



Impact statements
In Nigeria and much of sub-Saharan Africa, young people with first-episode psychosis face a dual burden. Even when pharmacological treatment is available, the cognitive difficulties associated with psychosis, including impairments in memory, attention, planning and processing speed, are rarely addressed within public mental health services. Nigeria exemplifies this gap: fewer than 300 psychiatrists serve a population exceeding 200 million, psychiatric care remains largely medication-focused and structured cognitive rehabilitation is virtually absent from public services. These omissions are consequential because cognitive functioning strongly influences education, employment, social participation and long-term recovery during a critical developmental period.
The Cognitive Intervention for First Episode Psychosis (CognIFiEd) study addresses this gap by adapting an evidence-based cognitive skills training programme for delivery in Nigerian public hospitals through existing mental health workers rather than specialist personnel that the system cannot reliably supply. This article describes how the research team, working with young people with lived experience, caregivers, clinicians, hospital managers and policymakers, developed a Theory of Change: a structured account of how the programme is expected to work, the conditions required for implementation and where failure may occur if these conditions are absent.
The implications extend beyond Nigeria. In many low- and middle-income countries, the central challenge is not only whether effective mental health interventions exist, but whether they can be delivered in ways that are culturally appropriate, affordable, acceptable and sustainable beyond research funding. By making the implementation logic explicit and testable, this work offers an adaptable method for research teams in Africa and comparable resource-constrained settings. Importantly, involving young people with lived experience as co-producers helped ensure that the model reflects Nigerian recovery realities rather than assumptions imported uncritically from high-income settings.
Introduction
The implementation of evidence-based mental health care in low- and middle-income countries involves at least two distinct but related challenges. The first is the challenge of availability: many evidence-based interventions have never been introduced into routine public services in these settings. The second is the challenge of sustainability: interventions that are introduced into services may fail to survive the withdrawal of research scaffolding, or may underperform when the causal logic embedded in the intervention is poorly aligned with the operational realities of the health systems expected to deliver it (Fixsen et al., Reference Fixsen, Naoom, Blase, Friedman and Wallace2005; Saraceno et al., Reference Saraceno, van Ommeren, Batniji, Cohen, Gureje, Mahoney, Sridhar and Underhill2007; Theobald et al., Reference Theobald, Brandes, Gyapong, El-Saharty, Proctor, Diaz and Peters2018). In sub-Saharan Africa, where mental health resources are severely constrained, both challenges are consequential (Patel et al., Reference Patel, Saxena, Lund, Thornicroft, Baingana, Bolton, Chisholm, Collins, Cooper, Eaton, Herrman, Herzallah, Huang, Jordans, Kleinman, Medina-Mora, Morgan, Niaz, Omigbodun, Prince, Rahman, Saraceno, Sarkar, de Silva, Singh, Stein, Sunkel and UnÜtzer2018; Fadele et al., Reference Fadele, Igwe, Toluwalogo, Udokang, Ogaya and Lucero-Prisno2024). At the same time, successful programmes such as the Programme for Improving Mental Health Care (PRIME) demonstrate that theory-informed integration of mental health care into primary care is achievable in low-resource settings (Breuer et al., Reference Breuer, De Silva, Shidaye, Petersen, Nakku, Jordans, Fekadu and Lund2016; Lund et al., Reference Lund, Tomlinson and Patel2016). The central problem is therefore not simply one of implementation failure, but of how to make evidence-based interventions available, contextually deliverable and sustainable within constrained health systems.
First-episode psychosis (FEP) illustrates this challenge acutely. Affecting roughly 34 per 100,000 persons annually worldwide (Kirkbride et al., Reference Kirkbride, Hameed, Ankireddypalli, Ioannidis, Crane, Nasir and Jones2017), FEP is frequently accompanied by cognitive impairment affecting verbal memory, processing speed, working memory, attention and executive functioning (McCutcheon et al., Reference McCutcheon, Keefe and McGuire2023). These difficulties are clinically important because cognitive impairment is among the strongest predictors of long-term functional disability, including educational discontinuation, unemployment and social isolation (Green et al., Reference Green, Kern, Braff and Mintz2000). For young people, the consequences are especially significant because the onset of psychosis often coincides with life stages in which educational progression, occupational preparation and social role formation are still unfolding.
In Nigeria, the gap between need and service capacity is pronounced. Fewer than 300 psychiatrists serve a population exceeding 200 million people, and public psychiatric care remains largely pharmacological, with structured psychosocial interventions available only inconsistently (Fadele et al., Reference Fadele, Igwe, Toluwalogo, Udokang, Ogaya and Lucero-Prisno2024). Cognitive rehabilitation is therefore largely absent from routine services, despite its potential relevance to functional recovery among young people with FEP (McCutcheon et al., Reference McCutcheon, Keefe and McGuire2023; Deste et al., Reference Deste, Kokou, Barlati, Nibbio, Del Debbio, Lucchi-Piccinini and Vita2024). The problem is not that cognitive interventions have repeatedly failed in Nigerian public services; rather, they have rarely been systematically adapted, planned and embedded within the service structures that would be required for routine delivery.
