

1. Introduction
Researchers and practitioners increasingly acknowledge that improving health and care systems is both urgent and complex. Numerous theories and frameworks have been developed to support such design and improvement efforts, ranging from human-centered design approaches (Reference Ackerman, Nigon, Wait, Ali, Wilkinson-Lee, Cohen, Jones, Cortez, Kelly and FabricantAckerman et al., 2025; Reference Fleming, Coutts, Pochard, Trivedi and SandersonFleming et al., 2025; Reference Kang, Poddar, Luitel, Rimal, Melaku and BlackKang et al., 2025; Reference Melles, Albayrak and GoossensMelles et al., 2021) and quality improvement frameworks (Reference Endalamaw, Khatri, Mengistu, Erku, Wolka, Zewdie and AssefaEndalamaw et al., 2024) to systems approaches (Reference Clarkson, Dean, Ward, Komashie and BashfordClarkson et al., 2018; Reference Komashie, Ward, Bashford, Dickerson, Kaya, Liu, Kuhn, Günay, Kohler and BoddyKomashie et al., 2021). Translating design theories into practice is not a straightforward application but a creative process that requires designers to shape, adapt, and reinterpret theories as malleable design materials through their skills and contextual understanding (Reference Bekker, Skovbjerg, Petersen, Johry, Sepahpour, Blackler, Chamorro-Koc, Gyi, Wilson and MorrisBekker et al., 2025). To bridge the gap between theory and practice, toolkits are promoted as structured and reusable resources that mediate knowledge transfer (Reference Hollanek and GaneshHollanek & Ganesh, 2024; Reference Petterson, Cheng and ChandraPetterson et al., 2023; Reference Wilner, Adavi, Mandava, Bhimdiwala, Frluckaj, Turns and ArifWilner et al., 2024), and promote creative and critical design thinking (Reference Clemente, Vieira and TschimmelClemente et al., 2016; Reference HoHo, 2017; Reference Marquardt, Houben, Beaudouin-Lafon and WilsonMarquardt et al., 2017).
Toolkits can make complex and inconvenient work approachable by breaking it into manageable steps and offering “easy wins” to sustain user engagement (Reference Hollanek and GaneshHollanek & Ganesh, 2024). They aim to provide awareness, structure, and information to support the understanding, selection, and application of related tools and processes (Reference Tidball, Stappers and MulderTidball et al., 2010), as well as enhance designers’ ability to carry out intended actions, and shape their understanding of design problems and solutions (Reference DalsgaardDalsgaard, 2017). In recent years, numerous toolkits and related studies have been developed, and researchers have identified an industry-wide phenomenon of “toolkit-ification” as well (Reference HollanekHollanek, 2025; Reference Hollanek and GaneshHollanek & Ganesh, 2024). However, despite the rapid growth in available toolkits, little is known about on the optimal components or formats of toolkits (Reference Hempel, Miake-Lye, Brega, Buckhold, Hassell, Nowalk, Rubenstein, Schreiber, Spector and KilbourneHempel et al., 2019a; Reference Hempel, O’Hanlon, Lim, Danz, Larkin and RubensteinHempel et al., 2019b). Developing effective toolkits is challenging, as they must go beyond simply compiling tools to provide structured guidance for scoping, planning, and sustaining improvement efforts (Reference Wilner, Adavi, Mandava, Bhimdiwala, Frluckaj, Turns and ArifWilner et al., 2024). Find a way to systematically design high quality technical and methodical toolkits is challenging (Reference Marquardt, Houben, Beaudouin-Lafon and WilsonMarquardt et al., 2017). Therefore, we believe reviewing the existing toolkits is valuable for identifying patterns, gaps, and strategies to guide their future design and development.
