

Introduction
Tobacco use remains a significant global public health challenge, causing more than 8 million deaths annually, primarily due to tobacco-related noncommunicable diseases (NCDs). Low- and middle-income countries (LMICs) bear the greatest burden, accounting for over 80% of the world’s tobacco users and experiencing the highest rates of tobacco-related morbidity and mortality [1–Reference Siddiqi, Elsey and Khokhar4]. In Botswana, tobacco use is a growing concern, with the 2024 WHO STEPwise survey estimating tobacco use at 22.2% among adults aged 15–69 [5]; an increase from 17.6% in 2017 [6] and consistently disproportionately affecting men [5–Reference Keetile, Ndlovu, Setshegetso, Yaya and Serojane7].
Despite this burden, Botswana – like many LMICs – faces critical challenges in tobacco control, including sub-optimal cessation services, insufficient provider training, low public awareness, partial smoke-free protections, weak enforcement of advertising bans, and tobacco taxes below best-practice levels, highlighting major gaps across the MPOWER measures [8]-a WHO technical package that supports implementation of the Framework Convention on Tobacco Control (FCTC) [8], consisting of six evidence-based measures: Monitor tobacco use; Protect people from tobacco smoke; Offer help to quit; Warn about the dangers of tobacco; Enforce advertising bans; and Raise taxes. These gaps highlight the need for coordinated and sustainable national tobacco control strategies and infrastructure.
Globally, Tobacco Control Resource Centers (TCRCs) have been established to consolidate training, policy support, research, and community resources on tobacco control [8]. Where implemented and documented, they function as one-stop platforms to strengthen policy implementation, build provider capacity, and disseminate best practices and are commonly affiliated or based within universities [9–Reference Goel, Kar, Singh, Chaudhary, Joseph and Mehta12]. In Africa, the WHO Centre for Tobacco Control in Africa [13] (CTCA) was established in 2010 at Makerere University in Uganda, with funding from the Bill & Melinda Gates Foundation, to provide regional technical support and advance implementation of the WHO FCTC [14]. While CTCA plays a crucial role in regional coordination and capacity-building, a national TCRC can further complement its broad cross-country mandate by providing sustained, country-specific infrastructure and operational support tailored to each country’s unique epidemiological, cultural, and health system contexts. Establishing a Botswana-based TCRC within existing health, research, and academic structures may help close gaps across the MPOWER package and provide a platform for locally driven policy, programming, and capacity-building to reduce tobacco initiation and use rates in Botswana.
Community engagement is increasingly recognized as a cornerstone of translational research and public health program development, ensuring interventions are responsive, equitable, and sustainable [Reference Ohmer, Mendenhall, Mohr Carney and Adams15–Reference Joosten, Israel and Williams21]. Community Engagement Studios (CES) offer a structured approach to community and stakeholder engagement, enabling patients, policymakers, providers, and civil society to collaborate in shaping research and implementation strategies [Reference Joosten, Israel and Williams21]. While CES has been applied in translational science and research design [Reference Joosten, Israel and Head22–Reference Scheffey, Avelis, Patel, Oon, Evans and Glanz29] in high-income settings, its use in tobacco control in LMICs, including in sub-Saharan Africa (SSA), remains limited. This study describes a CES convened with a multidisciplinary panel of stakeholders in Botswana to co-design a national TCRC, exploring stakeholder acceptability, defining the scope and priority functions of the TCRC (e.g., training, direct services, public education), and identifying potential challenges and strategies.
Materials and methods
The CES was nested within a larger study, the Botswana Smoking Abstinence Reinforcement Trial (BSMART) study, which established a multi-level stakeholder group to guide its successful implementation. The BSMART study is an effectiveness-implementation hybrid type 2 stepped wedge cluster randomized trial guided by the RE-AIM framework (Reach, Effectiveness, Adoption, Implementation, Maintenance) [30] being implemented as part of Botswana’s broader efforts to integrate tobacco cessation services into HIV care, specifically evaluating the impact of integrating the Screening, Brief Intervention, and Referral to Treatment (SBIRT) model, along with pharmacological therapies, into routine HIV care [Reference Bada, Mansfield and Okui31,Reference Okui, Ikgopoleng and Mokonopi32]. The BSMART research team sought to leverage their stakeholder group to convene a CES to inform the design of a TCRC for the Botswana context, which would guide a research study design and sustainability planning while ensuring alignment with both national priorities and community needs.
