


Severe mental illnesses (SMIs, referring here to schizophrenia-related and bipolar disorders) are associated with numerous adverse impacts on quality of life. Reference Bailey, Alvarez-Jimenez, Garcia-Sanchez, Hulbert, Barlow and Bendall1,Reference Bertelsen, Jeppesen, Petersen, Thorup, Øhlenschlæger and Quach2 Individuals who are victims of violence have an increased risk of developing psychotic disorders, Reference Chapple, Chant, Nolan, Cardy, Whiteford and McGrath3,Reference Hart, de Vet, Moran, Hatch and Dean4 with the reported prevalence of victimisation as high as 60% in those with SMI. Reference Walsh, Moran, Scott, McKenzie, Burns and Creed5 Victimisation has also been found to be associated with more severe psychotic illness, lower response to treatment and consequent higher doses of prescribed mood stabilisers and antipsychotics. Reference Bloomfield, Yusuf, Srinivasan, Kelleher, Bell and Pitman6–Reference Schneeberger, Muenzenmaier, Castille, Battaglia and Link9 It is also associated with higher rates of comorbidity, hospitalisation and suicide attempts, and with poorer functioning and response to treatment, including dopamine antagonists. Reference Aas, Andreassen, Aminoff, Færden, Romm and Nesvåg7,Reference Levine, Levav, Yoffe and Pugachova10–Reference Kraan, van Dam, Velthorst, de Ruigh, Nieman and Durston12 However, research has focused on either victimisation as a risk factor for psychosis or cross-sectional relationships with symptom severity and functioning, Reference Vila-Badia, Butjosa, Del Cacho, Serra-Arumí, Esteban-Sanjusto and Ochoa13,Reference Misiak, Krefft, Bielawski, Moustafa, Sąsiadek and Frydecka14 and there is a lack of prospective evidence on victimisation as a risk factor for clinical outcomes in these disorders.
Growing volumes of data from electronic mental healthcare records provide valuable opportunities for investigating victimisation as a predictor of course and outcome in SMI. In the absence of widely adopted structured instruments in routine practice, victimisation is primarily recorded in unstructured text fields within the records, which presents a challenge for data capture. However, natural language-processing (NLP) algorithms are increasingly being used to extract information on clinical entities such as symptoms and treatment Reference Robson, Spaducci, McNeill, Stewart, Craig and Yates15–Reference Wang, Wang, Rastegar-Mojarad, Moon, Shen, Afzal and Liu17 from unstructured text in electronic mental health records, ‘unlocking’ this information for use in large clinical populations that are potentially more representative than recruited samples from clinical practice. One recently developed NLP application ascertains violence according to its presence and subtypes (physical, domestic, sexual), Reference Botelle, Bhavsar, Kadra-Scalzo, Mascio, Williams and Roberts18 and in this study we investigated the extent to which victimisation recorded early in the course of specialist mental healthcare was associated with adverse clinical outcomes in patients with SMI, adjusted for previously established potential confounders. Reference Conus, Cotton, Schimmelmann, McGorry and Lambert11,Reference Vila-Badia, Butjosa, Del Cacho, Serra-Arumí, Esteban-Sanjusto and Ochoa13,Reference Bhavsar, Sanyal, Patel, Shetty, Velupillai and Stewart19,Reference Mann, Fisher, Major, Lawrence, Tapfumaneyi and Joyce20
Method
We extracted patient data from the case register of the South London and Maudsley NHS Foundation Trust (SLaM), a comprehensive secondary mental healthcare provider serving around 1.3 million residents in four boroughs of south-east London (Croydon, Lambeth, Lewisham and Southwark). SLaM services have used electronic health records since 2006, and in 2008 its Clinical Record Interactive Search (CRIS) platform was established to enable research use of deidentified data from the full record. CRIS is approved as a data resource for secondary analysis, including the analysis for this project (Oxford Research Ethics Committee C, reference no. 23/SC/0257; IRAS project ID: 326477). Pre-structured data from the source record available in CRIS have been extensively supplemented over the past 10–15 years, with entities derived from source text fields via over 100 developed NLP algorithms, detailed in an open-access catalogue 21 and including the above-mentioned algorithm for violence victimisation, as well as algorithms for medication use and symptom profiles used to generate covariates. Diagnoses are routinely recorded in a structured format according to ICD-10 codes.