1.1. Toolkit taxonomy
A key challenge in studying toolkits is the lack of a single, agreed-upon definition, with terms like “toolbox”, “field guide”, “playbook”, or “blueprint” often used interchangeably (Reference Hempel, O’Hanlon, Lim, Danz, Larkin and RubensteinHempel et al., 2019b; Reference HollanekHollanek, 2025; Reference Hollanek and GaneshHollanek & Ganesh, 2024; Reference Peters, Loke and AhmadpourD. Peters et al., 2021; Reference Wilner, Adavi, Mandava, Bhimdiwala, Frluckaj, Turns and ArifWilner et al., 2024). A toolkit has been described in various ways, for example, as “including multiple tools or methods to approach a given situation, as well as an explicit suggestion of how to use those tools or methods” (Reference Petterson, Cheng and ChandraPetterson et al., 2023) or as “generative platforms designed to create new interactive artifacts, provide easy access to complex algorithms, enable fast prototyping of software and hardware interfaces, and/or enable creative exploration of design spaces” (Reference Ledo, Houben, Vermeulen, Marquardt, Oehlberg and GreenbergLedo et al., 2018). This aligns with a previous study suggesting that human-centered design toolkits can be broadly classified as either methodical or technical, the former consist of collections of methods accompanied by guidance on when and how to apply them, the latter serve as rapid prototyping platforms comprising hardware and software building blocks (Reference Mucha and NebeMucha & Nebe, 2017). Build on this understanding and aligned with our research interests in health and care design and improvement, this study focuses on methodical toolkits. These methodical toolkits may draw on human-centred principles, be informed by design thinking and systems approaches, and/or incorporate risk and management perspectives to address complex societal challenges and achieve transformative impact in health and care, and social wellbeing. Therefore, in this study, we use the term “toolkit”, and related terms such as “guide”, “playbook”, or “methods library”, to refer to a curated collection of structured resources, particularly a set of tools or methods.
1.2. Research question
Considering that digital and interactive toolkit formats have been recognized for their potential to improve accessibility, enable customization, and support collaboration (Reference Dengel, Iqbal, Grafe and ManginaDengel et al., 2022; Reference Wölfel and MerrittWölfel & Merritt, 2013), and that web-based delivery further offers unique advantages for wide dissemination, continuous updating, and engaging diverse user communities (Reference Wang, Wang, Clarkson, Rietjens and MellesWang, Wang, et al., 2024; Reference Wilner, Adavi, Mandava, Bhimdiwala, Frluckaj, Turns and ArifWilner et al., 2024), in this study, we focused on web-based toolkits only.
Our overall objective was to examine toolkit characteristics, content components, and interactive features, and thereby informing the future design and development of such toolkits. Due to space limitations, this paper focuses on examining toolkit characteristics and addressing the following research question: what web-based toolkits are currently available to support health and care design and improvement, and how can they be categorized? The remaining findings will be published in a follow-up article.
2. Method
We conducted a web-based toolkit review inspired by a review of analogue tools for collaborative ideation (Reference Peters, Loke and AhmadpourD. Peters et al., 2021). Our approach combined elements of scoping review methodology (Reference Peters, Loke and AhmadpourM. D. Peters et al., 2021) with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Reference Page, Moher, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl and BrennanPage et al., 2021).
2.1. Search strategy
A web search was performed to identify and characterize web-based toolkits designed for, or applicable to, supporting health and care design and improvement. Our search drew primarily on two key databases: Toolkit Navigator (OPSI, 2011) and Toolbox Toolbox (Reference Theolin, Trigarszky, Elferink and ThakurataJenny Theolin et al., 2017). Toolkit Navigator, developed by the Observatory of Public Sector Innovation (OPSI), provides access to hundreds of freely available innovation toolkits created by public, private, academic, and non-profit organizations. Toolbox Toolbox, developed by a small crew of editors, designers, and facilitators, it offers a curated list of notable business, design, and organizational change toolboxes developed by leading companies, institutions, and practitioners. Both databases were systematically searched to identify all relevant web-based toolkits. The search was completed on 2 May 2025, yielding 192 toolkits from Toolkit Navigator and 176 from Toolbox Toolbox. In addition to these two databases, we employed snowball sampling (Reference GoodmanGoodman, 1961) to expand our search. Most of these additional toolkits were curated by the first author (TW) through prior research activities, expert recommendations, and follow-up searches of related toolkits, and were systematically stored in a dedicated Google Chrome bookmark folder for this study. This process yielded 135 unique links to potential toolkits and resources which were compiled into a master list for screening and analysis. The complete workflow of this study is illustrated in Figure 1.
Study flow

Figure 1 Long description
The flowchart illustrates the process of identifying, screening, and including toolkits for healthcare improvement. The process begins with the identification phase, where toolkits are sourced from databases and snowballing methods. Toolkits from databases include Toolkit Navigator with 192 entries and Toolbox Toolbox with 176 entries. Toolkits from snowballing include Google Search with 143 entries. Duplicates totaling 88 are removed. The next phase is screening, where 423 toolkits are screened. Toolkits are excluded for various reasons: not a toolkit or methods collection (246), not relevant to healthcare, design, or improvement tools (44), not accessible or restricted access (42), primarily highlights commercial product and service promotion (19), requires payment to access core toolkit content or components (14), contains only specialized technical contents (14), not written in English or without a full English translation (7), and not an independent, browser-accessible web-based interactive application or platform (1). Finally, 36 toolkits are included.
