


Introduction
Paediatric heart disease, whether congenital or acquired, presents a significant and escalating public health challenge worldwide. Reference van der Linde, Konings and Slager1 Each year, over a million neonates are diagnosed globally with CHDs, accounting for approximately one-third of all congenital birth defects. Reference van der Linde, Konings and Slager1 The prevalence of CHDs in low- and middle-income countries, particularly in Africa, is considerably underreported due to limitations in data collection, fragile healthcare infrastructure, and inadequate specialised cardiac care, among other reasons. Reference Musa, Hjortdal and Zheleva2 This results in substantial morbidity and mortality, as nearly 90% of children with CHD in low- and middle-income countries lack access to paediatric cardiac services. Reference Vervoort, Jin and Edwin3
Beyond CHDs, acquired heart diseases such as rheumatic heart disease remain prevalent, especially in resource-limited regions. 4,Reference Manuel, Mocumbi and Zühlke5 Rheumatic heart disease continues to impose a heavy burden on low- and middle-income countries, with an estimated 55 million cases globally and approximately 300,000 deaths annually, primarily among children and young adults. 4,Reference Manuel, Mocumbi and Zühlke5
A systematic review and meta-analysis involving over 24 million live births identified CHD in 164,396 individuals, the prevalence of CHD varied across regions, with Asia reporting the highest prevalence of 9.3 per 1000 live births, followed by Europe (8.2) and the United States of America (6.9). Reference van der Linde, Konings and Slager1 Among African children, a prevalence of 5.12 and 12.63 per 1000 children from hospital and population-based studies, respectively, has been observed. Reference Danso, Appah and Akuaku6 In a report from East Africa, among over 6000 children studied, more than half (52.8 %) had paediatric heart disease, mostly CHD (80%), with ventricular septal defect and rheumatic heart disease as the most common congenital and acquired heart diseases respectively. Reference Majani, Koster and Kalezi7 Among Mozambican school children, the reported prevalence of CHD was 2.3 in 1000, with ventricular septal defect as the most prevalent abnormality. Reference Marijon, Tivane and Voicu8 In Ugandan children, a ventricular septal defect was the most common lesion identified. Reference Aliku, Beaton and Lubega9 Studies from Nigeria have reported the prevalence of CHD ranging from 14–20 per 1000 children, and ventricular septal defect as the most common lesion. Reference Ujuabi, Tabansi and Otaigbe10–Reference Sadoh, Okonkwo and Okonkwo13
Transthoracic echocardiography remains an invaluable, non-invasive imaging modality for paediatric cardiac assessment. Reference Lai, Geva and Shirali14 For children with paediatric heart disease, early diagnosis and treatment are crucial in ensuring better outcomes and improved quality of life. Reference Vervoort, Jin and Edwin3,Reference Manuel, Mocumbi and Zühlke5 The increasing availability of diagnostic facilities in various regions has a significant impact on improving the outcome of paediatric heart disease. Reference Salari, Faryadras and Shohaimi15 The establishment of a Paediatric Cardiology Unit at the Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, represents a significant milestone, providing much-needed echocardiographic evaluations for paediatric patients over the last decade.
The aim of this study was to audit echocardiography (echo) reports by reviewing the trend of echocardiography, the indications for echocardiography, and to evaluate the frequency and pattern of paediatric heart diseases diagnosed at the Paediatric Cardiology Unit, Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, over a five-year period (March 2019 – February 2024). Through this study, we seek to contribute to existing knowledge, identify trends, and highlight areas for improvement in paediatric cardiac care in low- and middle-income countries.
Methodology
This retrospective descriptive study was conducted at the paediatric cardiology unit of the Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria. Echocardiography records of paediatric patients (aged 9 hours to 18 years) over a five-year period, from March 2019 to February 2024, were analysed. The echocardiographic trends, the indications for echocardiography and the frequency and pattern of paediatric heart diseases over the five-year period were reviewed.
During this period, a total of 1179 echocardiographic studies were performed by three paediatric cardiologists in the paediatric cardiology unit; 1155 echoes were found to have complete information. All patients underwent transthoracic echocardiography using the Esaote™ MyLab30Gold® Cardiovascular ultrasound machine (Serial No: 08538), equipped with colour-coded, pulsed, and continuous wave Doppler options.