CRIS data were extracted for all individuals aged 18 years and over who had received SLaM care between January 2007 and October 2022, with a primary diagnosis at any point in SLaM care of schizophrenia or related disorder (ICD-10 F20x–29x), manic episode (F30x) or bipolar disorder (F31x). The sample was restricted to those with active referrals of at least 3 months following the first face-to-face contact with SLaM services, and a historic cohort study was assembled by ascertaining ‘baseline’ exposure status and covariates over these first 3 months and ascertaining outcomes from the 3-month point onwards. The NLP algorithm ascertaining interpersonal violence was used to extract data on victimisation (i.e. receipt of violence) recorded during the 3-month baseline period, and to classify this according to physical, sexual and domestic types/contexts. Reference Botelle, Bhavsar, Kadra-Scalzo, Mascio, Williams and Roberts18 Victimisation was affirmed when the label referred to the patient as the recipient of the violence ascertained (rather than perpetration/witnessing status). Physical violence included violence using physical force or causing or having increased risk of causing physical injury. Sexual violence included unwanted sexual acts, unwanted sexual comments or advances or unwanted attempts to obtain a sexual act (e.g. rape, sexual harassment, sexual assault, forced marriage, stalking and reproductive coercion and control). Domestic violence included violence between family members, intimate partners, former intimate partners and household members. Reference Botelle, Bhavsar, Kadra-Scalzo, Mascio, Williams and Roberts18 ‘Any victimisation’ as a category was defined on the basis of any mention of any of the three victimisation types (physical, sexual or domestic). A binary variable was generated of any mention versus no mention of victimisation (categorised as physical, sexual, domestic or any type). Previous publications have measured precision (the proportion of mentions labelled as ‘positive’ that are actually positive), recall (the proportion of all actual positive mentions that were correctly identified) and F1 (the harmonic mean of precision and recall, combining them into a single metric), evaluating algorithm output against manually annotated source text, and have reported high scores on these measures. This includes high scores for general victimisation mentions, and for mentions of domestic, physical and sexual violence specifically Reference Botelle, Bhavsar, Kadra-Scalzo, Mascio, Williams and Roberts18,Reference Mason, Bhavsar, Botelle, Chandran, Li and Mascio22 ). More information regarding the NLP app’s development, drawn from previous publications, can be found in Supplementary Materials 1. Reference Botelle, Bhavsar, Kadra-Scalzo, Mascio, Williams and Roberts18,Reference Mason, Bhavsar, Botelle, Chandran, Li and Mascio22
Age, gender, ethnicity, diagnosis and neighbourhood deprivation were ascertained at, or closest to, the first clinical contact. Age was categorised into 10-year increments for descriptive statistics, but was retained in 1-year intervals for inclusion as a covariate in regression analyses. Ethnicity was categorised into six groups for analysis: ‘White British’ (British), ‘White other’ (Irish or any other White background), ‘Black’ (Caribbean, African or any other Black background), ‘Asian’ (Indian, Bangladeshi, Pakistani, Chinese or any other Asian background), ‘Other/mixed’ (White and Asian, White and Black Caribbean, White and Black African any other ethnic group) and ‘Not stated’. Inclusion primary diagnoses were categorised into the three categories previously stated (F20x–29x, F30x and F31x), and any listed secondary or additional diagnoses of substance misuse disorder (F1x), personality disorder (F6x) and learning disability (F7x, F84x) were also ascertained as binary variables to be considered as covariates. Additional diagnoses (e.g. depression and anxiety) were not included as covariates, because these are common comorbidities in individuals with SMI and therefore may be a part of the patient’s broader clinical syndrome rather than independent confounders. For the address at first contact, Index of Multiple Deprivation (‘neighbourhood deprivation’) was ascertained: a public-domain measure of socioeconomic status combining economic, social and housing dimensions Reference Noble, McLennan, Wilkinson, Whitworth and Barnes23 from national census returns and collated for Lower-level Super Output Areas (standard national enumeration units with around 1500 residents).
The following clinical covariates were ascertained for the first 3 months of care as binary present/absent variables: (a) home treatment team (HTT) care; (b) in-patient or liaison service input; (c) emergency event (mental health assessment in emergency care); (d) receipt of antidepressants or mood stabilisers (ascertained from recorded medication receipt in text fields via a bespoke NLP algorithm; precision (0.71–0.99) and recall (53–94% 21 ); and (e) recorded symptoms in this time period ascertained via individual NLP algorithms as binary (present/absent) variables and scaled according to the following subscales: positive schizophreniform (0–16), negative schizophreniform (0–12), manic (0–8), disorganisation (0–8) and catatonic (0–4). Precision and recall for each NLP symptom can be found in the CRIS NLP catalogue. 21 We focused on outcomes relating to mortality and use of healthcare services/help-seeking rather than clinical presentation. Considering this, aspects related to clinical presentation (e.g. symptom profiles and medication use that was not SMI-specific (e.g. antidepressants and mood stabilisers)) were included as clinical covariates rather than considered outcomes.