Compensatory cognitive training (CCT), originally developed by Twamley and colleagues (Twamley et al., Reference Twamley, Vella, Burton, Heaton and Jeste2012), offers one feasible response to this service gap. Rather than attempting to remediate underlying neural deficits through highly specialised or computerised approaches, CCT teaches practical compensatory strategies that help individuals manage cognitive difficulties in daily life. Delivered as a manualised group intervention, it targets prospective memory, attention, verbal learning and memory, executive functioning and problem-solving, and meta-analytic evidence supports the effectiveness of compensatory approaches for cognitive impairment in psychosis (Allott et al., Reference Allott, Van-der-El, Bryce, Parrish, McGurk, Hetrick, Bowie, Kidd, Hamilton, Killackey and Velligan2020). Its relatively brief, structured, group-based format makes it potentially suitable for resource-constrained settings. Nevertheless, direct transfer of interventions developed in high-income settings into LMIC health systems risks a “voltage drop” through poor cultural fit, linguistic mismatch, stigma, workforce constraints and incompatibility with routine clinical workflows (Singla et al., Reference Singla, Kohrt, Murray, Anand, Chorpita and Patel2017; Wiltsey Stirman et al., Reference Wiltsey Stirman, Baumann and Miller2019). Adaptation of content alone is therefore insufficient; implementation pathways also require deliberate design.
Theory of Change (ToC) methodology provides a useful approach for this purpose. Unlike conventional logic models that often describe linear input–output sequences, ToC methodology makes explicit the causal assumptions, contextual contingencies, mechanisms of change and preconditions through which an intervention is expected to achieve its effects in a specific setting (Blamey and Mackenzie, Reference Blamey and Mackenzie2007; Stein and Valters, Reference Stein and Valters2012; De Silva et al., Reference De Silva, Lee and Ryan2015). In global mental health, ToC has been used to plan and evaluate mental health services in LMICs, including through the work of Breuer and colleagues, the PRIME programme, participatory service-user involvement models in Ethiopia, integrated chronic disease and depression care in Zimbabwe and peer support implementation across high-, middle- and low-income countries (Breuer et al., Reference Breuer, De Silva, Shidaye, Petersen, Nakku, Jordans, Fekadu and Lund2016; Abayneh et al., Reference Abayneh, Lempp, Alem, Kohrt, Fekadu and Hanlon2020; Kamvura et al., Reference Kamvura, Turner, Chiriseri, Dambi, Verhey and Chibanda2021; Hiltensperger et al., Reference Hiltensperger, Ryan, Adler Ben-Dor, Charles, Epple, Kalha, Korde, Kotera, Mpango, Moran, Mueller-Stierlin, Nixdorf, Ramesh, Shamba, Slade, Puschner and Nakku2024). These studies demonstrate that ToC can support participatory planning, clarify implementation assumptions and link intervention design to evaluation (De Silva et al., Reference De Silva, Lee and Ryan2015; Breuer et al., Reference Breuer, De Silva, Shidaye, Petersen, Nakku, Jordans, Fekadu and Lund2016). However, systematic participatory ToC development for cognitive rehabilitation targeting psychosis in sub-Saharan Africa has not previously been documented.
The Cognitive Intervention for First Episode Psychosis in Nigeria (CognIFiEd) study was designed to address this gap through a phased programme consistent with the updated Medical Research Council framework for complex interventions (Skivington et al., Reference Skivington, Matthews, Simpson, Craig, Baird, Blazeby, Boyd, Craig, French, McIntosh, Petticrew, Rycroft-Malone, White and Moore2021). Following formative evaluation and systematic cultural adaptation through participatory expert panels and a trained Youth Research Team (YRT), the present phase undertook explicit ToC co-production before pilot trial initiation. The study is conducted across three tertiary public psychiatric hospitals in South-West Nigeria. This article describes the ToC development process and its outputs. Specifically, it documents a transparent and replicable methodology for participatory ToC development in an LMIC mental health context; presents the resulting ToC map, including implementation pathways, assumptions, contextual factors, accountability boundaries and mitigation strategies; describes stakeholder engagement processes and their contribution to ToC content and validation and discusses implications for the sustainability and scale-up of cognitive interventions in LMIC mental health systems.
Methods
Study design and positioning within the CognIFiEd programme
ToC development constituted Work Package 4 of the CognIFiEd programme, a multiphase implementation research initiative to culturally adapt, pilot test and evaluate a task-shifted CCT intervention for young adults with FEP in Nigerian public mental health services. Work Packages 2 and 3 addressed formative evaluation and systematic cultural adaptation, respectively, whereas Work Package 4 focused on articulating the causal pathways through which the adapted intervention might be implemented, sustained and scaled within routine care before initiation of the pilot randomised controlled trial. This sequencing reflects the view that explicit implementation theory should be treated as pre-trial infrastructure rather than post hoc rationalisation (De Silva et al., Reference De Silva, Lee and Ryan2015; Skivington et al., Reference Skivington, Matthews, Simpson, Craig, Baird, Blazeby, Boyd, Craig, French, McIntosh, Petticrew, Rycroft-Malone, White and Moore2021). The methodological orientation combined participatory co-production with implementation science frameworks, aiming to generate a theoretically grounded, context-sensitive and empirically testable account of how change might reasonably be expected to occur within the constraints of Nigerian public psychiatric hospitals (Breuer et al., Reference Breuer, De Silva, Shidaye, Petersen, Nakku, Jordans, Fekadu and Lund2016; Theobald et al., Reference Theobald, Brandes, Gyapong, El-Saharty, Proctor, Diaz and Peters2018).
