


Introduction
Approximately 1.4% of children in the United States are diagnosed with congenital or acquired cardiac disease. 1 Children with cardiac disease have unique factors contributing to the risk of thromboembolism, which include a hypercoagulable state (e.g., coagulation derangements, effects of cardiopulmonary bypass, and foreign materials), endothelial injury (e.g., central vascular catheters, turbulent flow, and extracorporeal membrane oxygenation), and blood stasis (e.g., blood flow disturbances due to cardiac anatomy, ventricular dysfunction, and dilated atrium or ventricle). Reference Silvey, Nguyen and Amankwah2–Reference Kiskaddon, Do, Williams, Betensky and Goldenberg8 Previous reports suggest that 14% to 29% of paediatric patients with cardiac disease have acute thromboembolism, and 25% to 35% have at least one recurrent thromboembolism. Reference Kiskaddon, Giglia and Betensky9–Reference Ali, Goldenberg and Foreman14
Most published studies on thromboembolism in children with cardiac disease have focused on risk factors for thromboembolism or thromboprophylaxis strategies. Reference Silvey, Nguyen and Amankwah2–Reference Murphy, Benneyworth, Moser, Hege, Valentine and Mastropietro7,Reference Portman, Jacobs and Newburger15–Reference McCrindle, Michelson and Van Bergen17 In paediatric patients, the current standard of care for thromboprophylaxis and treatment includes vitamin K antagonists, unfractionated heparin, low molecular weight heparins, direct thrombin inhibitors, and the direct oral anticoagulants. Reference Portman, Jacobs and Newburger15–Reference van Ommen, Albisetti and Chan25 Despite paediatric patients with cardiac disease being at risk for thromboembolism, most children with cardiac disease are excluded from major studies or trials evaluating thromboembolism treatment and duration, as well as associated outcomes of bleeding and recurrent thromboembolism.
Given the lack of data on treatment and outcomes in this patient population, we sought to characterise antithrombotic drug regimens for thromboembolism treatment in paediatric patients with cardiac disease and identify factors associated with outcomes of bleeding and recurrent thromboembolism.
Methods
Study design and population
This is a single-centre, retrospective cohort study of patients admitted to a paediatric cardiac ICU at Johns Hopkins All Children’s Hospital (St. Petersburg, FL) between October 1, 2020, and September 30, 2024. Patients were included if they 1) had a diagnosis of congenital or acquired cardiac disease, 2) were less than 21 years of age, and 3) had a first episode (“index”) of acute symptomatic thromboembolism (venous, arterial, or intracardiac thromboembolism), confirmed by radiological imaging. Exclusion criteria included: 1) patients with an incidental finding of thromboembolism (“asymptomatic thromboembolism”), or 2) patients with a history of a prior thromboembolism (venous, arterial, or intracardiac).
Data collection
Data collected included patient demographics, patient clinical characteristics, thromboembolism characteristics, cardiac physiology (single ventricle or biventricular), antithrombotic drug regimens in the acute (<1-week post-diagnosis) and subacute (≥1 week to <3 months post-diagnosis) phases, major and clinically relevant non-major bleeding, and recurrent thromboembolism. Data were abstracted from the patient’s electronic health record and entered into electronic case report forms in a REDCap study database. This study was approved by the Johns Hopkins All Children’s Hospital institutional review board.
Outcomes
The primary study outcome was to characterise antithrombotic drug regimens among paediatric patients with CHD who developed a thromboembolism. Secondary outcomes included 1) rates of recurrent thromboembolism, or 2) rates of clinically relevant bleeding—major or clinically relevant non-major bleeding, and 3) the types of acute thromboembolism (venous, arterial, intracardiac).