Outcomes were extracted over the period starting from 3 months following the first clinical contact, using structured data. These comprised: (a) number of different antipsychotics prescribed; (b) number of attended events (face to face or virtual contact) and dates of the first occurrences of the following events: (c) emergency care receipt (occurrence of emergency care mental health assessment); (d) crisis (HTT) input (input from a HTT – a model of care providing daily community monitoring as an alternative to in-patient admission); (e) evidence of mental health in-patient care; (f) compulsory in-patient care detention under the Mental Health Act (MHA); and (g) mortality (if the patient has died; date of death). Antipsychotic use was considered an outcome, because we felt that antipsychotic use after the index date could be investigated as a proxy for longer-term treatment resistance, whereas the number of antipsychotics in the first 3 months would have been measuring other processes concerned with immediate management.
Statistical analysis
The binary exposures under investigation were presence of recorded victimisation (experienced violence) during the first 3 months following initial clinical contact: (a) any victimisation; (b) physical victimisation; (c) domestic victimisation; and (d) sexual victimisation. The control group comprised patients who had no mention of physical, domestic or sexual victimisation within their clinical records during the first 3 months following initial clinical contact. Initial analyses compared covariates by exposure status.
Cox regression models were used to investigate associations with risk of emergency care, in-patient care, MHA detention and mortality. Poisson regression models were used to estimate associations with number of antipsychotics received and number of attended healthcare events with a mental health professional (restricted to participants who did not have in-patient care in the 12-month follow-up period). For Cox regressions, censoring points were date of death, date of outcome event and extraction date (3 February 2023). For Poisson regressions, duration of follow-up (from the 3-month point to data extraction date) was included as a covariate in all models.
The following regression models were assembled for each clinical outcome: model 1 was unadjusted; model 2 controlled for age and gender; model 3 additionally controlled for ethnicity and neighbourhood deprivation; and model 4 additionally controlled for primary diagnosis, secondary diagnoses, baseline in-patient/liaison care, emergency care, antidepressant use, mood stabiliser use and symptom scales. Because baseline clinical variables may be on the causal pathway (between victimisation and clinical outcomes) or might be potential confounders, we included these within model 4 as sensitivity analysis (where we can compare the regression models with and without these variables). All regression results were Bonferroni-adjusted to control for multiple comparisons when interpreting p-values. In secondary analyses, regression models 3 and 4 for each outcome were conducted on subsamples of the cohort stratified by gender; this was an a priori stratified analysis, given probable gender differences in violence context.
Competing risks of mortality may affect the incidence rate of the event of interest (emergency assessment, crisis (HTT) care, in-patient care, MHA admission). In the presence of competing risks including mortality, traditional survival analysis such as Cox proportional hazard regression may introduce biases into the estimation of survival probability. The competing risk regression, a semi-parametric modelling approach, uses sub-distribution hazard (SDH) function, Reference Fine and Gray24,Reference Austin and Fine25 where patients who have experienced competing events are not censored but remain in risk sets. This includes patients who have experienced competing events such as mortality, even if they are not at risk of the event of interest separately (emergency assessment, crisis (HTT) care, in-patient care, MHA admission). The Fine–Gray model is appropriate for predicting an individual’s risk. Considering this, as a sensitivity analysis, competing risk regression models were created for competing risk of mortality and SDH ratios with 95% confidence intervals; these focused on primary associations (between any victimisation and hazards outcomes in the full sample) to check for consistency in findings.
Results
The cohort comprised 16 372 individuals, 72% of whom had an ICD-10 F20–29 diagnosis, 24% an F31 diagnosis and 4% an F30 diagnosis (Supplementary Table 1). The largest group were aged 21–30 years, and a small majority of individuals were male. Nearly all characteristics differed significantly by exposure status (Supplementary Table 1). Recorded victimisation of all types was over-represented in younger age groups; in those from Black ethnic groups; in those with schizophrenia-related primary diagnoses; in those with any of the comorbid secondary diagnoses; and in those receiving higher levels of care or with higher medication use. A female predominance was apparent for recorded domestic and sexual victimisation, but not significantly for physical victimisation. Levels of recorded symptoms were lower for those experiencing victimisation of any sort.