Setting
ToC development took place in three tertiary public psychiatric hospitals in South-West Nigeria that also serve as trial sites for the CognIFiEd pilot randomised controlled trial: Lagos State University Teaching Hospital (LASUTH), Ikeja, Lagos; Federal Neuropsychiatric Hospital Yaba (FNPHY), Lagos and Neuropsychiatric Hospital Aro (NPHA), Abeokuta, Ogun State. These settings are characterised by high patient volumes, specialist concentration at the tertiary level, limited structured psychosocial programming and predominant reliance on psychiatric social workers and nurses for non-pharmacological care (Fadele et al., Reference Fadele, Igwe, Toluwalogo, Udokang, Ogaya and Lucero-Prisno2024). Because the CCT intervention is designed for delivery through a task-shifted model embedded within routine outpatient services, ToC development deliberately engaged with these real-world service environments (Singla et al., Reference Singla, Kohrt, Murray, Anand, Chorpita and Patel2017).
Theoretical frameworks guiding ToC development
The ToC process was guided by three complementary implementation frameworks. The World Health Organisation (WHO) ExpandNet model provided a systems-level lens for scalability and health system integration, highlighting the attributes of the innovation, the capacities of the resource team, the characteristics of user organisations and the wider environmental conditions influencing scale-up (World Health Organization, 2010). The RE-AIM framework, organised around Reach, Effectiveness, Adoption, Implementation and Maintenance, provided an outcome-level scaffold for mapping implementation pathways and identifying monitoring indicators at individual, service and system levels (Glasgow et al., Reference Glasgow, Harden, Gaglio, Rabin, Smith, Porter and Estabrooks2019). The Consolidated Framework for Implementation Research (CFIR) contributed a contextual mapping structure, focusing attention on inner setting characteristics such as structural capacity, organisational culture, leadership and workflow, outer setting influences such as policy environment and community context and individual determinants of adoption (Damschroder et al., Reference Damschroder, Aron, Keith, Kirsh, Alexander and Lowery2009).
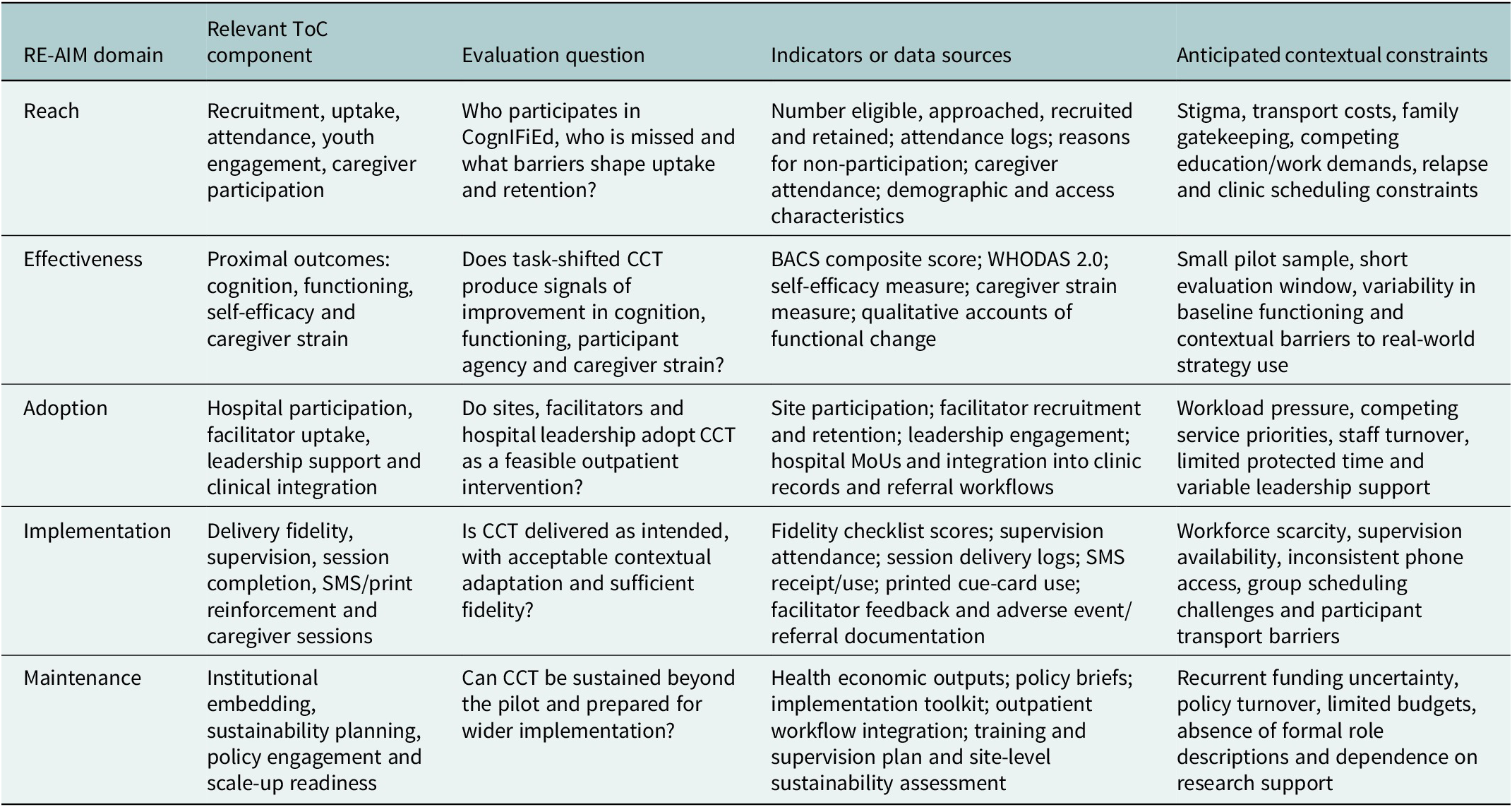
The integration of these frameworks was deliberate, with each performing a distinct analytical function. WHO ExpandNet shaped the backward-mapping exercise by prompting early deliberation on organisational readiness, user-system capacity and environmental conditions rather than treating scale-up as a post-trial concern (World Health Organization, 2010). RE-AIM served as the primary scaffold for defining implementation and outcome indicators, linking ToC domains to later evaluation of reach, effectiveness, adoption, implementation fidelity and maintenance (Glasgow et al., Reference Glasgow, Harden, Gaglio, Rabin, Smith, Porter and Estabrooks2019). The operational alignment between ToC domains and RE-AIM evaluation constructs is