


Introduction
Suicide is a global public health problem and causes significant economic and social costs, including distress to friends and family (Cerel et al., Reference Cerel, Maple, van de Venne, Moore, Flaherty and Brown2016; Samaritans, 2024). More than 700,000 people worldwide die by suicide annually (World Health Organization, 2021), of which three-quarters are men (World Health Organization, 2016; Office for National Statistics, 2021). In the UK specifically, over 7000 suicide deaths were registered in 2023 (Kirk-Wade, Reference Kirk-Wade2025), representing the highest suicide rate since 1999 (Office for National Statistics, 2024a), with over 76,000 hospital admissions related to self-harm in the same year (NHS England, 2024).
Intimate partner violence (IPV) is defined as any behaviour perpetrated by a current or former intimate partner that causes physical, sexual or psychological harm, including controlling behaviours (Heise and Garcia-Moreno, Reference Heise, Garcia-Moreno, Krug, Dahlberg, Mercy, Zwi Ve and Lozano2002; Council of Europe, 2014). In the year ending March 2024, the police in England and Wales recorded over 1.3 million domestic abuse-related incidents, of which 851,062 were recorded as crimes, leading to 51,183 prosecutions (Office for National Statistics, 2024b), although the actual prevalence of domestic abuse is likely much higher given that much goes unreported (Gracia, Reference Gracia2004; National Centre for Domestic Violence, 2022). Experiencing IPV is associated with suicide attempts (Seedat et al., Reference Seedat, Stein and Forde2005; Ellsberg et al., Reference Ellsberg, Jansen, Heise, Watts and Garcia-Moreno2008; Cavanaugh et al., Reference Cavanaugh, Messing, Del‐Colle, O’Sullivan and Campbell2011; Guillén et al., Reference Guillén, Panadero, Rivas and Vázquez2015; McManus et al., Reference McManus, Walby, Barbosa, Appleby, Brugha, Bebbington, Cook and Knipe2022), suicide ideation (Weaver et al., Reference Weaver, Allen, Hopper, Maglione, McLaughlin, McCullough, Jackson and Brewer2007; Ellsberg et al., Reference Ellsberg, Jansen, Heise, Watts and Garcia-Moreno2008; Yanqiu et al., Reference Yanqiu, Yan and Lin2011) and non-suicidal self-harming behaviours (Levesque et al., Reference Levesque, Lafontaine, Bureau, Cloutier and Dandurand2010; Blosnich and Bossarte, Reference Blosnich and Bossarte2012). Thus, IPV has been identified as relevant for suicide prevention in England’s National Suicide Prevention Strategy (Department of Health and Social Care, 2023).
Less attention has been paid to the relevance of IPV perpetration for suicide prevention. There is limited research on any association between perpetration of IPV and suicide in the general population. Evidence comes instead from selected populations, including people in contact with the criminal justice system, or engaged in behaviour change programmes or substance use treatment services. These studies suggest an association between perpetration of physical IPV and suicidal ideation in people using substance use treatment (Ilgen et al., Reference Ilgen, Chermack, Murray, Walton, Barry, Wojnar and Blow2009), and between dating violence perpetration and suicidal ideation in young people (Nahapetyan et al., Reference Nahapetyan, Orpinas, Song and Holland2014). Recent evidence from England suggests that men engaged in court-mandated behaviour change programmes for IPV perpetration experienced a nearly 30-fold increase in suicide rate (Conner et al., Reference Conner, Cerulli and Caine2002; Knipe et al., Reference Knipe, Vallis, Kendall, Snow, Kirkpatrick, Jarvis, Metcalfe, Eisenstadt and Bickham2024). However, these study populations are unlikely to be representative of the wider population. For example, those in contact with the criminal justice system may have poorer mental health, or have a higher suicide risk compared to those who are not (Webb et al., Reference Webb, Qin, Stevens, Mortensen, Appleby and Shaw2011; Bebbington et al., Reference Bebbington, McManus, Coid, Garside and Brugha2021), limiting the conclusions that can be drawn for population-based suicide prevention. Evidence from general population samples could be helpful in developing population-wide strategies to prevent suicide.
The association between IPV perpetration and suicidality is plausible because they may share common risk factors, for example, separate evidence links both childhood trauma to the perpetration of IPV (Li et al., Reference Li, Zhao and Yu2020) and to suicide (Zatti et al., Reference Zatti, Rosa, Barros, Valdivia, Calegaro, Freitas and Schuch2017). Suicidal behaviour and IPV perpetration may also share structural drivers, including masculine attitudes, which may involve finding violence more acceptable, and a greater reluctance to seek help when in distress (King et al., Reference King, Shields, Sojo, Daraganova, Currier, O’Neil, King and Milner2020). This association is further supported by theoretical frameworks. The interpersonal-psychological theory of suicide (Joiner, Reference Joiner2005) proposes that the concurrent presence of two interpersonal states, thwarted belongingness (i.e., feelings of loneliness or isolation) and perceived burdensomeness (i.e., feelings of liability or worthlessness), predicts suicide ideation, while suicide death also requires acquired capability (i.e., fearlessness and pain tolerance), which may develop after repeated exposure to painful events. All of these factors may be elevated in both those who experience IPV as victims and those who perpetrate IPV. For instance, in those who perpetrate IPV, thwarted belongingness may be exacerbated by negative impacts on social relationships as a result of violent behaviours and their legal consequences, which may in turn generate feelings of self-hatred. Increased suicide capability has also been linked to aggression (Smith et al., Reference Smith, Selwyn, D’Amato, Granato, Kuhlman and Mandracchia2016), which in turn is associated with IPV perpetration (Cascardi et al., Reference Cascardi, Chesin and Kammen2018).