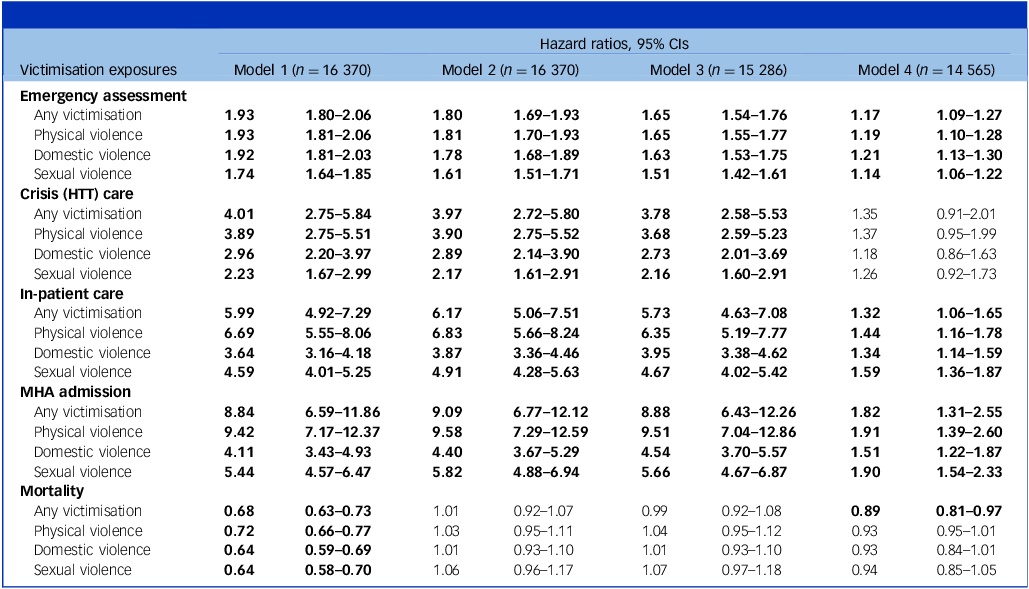
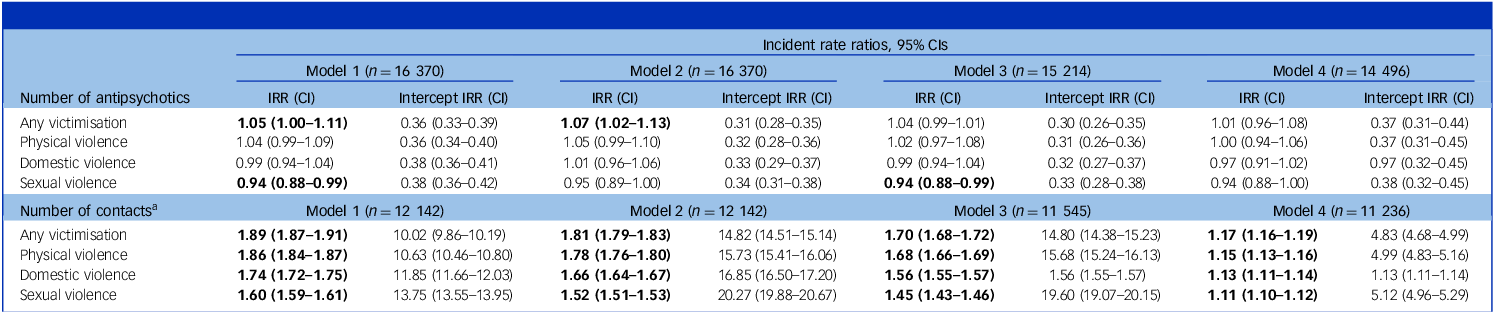
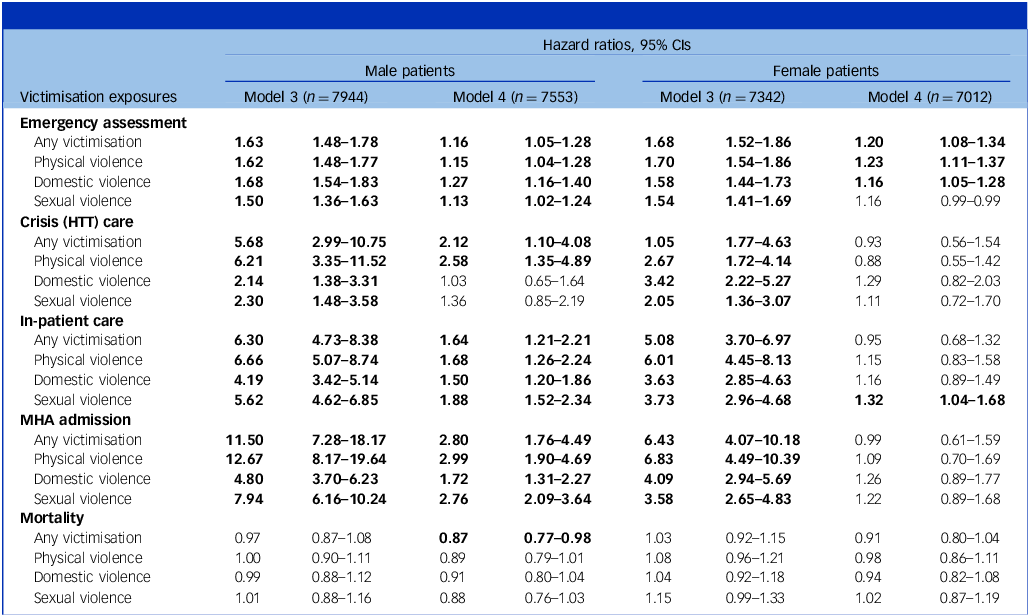
Victimisation was associated with significantly poorer outcomes relating to emergency assessment, crisis care, in-patient care and MHA admission following adjustment for sociodemographic factors (Table 1), with all remaining significant, apart from crisis care, following further adjustment for baseline clinical status (Table 1; model 4). Within gender-stratified analyses (Table 3), these results remained significant for both males and females separately in models adjusting for sociodemographic factors. However, the significantly poorer outcomes for in-patient care and MHA admission following further adjustment for baseline clinical status were significant for male patients only (Table 3). Confidence intervals overlapped for all definitions of victimisation, with no consistent ranking in the strengths of association. Although there were no associations with mortality for most victimisation groups individually in any of the models, there was a significant negative association between mortality and ‘any victimisation’ within models 1 and 4. Poisson regression analyses (Table 2) showed no association between any victimisation group and number of different antipsychotics received following adjustment for sociodemographic factors (model 3) or further adjustment for baseline clinical status (model 4), either in the total sample or for female and male patients analysed separately (Table 4). However, there was a significant association pre-adjustment (Table 2; model 1). Poisson regression analysis (Table 2) showed significant associations between all victimisation exposures and higher number of attended events, which persisted following adjustment for sociodemographic factors (model 3) and baseline clinical status (model 4). These associations were also significant for both male and female patients when analysed separately (Table 4).