summarised in Table 3. CFIR provided structured prompts for eliciting contextual determinants, especially those relating to workforce scarcity, leadership support, stigma, technology access and service workflow (Damschroder et al., Reference Damschroder, Aron, Keith, Kirsh, Alexander and Lowery2009). The process was additionally informed by De Silva and colleagues’ practical guidance on ToC development for complex health interventions, particularly the expectation that causal pathways, assumptions and preconditions should be made explicit rather than implied (De Silva et al., Reference De Silva, Lee and Ryan2015). Consistent with Breuer and colleagues’ reporting guidance for ToC in public health interventions, the final map includes directional causal arrows, assumptions, contextual conditions, mitigation strategies and an accountability boundary separating outcomes under direct programme monitoring from broader system-level impacts (Breuer et al., Reference Breuer, De Silva, Shidaye, Petersen, Nakku, Jordans, Fekadu and Lund2016).
Consistent with contemporary adaptation science, fidelity during ToC development was understood as preservation of core therapeutic mechanisms rather than strict adherence to the original intervention format (Wiltsey Stirman et al., Reference Wiltsey Stirman, Baumann and Miller2019). This distinction informed deliberations on modifications to session structure, facilitator roles, caregiver involvement, digital reinforcement and alignment with outpatient workflows.
Stakeholder identification and composition
Stakeholder selection used purposive maximum variation sampling to ensure representation across clinical, experiential, managerial, community and policy perspectives relevant to CCT implementation in Nigerian public psychiatric settings. This design choice reflected a deliberate methodological decision: maximum variation was used to ensure that the ToC captured the full ecology of implementation, from policy-level sustainability and hospital governance to facilitator workload, family involvement and young people’s lived experience of recovery (Breuer et al., Reference Breuer, De Silva, Shidaye, Petersen, Nakku, Jordans, Fekadu and Lund2016; Abayneh et al., Reference Abayneh, Lempp, Alem, Kohrt, Fekadu and Hanlon2020).
The authors recognise the tension between this approach and the risk that power differentials may suppress contributions from less powerful participants, particularly young people with lived experience and frontline social workers in the presence of clinicians, administrators and policymakers. This concern informed the power-mitigation procedures described below, including small-group work, anonymous voting, structured turn-taking and explicit solicitation of minority perspectives. Eligibility criteria included current involvement with youth mental health services in Lagos or Ogun States, experiential or organisational knowledge relevant to cognitive intervention delivery and willingness to participate in multiple workshops over a six-week period.