This work was conducted between May and July 2025 and the process followed a seven-step framework (See Figure 1) outlined in the literature [Reference Joosten, Israel and Williams21]: (1) consultation between CES facilitator and BSMART research team, (2) identification of the community expert panel, (3) researcher coaching, (4) community expert orientation, (5) research presentation and discussion, (6) evaluation, and (7) presentation summary.
Community Engagement Studio (CES) process used to guide the design of the Botswana Tobacco Control Resource Center (TCRC).

Step 1: Consultation
As recommended [Reference Joosten, Israel and Williams21], a neutral CES facilitator not involved in the BSMART study was selected to work with the in-country BSMART research team on the CES. An initial consultation was conducted with the facilitator during which the BSMART research team shared background information on smoking in Botswana, gaps in tobacco control, the BSMART study, and the stakeholder group. The research team also described a TCRC and outlined the type of feedback they hoped to gather from the expert panel to guide its design. Following this, the BSMART research team and the CES facilitator exchanged resource materials on the CES methodology to ensure they were well informed before implementation.
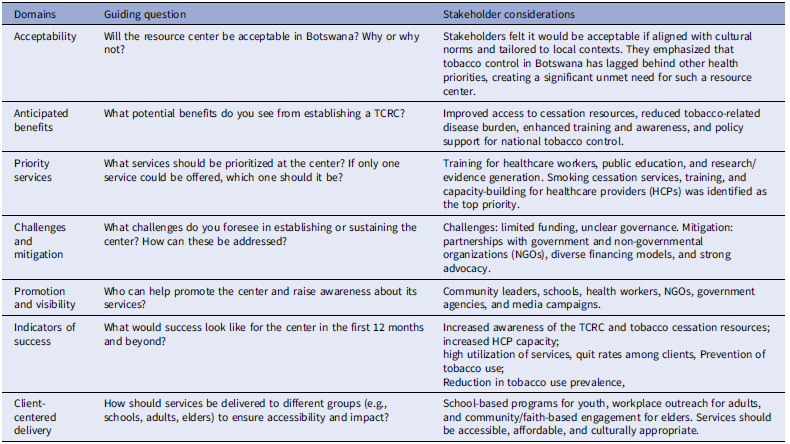
The BSMART research team sought to co-design a national TCRC with stakeholders, establishing its acceptability and gathering perspectives on its implementation in Botswana. Specifically, the research team invited stakeholders to evaluate and provide feedback on three core design elements: (a) the acceptability of a TCRC, (b) the scope and priority functions of the TCRC (e.g., training, direct services, public education), and (c) potential challenges and mitigation strategies. The research team also defined the population of interest as individuals and communities impacted by tobacco use. Table 1 outlines the questions developed to achieve the goals and objectives.
Guiding questions used in the Community Engagement Studio (CES) to inform the design of the Tobacco Control Resource Center (TCRC) in Botswana

Note: This table summarizes the thematic domains, guiding questions, and synthesized stakeholder considerations elicited during the CES conducted with multidisciplinary stakeholders. The CES was designed to inform the conceptualization and priority functions of a proposed national TCRC in Botswana. Stakeholder considerations reflect consensus themes emerging from facilitated discussion rather than verbatim quotations.
Step 2: Identify Community Expert Panel
The BSMART stakeholder group was identified as a sufficiently multidisciplinary panel of community experts capable of providing valuable insights to address the CES goals and objectives. The BSMART stakeholder group includes national-level policymakers, district and facility health managers, healthcare providers (HCPs), researchers, civil society representatives, and individuals with lived experience of tobacco use.
Step 3: Researcher Coaching
The CES facilitator and BSMART research team engaged in self-directed training on best practices for community engagement and participatory dialog. This preparation included reviewing published literature on the CES model [Reference Joosten, Israel and Williams21,Reference Joosten, Israel and Head22,Reference Stock, Ceïde, Lounsbury and Zwerling26,Reference Masel, Cavanaugh and Croisant27,Reference Scheffey, Avelis, Patel, Oon, Evans and Glanz29] and viewing recorded examples of CES sessions used to guide research and intervention design. These resources supported the team in learning how to present scientific concepts in accessible, non-technical language, foster inclusive and respectful discussion and minimize power imbalances between researchers and community participants.
Step 4: Community Expert Orientation
We conducted a single 2-hour CES session led by the CES facilitator. The session began with a brief orientation to familiarize participants with the CES model, including its purpose, format, and the value of their contributions to the research process.