Cox proportional hazards analyses of clinical outcomes associated with baseline victimisation exposures

HTT, home treatment team; MHA, Mental Health Act.
Model 1: controlling for follow-up time; model 2: model 1 plus age and gender; model 3: model 2 plus ethnicity; model 4: model 3 plus primary diagnosis, secondary diagnoses (substance misuse, intellectual disability, personality disorder), baseline receipt of crisis (HTT) input, in-patient/liaison care, emergency assessment, antidepressant treatment, mood stabiliser treatment and summed positive, negative, manic, disorganised and catatonic symptoms.
Figures in bold font represent significant findings following Bonferroni adjustment correcting for multiple comparisons.
Poisson regression analyses of victimisation exposures at baseline, subsequent number of antipsychotics received and number of contacts

IRR, incidence rate ratio.
Model 1: controlling for follow-up time; model 2: model 1 plus age and gender; model 3: model 2 plus ethnicity; model 4: model 3 plus primary diagnosis, secondary diagnoses (substance misuse, intellectual disability, personality disorder), baseline receipt of crisis (HTT) input, in-patient/liaison care, emergency assessment, antidepressant treatment, mood stabiliser treatment and summed positive, negative, manic, disorganised and catatonic symptoms.
a. Restricted to participants who did not have in-patient care in the 12-month follow-up period. Figures in bold font represent significant findings following Bonferroni adjustment correcting for multiple comparisons.
Gender-stratified Cox proportional hazards analyses of clinical outcomes associated with baseline victimisation exposures

HTT, home treatment team; MHA, Mental Health Act. Models are identical to those described in Table 1. Figures in bold font represent significant findings following Bonferroni adjustment correcting for multiple comparisons.