2.2. Selection criteria
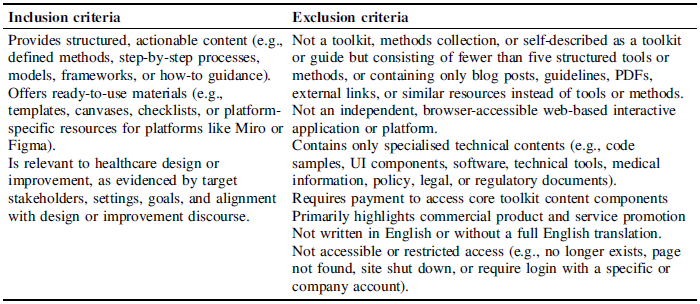
We developed explicit inclusion and exclusion criteria to guide the selection of toolkits from the compiled list, as Table 1 presents. These criteria were informed by our research aim and finalised through multiple rounds of team discussion before screening.
Selection criteria

2.3. Screening process
After de-duplication (88 duplicates removed), a total of 423 toolkits remained for screening. The collected toolkits were included in the final analysis if they met all the inclusion criteria following a two-stage screening process. First, TW assessed the eligibility of the remaining toolkits against the selection criteria and classified them into four categories: included (n=25), excluded (n=279), likely included (n=65), and likely excluded (n=54). Second, toolkits in the “likely included” and “likely excluded” categories were reviewed through team discussion to resolve uncertainties. Following clarification of any ambiguities relative to the criteria and consensus among the team, a total of 36 toolkits met the eligibility criteria and were included for data extraction.
2.4. Data extraction and analysis
For each included toolkit, we manually navigated through the main and sub webpages, extracting structured information related to toolkit characteristics, including the title, one-sentence summary, development team, origin, and target users of the toolkit. We employed a hybrid approach of inductive and deductive thematic analysis (Reference Fereday and Muir-CochraneFereday & Muir-Cochrane, 2006) to identify overarching themes capturing the characteristics of the toolkits. During the extraction process, we used a Google extension (Hypothesis – Web & PDF Annotation) to highlight and annotate key information directly on the toolkit webpages. We then used an Excel spreadsheet (see Appendix 1) to record data related to toolkit characteristics and conducted multiple rounds of review and cross-checking to ensure the data accurately reflected each toolkit.
3. Results
3.1. Overview
Figure 1 shows the flow diagram of the systematic web search. Ultimately, 36 toolkits were included in the review for data extraction. Please note that some records may have had multiple reasons for exclusion, but only the first identified reason was recorded.
3.2. Toolkit characteristics
Table 2 presents the basic characteristics of the 36 included toolkits, including their title and one-sentence summary. Additional details, such as URLs, leading development institutions(s), source of origin, target users and usage scenarios are provided in Appendix 1.
Toolkit characteristics (note: “*” indicates that the toolkit is related to the healthcare context.)

3.3. Classification of toolkits
To categorise the included toolkits, we identified five dimensions: (1) whether they include novel or known tools; (2) whether they target specialised or generic objectives; (3) whether they originate from research or practice-based experience; (4) whether they emphasise risk-reduction or benefit-increase as motivations for use; and (5) whether they are designed for individual- or group-level application.
3.3.1. Novel or known tools
This category examines whether toolkits mainly compile established methods or introduce newly developed tools. Tools were considered known if they reflected widely used approaches, such as journey maps or personas, even when adapted to specific contexts. Most toolkits (n=28), for example, card sorting in the CMD Methods Pack, relied on established tools, a smaller group (n=5) reframed existing methods for particular settings, and only a few (n=3) proposed genuinely new tools, for instance, anti-futures canvas in the Actionable Future Toolkit.