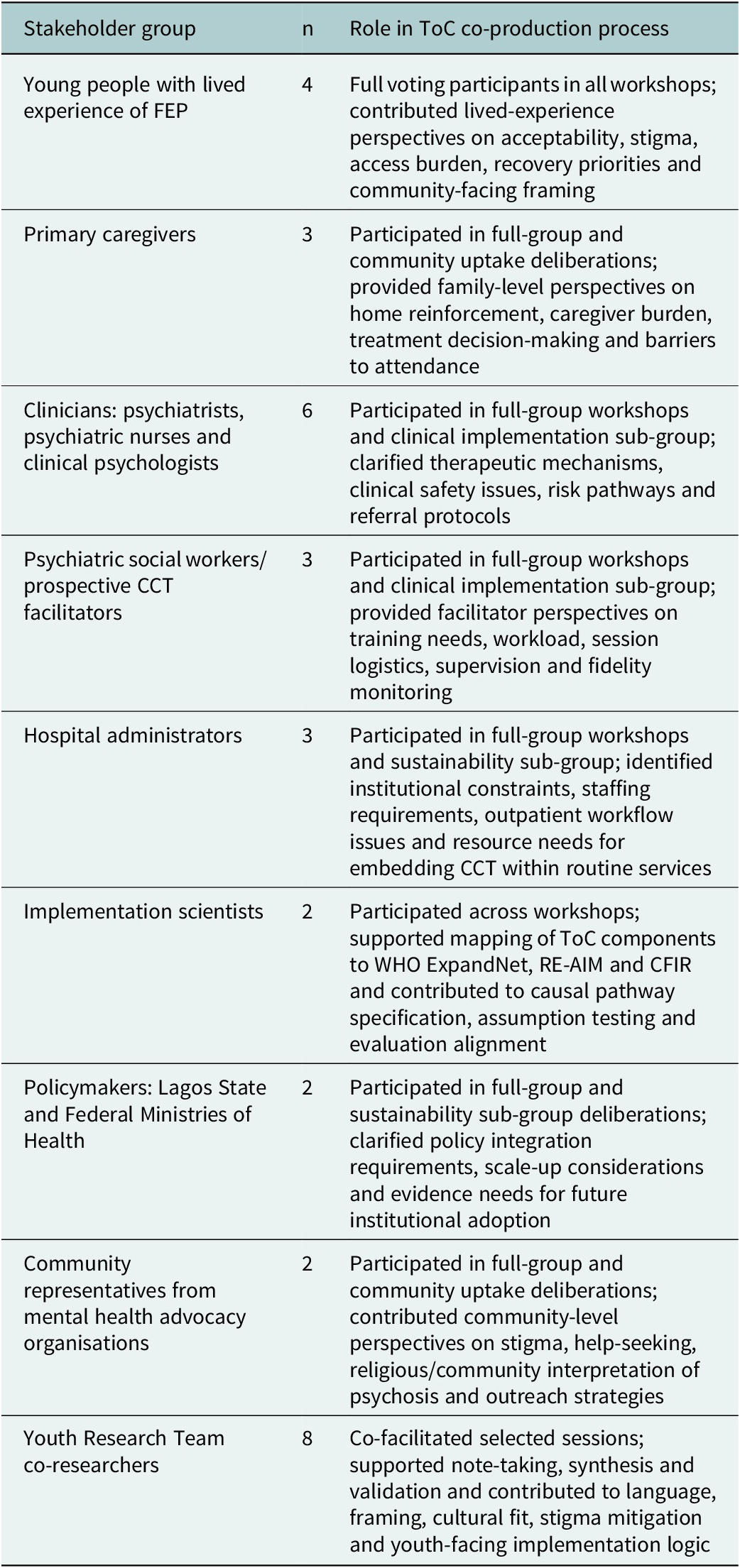
Twenty-five stakeholders were recruited across eight categories: young people with lived experience of FEP (n = 4, ages 22–28, all involved in earlier study phases); primary caregivers (n = 3); clinicians, including psychiatrists, psychiatric nurses and clinical psychologists (n = 6); psychiatric social workers identified as prospective CCT facilitators (n = 3); hospital administrators (n = 3); implementation scientists (n = 2); policymakers from Lagos State and Federal Ministries of Health (n = 2) and community representatives from mental health advocacy organisations (n = 2).
The YRT, comprising eight young people with lived experience of psychosis trained as co-researchers across the CognIFiEd programme, served as workshop co-facilitators and contributed to planning, facilitation, note-taking, synthesis and validation. Their contributions were weighted equally to those of other stakeholders in consensus procedures, and they received remuneration as research staff. Three thematic sub-groups were convened from the wider stakeholder pool: a clinical implementation sub-group (n = 8; clinicians, facilitators, hospital managers), a community uptake sub-group (n = 7; caregivers, YRT members and a community health worker) and a sustainability sub-group (n = 6; policymakers, administrators and two senior researchers). The composition of stakeholders, their institutional affiliations and their roles within full-group and thematic sub-group deliberations are summarised in Table 1.
Stakeholder composition and roles in CognIFiEd ToC co-production

Table 1. Long description
The table consists of three columns: Stakeholder group, n, and Role in T o C co-production process.
* Young people with lived experience of F E P: n equals 4. Full voting participants who contributed perspectives on acceptability, stigma, access, and recovery priorities.
* Primary caregivers: n equals 3. Provided family-level perspectives on home reinforcement, caregiver burden, and barriers to attendance.