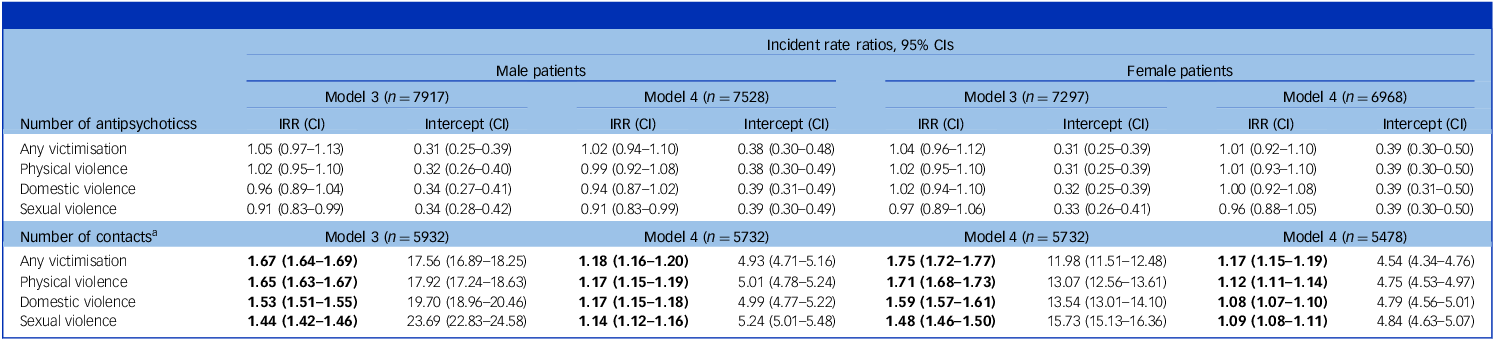
Gender-stratified Poisson regression analyses of victimisation exposures at baseline and subsequent number of antipsychotics received

IRR, incidence rate ratio.
Models are identical to those described in Table 2.
a. Restricted to participants who did not have in-patient care in the 12-month follow-up period.
Figures in bold font represent significant findings following Bonferroni adjustment correcting for multiple comparisons.
Hazards of crisis care for any victimisation were significantly increased after adjusting for sociodemographic factors (model 3) in both genders, but only physical victimisation was significantly increased following adjustment for both models 3 and 4 specifically in male patients. Associations with in-patient care and MHA admission were significant only in male patients following additional adjustment for baseline clinical status. The association between any victimisation and lower mortality in model 4 was significant specifically for men only (Table 3). Associations with number of antipsychotics (Table 4) were non-significant for both men and women in both models 3 and 4. Associations with number of attended events (Table 4) was significant for both genders independently in both models. These associations found for both women and men were positive for all types of victimisation across both models.
As summarised in Supplementary Table 2, there were no substantial differences between Cox proportional model hazard ratios and SDH ratios produced in the competing risk regression.
Discussion
To our knowledge, this is the first longitudinal study to examine the relationship between victimisation and clinical outcomes in patients with SMI using large-scale clinical health record data. Following adjustment for sociodemographic factors alone, victimisation recorded in the first 3 months following presentation predicted subsequent emergency assessment, crisis care, in-patient care and MHA-enforced in-patient care specifically, as well as higher numbers of attended clinical events. Following further adjustment for measures of clinical status over those 3 months, associations with higher risk of emergency assessment, in-patient care, MHA admission and higher number of attended events persisted. Most outcomes were similar in men and women following sociodemographic adjustment, but only emergency assessment outcomes remained consistently significant in women after further adjustment for clinical characteristics. A significant negative association was found between victimisation and mortality in the unadjusted model 1, and in the fully adjusted model 4 that was apparent only in men on further stratification. There were no consistent differences between the three subtypes of recorded victimisation (physical, domestic, sexual) as exposures.
The findings relating to increased hospitalisation are consistent with previous studies focusing on the effects of sexual victimisation in people with psychosis, Reference Turner, Harvey, Hayes, Castle, Galletly and Sweeney26 and with studies that have reported general, physical and sexual victimisation to be associated with frequency, duration and age of first hospitalisation. Reference Schenkel, Spaulding, DiLillo and Silverstein27,Reference Read28 In relation to MHA detention, most previous studies in SMI have focused on ethnicity as a predictor, Reference Mann, Fisher, Major, Lawrence, Tapfumaneyi and Joyce20 or on traumatisation occurring as a result of detention rather than as a predictor of future detainment. Reference Tarrier, Khan, Cater and Picken29 One previous study reported no association between psychotic experiences or involuntary detention and subsequent traumatic symptoms (in the absence of a life-threatening trauma). Reference Jackson, Knott, Skeate and Birchwood30 Although little research has specifically measured whether victimisation increases hospital contact, research has found reduced symptom improvement in patients with psychosis and previous victimisation. Reference Bloomfield, Yusuf, Srinivasan, Kelleher, Bell and Pitman6 Considering gender, although we had anticipated that victimisation might show different strengths of association between men and women, our findings for this were inconsistent across the different models, outcomes and type of victimisation. In model 3, adjusting for sociodemographic factors, most hazard ratios (Table 3) were similar between men and women, the exceptions being associations of physical victimisation with crisis care and MHA admission, and sexual victimisation with in-patient/MHA admission, all of which were markedly stronger for men compared with women. However, when further adjusted for clinical factors (model 4), most of these associations remained significant in men but most were no longer significant in women. On the other hand, Poisson models of number of clinical contacts were similar between men and women in both models. For crisis and in-patient outcomes, baseline clinical status therefore appears to be acting more strongly as a confounding factor for women than for men, perhaps indicating clinical pathway differences that emerge earlier; however, these conclusions must be viewed as speculative and requiring replication and further evaluation.