It is suggested that co-occurring IPV perpetration/victimization (i.e., the experience of both the victimization and perpetration of IPV by the same individual), also referred to as bidirectional IPV, has distinct mechanisms and impact from IPV perpetrated without co-occurring IPV victimization (Johnson and Leone, Reference Johnson and Leone2005), although this is debated (e.g., see Walby and Towers, Reference Walby and Towers2018). Whether the relationship between IPV perpetration and suicide is influenced by the co-occurrence of IPV victimization is unknown.
There are clear gender differences across both suicidality and IPV victimization and perpetration. For example, men are up to four times more likely to die by suicide despite women being more likely to attempt suicide, in part due to differences in the lethality of methods chosen (Mergl et al., Reference Mergl, Koburger, Heinrichs, Székely, Tóth, Coyne and Hegerl2015). On the other hand, women are more likely to engage in non-suicidal self-harm (Bresin and Schoenleber, Reference Bresin and Schoenleber2015). Women are also more likely to be victims of all types of domestic abuse than men (Office for National Statistics, 2024c), while perpetrators are more likely to be male (Hester, Reference Hester2013).
We examined the association between perpetration of IPV and suicide attempt, suicidal ideation, and non-suicidal self-harm in representative general population data from England. Our objectives were to:
1. Estimate the association of lifetime IPV perpetration with past-year suicide attempt, suicidal ideation and non-suicidal self-harm in men and women.
2. Explore heterogeneity in estimates based on the presence of IPV victimization.
Methods
Data collection
The Adult Psychiatric Morbidity Survey (APMS) is a cross-sectional, probability-sample survey with the most recent available data collected in 2014. Full details of the design can be found elsewhere (McManus et al., Reference McManus, Bebbington, Jenkins, Morgan, Brown, Collinson and Brugha2020). Briefly, the survey sampled the household residential population of England aged 16 and above, using a stratified, multistage random sampling design, based on the national Small User Postcode Address File. The study sample comprised 7546 individuals, representing a response rate of 57%. Data collection was conducted primarily through computer-assisted personal interviewing in people’s homes by trained interviewers, with some items collected during a computer-assisted self-completion interview (CASI) section of the interview, in which the participant used the interviewer’s laptop.
Measurements
IPV perpetration
Lifetime IPV perpetration was indicated if any of the following four items asked in the CASI were endorsed: ‘have you ever pushed, held or pinned down or slapped a partner or ex-partner?’; ‘have you ever kicked, bit, hit with a fist or something else, or thrown something at a partner or ex-partner that hurt them?’; ‘have you ever forced a partner or ex-partner to do something sexual that they didn’t want to do?’; and ‘have you ever frightened a partner or ex-partner, by threatening to hurt them or someone close to them?’. The wording of these items was adapted from the Short Form Conflict Tactics Scale (CTS2-S), which corresponds well to the full Conflict Tactics Scale (CTS; Straus, Reference Straus1979), with good concurrent and construct validity (Straus and Douglas, Reference Straus and Douglas2004). Dichotomous (yes/no) variables were created for the lifetime experience of each type of IPV perpetration (threats, pushing, kicking and forcing your partner to do something sexual), any lifetime IPV perpetration and the number of types of IPV perpetration.
Suicide attempt, suicidal ideation and non-suicidal self-harm
Information on past-year suicide attempt was collected using the items: ‘have you ever made an attempt to take your life by taking an overdose of tablets or in some other way?’; and ‘was this in the last year?’; asked both in the face-to-face interview and the self-completion questionnaire, to give individuals more opportunities to disclose. Our variable measuring past-year suicide attempt was based on endorsement of either of these items. Lifetime suicide attempt was based on the item: ‘have you ever made an attempt to take your life by taking an overdose of tablets or in some other way?’, endorsed either face-to-face or during self-completion. Past-year suicidal ideation was measured based on the items ‘have you ever thought of taking your life, even if you would not really do it?’ and ‘was this in the past year?’, which were administered face-to-face only. Non-suicidal self-harm in the past year was measured based on the items ‘have you ever deliberately harmed yourself in any way but not with the intention of killing yourself?’ and ‘was this in the past year?’, endorsed either face-to-face or during self-completion. Dichotomous (yes/no) variables were created for past-year experience of suicide attempt, suicidal ideation and non-suicidal self-harm, and for lifetime experience of suicide attempt.
