoglu and Keskin2018). Studies in Turkey and Italy further emphasized the role of humidity, thunderstorms and extreme weather in increasing the risk of suicide (Doganay et al., Reference Doganay, Tevfik Sunter, Guz, Ozkan, Altintop, Kati, Colak, Aygun and Guven2003; Di Nicola et al., Reference Di Nicola, Mazza, Panaccione, Moccia, Giuseppin, Marano, Grandinetti, Camardese, De Berardis, Pompili and Janiri2020). Hiltunen et al. (Reference Hiltunen, Haukka, Ruuhela, Suominen and Partonen2014) in Finland found that a decrease in temperature over five days was associated with lower male suicide rates, suggesting stronger climate–suicide interactions. Additionally, a study in the United States found that grass pollen exposure was linked to suicide on the same day, particularly among women and individuals with lower education levels (Bergmans et al., Reference Bergmans, Larson, Bennion, Mezuk, Wozniak, Steiner and Gronlund2021).
Climate change anxiety and suicide
Several studies highlighted the impact of climate change distress on suicidality. Psychological distress linked to climate change-related stressors was found to be a significant risk factor for suicidal ideation among university students and employees in Germany (Brailovskaia and Teismann, Reference Brailovskaia and Teismann2024). Similarly, among high school students in Kenya, perceived threats of climate change were associated with an increased risk of suicidal thoughts and attempts (Ndetei et al., Reference Ndetei, Wasserman, Mutiso, Shanley, Musyimi, Nyamai, Munyua, Swahn, Weisz, Osborn, Bhui, Johnson, Pihkala, Memiah, Gilbert, Javed and Sourander2024).
Vulnerable populations
Vulnerable populations, including older adults, pregnant women, migrant populations and people with mental illness, exhibit a greater susceptibility to climate-related suicide risks. Studies in individuals with bipolar disorder indicate that increased sensitivity to weather changes is correlated with a higher risk of suicide attempts (Di Nicola et al., Reference Di Nicola, Mazza, Panaccione, Moccia, Giuseppin, Marano, Grandinetti, Camardese, De Berardis, Pompili and Janiri2020). Research in 40 countries found that significant seasonal changes in solar insolation increased the likelihood of suicidal ideation and attempts in individuals with bipolar disorder (Bauer et al., Reference Bauer, Glenn, Achtyes, Alda, Agaoglu, Altınbaş, Andreassen, Angelopoulos, Ardau, Vares, Aydin, Ayhan, Baethge, Bauer, Baune, Balaban, Becerra-Palars, Behere, Behere, Belete, Belete, Belizario, Bellivier, Belmaker, Benedetti, Berk, Bersudsky, Bicakci, Birabwa-Oketcho, Bjella, Brady, Cabrera, Cappucciati, Castro, Chen, Cheung, Chiesa, Crowe, Cuomo, Dallaspezia, del Zompo, Desai, Dodd, Donix, Etain, Fagiolini, Fellendorf, Ferensztajn-Rochowiak, Fiedorowicz, Fountoulakis, Frye, Geoffroy, Gonzalez-Pinto, Gottlieb, Grof, Haarman, Harima, Hasse-Sousa, Henry, Høffding, Houenou, Imbesi, Isometsä, Ivkovic, Janno, Johnsen, Kapczinski, Karakatsoulis, Kardell, Kessing, Kim, König, Kot, Koval, Kunz, Lafer, Landén, Larsen, Lenger, Lewitzka, Licht, Lopez-Jaramillo, MacKenzie, Madsen, Madsen, Mahadevan, Mahardika, Manchia, Marsh, Martinez-Cengotitabengoa, Martiny, Mashima, McLoughlin, Meesters, Melle, Meza-Urzúa, Ming, Monteith, Moorthy, Morken, Mosca, Mozzhegorov, Munoz, Mythri, Nacef, Nadella, Nakanotani, Nielsen, O‘Donovan, Omrani, Osher, Ouali, Pantovic-Stefanovic, Pariwatcharakul, Petite, Pfennig, Ruiz, Pilhatsch, Pinna, Pompili, Porter, Quiroz, Rabelo-da-Ponte, Ramesar, Rasgon, Ratta-apha, Ratzenhofer, Redahan, Reddy, Reif, Reininghaus, Richards, Ritter, Rybakowski, Sathyaputri, Scippa, Simhandl, Severus, Smith, Smith, Stackhouse, Stein, Stilwell, Strejilevich, Su, Subramaniam, Sulaiman, Suominen, Tanra, Tatebayashi, Teh, Tondo, Torrent, Tuinstra, Uchida, Vaaler, Veeh, Vieta, Viswanath, Yoldi-Negrete, Yalcinkaya, Young, Zgueb and Whybrow2021b). Pregnant women also face increased vulnerability, with a study reporting a 28% increase in suicidal thoughts for every 5 ° C temperature increase (Runkle et al., Reference Runkle, Sugg, Berry, Reed, Cowan, Wertis and Ryan2024). Similarly, older adults (≥65 years) experience greater sensitivity to high temperatures and seasonal variations, with stronger effects observed during summer and autumn (Schneider et al., Reference Schneider, Hampel, Ladwig, Baumert, Lukaschek, Peters and Breitner2020).