Our findings emphasise the potential importance of victimisation as a prognostic marker (consistent with previous literature Reference Schenkel, Spaulding, DiLillo and Silverstein27 ), although they do not support substantial or consistent differences between broad categories of violence received, suggesting that the personal impact of the experience is more important across these subtypes. In considering the meaning of the final adjusted (model 4) associations, it is important to bear in mind that covariates were ascertained over an important period of clinical care, namely the first 3 months following referral. Some of these covariates may therefore be causal pathway rather than confounding factors – for example, pre-referral trauma might result in worse clinical status or more intensive (e.g. in-patient/MHA) care shortly after referral, accounting in turn for associations with later outcomes; the model 4 regression output may therefore represent over-adjustment. Of note, all associations were substantially attenuated when adjusted for these clinical measures, supporting an important role of early clinical presentation and care receipt. If correct, this process may be particularly pertinent in female patients, with more independent subsequent associations observed in men. Unlike previous studies, Reference Misiak and Frydecka8,Reference Schneeberger, Muenzenmaier, Castille, Battaglia and Link9 victimisation (of all types) was not associated with increased frequency of prescribed antipsychotics.
Numerous studies have reported excess mortality in patients with SMI compared with the general population, potentially due to medical comorbidity, adverse social factors and unhealthy lifestyles, and to increased suicide rates. Reference Castagnini, Foldager and Bertelsen31,Reference Castagnini and Bertelsen32 Associations have been reported between victimisation and alcohol and substance misuse and increased suicide rates, Reference Conus, Cotton, Schimmelmann, McGorry and Lambert11 and increased psychiatric medication use, Reference Schneeberger, Muenzenmaier, Castille, Battaglia and Link9 although no study has investigated associations of victimisation with mortality in SMI. Our study found a negative association between victimisation and mortality in the unadjusted model 1 and in one of the adjusted models (model 4). This negative association appears to have been confined to male patients, as suggested in the gender-stratified analysis, possibly because male patients who engaged sufficiently with services to report victimisation are also more able to seek healthcare and adhere to treatments. However, this interpretation is speculative and requires further investigation.
Strengths and limitations
Strengths of the study include the large, naturalistic sample and routine, ‘real-world’ outcomes evaluated. Electronic health records, universally implemented in many settings, provide valuable opportunities for investigating novel research questions in data resources that are both large and granular. In mental health data science, this is being realised via the growing use of NLP applied to extract clinical entities of interest at scale from the extensive text data in the source records, exemplified by the algorithms for victimisation deployed in this analysis. Important covariates, such as medication use and symptom profiles, can also be derived in a similar way. Routine data resources should be seen as complementary to traditional research approaches – providing substantially larger and more representative clinical samples than would be possible in a recruited cohort, but subject to challenges in the quality and availability of data achievable because health records are not set up for research objectives.
Considering the sample, its definition and the timing of exposures were based on first contact with one catchment-based mental health service (SLaM). Although we believe that the majority of cases will thereby have been included at their first presentation, we do not have information on past mental healthcare contact and are not able to exclude those with earlier diagnoses from other providers migrating into the catchment and studied from a later point in their disorder. Also, no limitation was placed on the timing of the subsequent SMI diagnosis, bearing in mind diagnostic delays in routine practice; therefore, first presentations cannot all be assumed to reflect SMI emergence.