Outcome definitions
Recurrent thromboembolism was defined as a thromboembolism that occurred at least 7 days after the index venous thromboembolism in a separate location from the initial event or the same location as the index venous thromboembolism, only if there was radiologic evidence of resolution before the second event. Reference Whitworth, Amankwah and Betensky26 Bleeding was classified as clinically relevant bleeding, either major or clinically relevant non-major bleeding, as defined by the International Society of Thrombosis and Haemostasis. Reference Whitworth, Amankwah and Betensky26 Immobility was defined using the Braden Q score. Reference Curley, Hasbani and Quigley27
Statistical analysis
Continuous variables for patient demographics, antithrombotic drug duration, antithrombotic time within therapeutic range, and time to recurrent thromboembolism or clinically relevant bleeding were summarised with medians and interquartile ranges, while categorical variables for thromboembolism type, antithrombotic agent types, recurrent thromboembolism, and bleeding were described using frequencies and percentages. Antithrombotic drug regimens were summarised with counts and percentages. Inter-group comparisons were performed with Mann–Whitney U tests for continuous variables and chi-square or Fisher’s exact test for categorical variables as appropriate. A multivariable Firth logistic regression model was constructed to evaluate risk factors for recurrent thromboembolism. Risk factors with significant inter-group comparisons (by recurrence/non-recurrence) were included in the final multivariable model, with the exception of held therapy, which was excluded due to power limitations. Given the small sample size of patients with index arterial thromboembolism, the model was restricted to only those with index venous thromboembolism. p-values < 0.05 were considered statistically significant. All analyses were conducted with Stata Version 17.1.
Results
Patient characteristics
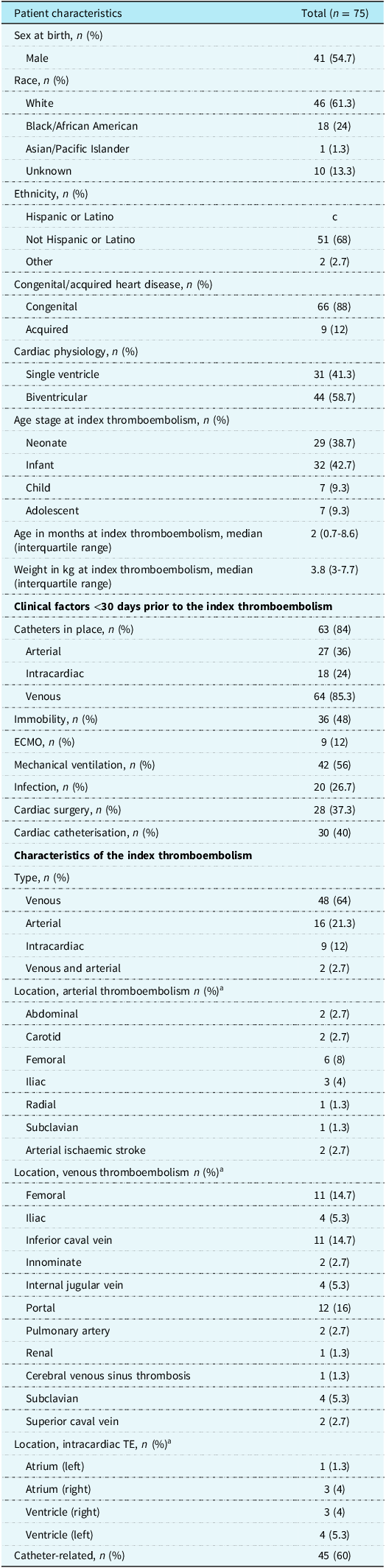
Of 865 patients admitted to the Johns Hopkins All Children’s Hospital paediatric cardiac ICU during the study phase, 75 (8.7%) developed an index acute thromboembolism. Sixty-one (81.4%) of patients who developed an index thromboembolism were <12 months of age at the time of the index event. The median (interquartile range) age and weight at the time of the index thromboembolic event were 2 (0.7–8.6) months and 3.8 (3–7.7) kg, respectively. Most patients were white (n = 46, 61.3%) or male (n = 41, 54.7%). Of the 75 patients who developed an index thromboembolism, 66 (88.0%) had CHD and 31(41.3%) had single-ventricle physiology (Table 1). In the 30 days preceding the index thromboembolism event, 63 (84.0%) patients had a central catheter (i.e., peripherally inserted central catheter, central venous catheter, central arterial catheter, right atrial catheter) placed, 36 (48.0%) were immobile, 30 (40.0%) had a cardiac catheterisation, 28 (37.3%) had cardiac surgery, and 42 (56.0%) were on mechanical ventilation (Table 1). A total of 12 (16%) patients were on an anticoagulant agent at the time of the index thromboembolism: 8/12 (66.7%) on prophylactic unfractionated heparin, 1/12 (8.3%) on prophylactic enoxaparin, and 3/12 (25%) on bivalirudin.