3.3.2. Specialised or generic objectives
Building on previous studies that classify toolkits by their applicability and specificity (Reference Peters, Loke and AhmadpourD. Peters et al., 2021; Reference Wölfel and MerrittWölfel & Merritt, 2013), we grouped the included toolkits into two categories based on their stated objectives: generic and specialised. Generic toolkits (n=32) are broadly applicable across domains and contexts. For example, the Design Kit provides more than 50 tools applicable to many types of design projects and Gamestorming offers 207 games that can be flexibly applied in workshops. In contrast, specialised toolkits (n=4) explicitly constrained to a particular domain (e.g., healthcare, government, or specific technologies). For instance, the AI Blindspot Cards focuses on guiding users through a discovery process to identify unconscious biases and structural inequalities in AI systems, and the Improving Improvement Toolkit supports the application of systems approaches to health and care improvement. Additionally, among these toolkits, nine include case studies to illustrate contextual application, and five specifically feature healthcare-related examples.
3.3.3. Research- or practice-based origins
This category describes where toolkit knowledge mainly comes from. Most toolkits were practice-based (n=22), developed from professional practice, organisational projects, or consultancy experience (e.g., Design Kit, which draws on IDEO’s global human-centred design projects). Some were compiled or adapted (n=9) from multiple existing resources, community contributions, or case study syntheses (e.g., BetterEvaluation, built from contributions by members of the Global Evaluation Initiative network). A smaller group were research-based (n=6), originating from academic research, applied research programmes, or graduate projects (e.g., AI Blindspot Cards, developed through the Berkman Klein Center’s Assembly program at Harvard and informed by research on AI ethics and fairness).
3.3.4. Risk-reduction or benefit-increase motivations
We examined how toolkits encourage use. Most toolkits (n=35) framed their value around positive outcomes, such as greater efficiency, stronger collaboration, enhanced creativity, improved knowledge, and business success. For example, Enterprise Design Thinking states that it can “give you a shared language to align faster”. In contrast, only a small number (n=4) emphasised risks they seek to mitigate, including commercial failure, slow innovation, and social inequities. For instance, the Actionable Futures Toolkit warns that “a lack of an actionable future vision leads to longer time to market, unsuccessful market reach, and reduced ability to act in a constantly changing environment”.
3.3.5. Individual- or group-oriented application
We found that the majority (n=24) are designed to be flexible, supporting both individual self-study and group use, and offering resources that scale from personal exploration to facilitated team sessions. For example, Enterprise Design Thinking combines self-paced learning courses with structured toolkits to help teams align, focus, and apply design thinking to complex organizational challenges. Some toolkits focused mainly on individual use (n=7), while others were primarily designed for group settings (n=5), emphasising workshops and collaborative sessions. For instance, the Design Kit supports individuals in learning human-centered design and starting to solve problems like a designer, while the Actionable Futures Toolkit explicitly recommends a diverse group of 6 to 10 participants for optimal results.
3.4. Five types of toolkit developers
Based on the primary developers identified for each toolkit, most were created by commercial entities (n=17; e.g., Atlassian Team Playbook by Atlassian), academic institutions (n=7; e.g., CMD Methods Pack by HAN University of Applied Sciences and Amsterdam University of Applied Sciences), non-profit organisations (n=6; e.g., Circular Design Guide by the Ellen MacArthur Foundation and IDEO), or public-sector agencies (n=4; e.g., NYC Civic Service Design Tools + Tactics by the NYC Mayor’s Office for Economic Opportunity, Service Design Studio). The remaining toolkits were developed by individuals (n=2; e.g., Project of How Methods by Hyper Island alumni) or had no clear institutional attribution (n=2; e.g., Product Discovery Methods). Notably, several toolkits appear in more than one category when leadership is jointly shared across sectors.
3.5. Seven types of toolkit end-users
Identifying the target users of these toolkits proved challenging. Many toolkits (n=15) refer to their intended users simply as “you”, “your team”, or “your organization”. For example, the Actionable Future Toolkit states that it works for “you in building and aligning a future for an organisation, service or a product.” Based on a subset explicitly specifies end-user roles, we identified seven primary user roles: practitioner (n=17), leader (n=13), facilitator (n=4), policy maker (n=2), evaluator (n=2), learner (n=2), and researcher (n=1). For example, the Continuous Improvement Toolkit targets “professionals, teams, and students,” and the Design Sprint Toolkit specifies “design leaders, product owners, developers, or anyone who is learning about or running Design Sprints.”
4. Discussion
4.1. Principle findings
This study investigated what web-based toolkits are available to support health and care design and improvement, we collected 36 web-based toolkits. Through an analysis of their characteristics, we identified five toolkit characteristics: (1) novel or known tools; (2) specialised or generic objectives; (3) research- or practice-based origins (4) risk-reduction or benefit-increase motivations; and (5) individual- or group-oriented application. We further identified five types of toolkit developers and seven roles of toolkit end-users.