The examinations were performed using phased-array transducers with frequencies ranging from 2 to 8 MHz. Each patient underwent a 2D transthoracic echocardiography with M-mode, spectral Doppler, and colour Doppler evaluation, following which diagnostic reports were prepared and communicated to parents and referring physicians. Copies of these reports were retained within the paediatric cardiology unit.
Patients with a patent foramen ovale were excluded from the study. A structured proforma was used to extract data from each echocardiography report.
Data were analysed using IBM SPSS Statistics version 25 (IBM Corp., Armonk, NY, USA). Continuous variables were summarised as mean (standard deviation), and categorical variables were presented as frequencies and percentages. Tables and graphs were used where appropriate.
Ethical approval
Ethical approval for this study was granted by the Obafemi Awolowo University Teaching Hospitals Complex Ethics and Research Committee (International: IRB/IEC/20004553, National: NHREC/17/03/2021).
Results
Demographic characteristics
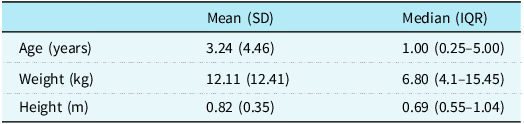
Of the 1,155 echocardiography reports analysed, 602 (52.12%) were from male patients and 553 (47.88%) from females, yielding a male-to-female ratio of 1.1:1. The participants’ ages ranged from 9 hours to 18 years, with a mean age of 3.24 ± 4.46 years and a median (IQR) of 1.00 (0.25–5.00) years.
The mean and median (IQR) weight of the participants was 12.11 ± 12.41 kg and 6.8 (4.1–15.45) kg, respectively. Similarly, the mean height was 0.82 ± 0.35 m, while the median (IQR) height was 0.69 (0.55–1.04) m (Table 1).
Anthropometric indices of subjects

Echocardiography trends over 5 years
Echocardiography trends over the 5-year period are shown in Figure 1 below. A total of 245 echocardiography studies were performed in the first year, followed by a drop in the second year to 158, which can be attributed to the COVID-19 pandemic. Subsequently, there was an increasing trend in echocardiography performed post-COVID, with the highest echocardiography performed in Year 5 (282). There was no appreciable difference in the proportion of echo-confirmed heart disease.
Echocardiography trends over 5 years.

Figure 1. Long description
The bar graph compares the number of echo studies and heart disease cases over 5 years. It features vertical bars grouped in pairs for each year, with blue representing echo studies and orange representing heart disease. The x-axis is labeled with years 1 through 5, and the y-axis ranges from 0 to 300. Year 1 shows 246 echo studies and 169 heart disease cases. Year 2 shows 158 echo studies and 119 heart disease cases. Year 3 shows 211 echo studies and 146 heart disease cases. Year 4 shows 258 echo studies and 168 heart disease cases. Year 5 shows 282 echo studies and 185 heart disease cases. The graph indicates an overall increasing trend in both echo studies and heart disease cases over the 5-year period. All values are approximated.
Indications for echocardiography
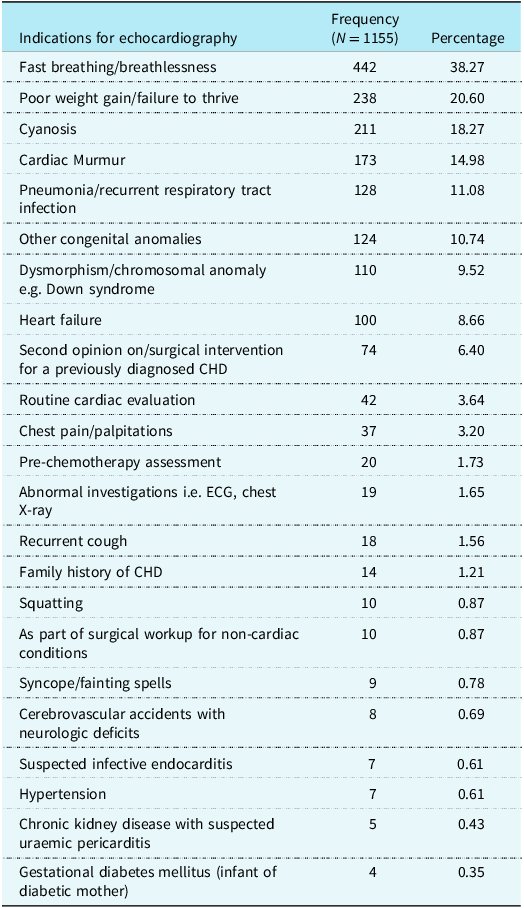
Patients presented with a variety of indications, with some cases exhibiting multiple symptoms. The most frequent indication was fast breathing 442 (38.27%), followed by poor weight gain 238 (20.60%), cyanosis 211 (18.27%), and cardiac murmurs 173 (14.98%) (Table 2). Other indications included recurrent pneumonia, the presence of congenital anomalies, and chromosomal disorders.