Demographics and clinical characteristics

Table 1. Long description
The table presents data on 75 patients who developed thromboembolism out of 865 admitted to the pediatric cardiac ICU. Key characteristics include sex at birth, race, ethnicity, congenital or acquired heart disease, cardiac physiology, age, and weight at the time of the thromboembolic event. Clinical factors within 30 days prior to the event include the presence of catheters, immobility, cardiac catheterization, cardiac surgery, mechanical ventilation, and anticoagulant use. The table details the distribution of these factors among the patients, highlighting the prevalence of central catheters, immobility, and surgical interventions. Specific anticoagulant agents used at the time of the event are also listed.
Percentages may not add to exactly 100% due to rounding.
a 9 patients had an index thromboembolism in more than 1 location; therefore, the sum of thromboembolism locations may be greater than the total number of patients.
Index thromboembolism characteristics
Of the 75 patients who developed acute thromboembolism, 48 (64.0%) had venous thromboembolism, 16 (21.3.0%) had arterial thromboembolism, 9 (12.0%) had intracardiac thrombosis, and 2 (2.7%) had both venous thromboembolism and arterial thromboembolism (Table 1). Of the 50 patients with the index event being venous thromboembolism or simultaneous venous + arterial thromboembolism, the most common locations were the portal vein (n = 12, 24.0%), inferior vena cava (n = 11, 22.0%), and femoral vein (n = 11, 22.0%). Of the 18 patients with the index event being arterial thromboembolism or simultaneous arterial+venous thromboembolism, the most common locations were the femoral artery (n = 6, 33.3%) and the iliac artery (n = 3, 16.7%). Among the 9 patients with an index thromboembolism being intracardiac, the left ventricle (n = 4, 44.4%) was the most common location (Table 1).
Treatment strategies
Of the 75 patients with index venous thromboembolism (VTE), 63 (84%) were treated with anticoagulation. Twelve patients did not receive anticoagulation, including 11 (91.2%) with portal vein thrombus, a condition without established treatment guidelines.
Of the 50 patients with either index venous thromboembolism or both venous + arterial thromboembolism, 33 (66.0%) received anticoagulation in the acute phase (<1-week post-diagnosis), and 27 (54.0%) in the subacute (≥1 week to <3 months post-diagnosis). Most patients received enoxaparin (n = 16, 32.0%) or unfractionated heparin (n = 14, 28.0%) with or without aspirin in the acute phase, and enoxaparin (n = 16, 32.0%) in the subacute phase (Figure 1). No patients received warfarin. The median (interquartile range) days of anticoagulation received for patients with venous thromboembolism were 37 (16–55) days, and the percentage time in therapeutic range was 50% (42.0–80.0%). A total of 19 (38.0%) patients with an index venous thromboembolism had held doses during the therapy course (Table 2).
Antithrombotic drug administration by index thromboembolism type and agent during the ( a ) acute and ( b ) subacute period post-diagnosis of thromboembolism.

Figure 1. Long description
The bar graph compares the number of thromboembolisms associated with different antithrombotic drugs during the acute and subacute periods post-diagnosis. The x-axis represents the number of thromboembolisms, while the y-axis lists various antithrombotic agents. The graph includes horizontal bars categorized by the type of index thromboembolism: arterial, venous, and intracardiac, represented by different colors. In the acute period, the highest number of thromboembolisms occurs with no drug administration, followed by heparin and aspirin. In the subacute period, enoxaparin shows the highest number of thromboembolisms, followed by aspirin and a combination of enoxaparin and aspirin. The color scheme differentiates between arterial (dark blue), venous (light blue), and intracardiac (gray) thromboembolisms. All values are approximated.