Lifetime experience of IPV
Items measuring lifetime experience of IPV were adapted from those included in the Crime Survey for England and Wales (Office for National Statistics, 2015), which is originally based on the CTS, a measure of IPV which has evidence of high reliability, with a median alpha coefficient of reliability of 0.86 across 10 studies (Straus and Mickey, Reference Straus and Mickey2012). One dichotomous (yes/no) variable was created for lifetime experience of IPV, based on endorsement of any of the following items: ‘experience of a partner preventing you from having a fair share of the household money’; ‘repeatedly belittling you to the extent that you felt worthless’; ‘pushing you, holding you, pinning you down or slapping’; ‘sending you more than one unwanted letter, email, text message or card that was either obscene or threatening and which caused you fear, alarm or distress’; or ‘kicking you, biting you, hitting you with a fist or something else, or throwing something at you that hurt you’.
Sociodemographic characteristics
Sociodemographic characteristics were self-reported by participants and included gender, age, educational attainment, marital status and ethnicity. Neighbourhood deprivation was measured according to the English Indices of Deprivation 2010 (Her Majesty’s Department of Communities and Local Government, 2011) and grouped into quintiles. Socioeconomic class was measured using the National Statistics Socio-Economic Classification (Leete and Fox, Reference Leete and Fox1977). All sociodemographic characteristics were treated as categorical variables.
Other life adversities
To assess the number of lifetime adversities experienced other than IPV, a scale was created using the List of Threatening Experiences scale (LTE; Brugha et al., Reference Brugha, Bebbington, Tennant and Hurry1985; McManus et al., Reference McManus, Walby, Barbosa, Appleby, Brugha, Bebbington, Cook and Knipe2022), described as a binary variable cut at the median (0–2 vs. 3 or more), and handled as a continuous variable for modelling. Lifetime adversities included: serious illness or injury, serious illness or injury to a close relative, serious assault of a close relative, death of an immediate family member, death of a close family friend or other relative, violence at work, homelessness, redundancy or being sacked from a job, extended work search without success, major financial crisis, something valued being lost or stolen, having trouble with the police involving court appearance and serving time in prison. While psychometric validation of this adapted version of the LTE scale is unavailable, the original version shows good concurrent validity (sensitivity of 0.89–1.0 and specificity of 0.74–0.88), and test–retest reliability in all but one item (Cohen’s kappa 0.78–1.0) (Brugha and Cragg, Reference Brugha and Cragg1990).
Hazardous alcohol use
Hazardous alcohol use was determined using the 10-item Alcohol Use Disorders Identification Test (AUDIT-10) scale (Saunders et al., Reference Saunders, Aasland, Babor, de la Fuente and Grant1993). A score of 8 or above indicated hazardous (including harmful or dependent) alcohol use. The AUDIT-10 has high diagnostic validity, with a sensitivity of 0.92 and specificity of 0.94 (Saunders et al., Reference Saunders, Aasland, Babor, de la Fuente and Grant1993), and high reliability with an average Cronbach’s α of 0.8 over 10 studies (de Meneses-gaya et al., Reference de Meneses-Gaya, Zuardi, Loureiro and Crippa2009). This outcome was treated as a dichotomous variable, with responses categorized as ‘yes’ (where an individual scored 8 or above) or ‘no’.
Drug use in the past year
Measurement of drug use in the past year was based on any use of cannabis, amphetamines, cocaine, crack, ecstasy, heroin, crystal methamphetamine, tranquilizers, amyl nitrate/poppers, anabolic steroids, glue/solvents/gas/aerosols, acid/LSD and magic mushrooms in the past year. This was treated as a dichotomous variable, with responses categorized as ‘yes’ (where responses indicated the use of any of the aforementioned drugs) or ‘no’.
Analysis
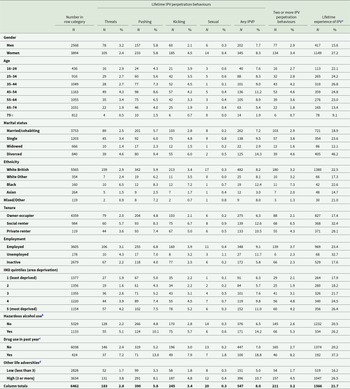
Analyses were done in Stata 17 (StataCorp, 2022) and were based on 6462 participants with complete data on the study variables. We described any IPV perpetration, two or more IPV perpetration behaviours, the four IPV perpetration behaviours separately and lifetime experience of IPV victimization (Table 1 and Figure 1), and past-year suicide attempt, lifetime suicide attempt, past-year suicidal ideation and past-year non-suicidal self-harm (Table 2) according to sociodemographic and other covariates, using counts and survey-weighted percentages. We present a complete case analysis, with respondents with complete data defined as those with observed data on all exposure, outcome and covariate variables described in Table 1. Inference assumes that data were missing completely at random, that is, that the probability of being missing for each data point is independent of both observed and unobserved data.
Diagram displaying the distribution of IPV perpetration by sociodemographic characteristics.