* Clinicians (psychiatrists, nurses, psychologists): n equals 6. Clarified therapeutic mechanisms, clinical safety, and referral protocols.
* Psychiatric social workers or prospective C C T facilitators: n equals 3. Provided perspectives on training needs, workload, and fidelity monitoring.
* Hospital administrators: n equals 3. Identified institutional constraints, staffing, and resource needs for embedding C C T.
* Implementation scientists: n equals 2. Mapped T o C components to W H O ExpandNet, R E - A I M, and C F I R frameworks.
* Policymakers (Lagos State and Federal Ministries of Health): n equals 2. Clarified policy integration and scale-up considerations.
* Community representatives from mental health advocacy organisations: n equals 2. Contributed perspectives on stigma, help-seeking, and outreach.
* Youth Research Team co-researchers: n equals 8. Co-facilitated sessions and contributed to cultural fit and stigma mitigation.
Notes define C C T as Compensatory Cognitive Training, C F I R as Consolidated Framework for Implementation Research, F E P as first-episode psychosis, R E - A I M as Reach, Effectiveness, Adoption, Implementation and Maintenance, and T o C as Theory of Change.
Notes: CCT = Compensatory Cognitive Training; CFIR = Consolidated Framework for Implementation Research; FEP = first-episode psychosis; RE-AIM = Reach, Effectiveness, Adoption, Implementation and Maintenance; ToC = Theory of Change; YRT = Youth Research Team. The Youth Research Team comprised young people with lived experience of psychosis trained as co-researchers across the wider CognIFiEd programme. Their contributions were weighted equally to those of other stakeholders in consensus procedures. Policymaker representation was limited to two individuals, which is acknowledged as a limitation.
ToC co-production process
ToC development proceeded through a structured, iterative sequence between March and April 2025. Before convening workshops, the research team synthesised formative evaluation findings from Work Package 2, cultural adaptation outputs from Work Package 3 and implementation constructs embedded in the trial protocol. This preparatory synthesis generated provisional domain scaffolding to guide facilitation without predetermining causal conclusions (De Silva et al., Reference De Silva, Lee and Ryan2015; Breuer et al., Reference Breuer, De Silva, Shidaye, Petersen, Nakku, Jordans, Fekadu and Lund2016).
Five sequential workshops then followed. Workshop 1 oriented stakeholders to ToC concepts, CCT components and the three guiding implementation frameworks and used group exercises to surface priorities, uncertainties and anticipated implementation tensions. Workshop 2 used small-group backward mapping, starting from desired long-term impact and reasoning backward to identify preconditions, inputs, activities and outputs along the implementation pathway. Workshop 3 refined these components and extended the analysis to proximal and longer-term outcomes. Workshop 4 focused on eliciting critical assumptions and mapping contextual factors, with prompts designed to surface beliefs that might otherwise be treated as self-evident rather than testable propositions. Workshop 5 addressed barrier mitigation pathways, monitoring framework design, accountability boundaries and integration of the visual ToC map, culminating in consensus validation of the complete map.
Between workshops, the facilitation team produced structured summaries documenting causal claims, assumptions, contested areas, minority views and emerging themes for subsequent deliberation. A structured summary of the full co-production protocol, including workshop sequencing, consensus thresholds and documentation procedures, is available in Supplementary File S1.
Decision-making and consensus procedures
Decision-making used a structured consensus procedure with modified Delphi features. For each proposed ToC component, a five-stage process was used: small-group proposal generation; plenary discussion with structured turn-taking; anonymous voting on inclusion using a five-point scale (1 = strongly disagree to 5 = strongly agree); application of a prospectively defined 80% agreement threshold, based on the proportion of participants scoring the item 4 or 5 and iterative revision for components scoring 60–79%, followed by second-round voting. Components falling below 60% agreement were to be excluded or substantially reformulated.
All 25 stakeholders participated in voting rounds on equal terms, including YRT members, whose contributions were weighted identically to those of clinicians, administrators and policymakers. Two rounds of voting were conducted. Forty-seven of 51 proposed components reached consensus in the first round; the remaining four underwent structured deliberation and second-round voting, after which all reached consensus without exclusion. To minimise power differentials, facilitators used anonymous digital voting, small-group breakouts before plenary discussion, structured turn-taking and explicit solicitation of dissenting or minority perspectives.
This procedure met the core criteria for a modified Delphi approach in the sense that it incorporated iterative rounds, anonymous scoring, predefined consensus thresholds and structured revision. However, it departed from classical Delphi methodology because consensus development occurred within face-to-face co-production workshops rather than through sequential questionnaire rounds conducted remotely. The procedure is therefore described here as a structured consensus process with modified Delphi features.
Data collection and synthesis
Multiple data streams informed ToC development: audio recordings and facilitator field notes from all workshops; structured inter-session summaries prepared by two observers; flip-chart photographs and collaborative diagrams; formative evaluation findings from Work Package 2, including 36 key informant interviews and five focus group discussions; cultural adaptation documentation from Work Package 3; quantitative consensus voting records and a targeted synthesis of implementation science evidence on task-shifting and cognitive intervention delivery in LMICs (Singla et al., Reference Singla, Kohrt, Murray, Anand, Chorpita and Patel2017; Theobald et al., Reference Theobald, Brandes, Gyapong, El-Saharty, Proctor, Diaz and Peters2018).