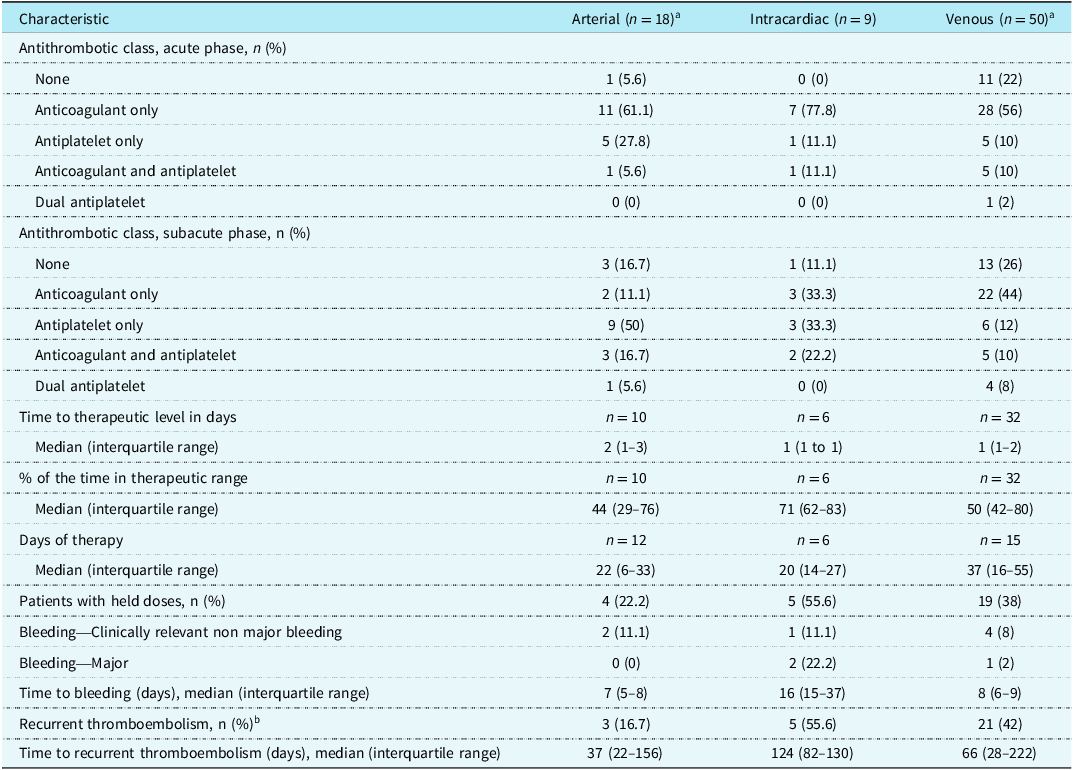
Antithrombotic treatment strategies for index thromboembolism

Table 2. Long description
The table compares antithrombotic treatment strategies for index thromboembolism across arterial, intracardiac, and venous categories. It has 20 rows and 4 columns, including headers. The columns are labeled ‘Characteristic’, ‘Arterial (n = 18)’, ‘Intracardiac (n = 9)’, and ‘Venous (n = 50)’. The table details the distribution of antithrombotic classes in both acute and subacute phases, time to therapeutic level, percentage of time in therapeutic range, days of therapy, patients with held doses, bleeding events, and recurrent thromboembolism. Notable trends include a higher percentage of patients receiving anticoagulant only in the acute phase for intracardiac (77.8 percentage) and venous (56 percentage) categories compared to arterial (61.1 percentage). The median days of therapy vary significantly, with venous patients receiving the longest median days of therapy at 37 days. The percentage of time in therapeutic range is highest for intracardiac patients at 71 percentage. Bleeding events and recurrent thromboembolism are also detailed, with intracardiac patients showing a higher percentage of major bleeding events (22.2 percentage) compared to arterial (0 percentage) and venous (2 percentage) categories.
Percentages may not add to exactly 100% due to rounding.
a 2 patients had both arterial thromboebmolsim and VTE at the index event.
b 1 patient with recurrent thromboembolism had an index thromboembolism event that was both arterial thromboembolism and VTE .
Of 18 patients with arterial thromboembolism or both arterial + venous thromboembolism, 12 (66.7%) received anticoagulation (with or without antiplatelet) in the acute phase, and 5 (27.8%) received antiplatelet monotherapy in the acute phase. The most common agents used in the acute phase were unfractionated heparin (n = 6, 33.3%) or enoxaparin (n = 6, 33.3%) with or without an antiplatelet agent (Figure 1). In the subacute phase, most patients received antiplatelet monotherapy with aspirin (n = 9, 50.0%). The median (interquartile range) days of antithrombotic (anticoagulant or antiplatelet) therapy received for patients with an index arterial thromboembolism was 22 (6–33) days. A total of 4 (22.2%) patients with an index arterial thromboembolism had held doses of antithrombotic agents during the therapy course; 1 patient had therapy held for clinically relevant non-major bleeding, and 3 patients had medication held for other reasons (Table 2).