Characteristics of the sample reporting lifetime IPV perpetration behaviours and indicators for non-partner violence and IPV perpetration. Proportions (%) are weighted for the study design

a Experience of IPV was measured based on items for: ‘experience of a partner preventing you from having a fair share of the household money’; ‘repeatedly belittling you to the extent that you felt worthless’; ‘pushing you – holding you – pinning you down or slapping’; ‘sending you more than one unwanted letter – email – text message or card that was either obscene or threatening and which caused you fear – alarm or distress’; or ‘kicking you – biting you – hitting you with a fist or something else – or throwing something at you that hurt you’.
b Indicated by a score of 8 or above on the AUDIT-10 scale.
c Based on any use of cannabis – amphetamines – cocaine – crack – ecstasy – heroin – crystal methamphetamine – tranquilizers – amyl nitrate/poppers – anabolic steroids – glue/solvents/gas/aerosols – acid/LSD – and magic mushrooms in the past year.
d Lifetime adversities included experience of: serious illness or injury – serious illness or injury to a close relative – serious assault of a close relative – death of an immediate family member – death of a close family friend or other relative – violence at work – homelessness – redundancy or being sacked from a job – extended work search without success – major financial crisis – something valued being lost or stolen – having trouble with the police involving court appearance – and serving time in prison.
Characteristics of the sample reporting past-year and lifetime suicide attempts – past-year suicidal ideation and past-year non-suicidal self-harm

To test objective 1, we estimated survey-weighted logistic regression models including a multiplicative interaction term (IT) for gender in all models a priori, to allow gender-disaggregated estimates to be reported by applying a linear combination to estimate odds ratios (ORs) with 95% confidence intervals (95% CIs) (Howard et al., Reference Howard, Ehrlich, Gamlen and Oram2017). We selected covariates for adjustment based on the shared risk factors for IPV perpetration (Moore et al., Reference Moore, Stuart, Meehan, Rhatigan, Hellmuth and Keen2007; Foran and O’Leary, Reference Foran and O’Leary2008; Clare et al., Reference Clare, Velasquez, Mujica Martorell, Fernandez, Dinh and Montague2021; Spencer et al., Reference Spencer, Stith and Cafferky2022) and suicide (Masango et al., Reference Masango, Rataemane and Motojesi2008; DeBastiani et al., Reference DeBastiani, Norris and Kerr2019; Park et al., Reference Park, Lee, Lee, Moon, Jeon, Shim, Cho, Kim, Lee and Paik2020; Favril et al., Reference Favril, Yu, Uyar, Sharpe and Fazel2022). These were age, ethnicity, marital status, tenure, area deprivation, other life adversities, hazardous alcohol use, drug use in the past year and experience of IPV. We estimated associations between indicators of IPV perpetration, which were threats towards your partner; pushing your partner; kicking your partner; forcing your partner to do something sexual; any lifetime IPV perpetration; and the count of distinct IPV perpetration behaviours, with each outcome (past-year suicide attempt; lifetime suicide attempt; past-year suicidal ideation; and past-year self-harm). To explore the impact of covariate adjustment on associations, we report partially adjusted models including only age, ethnicity, marital status, tenure and area deprivation (model 1), adding other life adversities (model 2), further adding hazardous alcohol use and drug use in the past year (model 3) and finally including the experience of IPV in the lifetime (model 4). For any lifetime IPV perpetration only, we report IT estimates with 95% CIs, and Wald test p-values, to assess interaction by gender for past-year and lifetime suicide attempt, past-year suicidal ideation, and past-year self-harm.
To test objective 2, we estimated multiplicative ITs for the experience of IPV, presenting estimates for those with and without lifetime experience of IPV. All covariates were entered into models, and partially adjusted estimates were reported (models including only age, ethnicity, marital status, tenure and area deprivation defined as model 1, adding other life adversities to estimate model 2, further adding hazardous alcohol use and drug use in the past year to estimate model 3). For any lifetime IPV perpetration only, we reported IT estimates with 95% CIs, and Wald test p-values to assess interaction by IPV exposure for past-year and lifetime suicide attempt, past-year suicidal ideation, and past-year self-harm.
Results
Description of the study population
A total of 6462 participants provided complete data on variables included in this analysis, of whom 2568 were men, and 3894 were women. The prevalence of reporting any lifetime IPV perpetration was 7.7% in men and 8.3% in women (Table 1 and Figure 1). In terms of specific IPV perpetration behaviours, the prevalence of reporting threats was 3.2% in men and 2.4% in women. The prevalence of reporting pushing was 5.8% in both men and women. For kicking, the prevalence was 2.1% in men and 4.5% in women, and for sexual violence, the prevalence was 0.3% in men and 0.4% in women. Lifetime IPV perpetration was most commonly reported by participants aged 45–54 years (11.2%), and least commonly by those aged 75 years and older (1.9%). The prevalence of IPV perpetration was 7.2% among married/cohabiting participants, 9.5% among single participants, 2.9% among widowed participants and 14.3% among divorced participants. The prevalence of any reported lifetime IPV perpetration was 8.2% among White British participants, 8.1% among White Other participants and 8.0% among Mixed/Other participants. The proportion of Black participants reporting lifetime IPV perpetration was 12.4%, while the proportion for Asian participants was 3.0%.