Indications for echocardiography

Table 2. Long description
The table presents data on various indications for echocardiography, detailing the frequency and percentage of each indication among 1155 patients. The table includes 20 rows and 3 columns, with headers for ‘Indications for echocardiography’, ‘Frequency (N = 1155)’, and ‘Percentage’. The first row shows fast breathing/breathlessness with a frequency of 442 and a percentage of 38.27%. The second row lists poor weight gain/failure to thrive with a frequency of 238 and a percentage of 20.60%. The third row indicates cyanosis with a frequency of 211 and a percentage of 18.27%. The fourth row shows cardiac murmur with a frequency of 173 and a percentage of 14.98%. Other notable indications include pneumonia/recurrent respiratory tract infection with a frequency of 128 and a percentage of 11.08%, and other congenital anomalies with a frequency of 124 and a percentage of 10.74%. The table also includes less frequent indications such as dysmorphism/chromosomal anomaly, heart failure, and second opinion on/surgical intervention for a previously diagnosed CHD.
CHD = congenital heart disease; ECG = electrocardiograph.
Echocardiographic findings
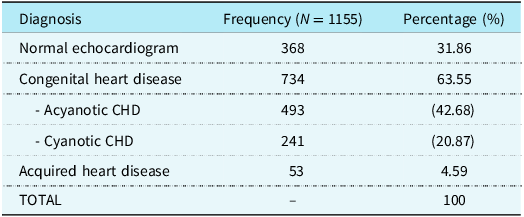
A normal echocardiogram was reported in 368 (31.86%) of the cases. CHD was diagnosed in 734 (63.55%) patients, of which 493 (67.17%) had acyanotic CHD, and 241 (32.83%) had cyanotic CHD (Table 3). Acquired heart disease was identified in 53 (4.59%) participants.
Outcome of echocardiographic studies

CHD = congenital heart disease.
Distribution of CHDs
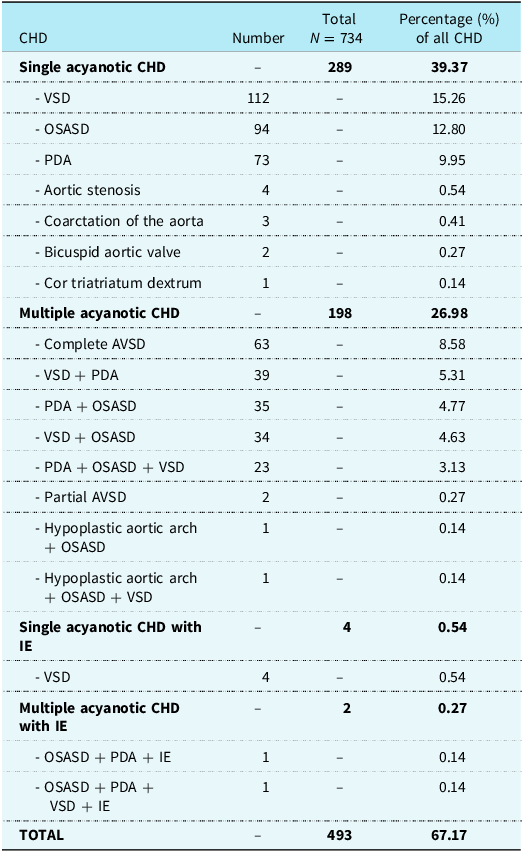
Among acyanotic CHDs, ventricular septal defect was the most common defect, occurring in 112 (15.26%) patients, followed by ostium secundum atrial septal defect (94 cases, 12.80%) and patent ductus arteriosus (73 cases, 9.95%) (Table 4).