Discussion
This systematic review investigated the complex relationship between climate change and suicidality, synthesizing findings from 43 studies conducted throughout the world. The results highlighted the link between climate indicators, such as rising temperatures, air pollution and extreme weather events, and suicidality, with important implications for public health, particularly among vulnerable populations.
Most of the research related to climate change and suicidality comes from high-income countries, while LAMICs, which are disproportionately exposed to extreme climate events, remain severely underrepresented in the existing evidence base. Although the 43 included studies represent 13 countries worldwide, the overwhelming majority originate from Europe, North America and Australia. This imbalance represents a major structural limitation of the field, rather than this review alone, given that many of the world’s most climate-vulnerable populations reside in LAMICs where climate shocks, food insecurity, forced displacement, political instability and poverty are more prevalent. In such settings, climate stressors may interact more strongly with adverse social determinants of health and limited access to mental health services, potentially amplifying suicide risk beyond what is observed in high-income countries, while protective community factors remain poorly understood. The absence of robust suicidality data from these regions is therefore a critical global evidence gap that limits equitable prevention planning and policy development. People exposed to extreme weather, high temperatures, rainfall, air pollutants, floods and humidity demonstrate high suicidal behaviour (from ideation to fatal outcomes). A positive association between seasonal variation and suicidal behaviour is also reported, particularly in women. While two studies provided important evidence on climate-related suicidal ideation, their limited number and population-specific focus underscore the critical lack of research on non-fatal stages of suicidality compared with the extensive focus on fatal suicide. The review revealed a consistent association between increased ambient temperature and increased risk of fatal suicide. For example, studies in the United States, Mexico and India demonstrated a clear increase in suicide rates correlated with elevated temperatures and prolonged heatwaves. This is consistent with physiological and psychological mechanisms in which high temperatures exacerbate psychological problems such as aggression, irritability and impulsivity, which can lead to increased suicidal behaviour (Hou et al., Reference Hou, Wang, Wang and Zhang2023; Fischer et al., Reference Fischer, Nägeli, Cardone, Filippini, Merla, Hanusch and Ehlert2024). Evidence from meta-analyses also supported that increased temperature and temperature variability could be associated with an increase in suicide and suicidal behaviour (Björkstén et al., Reference Björkstén, Bjerregaard and Kripke2005; Thompson et al., Reference Thompson, Lawrance, Roberts, Grailey, Ashrafian, Maheswaran, Toledano and Darzi2023; To et al., Reference To, Messias, Burch and Chibnall2024). Additionally, seasonal patterns observed in several studies indicated higher rates of suicidality during the summer months, particularly among women, suggesting the possibility of female gender in climatic adversities. Climatic changes and an extreme rise in temperature have been reported in recent decades globally. This trend is expected to continue in the coming days and is likely to influence suicidal behaviour. Hence, it is important to consider climatic adversities in the suicide-prevention programme.
Extreme weather events, such as floods, hurricanes and droughts, were also linked to adverse mental health outcomes, including PTSD, depression and suicidality (Cianconi et al., Reference Cianconi, Betrò and Janiri2020; Walinski et al., Reference Walinski, Sander, Gerlinger, Clemens, Meyer-Lindenberg and Heinz2023; Heanoy and Brown, Reference Heanoy and Brown2024; Patwary et al., Reference Patwary, Bardhan, Haque, Moniruzzaman, Gustavsson, Khan, Koivisto, Salwa, Mashreky, Rahman, Tasnim, Islam, Alam, Hasan, Harun, Nyberg and Islam2024). These findings highlight the psychosocial burden of climate disasters, driven by loss of livelihoods, displacement and community disintegration. Such disasters are common in specific geographical regions (more so in coastal areas). Unfortunately, the disaster-affected countries have little research on suicidal behaviour in reference to the disasters. Therefore, it is important to have more research in these countries on the mental health aspects of disasters to understand the region-specific needs.