Step 5: Research Presentation and Discussion
Following the orientation, the BSMART PI delivered a research presentation to provide stakeholders with background on the rationale and objectives for the proposed TCRC in Botswana. The PowerPoint presentation was reviewed in advance by the facilitator to ensure use of plain language. It included a summary of the burden of tobacco use in the country, gaps in existing tobacco control infrastructure, and the envisioned role of the TCRC in strengthening coordination, capacity-building, and access to services. To support stakeholder engagement, the PI incorporated real-world examples from tobacco control efforts in other contexts and outlined proposed components of the TCRC, such as training for frontline providers, resource dissemination platforms, and client referral pathways, closely coordinated with the Botswana Ministry of Health (MoH), district health structures, and aligned with public policy. The proposed model of the TCRC presented included its location within the University of Botswana (UB).
This presentation was followed by a discussion facilitated by the CES facilitator, using the questions outlined in Table 1, guided by the objectives listed above. The facilitator led the session with open-ended questions, providing additional prompts as needed to clarify, deepen, or expand participants’ responses and minimize power imbalances. The facilitator also monitored participation to prevent any one group from dominating. Notes were taken during the session by a designated scribe. After the session, the facilitator reiterated that participant input would inform and refine the design of the TCRC, to ensure contextual relevance and community alignment.
Step 6: Evaluation
At the end of the CES, participants verbally shared their experiences of the studio and the perceived value of the engagement in a group discussion.
Step 7: Presentation Summary
After the CES, the summary notes of participant feedback were compiled and shared with the community expert panel and research team. The research team then reviewed the summary with participants to validate that all stakeholder comments and input had been captured correctly.
Data analysis
We used a rapid thematic analysis approach to synthesize data generated during the CES. Immediately following the CES. The lead local PI and the first author independently reviewed all available data sources, which included: (a) field notes captured by the designated scribe; and (b) notes by the PI and author. Both analysts identified preliminary concepts and recurring patterns relevant to stakeholder perspectives on the design and feasibility of a TCRC in Botswana. Each analyst documented potential thematic categories that emerged. The lead author convened two meetings with the PI to refine thematic interpretations to reach consensus on major themes and to identify the most salient considerations for TCRC design under each objective.
Ethical considerations
This study was reviewed and approved by the Institutional Review Boards (IRBs) at the Botswana MoH – IRB#IORG0001746 and the University of Maryland, Baltimore, School of Medicine (IRB# IRB00000233). Consent was obtained from all participants for this engagement.
Results
Expert panel characteristics
A total of 12 stakeholders participated in the CES expert panel. The group was composed of seven men and five women. In terms of stakeholder representation, the largest proportion came from policy and practitioners (n = 5) including members of the tobacco control program at the Botswana MoH, WHO country office and National AIDS and Health Promotion Agency (NAHPA), followed by members of in country academic institutions engaged in tobacco research (n = 3), civil society organizations (CSOs) (n = 3) involved in tobacco control advocacy and activities, and community members with lived experience of smoking (n = 1).
Feedback from expert panel
Acceptability of proposed TCRC
Stakeholders unanimously endorsed the establishment of a TCRC, citing an urgent and long-standing unmet need for tobacco control infrastructure in Botswana. Participants highlighted that such a center would be acceptable to both policymakers and tobacco users, noting that this type of work is needed in Botswana. A key point of differentiation from existing rehabilitation services was that the TCRC would function not as a clinic, but as a comprehensive support hub offering cessation treatment, capacity-building, knowledge dissemination, and system strengthening. Despite overall acceptability toward TCRC, participants also expressed key considerations for optimizing the implementation and relevance of the program, including the need for transparent governance and accountability structures, integration within existing health and academic systems, culturally tailored communication strategies, and equitable access across urban and rural settings.
Anticipated benefits
Participants identified multiple anticipated benefits, with direct public health outcomes including reductions in tobacco use, nicotine dependence, and associated NCDs such as chronic obstructive pulmonary disease (COPD) and lung cancer. Stakeholders also highlighted potential indirect or longer-term societal benefits, such as improved mental health and reductions in substance use, noting the high comorbidity of tobacco and other substance use disorders with psychiatric conditions in Botswana.
Priority services for inclusion
Participants were asked to identify and prioritize potential services the TCRC could offer. Training and capacity-building for HCPs emerged as the top priority. Others included knowledge exchange through webinars, seminars, and professional networks; and the development of Information, Education, and Communication (IEC) materials tailored to Botswana’s diverse populations, establishing call centers and virtual platforms to engage tobacco users such as AI tools, and social media apps; implementing hybrid service delivery models that combine direct support with referrals; and initiating services and client engagement using tools such as SBIRT. Partnerships with organizations already offering complementary services were also encouraged to leverage synergies with existing outreach and CSO activities.