Distribution of acyanotic CHD

Table 4. Long description
The table presents the distribution of acyanotic congenital heart defects (CHD) among 734 patients. It categorizes the defects into single acyanotic CHD, multiple acyanotic CHD, single acyanotic CHD with infective endocarditis (IE), and multiple acyanotic CHD with IE. The table includes columns for CHD type, number of cases, total cases, and percentage of all CHD. Single acyanotic CHD is the most common, with 289 cases (39.37%), followed by multiple acyanotic CHD with 198 cases (26.98%). Ventricular septal defect (VSD) is the most prevalent single acyanotic CHD, occurring in 112 patients (15.26%), followed by ostium secundum atrial septal defect (OSASD) in 94 patients (12.80%) and patent ductus arteriosus (PDA) in 73 patients (9.95%). The table also lists less common defects such as aortic stenosis, coarctation of the aorta, and bicuspid aortic valve. Multiple acyanotic CHD includes combinations like complete atrioventricular septal defect (AVSD), VSD with PDA, and PDA with OSASD. The table further categorizes cases with infective endocarditis (IE), noting their occurrence in both single and multiple acyanotic CHD. The total number of cases is 493, accounting for 67.17% of all CHD.
CHD = congenital heart disease; PDA = patent ductus arteriosus; OSASD = ostium secundum atrial septal defect; VSD = ventricular septal defect; IE = infective endocarditis; AVSD = atrioventricular septal defect.
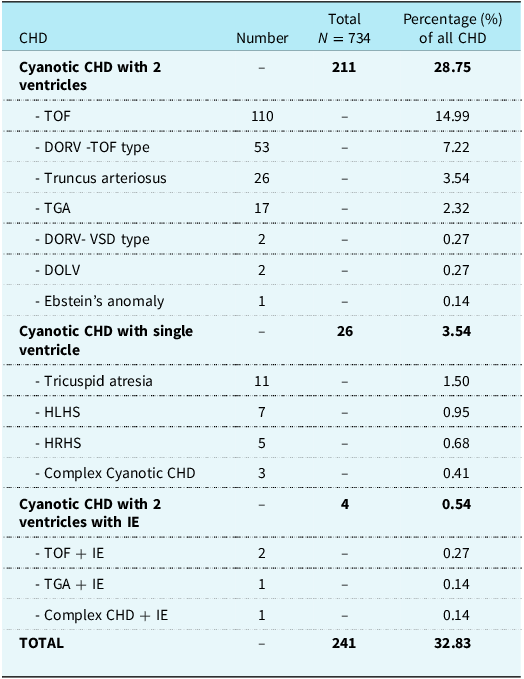
Regarding cyanotic CHDs, tetralogy of Fallot was the most prevalent, affecting 110 (14.99%) patients, followed by double outlet right ventricle — tetralogy of Fallot type (53, 7.22%), truncus arteriosus (26, 3.54%), and transposition of the great arteries (17, 2.32%) (Table 5).
Distribution of cyanotic CHD

Table 5. Long description
The table presents the distribution of cyanotic congenital heart defects (CHD) among 734 patients. It categorizes CHD into three main groups: cyanotic CHD with two ventricles, cyanotic CHD with a single ventricle, and cyanotic CHD with two ventricles and infective endocarditis. The table lists specific conditions under each category, along with the number of patients affected and the percentage of all CHD cases. For instance, tetralogy of Fallot affects 110 patients, accounting for 14.99% of all CHD cases. Other conditions include double outlet right ventricle tetralogy of Fallot type, truncus arteriosus, and transposition of the great arteries. The table also includes less common conditions like Ebstein’s anomaly and complex cyanotic CHD. The total number of patients with cyanotic CHD is 241, which constitutes 32.83% of all CHD cases.
TOF = tetralogy of Fallot; TGA = transposition of the great arteries; DORV = double outlet right ventricle; VSD = ventricular septal defect; DOLV = double outlet left ventricle; CHD = congenital heart disease; HLHS = hypoplastic left heart syndrome; HRHS = hypoplastic right heart syndrome, IE = infective endocarditis.
Distribution of acquired heart disease
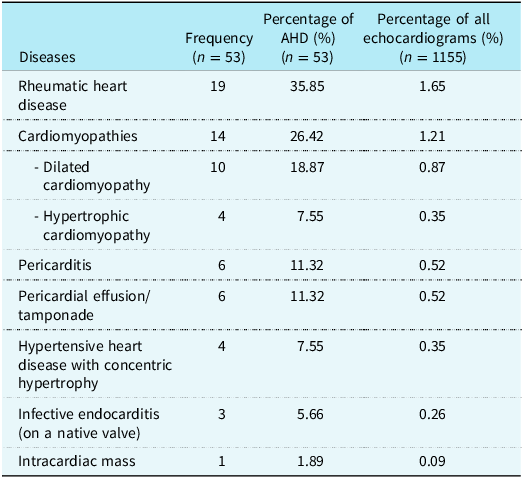
Acquired heart diseases were diagnosed in 53 (4.59%) of the participants. Rheumatic heart disease (19, 35.85 %) was the most frequently diagnosed acquired heart disease, followed by cardiomyopathies, which constituted 14 (26.42%) (dilated cardiomyopathy: (10, 18.87%) and hypertrophic cardiomyopathy: (4, 7.55%)). Other diagnoses included pericarditis, hypertensive heart disease, infective endocarditis, and intracardiac masses (Table 6).