Furthermore, the review identified air pollution as a compounding factor, with pollutants such as particulate matter and nitrogen dioxide contributing to poor mental health and suicide risk (Braithwaite et al., Reference Braithwaite, Zhang, Kirkbride, Osborn and Hayes2019; Bhui et al., Reference Bhui, Newbury, Latham, Ucci, Nasir, Turner, O’leary, Fisher, Marczylo, Douglas, Stansfeld, Jackson, Tyrrel, Rzhetsky, Kinnersley, Kumar, Duchaine and Coulon Background2023; Nobile et al., Reference Nobile, Forastiere, Michelozzi, Forastiere and Stafoggia2023). Measures being taken to control pollution should aim at reducing the level of nitrogen dioxide (decreasing its production by intervening at the levels of sources from where it is being produced) and particulate matter suspended in air.
Methodological considerations
Importantly, all studies assessed using the ROBINS-E tool were judged to have some concerns regarding confounding bias, particularly due to unmeasured or residual factors such as socioeconomic conditions, unemployment, substance use, comorbid mental disorders, social isolation and access to mental health services. This pervasive limitation reflects the inherent challenges of observational climate–health research rather than methodological weaknesses of individual studies. Consequently, the associations identified in this review should not be interpreted as causal effects but rather as population-level correlations between climate indicators and suicidality that may be shaped by broader contextual and social determinants. This consideration warrants cautious interpretation of effect estimates and highlights the need for future longitudinal and quasi-experimental research designs that can better address confounding. The prevalence of cross-sectional and retrospective study designs restricts causal inferences, highlighting a methodological gap in the literature. Longitudinal studies are essential to elucidate the temporal dynamics between climate change and suicidality. Furthermore, the variability in climate and suicidality measures in all studies complicates comparability and synthesis. Standardizing methodologies, including consistent definitions and measurement tools for climate indicators and suicidal behaviours, could enhance the robustness of future research. The methods used, the parameters studied and the results measured in most existing research are heterogeneous; therefore, it is challenging to accurately compare the outcomes between the studies.
Recommendations and implications for policy and practice
The findings of this review have direct and actionable implications for public health policy and suicide prevention practice. First, climate-sensitive mental health early warning systems should be developed in regions experiencing recurrent heatwaves and extreme weather events. Several included studies demonstrated significant increases in suicide risk at temperature rises of 1–5 °C, suggesting that locally calibrated temperature thresholds could serve as triggers for activating mental health surge responses, crisis hotlines and outreach services to vulnerable populations such as older adults, individuals with mental illness, pregnant women and outdoor workers. Second, establishing publicly accessible cooling centres in different urban and rural locations during periods of extreme summer heat represents a feasible and cost-effective preventive intervention. These centres can support both physical and mental health, reduce heat-related psychological distress, stabilize autonomic nervous system responses and potentially mitigate heat-associated risks of suicidal behaviour, particularly among vulnerable populations who lack access to adequate cooling at home. Third, air-quality monitoring systems should be integrated with suicide surveillance, particularly in urban and industrial areas with high concentrations of PM₂.₅, NO₂ and SO₂. Public health agencies should issue combined air-pollution and mental-health alerts, alongside temporary restrictions on outdoor work and targeted psychosocial support during peak pollution periods. Fourth, standardized climate-suicidality measurement protocols are urgently needed to improve comparability across studies and surveillance systems. These should include harmonized definitions of heat exposure, extreme events and suicidality outcomes, as well as routine collection of data on suicidal ideation, attempts and fatal suicide, not mortality alone. Fifth, disaster preparedness and response plans should formally include mental health and psychosocial support (MHPSS), including digital and electronic mental health (Ahmed and Heun, Reference Ahmed and Heun2024) components tailored to climate-related disasters such as floods, droughts, dust storms and wildfires, particularly to ensure continuity of care in remote and hard-to-access areas during disasters. This should involve pre-positioned psychological first aid teams, mobile mental health units and structured community follow-up for affected populations. Finally, in LAMICs, implementation of these interventions must account for resource constraints, limited mental health workforces and fragile health systems. Climate–mental health early warning systems may therefore be most feasible when integrated into existing meteorological, primary healthcare and civil protection infrastructures rather than developed as stand-alone platforms. Cooling centres can be adapted using low-cost community spaces such as schools, mosques, churches or municipal buildings, supported by local governments, NGOs and community volunteers. Similarly, eMHPSS approaches offer particular promise in LAMICs by enabling task-shifting, remote psychological first aid and continuity of care during climate disasters, especially where specialist services are scarce. Leveraging mobile phone penetration, community health workers and partnerships with humanitarian organizations may allow scalable and cost-effective implementation in resource-limited settings.