Consensus voting data were analysed descriptively. For each proposed ToC component, the proportion of participants scoring the component 4 or 5 on the five-point agreement scale was calculated and compared with the prospectively defined 80% inclusion threshold. Components scoring 60–79% were revised based on documented deliberation and submitted to second-round voting. Components scoring below 60% were designated for exclusion or substantial reformulation, although no component ultimately met this criterion.
Qualitative deliberation data were analysed using framework analysis (Ritchie and Spencer, Reference Ritchie, Spencer, Huberman and Miles2002). Initial coding was organised deductively around RE-AIM and WHO ExpandNet domains, with CFIR constructs used to capture inner setting, outer setting and individual-level determinants (Damschroder et al., Reference Damschroder, Aron, Keith, Kirsh, Alexander and Lowery2009; World Health Organization, 2010; Glasgow et al., Reference Glasgow, Harden, Gaglio, Rabin, Smith, Porter and Estabrooks2019). Inductive coding was then used to identify contextual, cultural, relational and workflow-related themes not fully captured by the a priori framework categories. Particular attention was paid to how contested components were reformulated, how assumptions were linked to specific causal pathways and how stakeholder deliberation shaped the final ToC logic. NVivo was used to organise qualitative data. The final ToC map was produced using collaborative diagramming tools and subsequently rendered as a professional graphic, with two rounds of stakeholder email review before finalisation.
Reflexivity
Workshops were facilitated by Nigerian academics with formal training in psychiatry, public mental health and implementation science, several of whom had also led the preceding formative evaluation and cultural adaptation phases of CognIFiEd. YRT co-facilitators were young adults aged 22–28 with lived experience of psychosis who had been trained as co-researchers across the wider programme. This configuration carried specific reflexivity risks. Academic facilitators’ prior investment in the intervention may have predisposed them toward particular causal assumptions, while institutional authority differentials may have shaped whose views were voiced, amplified or withheld during deliberation. The Nigerian professional context, in which hierarchy by age, clinical status and institutional seniority may be socially salient, could have further intensified these dynamics.
Several mitigation strategies were used. Workshops incorporated small-group sessions that included stakeholders with no prior involvement in intervention adaptation; validation exercises explicitly invited critique of causal links, assumptions and feasibility claims; YRT co-facilitation created structured opportunities for lived-experience perspectives to shape discussion and anonymous voting reduced the visibility of disagreement during consensus procedures. Where facilitator assumptions appeared to be shaping group agreement, structured interruption prompts were used to reopen deliberation and invite alternative interpretations. The authors nonetheless acknowledge that the reflexivity record remains partial. External facilitation or a fuller participatory action research design might have provided a stronger mechanism for examining facilitator positionality, particularly in relation to gender, professional hierarchy, socio-economic position and institutional authority.
Ethical considerations
Ethical approval was obtained from the Health Research Ethics Committee of Lagos State University Teaching Hospital (LREC/06/10/2373), Federal Neuropsychiatric Hospital Yaba (FNPHY/HREC/2024/001/11/279) and Neuropsychiatric Hospital Aro (PR/0031/25). All procedures adhered to the principles of the Declaration of Helsinki. Workshop participants provided written informed consent emphasising voluntary participation, the right to withdraw without penalty and confidentiality protections. YRT members and service user representatives received financial remuneration for time and transport at rates equivalent to research assistant roles, reflecting the study’s commitment to non-tokenistic co-production.
Results
Participatory process outcomes
Workshop participation was high across the five-session ToC development process. Attendance was 25/25 participants in Workshop 1, 24/25 in Workshop 2, 25/25 in Workshop 3, 24/25 in Workshop 4 and 23/25 in Workshop 5. All participants who missed a workshop received structured inter-session summaries and briefing materials before the next session. Overall, all 25 stakeholders attended at least four of the five workshops, with a median attendance of five workshops, giving an overall retention rate of 96%. Session-by-session attendance by stakeholder group is provided in Supplementary Table S2.