Pattern of acquired heart disease

Table 6. Long description
The table presents data on the frequency and percentage of different acquired heart diseases diagnosed in 53 participants. It includes three columns: Diseases, Frequency, Percentage of AHD, and Percentage of all echocardiograms. The diseases listed are Rheumatic heart disease, Cardiomyopathies (including Dilated cardiomyopathy and Hypertrophic cardiomyopathy), Pericarditis, Pericardial effusion/tamponade, Hypertensive heart disease with concentric hypertrophy, Infective endocarditis, and Intracardiac mass. Rheumatic heart disease has the highest frequency at 19 cases, constituting 35.85% of AHD and 1.65% of all echocardiograms. Cardiomyopathies follow with 14 cases, making up 26.42% of AHD and 1.21% of all echocardiograms. Other notable entries include Pericarditis and Pericardial effusion/tamponade, each with 6 cases, and Infective endocarditis with 3 cases.
Discussion
This study reviewed echocardiography trends, indications for echocardiography and examined the frequency and pattern of paediatric heart diseases diagnosed by echocardiography at a tertiary facility in southwest Nigeria over a five-year period.
Trends in echocardiography
There was a sharp decline in service volume in the second year, shaped primarily by the global and local impact of the COVID-19 pandemic on non-emergency medical procedures and patient attendance. Reference Bamigboye-Taiwo, Ojo and Okeniyi16,Reference Chen, Grignani, Lim and Quek17 This disruption was followed by a sustained, increasing volume in echocardiography performed in subsequent years. The upward trend continued with the fourth year recording 258 echo studies, surpassing the initial pre-COVID-19 volume and peaking in year five, showing the growing role of echocardiography in the evaluation of PHDs. There was no significant difference in the proportion of echocardiography-confirmed diagnoses of heart disease.
Indications for echocardiography
The most common indication for echocardiography was fast breathing, accounting for well over a third of cases, followed by poor weight gain, cyanosis, and cardiac murmurs. This was like the observations of other researchers who reported fast breathing as the most common indication for echocardiography. Reference Osarenkhoe, Aiwuyo and Osaghae11,Reference Golmei, Shyamsunder, Buam, Meenakshi, Sachindeba and Mangi18,Reference Surendiran, Kulkarni and Kawade19 Fast breathing is a common symptom of CHD seen mostly in symptomatic babies and infants with heart disease. 20 Fast breathing makes the child uncomfortable, is associated with difficulty in feeding, risk of aspiration and poor weight gain. 20 Chinawa et al. noted that an isolated ventricular septal defect, followed by tetralogy of Fallot, was the most common lesion seen in children with CHD and severe respiratory distress. Reference Chinawa, Uleanya, Onukwuli, Chinawa, Obidike and Chukwu21 Other researchers have reported cardiac murmurs as the leading indication for echo. Reference Nkoke, Balti and Menanga22–Reference Animasahun and Ekhomu24 These findings highlight cardiac murmur as a frequent trigger for echocardiographic evaluation in paediatric patients. While murmurs can be innocent, they may also indicate underlying congenital or acquired cardiac abnormalities, necessitating specialist assessment. Reference Ford, Lara and Park25,Reference Huq and Rahman26 In this current study, we did not investigate the cardiac lesions associated with fast breathing or cardiac murmurs.
Several studies support the idea that non-elective echocardiograms, conducted in response to concerning symptoms, often reveal significant cardiac pathology. Reference Grech, Desira, Bailey and Mercieca27 However, nearly one-third of echocardiograms in this study yielded normal findings, mirroring trends observed in previous audits. Reference Nkoke, Balti and Menanga22,Reference Animasahun and Ekhomu24 The presence of normal studies suggests that some indications for echocardiography may not always align with the appropriate use criteria for paediatric echocardiography. Reference Grech, Desira, Bailey and Mercieca27,Reference Campbell, Douglas, Eidem, Lai, Lopez and Sachdeva28 Future research should evaluate the appropriateness of indications for echocardiography in this setting.