The prevalence of suicide attempt in the past year was the same in men and women (0.9%), and the prevalence of lifetime suicide attempt was 5.2% in men and 7.8% in women (Table 2). Prevalence of past-year suicidal ideation in men and women was similar (4.6% men; 4.4% women). The prevalence of past-year non-suicidal self-harm was 2.2% in women and 1.2% in men. The prevalence of suicide attempts (past-year and lifetime), suicidal ideation and non-suicidal self-harm, reduced with increasing age of participants (e.g., comparing 16–24-year-olds with 75-year-olds and above: past-year suicide attempt: 3.9% vs. 0.0%; lifetime suicide attempt: 9.8% vs. 1.4%; past-year suicidal ideation: 8.3% vs. 1.5%; and past-year self-harm: 7.7% vs. 0.1%). Compared to other groups based on marital status, single participants had the highest prevalence of past-year suicide attempt (3.0%), past-year suicidal ideation (8.9%) and past-year self-harm (5.6%). The prevalence of lifetime suicide attempt was highest among divorced participants (12.7%). Black participants experienced a greater prevalence of past-year and lifetime suicide attempts (3.2% and 8.9%, respectively), past-year suicidal ideation (5.0%), and past-year self-harm (3.0%), compared to other ethnic groups.
Associations of IPV perpetration with suicide attempt, suicidal ideation and non-suicidal self-harm
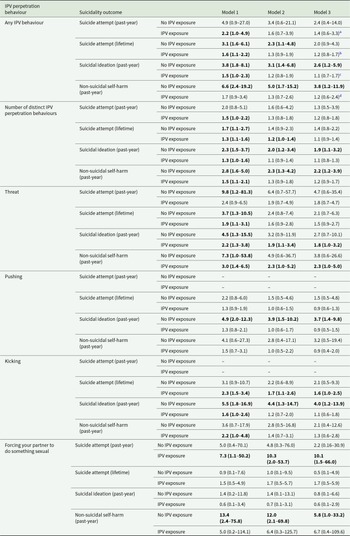
For any lifetime IPV perpetration, model 1 estimates were statistically significant for all comparisons (Table 3). After all adjustments (model 4), associations were attenuated, and the only comparison remaining statistically significant was between lifetime IPV perpetration and lifetime suicide attempt in women (OR 1.6, 95% CI 1.1–2.3).
Associations (odds ratios – ORs – with 95% CIs in parentheses) of IPV perpetration behaviours with suicide attempt – suicidality and non-suicidal self-harm in men and women. All models based on 6462 records with complete data on modelled variables

Note: Model 1: adjusted for age – ethnicity – marital status – tenure – and area deprivation. Model 2: adjusted for model 1 variables – and also for other life adversities. Model 3: adjusted for model 2 variables – and also for hazardous alcohol use – and drug use in the past year. Model 4: adjusted for model 3 variables and also for experiencing IPV in the lifetime. Bold text indicates statistical significance.
a Gender IT: 1.5 (95% CI 0.3–7.2) – p = 0.628.
b Gender IT: 1.7 (95% CI 0.9–3.4) – p = 0.118.
c Gender IT: 1.1 (95% CI 0.5–2.5) – p = 0.763.
d Gender IT: 0.8 (95% CI 0.8–2.9) – p = 0.728.
Similarly, model 1 estimates for the number of IPV perpetration behaviours were statistically significant for all comparisons and displayed attenuation on adjustment for covariates, with lifetime suicide attempt in women (OR 1.3, 1.0–1.5), and past-year suicidal ideation in women (OR 1.2, 1.2–1.5) remaining statistically significant among model 4 estimates.
For threats, estimates adjusted only for sociodemographic and socioeconomic variables (model 1) were statistically significant except for past-year suicide attempt, and lifetime suicide attempt, in men. After all adjustments (model 4), ORs remained statistically significant for past-year suicide attempt in women (OR 3.0, 1.0–8.8), lifetime suicide attempt in women (OR 2.7, 1.5–5.0), past-year suicidal ideation in women (OR 2.8, 1.5–5.3) and past-year self-harm in women (OR 2.4, 1.1–5.2).
For pushing, estimates from model 1 were statistically significant except for past-year non-suicidal self-harm in men. After all adjustments, no estimates remained statistically significant for this outcome in either men or women.
For kicking, OR estimates for model 1 were large (between 2.5 and 4.2 across variables and gender), except for past-year suicide attempt in men, where the OR was 0.9 (0.1–7.2). Other estimates were also statistically significant except for past-year non-suicidal self-harm in men. After all adjustments (model 4), estimates remained statistically significant for lifetime suicide attempt in women only (OR 1.7, 1.1–2.6).
For sexual IPV, models for suicide attempt and suicidal ideation did not produce stable estimates owing to sparse strata and are not reported. For past-year non-suicidal self-harm, the model 1 estimate for men was large in magnitude (OR 33.9, 1.2–954.5), and smaller for women (OR 5.5, 1.0–29.6). After adjustment for all covariates, these estimates were substantially attenuated and no longer statistically significant. CIs, particularly for men, were very wide (men: OR 17.8, 0.7–455.2; women: OR 4.2, 0.8–21.0), indicating strongly that these estimates should be interpreted with caution and that the role of chance cannot be ruled out.
Tests for interaction by gender in the association of any lifetime IPV perpetration with suicide attempt, suicidal ideation and non-suicidal self-harm were non-significant (past-year suicide attempt IT: 1.5 [0.3–7.2], p = 0.628; lifetime suicide attempt IT: 1.7 [0.9–3.4], p = 0.118; past-year suicidal ideation IT: 1.1 [0.5–2.5], p = 0.763; and past-year non-suicidal self-harm IT: 0.8 [0.8–2.9], p = 0.728).