4.2. Toolkit characteristics
4.2.1. Novel vs. known
Consistent with prior reviews (Reference Hempel, O’Hanlon, Lim, Danz, Larkin and RubensteinHempel et al., 2019b), we found that only a few toolkits introduce genuinely new tools. Most rely on well-known methods, such as interviews and journey mapping, often adapting or combining them. Their main contributions lie instead in new ways of framing tools, redesigning templates and instructions, adapting tools to specific contexts through new case studies, or expanding tool collections into broader repositories. Previous work similarly shows that toolkits differ more in organisation than in the tools themselves (Reference Tidball, Stappers and MulderTidball et al., 2010). Toolkits built around known methods usually function as flexible repositories, while those introducing new tools tend to include fewer tools with a guided workflow. To reduce redundancy, future toolkits should more clearly state their unique contributions.
4.2.2. Generic vs. specialised
Most toolkits are generic, designed to support a broad design and improvement process. They usually include widely used tools for activities such as research, teamwork, and evaluation, and often add case studies to show how tools apply in specific situations. Although design processes are similar across domains, effective use in health and care requires stronger contextual information and healthcare-related case studies to help explore and elaborate toolkits in greater depth (Reference Ledo, Houben, Vermeulen, Marquardt, Oehlberg and GreenbergLedo et al., 2018; Reference Wang, Zhu, Qian, Giunti, Goossens and MellesWang, Zhu, et al., 2024). A few toolkits are specialized and tailored to a specific design or improvement context, such as healthcare, AI, or government, and offering tailored knowledge and guidance for those contexts. Consistent with previous studies, we believe that specialised toolkits integrating domain knowledge, providing contextual guidance are more likely to support effective practice change (Reference Godinho, Ansari, Guo and LiawGodinho et al., 2021; Reference Hempel, O’Hanlon, Lim, Danz, Larkin and RubensteinHempel et al., 2019b). To better support health and care design and improvement, future efforts should prioritise domain-specific toolkits or enrich generic ones with healthcare case studies and contextual guidance.
4.2.3. Practice-based vs. research-based
Practice-based toolkits, often created by public or commercial organisations, focus on accessibility and practical use but usually lack systematic evaluation or strong evidence, aligning with previous findings that many toolkits are largely descriptive and have limited empirical validation (Reference Hempel, O’Hanlon, Lim, Danz, Larkin and RubensteinHempel et al., 2019b). In contrast, research-based toolkits, developed mainly by academic institutions, provide stronger theoretical and methodological foundations but are often harder for practitioners to adopt without translation or facilitation, consistent with previous findings that academic collections emphasise theory and references (Reference Tidball, Stappers and MulderTidball et al., 2010). We believe this suggests a need for stronger cross-sector collaboration: practice-based toolkits could benefit from the evidence standards and methodological depth of academia, while research-based toolkits could increase their practical impact by drawing on the usability, dissemination strategies, and contextual sensitivity that characterize practice-based approaches. As previous study suggested, let the toolkit be informed by research but remain “jargon-free” through consultations with practitioners (Reference Hollanek and GaneshHollanek & Ganesh, 2024). Additionally, providing information on supporting data for the practices or strategies on which the toolkit is based, promoting evidence-based practices is suggested (Reference Hempel, Miake-Lye, Brega, Buckhold, Hassell, Nowalk, Rubenstein, Schreiber, Spector and KilbourneHempel et al., 2019a).
4.2.4. Risk-reduction vs. benefit-increase
Building on our findings, most toolkits motivate adoption by emphasising promised benefits, such as improved efficiency, collaboration, creativity, and business outcomes, rather than risks to be avoided. However, it remains unclear how different motivational framings influence adoption, trust, and sustained use. Moreover, consistent with prior research showing that many methods claimed impacts lack strong empirical support (Reference Cash, Daalhuizen and HekkertCash et al., 2023), we found that these benefits are often presented in a promotional manner rather than grounded in robust evidence. Future research should examine how motivational strategies shape user engagement, while toolkit developers should more rigorously substantiate their claimed impacts.