Anticipated challenges and implementation strategies
Sustainability and financing were identified as major concerns. Stakeholders proposed exploring government funding streams, including Botswana’s alcohol levy – a national tax on alcoholic beverages that funds public health initiatives. They also suggested pursuing partnerships with philanthropic organizations and leveraging university accreditation mechanisms to generate income. Accessing new or existing funding streams was identified as one of the TCRC’s key implementation strategies. Other challenges centered on potential ambiguity regarding ownership and governance, particularly in relation to the center’s proposed location at the UB. Examples from other countries where similar centers were housed within universities helped clarify possible models. Suggested implementation strategies included early involvement of the MoH to designate the center’s location at UB to create a central hub for technical assistance and coordination. Participants strongly emphasized that collaboration with the MoH and district health structures would be essential for legitimacy and long-term impact.
Promotion and advocacy opportunities
Participants identified a broad range of potential champions and promotion channels, including government bodies such as the MoH, Local Government, NAHPA, and the Parliamentary Health Committee; traditional leadership and local authorities; community structures such as CSOs, churches, and schools; stakeholders from the UB, including faculty, students, and UB radio; as well as health professionals and media outlets with national reach. Stakeholders emphasized the importance of culturally resonant, multi-platform marketing strategies, supported by credible institutions to build public trust.
Defining success
Proposed measures of success ranged from national to individual-level outcomes. At the national level, success would be reflected in the uptake of evidence-based policies, the visibility of the TCRC in planning and budgeting processes such as parliamentary discussions, and the publication of research outputs and technical briefs that inform policy and practice. At the system level, stakeholders emphasized reductions in tobacco use prevalence and service delivery gaps, alongside increased facility- and district-level capacity of providers and the integration of cessation interventions into existing services. At the organizational level, sustained service delivery beyond initial funding and clear delineation of the TCRC’s role in relation to other entities, such as rehabilitation centers, were seen as critical indicators. Finally, at the individual level, empowered clients sharing success stories in public forums and media was viewed as a tangible marker of impact.
Person-centered delivery models
Participants proposed a person-centered delivery model that is tailored to the unique needs, preferences, and context of individuals. For school-aged children and adolescents, they recommended incorporating smoking cessation into guidance curricula, health clubs, and peer-to-peer programs, while engaging with school health coordinators and parent–teacher associations (PTAs). For adults, strategies included interpersonal counseling, community-based support groups, workplace engagement, social media, and traditional forums such as kgotla meetings. For elderly populations, participants emphasized leveraging interpersonal relationships and community groups, although this group was less discussed and warrants targeted engagement in future planning. Stakeholders emphasized the importance of partnering with CSOs and existing networks to expand reach and maintain cultural relevance across Botswana’s diverse populations.
Discussion
To our knowledge, this study is among the first to document the application of the CES methodology in designing a TCRC in LMICs and SSA. While CES has been widely used in high-income countries to guide clinical trial design [Reference Quinn, Cotter, Kurin and Brown25,Reference Stock, Ceïde, Lounsbury and Zwerling26], intervention adaptation [Reference Scheffey, Avelis, Patel, Oon, Evans and Glanz29], and improve participant recruitment [Reference Jeppson, Gonzalez and Rishel Brakey28], its application to designing tobacco control centers remains limited. Our findings extend this evidence base by demonstrating that CES can be a valuable tool for shaping TCRCs in LMICs.
Overall, key partners identified that the TCRC model would be highly acceptable within the Botswana context, emphasizing the absence of a dedicated tobacco control infrastructure within the country. The rise in tobacco use between 2017 and 2024 and poor MPOWER scores [1,5,6], occurring despite the existence of a regional TCRC, may suggest that while regional support structures are valuable, they may not be sufficient substitutes for national infrastructure. The WHO-established CTCA has undoubtedly played a crucial role in strengthening policy capacity across the region [Reference Egbe, Magati, Wanyonyi, Sessou, Owusu-Dabo and Ayo-Yusuf33]; however, country-level infrastructure remains essential to addressing Botswana’s specific epidemiological patterns, service delivery gaps, and policy implementation challenges. A Botswana-based TCRC could therefore complement the CTCA by translating regional guidance into local strategies, and embedding national capacity, ensuring culturally tailored interventions, and supporting implementation of national policies and services.