Of the 9 patients with intracardiac thrombosis, anticoagulation with or without antiplatelet therapy was administered to 8 (88.9%) patients in the acute phase and 5 (55.6%) patients in the subacute phase. Unfractionated heparin (n = 3, 33.3%) or bivalirudin (n = 3, 33.3%) were the most common anticoagulant agents utilised in the acute phase. In the subacute phase, enoxaparin with or without aspirin (n = 3, 33.3%) was most commonly used (Figure 1). The median (interquartile range) days of therapy for patients with index intracardiac thrombus was 20 (14–27) days. A total of 5 (55.6%) patients had held doses (Table 2).
Recurrent thromboembolism
Of the 75 patients with index thromboembolism, 28 (37.3%) had ≥1 recurrent event. Twenty-one of the 28 patients (75.0%) with ≥1 recurrent thromboembolism had a venous thromboembolism as the index thromboembolic event, 5 (17.9%) had an intracardiac thrombus as the index thromboembolic event, and 3 (10.7%) had an arterial thromboembolism as the index thromboembolic event. The median (interquartile range) time to recurrent thromboembolism was 69 (22–135) days. The most common type of recurrent thromboembolism was venous (n = 19, 67.9%), and the common locations of recurrent thromboembolism included: inferior vena cava (n = 6, 21.4%) and right atrium (n = 4, 14.3%). Clinical factors present within 30 days of the recurrent thromboembolism included: immobility (n = 19, 67.9%), mechanical ventilation (n = 17, 60.7%), infection (n = 15, 53.6%), cardiac catheterisation (n = 13, 46.4%), or cardiac surgery (n = 12, 42.9%) (Supplemental Appendix, Table 1). Of note, 2 (7.1%) patients who developed recurrent thromboembolism were on unfractionated heparin at the time of the recurrent event.
Of the 21 patients with an index venous thromboembolism who developed a recurrent thromboembolism compared to the 29 who did not, single ventricle physiology [14/21 (66.7%) vs 10/29 (34.5%), p = 0.02], and younger age [1.6 mo. (0.6–3.6) vs. 2.7 mo. (0.9–18.3), p = 0.02], and have held anticoagulant doses [15/21 (71.4%) vs. 4/29 (13.8%) patients, p < 0.001] were more common (Supplemental Table 2). Three of the 11 (27.3%) patients with portal vein thrombosis who did not receive anticoagulation had a recurrent thromboembolism. In multivariable analysis, we observed that patients with single ventricle physiology at the time of index venous thromboembolism had an increased risk for recurrent thromboembolism than patients with bi-ventricle physiology [OR 3.2, 95% CI 1.1 to 9.4, p = 0.04] (Supplemental Appendix, Table 3).
Of the 3 patients with an index arterial thromboembolism who developed recurrent thromboembolism, patients with recurrent thromboembolism had more held anticoagulant doses [3/3 (100%) vs. 4/29 (13.8%) patients, p = 0.005] compared to those with index arterial thromboembolism who did not (n = 29) have recurrent thromboembolism. Compared to patients with index arterial thromboembolism who developed recurrence versus those who did not, those with recurrence were primarily treated with anticoagulant therapy in the acute phase [n = 3 (100.0%) vs. n = 8 (53.3%), p = 0.2], specifically with unfractionated heparin [n = 3 (100.0%) vs. 3 (20.0%), p = 0.02]. There were no differences in patient characteristics, other than ventricular morphology, between patients with index arterial thromboembolism who developed recurrent thromboembolism versus those without recurrence (Supplemental Appendix, Table 4).
Of the 5 patients with an index intracardiac thromboembolism who developed recurrent thromboembolism, patients with recurrent thromboembolism had more held anticoagulant doses [4/5 (80%) vs. 1/4 (25%) patients, p = 0.2] compared to those with an index cardiac thromboembolism who did not (n = 4) have recurrent thromboembolism. There were no differences observed in patient characteristics among those who developed recurrent thromboembolism versus those without recurrence (Supplemental Appendix, Table 5).