Prevalence and patterns of PHDs
Among patients with diagnosed heart disease, CHDs were significantly more prevalent (63.55%) than acquired heart diseases (4.59%)—a ratio of approximately 14:1. This predominance of CHDs mirrors global estimates, where CHDs constitute a major proportion of paediatric cardiac conditions. Reference Zimmerman, Smith and Sable29
In this study, within acyanotic CHDs, ventricular septal defect emerged as the most frequent lesion, followed by ostium secundum atrial septal defect and patent ductus arteriosus. The relatively higher prevalence of ventricular septal defect aligns with previous studies, which document ventricular septal defect as the most common CHD globally, accounting for nearly one-third of all CHD. Reference Ujuabi, Tabansi and Otaigbe10,Reference Otaigbe and Tabansi12,Reference Animasahun and Ekhomu24,Reference Chinawa, Eze and Obi30–Reference Doshi and Wang-Giuffre32
Among cyanotic CHDs, tetralogy of Fallot was the most prevalent lesion, followed by double outlet right ventricle - tetralogy of Fallot type, truncus arteriosus, and transposition of the great arteries. Consistent with the literature, tetralogy of Fallot remains the most frequently diagnosed cyanotic CHD worldwide, with higher prevalence reported in sub-Saharan Africa compared to industrialised nations. Reference Geleta and Mulu33,Reference Faruk, Mohammed, Anjorin, Baba and Ibrahim34
Acquired heart diseases
While acquired heart diseases were relatively infrequent in this study (4.59%), rheumatic heart disease (35.85%) accounted for the largest proportion of cases. This observation does not necessarily reflect the broader epidemiological patterns, as rheumatic heart disease remains endemic in low- and middle-income countries due to persistent gaps in healthcare access, late diagnoses, and inadequate preventive strategies. Reference Manuel, Mocumbi and Zühlke5,Reference Ekure, Amadi and Sokunbi35–Reference Morais and da Silva Ferreira37
Next to rheumatic heart disease was cardiomyopathies, with dilated cardiomyopathy (18.87%) as the leading form of cardiomyopathy. Previous researchers have also reported this and noted that dilated cardiomyopathy in children is a cause of significant morbidity and mortality (M&M) and also a common indication for cardiac transplants. Reference Animasahun, Akpoembele, Ogunkunle, Gbelee and Oke38,Reference Rath and Weintraub39 Improved paediatric cardiology services and expanded echocardiographic screening may uncover a higher burden of cardiomyopathies in future studies.
Implications for paediatric cardiac care
This study underscores the critical role of echocardiography in the early detection of heart diseases in children. Given the high proportion of CHDs, enhanced paediatric cardiology services, early referrals, and screening initiatives are essential to reduce morbidity and nortality among affected children. Additionally, there is a need for improved access to surgical interventions and long-term management for congenital and acquired heart diseases in Nigeria and similar low- and middle-income countries.
Future research should evaluate the efficacy of screening protocols, the appropriateness of indications for echocardiography, and the long-term outcomes of diagnosed CHD and acquired heart disease cases. Strengthening paediatric cardiac care in tertiary institutions would significantly impact early diagnosis and treatment, ultimately improving outcomes for affected children.
Conclusion
Transthoracic echocardiography remains indispensable in the diagnosis of PHDs, providing crucial insights into congenital and acquired cardiac conditions. The study demonstrates that fast breathing was the most frequent indication for echocardiography. CHDs were diagnosed in almost two-thirds of cases, significantly outnumbering acquired heart diseases by a ratio of nearly 14:1. Ventricular septal defect was the most identified acyanotic CHD, while tetralogy of Fallot was the predominant cyanotic CHD. The frequency of acquired heart disease in this audit was comparatively low, with rheumatic heart disease as the leading abnormality. This does not reflect the true burden of rheumatic heart disease reported in epidemiological studies. This study reinforces the critical role of paediatric echocardiography in the early detection, diagnosis, and management of heart diseases. The high prevalence of CHD signals the urgent need for enhanced cardiac care services, specialised paediatric cardiac centres, and access to corrective surgical interventions in low- and middle-income countries.
Acknowledgements
The authors wish to appreciate the kind assistance of Mrs. Nsikan Bolarinwa in the initial extraction of data.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.


 Open access
Open access