The results from Botswana align with global experience showing that TCRCs typically prioritize capacity-building, technical assistance, and knowledge dissemination. Examples include TCRCs in India, Thailand, and United States of America (e.g. Maryland State) that are hubs for training, policy support, and dissemination of evidence [14–Reference Petkovic, Magwood and Lytvyn17]. Stakeholders in Botswana echoed these priorities, emphasizing training of health workers and knowledge exchange as the most critical functions of a national TCRC. A Botswana-based TCRC would be well positioned to support implementation and enforcement of MPOWER measures by strengthening provider training, generating and disseminating evidence to inform tobacco taxation and policy, increasing public awareness of health warnings and product labeling, supporting compliance with smoke-free laws, and expanding national capacity for tobacco cessation services.
Across various contexts, CES has been shown to identify implementation barriers early and generate local and context-specific implementation strategies to overcome challenges, thereby enhancing research relevance, fostering trust, and promoting the uptake of interventions [Reference Joosten, Israel and Williams21–Reference Zisman-Ilani, Buell, Mazel, Hennig and Nicholson24,Reference Stock, Ceïde, Lounsbury and Zwerling26–Reference Scheffey, Avelis, Patel, Oon, Evans and Glanz29,Reference Kas-Osoka, Israel and Ahonkhai34] In Botswana, participants emphasized financing, governance, and political buy-in as key concerns. These challenges align with findings in the TCRC literature, which highlight funding as a crucial consideration for sustainability [Reference Salloum, D’Angelo and Theis35,Reference Lapelle, Zapka and Ockene36]. Embedding CES into the design phase of Botswana’s TCRC could therefore support proactive planning for sustainability.
This CES process was unique in that no CES experts were available in-country; instead, a neutral facilitator self-trained using CES literature and online resources. Despite this, the session yielded actionable insights, consistent with evidence that CES is adaptable to diverse contexts [Reference Zisman-Ilani, Buell, Mazel, Hennig and Nicholson24]. Our CES had limitations; broader representation – including youth, smokeless tobacco users, policy makers not involved in tobacco control, and rural communities – as well as multiple iterative sessions, as seen in the literature[Reference Joosten, Israel and Williams21,Reference Joosten, Israel and Head22,Reference Scheffey, Avelis, Patel, Oon, Evans and Glanz29], would likely have strengthened it.
This CES was conducted at an early planning stage of a proposed national TCRC, allowing for timely integration of stakeholder input into the center’s co-design. Consistent with the Maintenance dimension of the RE-AIM framework [30], this work could potentially sustain and extend the impact of the BSMART study beyond the trial period. Specifically, stakeholder-informed recommendations will be used to pursue existing and new funding avenues to operationalize the TCRC as a national platform that can support long-term coordination of tobacco cessation training, service delivery, and policy-relevant knowledge translation. Recommendations may be operationalized into an implementation plan that includes governance structures, financing strategies, workforce development, and hybrid service delivery models. In doing so, the proposed TCRC would support maintaining BSMART as an evidence-based intervention and sustaining implementation gains after the trial ends.
In conclusion, our study contributes to the growing body of literature applying CES to the co-production of public health programs and research. It provides a novel proof-of-concept demonstrating that CES can be used to co-design national-level tobacco control infrastructure in LMICs. These findings offer a replicable model for other LMICs in SSA seeking to strengthen tobacco control and advance the WHO FCTC [14] through locally grounded, participatory approaches.
Acknowledgements
We would like to express our gratitude to the CES facilitator and expert panel who participated in the CES for their valuable contributions and insights.
Author contributions
Lillian Okui: Conceptualization, Methodology, Project administration, Supervision, and Writing – original draft; Marie-Claude C. Lavoie: Conceptualization, Methodology, and Writing – review and editing; Florence Bada: Writing – review and editing; Selebaleng Mokonopi: Project administration and Writing – review and editing; Kaizer Ikgopoleng: Data curation, Project administration, and Writing – review and editing; Mpho Zwinila: Project administration and Writing – review and editing; Ndwapi Ndwapi: Project administration, Supervision, and Writing – review and editing; Manhattan Charurat: Conceptualization, Funding acquisition, Supervision, and Writing – review and editing; Niharika Khanna: Conceptualization, Investigation, Supervision, and Writing – review and editing; Bontle Mbongwe: Conceptualization, Data curation, Methodology, Project administration, Supervision, and Writing – review and editing.
Funding statement
This study has been supported by funding from the National Cancer Institute at the National Institutes of Health (U01CA275048).
Competing interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.


 Open access
Open access