On stratification by IPV victimization (Table 4), all estimates were greater in magnitude for those without IPV victimization compared to those with IPV victimization for threats, pushing and kicking, any IPV, and the number of IPV behaviours. In contrast, for sexual IPV perpetration, estimates were greater in magnitude for those with IPV victimization compared to those without IPV victimization in relation to past-year and lifetime suicide attempt, although final estimates were unstable due to small numbers with the outcome. After all adjustments, only the association of any IPV perpetration with past-year suicidal ideation in those without IPV victimization (OR 2.6, 1.2–5.9), and past-year non-suicidal self-harm in those without IPV victimization (OR 3.8, 1.2–11.9) remained statistically significant. Tests for interaction by IPV victimization in the association of any lifetime IPV perpetration with suicide attempt, suicidal ideation and non-suicidal self-harm were also non-significant (past-year suicide attempt IT: 0.6 [0.1, 4.2], p = 0.604; lifetime suicide attempt IT: 0.6 [0.3–1.4], p = 0.217; past-year suicidal ideation IT: 0.4 [0.2–1.0], p = 0.059; and past-year non-suicidal self-harm IT: 0.3 [0.1–1.2], p = 0.081).
Associations (odds ratios – ORs – with 95% CIs in parentheses) of IPV perpetration behaviours with suicide attempt (past year and lifetime) – suicidal ideation in the past year – and self-harm in the past year – stratified by IPV exposure. All models based on 6462 records with complete data on modelled variables

Note: Model 1: adjusted for gender – age – ethnicity – marital status – tenure and area deprivation. Model 2: adjusted for model 1 variables – and also for other life adversities. Model 3: adjusted for model 2 variables – and also for hazardous alcohol use – and drug use in the past year. Bold text indicates statistical significance.
a IPV exposure IT: 0.6 (95% CI 0.1–4.2) – p = 0.604.
b IPV exposure IT: 0.6 (95% CI 0.3–1.4) – p = 0.217.
c IPV exposure IT: 0.4 (95% CI 0.2–1.0) – p = 0.059.
d IPV exposure IT: 0.3 (95% CI 0.1–1.2) – p = 0.081.
Discussion
Summary of findings
Lifetime IPV perpetration, number of IPV perpetration behaviours and the separate IPV behaviour indicators were each associated with past-year and lifetime suicide attempt, past-year suicidal ideation, and past-year non-suicidal self-harm, after adjustment for sociodemographic and socioeconomic explanatory variables. Associations were evident in men and women separately, with no evidence for interaction by gender. Further adjustment for other (non-IPV-related) life adversity, hazardous alcohol use, drug use and IPV victimization substantially attenuated most associations (objective 1). Estimates for the association between IPV perpetration and suicide attempt, suicidal ideation, and non-suicidal self-harm were generally higher among participants without lifetime IPV victimization, although we did not find statistical evidence for interaction (objective 2).
Interpretation and previous findings
The association between IPV perpetration and suicidality is evident in the general population, where many will not be engaged with criminal justice or health/social care services. The association is largely accounted for by shared risk factors for both suicidality and IPV perpetration, including non-IPV life adversity, drug/alcohol misuse and IPV victimization. While we did not formally assess causality, our results are consistent with a link between psychiatric disorders and IPV perpetration (Oram et al., Reference Oram, Trevillion, Khalifeh, Feder and Howard2013; Yu et al., Reference Yu, Nevado-Holgado, Molero, D’Onofrio, Larsson, Howard and Fazel2019). Extending our previous work on IPV perpetration and mental health service use (Bhavsar et al., Reference Bhavsar, McManus, Saunders and Howard2023), these results indicate that IPV perpetration, as well as IPV victimization, may be a clinically relevant feature of mental health encounters in crisis services.
It has been proposed that ‘bi-directional’ IPV, where both partners use and experience violence within a relationship (Machado et al., Reference Machado, Sousa and Cunha2024), represents a qualitatively different phenomenon compared to unidirectional and asymmetrical situations. Our results imply that the association of IPV perpetration with suicidality is evident even among those who do not report IPV victimization (i.e., unidirectional IPV) and, indeed, may be stronger among this group. Further research should consider psychological factors that may explain greater suicidality experienced by perpetrators of IPV, some of which may contribute to stronger associations in unidirectional perpetrators of IPV compared to bi-directional perpetrators of IPV. For example, unidirectional IPV perpetrators may feel greater shame about perpetrating harm towards one’s partner, or conflict of one’s behaviour with one’s moral code, or greater rejection by others, compared to perpetrators of bi-directional IPV (although these mechanisms may also be relevant to suicidality in perpetrators of bi-directional IPV). Given that the elevated odds of suicidality were attributable to other life adversities, our results suggest that IPV perpetration may be related to the experience of multiple adversities, and that these multiple adversities may, in turn, increase suicide risk.