4.2.5. Inclusive vs. selective
Most toolkits target broad audiences, from novices to experienced practitioners, and support both individual and team-based use, reflecting an intention to maximise accessibility across disciplines. This aligns with a previous study on toolkits for advancing diversity and inclusion in AI (Reference Hollanek and GaneshHollanek & Ganesh, 2024), which found that their intended audience is everyone in the AI ecosystem. While such inclusivity is valuable, prior studies highlight persistent mismatches between toolkits and users’ skills, needs, and contexts, which can hinder adoption and effective use (Reference Ledo, Oehlberg and GreenbergLedo et al., 2017; Reference Tidball, Stappers and MulderTidball et al., 2010). “Design methods are like toothbrushes, everyone uses them, but no one likes to use someone else’s” (Reference Harrison and TatarHarrison & Tatar, 2011). While this may sound like a joke, it raises an important question: why are people often reluctant to use toolkits developed by others? Perhaps it is because many toolkits, in trying to design for everyone, end up fitting no one particularly well. Designing for “everyone” often results in generic content, unclear user fit, and increased cognitive load, as users must navigate extensive materials to find relevant value. We therefore suggest that toolkits should not pursue unlimited inclusivity but instead aim for a balanced approach that clarifies their boundaries and combines inclusivity with a degree of selectivity.
4.3. Limitations and future research
This study has several limitations. First, although we aimed for a comprehensive collection of web-based toolkits, some eligible resources may not have been identified due to database constraints and the dynamic nature of online platforms. To mitigate this, we applied a snowballing strategy throughout the search process to reduce potential bias. Second, we did not evaluate toolkit quality, impact, or effectiveness, as our focus was on mapping developers and structural characteristics rather than outcomes of use. While we excluded clearly commercial or inaccessible platforms, the included toolkits should be interpreted as illustrative examples rather than evidence of best practice. Third, while our focus was on toolkits relevant to health and care design and improvement, only five toolkits directly related to the healthcare domain. Nevertheless, we consider general design and improvement toolkits to be a useful starting point for generating insights applicable to healthcare contexts.
According to our research findings, we suggest that future research should explore ways to better integrate practice-based and research-based approaches in toolkit development. Toolkits developed through research should be refined in practice to align with practitioners’ needs, while practice-based toolkits should be systematically evaluated through research to ensure rigor and effectiveness. As previous study pointed out, many toolkits designed to share health knowledge or support practice change lack clear evidence bases and are rarely evaluated for effectiveness. To better inform health and care, toolkits should clearly describe their content, identify evidence-based components, and assess their impact on both clinical and implementation outcomes (Reference Barac, Stein, Bruce and BarwickBarac et al., 2014). Another future research direction is to consider how toolkits can balance inclusivity and selectivity. On the one hand, toolkits should aim to accommodate diverse users and needs; on the other hand, they must also reduce ambiguity to avoid overwhelming users or leaving them uncertain about the toolkit’s relevance. The previous study recommend that toolkits should clearly state their purpose, audience, and context of use; provide summaries, navigation aids, and actionable steps; disclose development processes, supporting evidence, and conflicts of interest; and include supporting materials and measures to assess effectiveness (Reference Hempel, Miake-Lye, Brega, Buckhold, Hassell, Nowalk, Rubenstein, Schreiber, Spector and KilbourneHempel et al., 2019a).
5. Conclusion
This study systematically reviewed 36 web-based toolkits relevant to health and care design and improvement. Most were generic, practice-based toolkits developed by commercial or academic actors, broadly supporting both individual and group use. For future development, toolkit developers should more clearly articulate their unique contributions, such as introducing novel tools, offering new conceptual frameworks for organising tools, refining templates and instructions to improve usability, adapting tools through contextualised case studies, or expanding repositories to provide broader overviews. To better support health and care contexts, future efforts should prioritise healthcare-specific toolkits or enrich generic ones with healthcare-related case studies and guidance. Rather than aiming to “design for everyone,” developers could also prioritise user groups and offer tailored entry points that reflect users’ diverse backgrounds and experiences, thereby reducing cognitive load and enhancing usability. Moreover, collaboration across academia, industry, and government may play a vital role in addressing complex societal challenges. Jointly developed toolkits can integrate the methodological rigour of research with the practical relevance and contextual sensitivity of practice-based approaches. Together, these findings provide an overview of current toolkit practices and offer insights into content innovation, user prioritisation, and cross-sector collaboration, informing the future design and development of web-based toolkits in health and care design and improvement contexts.



 Open access
Open access