Strengths and limitations
The strengths of this review stem from being the first systematic review on this topic, providing a comprehensive analysis of 43 studies in various geographic regions and climate indicators, offering solid information on the relationship between climate change and suicidality. Furthermore, the review identifies notable research gaps, offering actionable recommendations for future studies and filling a critical public health evidence gap. However, limitations persist, including the predominance of cross-sectional and retrospective studies, which restrict causal inferences, and the exclusion of qualitative research may overlook valuable insights into lived experiences and cultural contexts of climate change and suicidality. Additionally, the reliance on secondary data limits the ability to assess study quality and methodological rigor directly, also the heterogeneity in study designs and methodologies complicates the synthesis of findings, and the underrepresentation of LAMICs limits the global applicability of the conclusions. Furthermore, the restriction to English-language publications may have led to the exclusion of relevant studies conducted especially in climate-vulnerable LAMIC regions and published in local languages; future multilingual systematic reviews may therefore help to partially address the geographic and socioeconomic evidence gaps identified in this review. Although qualitative studies were excluded due to the review’s focus on quantitatively measurable associations, this represents an important conceptual limitation. Qualitative research can provide valuable insights into lived experiences of climate-related distress, cultural interpretations of environmental stressors, help-seeking behaviours and barriers to mental health care. Such insights are particularly relevant for understanding how and why climate exposures translate into suicidality in specific contexts and can meaningfully inform the design, acceptability and cultural appropriateness of preventive interventions. Future reviews integrating mixed-methods evidence may therefore strengthen intervention development and implementation strategies.
Conclusion
The relationship between climate change and suicidality represents an emerging public health crisis with extensive implications. Evidence indicated that higher temperatures and extreme weather events increase the risks of suicide. By promoting research, improving policy integration and strengthening community resilience, it can alleviate the mental health consequences of climate change and build a more sustainable and equitable future. This undertaking requires collective action, connecting disciplines, regions and sectors to protect mental health in the context of a changing climate. Climate is a dynamic state that is constantly changing. In the coming days we are expected to see significant global climate change, likely significantly impacting mental well-being. Therefore, it is important to keep track of suicidal behaviour in relation to climate change around the world.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10176.
Data availability statement
All data generated or analysed during this study are included in this published article. The full search strategy and extracted dataset are available from the corresponding author upon reasonable request.
Author contributions
D.R.A. conceived and initiated the study idea and led the study design, contextualization, illustration, data interpretation, study selection, literature search, data extraction, manuscript writing and critical revision. S.K.K. contributed to manuscript writing and revision. M.D.A. contributed to the literature search, study selection, quality assessment and risk of bias assessment. R.H. provided critical feedback and substantive comments on the manuscript. All authors reviewed and approved the final version of the manuscript.
Financial support
This study received no specific grant from any funding agency in the public, commercial or not-for-profit sectors and was conducted solely using the authors’ own time and resources.
Competing interests
The authors declare that they have no competing interests.
Ethical approval
Ethical approval was not required for this study as it is a systematic review based exclusively on previously published data and did not involve direct contact with human participants. The review protocol was prospectively registered in PROSPERO under the registration number CRD42024539305.
Appendix

Source: Page et al. (Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl, Brennan, Chou, Glanville, Grimshaw, Hróbjartsson, Lalu, Li, Loder, Mayo-Wilson and McDonald2021b). This work is licensed under CC BY 4.0. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/

 Open access
Open access
Comments
Editor-in-Chief
Cambridge Prisms: Global Mental Health
Full title: A Systematic Review of the Association Between Climate Change and Suicidality Reveals that Climate Indicators Increase Suicide Rates
Short title: Climate Change and Suicide
Dear Editor,
We are pleased to submit our manuscript titled “A Systematic Review of the Association Between Climate Change and Suicidality Reveals that Climate Indicators Increase Suicide Rates” for consideration in Cambridge Prisms: Global Mental Health, in response to your Call for Papers on Self-harm and Suicide: A Global Priority.
This study represents the first comprehensive systematic review examining the association between climate change and suicidality. It was prospectively registered in PROSPERO and includes 43 peer-reviewed studies, making it the largest synthesis to date. Importantly, it evaluates a broad range of climate change variables—including rising temperatures, air pollution, seasonal changes, and extreme weather events—in relation to suicide outcomes across diverse populations and contexts.
Given the escalating global concerns about climate change and its profound consequences for mental health, we believe our findings provide timely and critical evidence. This review not only advances scientific understanding but also informs global suicide prevention strategies and climate adaptation policies. We anticipate it will be of significant interest to researchers, mental health professionals, and policymakers worldwide.
We affirm that this manuscript has not been previously published and is not under consideration elsewhere. All authors contributed substantially, and the research was conducted in adherence to international ethical standards.
Thank you for considering our submission. We look forward to your response and the opportunity to contribute to this important thematic issue.
Yours sincerely,
Darya Rostam Ahmed
on behalf of all authors