Few studies have explored IPV perpetration and suicidality in the general population data, particularly in high-income settings. A UK study found evidence for crude associations between perpetrating dating violence and self-harm in 16-year-old male and female participants (Herbert et al., Reference Herbert, Heron, Barter, Szilassy, Barnes, Howe, Feder and Fraser2021), consistent with but slightly smaller than our estimates. However, it focused only on birth cohort participants and did not evaluate explanatory variables. Global studies also predominantly focus on younger populations, with mixed findings regarding gender differences in the association between IPV perpetration and suicidality (Verduin et al., Reference Verduin, Engelhard, Rutayisire, Stronks and Scholte2013; Ulloa and Hammett, Reference Ulloa and Hammett2016; Stark et al., Reference Stark, Seff, Weber, Cislaghi, Meinhart, Bermudez, Atuchukwu, Onotu and Darmstadt2020).
Verduin et al. (Reference Verduin, Engelhard, Rutayisire, Stronks and Scholte2013) examined suicidal ideation in victims and perpetrators of IPV in a Rwandan general population survey, but only analysed coupled individuals and reported gender-adjusted estimates only, conflating results from men and women. They found that the OR for suicidal ideation comparing participants reporting to be both victim and perpetrator compared to others was 1.5 (0.6–3.9). No participants in this study reported themselves to be only perpetrators of IPV. A US study focusing on 18–34-year-olds only found that past-year IPV status (non-violent, perpetrator-only, victim-only, bidirectional) was associated with suicidal ideation, but not suicide attempt (Ulloa and Hammett, Reference Ulloa and Hammett2016). Bi-directional violence had the highest prevalence of suicidal ideation, while the perpetrator-only group had higher prevalences compared to the victim-only group. A Nigerian study of 13–24-year-olds (Stark et al., Reference Stark, Seff, Weber, Cislaghi, Meinhart, Bermudez, Atuchukwu, Onotu and Darmstadt2020) found that in females, and this remained statistically significant after adjusting for IPV exposure, in contrast to our findings. This may be suggestive of an influence of age on the strength of associations between IPV perpetration and suicidal ideation in women, with stronger associations in younger age groups. In men, the association was non-significant and was further attenuated after adjustment. In contrast to Stark et al. (Reference Stark, Seff, Weber, Cislaghi, Meinhart, Bermudez, Atuchukwu, Onotu and Darmstadt2020), a Ugandan study of the same age group found a significant association between IPV perpetration and suicidal ideation in males, including after adjustment for IPV exposure, but not females (Cohen et al., 2022). Again, this contrasts our findings, which suggest that after adjustment for IPV exposure, the association between suicidal ideation and lifetime IPV perpetration is non-significant for both genders, and in contrast to Stark et al. (Reference Stark, Seff, Weber, Cislaghi, Meinhart, Bermudez, Atuchukwu, Onotu and Darmstadt2020), suggests that the association is stronger in younger men, rather than younger women. Therefore, whether IPV perpetration is a stronger risk marker for suicide in women compared to men requires further investigation in age-representative samples. While we found no statistical interaction by gender of the association of IPV perpetration with suicidality, evidence strongly suggests distinct differences in IPV and suicidality between men and women, and future research should consider the possibility of gender-specific mechanisms underlying this association, in gender-disaggregated analyses.
Strengths and limitations
In contrast to previous research focusing on those in contact with criminal justice or health services or with IPV perpetrator programmes, our study presents the first examination of the association between IPV perpetration and suicidality in a recent UK general population sample, which can contribute to the development of a national picture of this association and inform population-level strategies to address both suicide (Department of Health and Social Care, 2023) and IPV perpetration (Hester et al., Reference Hester, Feder, Burrell, Gilchrist, Gadd, Kirk, Bellini, Donovan, Katz, Howard and Robinson2020). With the exception of perpetration of sexual IPV (where small numbers reporting this meant estimates were unstable), associations were successfully estimated, and we were able to explore the impact of adjustment for various risk factors, which led to the attenuation of nearly all associations. This suggests that the experience of multiple adversities, together with IPV perpetration, poses a suicide risk.
Our study has limitations. The data analysed were cross-sectional, preventing temporal and causal inference. While we included covariates based on theoretical knowledge, some relevant factors may have been omitted and/or remain unknown. IPV is a broad construct containing multiple domains of harm occurring both as temporally separate incidents and as periods of exposure to harm incurred over time (Oram et al., Reference Oram, Fisher, Minnis, Seedat, Walby, Hegarty, Rouf, Angénieux, Callard and Chandra2022). Items for IPV perpetration analysed in this paper did not measure coercive control, financial abuse, online or technology-assisted harm, the severity or frequency of harm, or patterns of escalation, which are all important aspects of IPV (Hamby, Reference Hamby2014). This limits the generalizability of our findings. Some IPV harmful behaviour not analysed in this paper may display different patterns of association with suicidality. For example, financial IPV may be more strongly related to suicide because of underlying economic food insecurity, which is in turn related to suicidality (Kaggwa et al., Reference Kaggwa, Akatussasira, Al-Mamun, Prat, Mamun, Combey and Olagunju2023). Our analyses were disaggregated by gender a priori, to allow assessment of the results for men and women separately. Nevertheless, any direct comparison of descriptive data on the prevalence of IPV perpetration and different types of harmful behaviour in men and women should be done with caution, because of the incomplete measurement of IPV perpetration in our data, and the possibility of differential misreporting. Both perpetration of IPV and suicidality are considered socially undesirable in some contexts, and may have been vulnerable to under-reporting (Freeman et al., Reference Freeman, Schumacher and Coffey2015). This could have resulted in biased estimates given any differential misclassification, for example, if those reporting IPV perpetration were less likely to disclose a suicide attempt if it had occurred. We know of no evidence on how and whether IPV perpetration influences disclosure of suicidality or vice versa. Missing data could have biased our results if the association of interest was negative or null among those with missing data, for example, on IPV perpetration and suicidality.