Clinically relevant bleeding
Clinically relevant bleeding (as defined by the International Society of Thrombosis and Hemostasis) occurred in 10 (13.3%) patients: 3 (30%) major bleeding and 7 (70%) clinically relevant non-major bleeding. Of those patients, concomitant anticoagulation and antiplatelet use were more common in the patients with clinically relevant bleeding compared to those who did not have clinically relevant bleeding [4 (40.0%) vs. 6 (9.2%), p = 0.02] in the subacute phase. Median (interquartile range) time to a bleeding event was 10 (7-14) days. There were no differences in clinical factors in patients with and without bleeding event(s) (Supplemental Appendix, Table 6).
Discussion
In this single-centre retrospective study, we report variation in anticoagulant treatment strategies in children with cardiac disease admitted to a cardiac ICU, a 37.3% recurrence rate, and a 13.3% clinically relevant bleeding rate. Both thromboembolism recurrence and bleeding are detrimental in children with cardiac disease, indicating an urgent need to establish evidence for thromboembolism treatment to ensure optimised outcomes for paediatric patients with cardiac disease.
Prior studies on thromboembolism treatment specifically in children with cardiac disease have included both cardiac intensive care, non-critical inpatient, and outpatient settings, and the findings reveal variation in the antithrombotic therapy use and agents employed, and the current evidence is not sufficient to establish guidance as to anticoagulant, dose intensity, duration, or use of a combination of antithrombotic agents. Reference Kiskaddon, Do and Amankwah10–Reference Kiskaddon, Stock and Betensky12,Reference Albisetti, Tartakovsky and Halton28–Reference Goldenberg, Kittelson and Abshire36 While there was no change in the anticoagulation strategy over the course of this study, we observed variation, which may be a result of clinical, patient, or provider factors.
The evidence from larger studies rarely includes children with cardiac disease. In a large clinical trial evaluating low molecular weight heparin, unfractionated heparin, and warfarin for venous thromboembolism treatment in children, fewer than 10% of patients had reported cardiac disease. Similarly, in major clinical trials establishing venous thromboembolism treatment in children, including FondaKIDS (evaluating fondaparinux) and DIVERSITY (evaluating dabigatran), less than 15% of their cohorts consisted of patients with cardiac disease. Reference Male, Lensing, Palumbo and etal20–Reference van Ommen, Albisetti and Chan25 More recently, DOACs have been studied for venous thromboembolism treatment (e.g., EINSTEIN-Jr), but unfortunately did not specify the number of patients with cardiac diseases, making it difficult to extrapolate results to this patient population. Reference Male, Lensing, Palumbo and etal20,Reference Halton, Brandão and Luciani21,Reference van Ommen, Albisetti and Chan25 Few studies report optimal treatment of arterial or venous thromboembolism, specifically in children with cardiac disease. Overall, there is variation in the types of antithrombotic agents utilised and outcomes reported. Reference Kiskaddon, Do and Amankwah10–Reference Kiskaddon, Stock and Betensky12,Reference VanderPluym, Esteso and Ankola29–Reference Goldenberg, Kittelson and Abshire36 To date, most studies specifically reporting the treatment and outcomes of arterial or venous thromboembolism report the use of enoxaparin or unfractionated heparin. More recent literature identifies the use of dabigatran, apixaban, rivaroxaban, edoxaban, or bivalirudin for the treatment of thromboembolism. However, there is variation in agent selection; most studies do not report duration of therapy or duration of follow-up, and standard definitions for bleeding or recurrent thromboembolism are not well-defined. In our study, we also report variation in antithrombotic drug regimens for both venous and arterial thromboembolism. Regarding duration of treatment for provoked venous thromboembolism, the recent KidsDOTT study reported that a treatment duration of 6 weeks compared to 12 weeks resulted in no difference in recurrent venous thromboembolism (0.65% vs. 1.40%) in selected patients. However, only 4 (1.3%) patients in the study had a cardiac disease diagnosis, which makes it challenging to draw any conclusions from the study regarding treatment duration in this population. Reference Beg, Chen, Makoni and Khan37 In our study, we identified variation in treatment agent, duration of therapy, and use of antiplatelet agents in addition to anticoagulation. The variation in the type of agent utilised is possibly reflective of the clinical course (e.g., anticipated procedures) of patients that may warrant deviation from our institutional standard practice of enoxaparin for management of a venous thromboembolism in the critical care setting. We report a median duration of 37 days for venous thromboembolism treatment; however, there is a need for evidence to support treatment duration in children with cardiac disease, given their limited patient representation in the KidsDOTT study.