It is important to consider that the NLP victimisation algorithm can ascertain this exposure only in patients who were willing to report any victimisation experience, and whose clinicians asked about this in the first place and recorded the experience in a way that could be ascertained. These patients may be different from those who had been exposed to victimisation but whose exposure was not ascertained and/or reported and/or recorded. Reference Read, Harper, Tucker and Kennedy33,Reference Acierno, Resnick and Kilpatrick34
Another current limitation of the NLP victimisation algorithm used in our analyses is that it does not attempt to characterise the timing of the victimisation experiences, thus conflating recent experiences (including those occurring during the 3-month ‘baseline’ assessment period) from more distant (e.g. childhood) exposures, as well as discrete and sustained exposures. Therefore, whereas it was possible to separate exposure and outcome ascertainment, it was not possible to disentangle the relative timings of exposures and covariates (hence the limitation of model 4 analyses described earlier), or to consider the effects of post-observation victimisation on clinical outcomes. Temporality is a feature that is being sought in ongoing development of the source algorithms. In addition, we did not attempt to consider the causative effects of violence perpetration or witnessing, Reference Green, Browne and Chou35,Reference Ranu, Kalebic, Melendez-Torres and Taylor36 and violence type/context was characterised only very broadly. We did not include other mental health disorders (e.g. depression and anxiety) as covariates, because these are common comorbidities in SMI and may not represent independent confounders. Outcome measurements had the advantages of being focused on clinically salient events, optimally ascertained in routine data sources, but will have been missed in patients who migrated out of the catchment, although we know of no reasons to suppose that exposure–outcome relationships would have influenced out-migration.
Implications
Our results indicate that experiences of violence that are recorded in routine mental healthcare shortly after referral predict worse subsequent service outcomes for people with SMI. There are several potential clinical implications from these findings. More assertive screening of previous and contemporaneous victimisation should be considered in routine practice for more effective prevention strategies to be offered. This is imperative considering the high prevalence of victimisation seen in previous research, as well as the lack of adequate screening highlighted in this population. Reference Read, Harper, Tucker and Kennedy33 Increased screening would allow more patients to be provided with specialist and effective trauma-focused treatment. Reference Bloomfield, Chang, Woodl, Lyons, Cheng and Bauer‐Staeb37 Additionally, the study raises the importance of staff building a therapeutic engagement with patients to ensure that they feel comfortable disclosing victimisation experienced and are subsequently more open to trauma-informed or focused treatment. Given that victimisation was associated with increased MHA detention and emergency events, it is also important to consider how trauma-informed care could reduce re-traumatisation from subsequent mental health treatment. Future research should investigate these relationships further – for example, ascertaining any differential impact on early versus later care receipt, and interrelationships between effects on clinical severity, medication requirements and service responsiveness.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjp.2026.10648
Data availability
The security model for the source data (approved by successive Research Ethics Committees over the past 15+ years) does not permit export to open science platforms because it is directly derived from patient records, and it would not be possible to guarantee absolute anonymity with the variables represented. The source data are archived within an appropriately secure NHS domain and can be externally accessed with appropriate clearance; please contact the corresponding author (R.S.) regarding this.
Author contributions
A.J.C.M. formulated the study question and design, completed the forms required for data collection, analysed the data and wrote the first and updated drafts of the paper. R.S. supervised the project from study question formulation and design, through data collection to the final version of the paper, including reviewing data analysis methods. All authors commented and critically reviewed drafts of the paper, including commenting on data analysis and results interpretation and giving final approval for the final published version.
Funding
A.J.C.M., G.K.-S., G.P. and R.S. are part-funded by the National Institute for Health Research (NIHR) Biomedical Research Centre at the South London and Maudsley NHS Foundation Trust and King’s College London. G.K.-S. has also received funding by Violence and Abuse Mental Health Network UKRI. R.S. is additionally funded by (a) NIHR Applied Research Collaboration South London (NIHR ARC South London) at King’s College Hospital NHS Foundation Trust and (b) the DATAMIND HDR UK Mental Health Data Hub (MRC grant no. MR/W014386). Both R.S. and A.R. are funded by the UK Prevention Research Partnership (Violence, Health and Society, no. MR-VO49879/1), an initiative funded by UK Research and Innovation Councils, the Department of Health and Social Care (England), the UK devolved administrations and leading health research charities. V.B. is funded by an NIHR Advanced Fellowship in health services research (no. NIHRAF 302243). R.B. has no funding to declare.
Declaration of interest
G.K.-S. has received research funding from Janssen and H Lundbeck. The other authors have no other interests to declare.
Transparency declaration
A.J.C.M. affirms that the manuscript is an honest, accurate and transparent account of the study being reported, that no important aspects of the study have been omitted and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.



 Open access
Open access
eLetters
No eLetters have been published for this article.