Implications for practice
Perpetration of IPV is an epidemiological marker of suicide risk in men and women, even in those who have not been victims of IPV. Efforts to improve clinical responses to the perpetration of IPV in people with psychiatric conditions, particularly those who have the experience of other adversities, through strengthened identification, assessment and management practices, including being aware of and sensitive to the risk of suicide, could reduce suicidality and self-harm in this population. Services encountering people who have perpetrated IPV, such as perpetrator programmes and police/probation services, could benefit from specific training in the identification and management of suicide risk in this group. Behaviour change programmes for perpetrators of IPV could be refined to place greater emphasis on suicide prevention and harm reduction, informed by our findings. Our results also highlight the need for evidence-based interventions to reduce suicidality in people perpetrating IPV who are in contact with mental health services.
Implications for research
Our results highlight the overall association of IPVP with suicidal behaviours, but assume similar associations across sociodemographic groups. Future research, for example, generating adequately powered evidence on differences in these associations based on age or ethnic group, could inform targeted prevention/intervention strategies. Future work assessing the impact of increasing severity, or frequency, of IPV perpetration on risk of suicidality could also be helpful in informing future intervention strategies. Finally, further work should also consider the relevance of suicidality to a variety of harmful behaviours perpetrated within IPV. There remains limited evidence for interventions to reduce suicidality for perpetrators of IPV, including perpetrators who are also IPV victims. A recent review of interventions for suicidality among victims of IPV found limited and mixed evidence (Jiwatram-Negrón et al., Reference Jiwatram-Negrón, Brooks, Ward and Meinhart2023), indicating the need to develop interventions to address suicidality for both victims and perpetrators of IPV. In this context, our results suggest that developing interventions for people presenting to services with both IPV perpetration and suicidality may require attention to shared risk factors, including life adversity, IPV exposure and substance misuse.
Conclusions
Perpetration of IPV is associated with suicide attempt, suicidal ideation and non-suicidal self-harm in the English household population. These associations are accounted for by life adversities, IPV victimization and substance use. Targeted identification and support for perpetrators of IPV could positively impact responses to suicidality and non-suicidal self-harm.
Availability of data and materials
Requests for access to the 2014 dataset should be made to the Data Access Request Service at NHS Digital. Code availability: Survey data collection was programmed in Blaise, a computer-assisted interviewing system and survey processing tool for the Windows operating system. The system is developed by Statistics Netherlands and has been designed for use in official statistics. It is available to National Statistical Institutes and related research institutes. Data management and analysis was conducted in Stata 17, and syntax is available from the authors on request.
Acknowledgements
The authors acknowledge the assistance of NHS Digital in making available survey data for analysis, and the authors thank the participants of the survey.
Financial support
APMS was commissioned by NHS Digital and funded by the Department for Health and Social Care (DHSC) in England. Current analyses were supported by an NIHR Advanced Fellowship awarded to Vishal Bhavsar (NIHR302243). Sophie Carlisle, Sally McManus and Siân Oram are supported by the UK Prevention Research Partnership (Violence, Health and Society; MR-V049879/1), which is funded by the British Heart Foundation, Chief Scientist Office of the Scottish Government Health and Social Care Directorates, Engineering and Physical Sciences Research Council, Economic and Social Research Council, Health and Social Care Research and Development Division (Welsh Government), Medical Research Council, National Institute for Health and Care Research, Natural Environment Research Council, Public Health Agency (Northern Ireland), The Health Foundation and the Wellcome Trust. Katherine R. K. Saunders was previously funded by the National Institute for Health and Care Research (NIHR) Policy Research Programme [grant no. PR-PRU-0916–22003] and is now funded by the Economic and Social Research Council [grant number ES/Y001044/1]. The views expressed in this article are those of the authors and not necessarily those of the UK Prevention Research Partnership or any other funder. The funders had no input in the design or the analysis.
Competing interests
The authors declare they have no conflicts of interest.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1965, as revised in 2008. Verbal consent was obtained from all survey participants, witnessed and formally recorded; details are contained in APMS documentation. Consent to participate: Consistent with standard practice on official surveys of the general population, after provision of advance written information and face-to-face explanation of survey process and data uses, verbal consent for voluntary participation was obtained on the doorstep, witnessed and formally recorded. Consent for publication: NHS Digital provided permission for data use, which allows for the publication of aggregated results. The views expressed in this publication are those of the authors and not necessarily those of the UK Prevention Research Partnership, National Institute for Health Research or the Department for Health and Social Care. The funder had no role in the study design, data collection, data analysis, data interpretation or writing of this paper. Ethical approval for APMS 2014 was obtained from the West London National Research Ethics Committee with reference number 14/LO/0411.




 Open access
Open access