Recurrent thromboembolism rates in children with cardiac disease have only been reported in a few studies, as most studies include very few patients with CHD. In a large multicentre retrospective study describing treatment strategies of venous thromboembolism in 24,879 children with cardiac disease undergoing cardiac surgery, there was a 5.9% index venous thromboembolism rate and a 25% one-year recurrence rate. Reference Kiskaddon, Do and Amankwah10 Unlike our study, which primarily reported the use of enoxaparin in the acute and subacute venous thromboembolism treatment periods, unfractionated heparin was most commonly used for venous thromboembolism treatment. In a single-centre prospective study, the presence of a central venous catheter at the time of index thromboembolism was found to be associated with subsequent recurrent thromboembolic events. Reference Kiskaddon, Giglia and Betensky9
As reflected by prior published literature, there is very limited data regarding thromboembolism treatment and bleeding rates. In a single-centre retrospective study of 81 neonatal patients (49, 60.5% of patients with CHD), 7.4% of patients who received anticoagulation for treatment of central venous catheter-associated venous thromboembolism had clinically relevant bleeding events. Reference Albisetti, Tartakovsky and Halton28 However, it is difficult to compare these results to our study, given the heterogeneity in the study populations.
Limitations of this study include a small sample size derived from a single institution, and thus, caution should be used regarding generalising the findings. Due to sample size limitations, we were unable to include patients with held doses in the multivariate model. Further, the lack of standardised care within our institution is challenging. These limitations emphasise the necessity for future larger, multi-centre studies, using standardised care protocols. Additionally, given that a diagnosis of thromboembolism in this retrospective study depended on the presence of symptoms and documentation within the electronic medical record, these findings may underestimate the true frequency of thromboembolism and its recurrence (especially regarding asymptomatic thromboembolic events). In accordance with recommendations from the American Society of Hematology Pediatric Venous Thromboembolism Guidelines, there was no surveillance ultrasound performed. Reference Monagle, Azzam and Bercovitz19 Notwithstanding these potential limitations, this study and its findings represent a crucial step in fulfilling a critical knowledge gap on thromboembolism treatments and associated outcomes of thromboembolism in children with cardiac disease.
Conclusions
Children with cardiac disease, particularly those with single ventricle physiology, admitted to a cardiac ICU, are at high risk for first episode (“index”) and recurrent thromboembolic events. Prospective multicentre studies are needed to substantiate and extend our observation that single ventricle physiology, younger age, and reduced duration of effective anticoagulation are associated with increased risk of thromboembolism recurrence among children with cardiac disease admitted to a critical care unit who develop a first venous thromboembolism.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951126113328.
Acknowledgements
None.
Financial support
None.
Competing interests
Dr Kiskaddon receives research and salary support from the American Heart Association.
Dr Neil Goldenberg receives research support and salary support from the National Institutes of Health and the National Heart, Lung, and Blood Institute for clinical and translational investigation in venous thromboembolism in patients < 21 years old. He receives or has recently received (past 12 months) consultancy fees from Anthos Therapeutics, Bayer, and the University of Colorado-affiliated Academic Research Organization CPC Clinical Research for roles in clinical trial planning or oversight committees (e.g., advisory committee, steering committee, data and safety monitoring committee) in pharmaceutical industry-sponsored paediatric multicentre clinical trials of antithrombotic agents. He also receives consultancy fees from Novartis for data and safety monitoring committee membership in multicentre clinical trials of an immunomodulatory agent. His employer, Johns Hopkins University, receives salary support on his behalf from Boehringer-Ingelheim for data coordinating centre leadership for a paediatric antithrombotic multicentre prospective observational study.
Dr Marisol Betensky receives research support and salary support from the National Institutes of Health and the National Heart, Lung, and Blood Institute for clinical and translational investigation in venous thromboembolism in patients < 21 years old.
All other authors report no COI relevant to this study.
Ethical standard
The authors assert that all procedures contributing to this work comply with the Helsinki Declaration of 1975, as revised in 2008, and have been approved by the institutional committees at Johns Hopkins Medicine.




 Open access
Open access