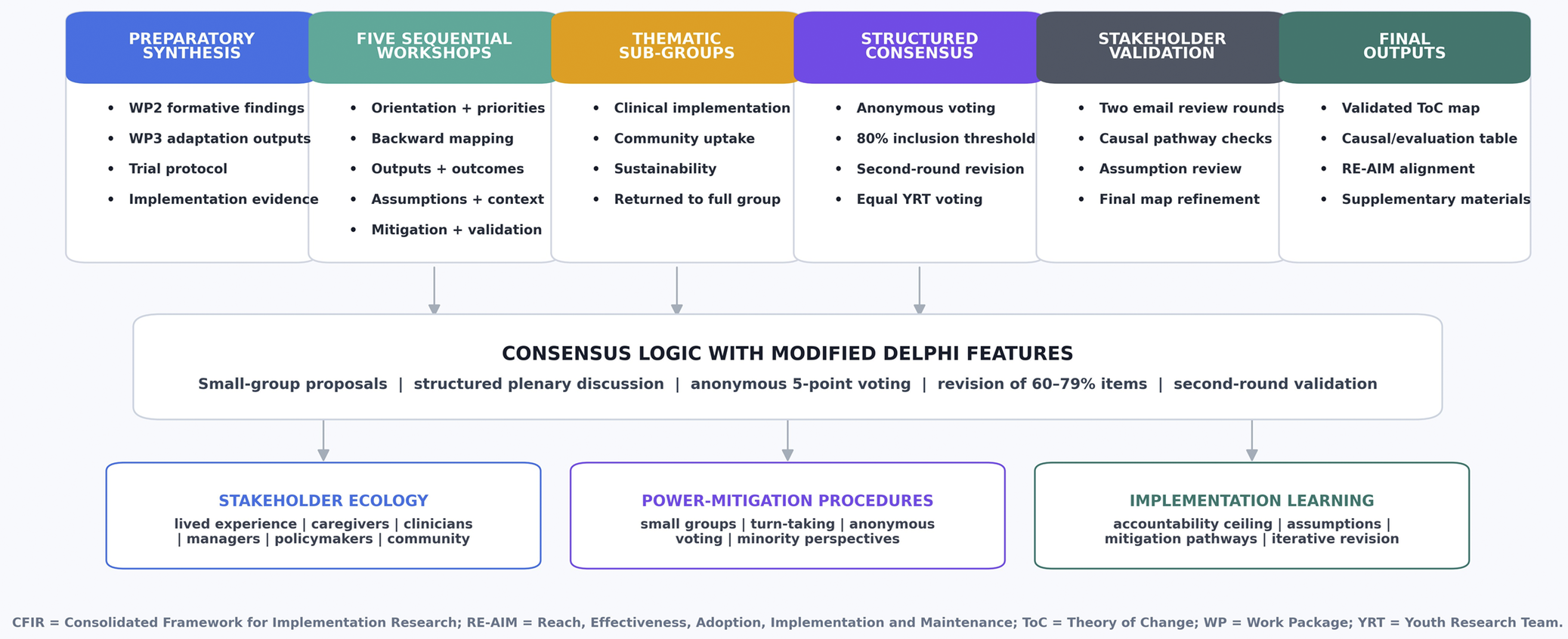
Consensus was achieved for 47 of 51 proposed ToC components, or 92%, in first-round voting. The remaining four components reached consensus after structured deliberation and second-round voting, with no components excluded. Post-workshop surveys indicated high satisfaction with the process (mean 4.6/5.0), strong perceived influence on ToC content (mean 4.4/5.0) and high confidence in the ToC as an implementation guide (mean 4.5/5.0). These process indicators suggest that the structured consensus procedure was both feasible and acceptable to stakeholders, including young people with lived experience, caregivers, frontline providers, hospital administrators and policymakers (Figure 1).
Participatory theory of change co-production process.

Figure 1. Long description
The flowchart is organized into three vertical tiers.
Top Tier: Six sequential stages represented by colored headers with bulleted lists.
1. PREPARATORY SYNTHESIS (Blue): Includes W P 2 formative findings, W P 3 adaptation outputs, trial protocol, and implementation evidence.
2. FIVE SEQUENTIAL WORKSHOPS (Green): Includes orientation plus priorities, backward mapping, outputs plus outcomes, assumptions plus context, and mitigation plus validation.
3. THEMATIC SUB-GROUPS (Yellow): Includes clinical implementation, community uptake, sustainability, and returned to full group.
4. STRUCTURED CONSENSUS (Purple): Includes anonymous voting, 80 percent inclusion threshold, second-round revision, and equal Y R T voting.
5. STAKEHOLDER VALIDATION (Grey): Includes two email review rounds, causal pathway checks, assumption review, and final map refinement.
6. FINAL OUTPUTS (Teal): Includes validated T o C map, causal/evaluation table, R E-A I M alignment, and supplementary materials.
Middle Tier: A central horizontal box labeled CONSENSUS LOGIC WITH MODIFIED DELPHI FEATURES. It lists small-group proposals, structured plenary discussion, anonymous 5-point voting, revision of 60-79 percent items, and second-round validation.
Bottom Tier: Three foundational boxes.
1. STAKEHOLDER ECOLOGY: Lived experience, caregivers, clinicians, managers, policymakers, and community.
2. POWER-MITIGATION PROCEDURES: Small groups, turn-taking, anonymous voting, and minority perspectives.
3. IMPLEMENTATION LEARNING: Accountability ceiling, assumptions, mitigation pathways, and iterative revision.
Footer: Defines C F I R as Consolidated Framework for Implementation Research, R E-A I M as Reach, Effectiveness, Adoption, Implementation and Maintenance, T o C as Theory of Change, W P as Work Package, and Y R T as Youth Research Team.
Overview of the CognIFiEd theory of change
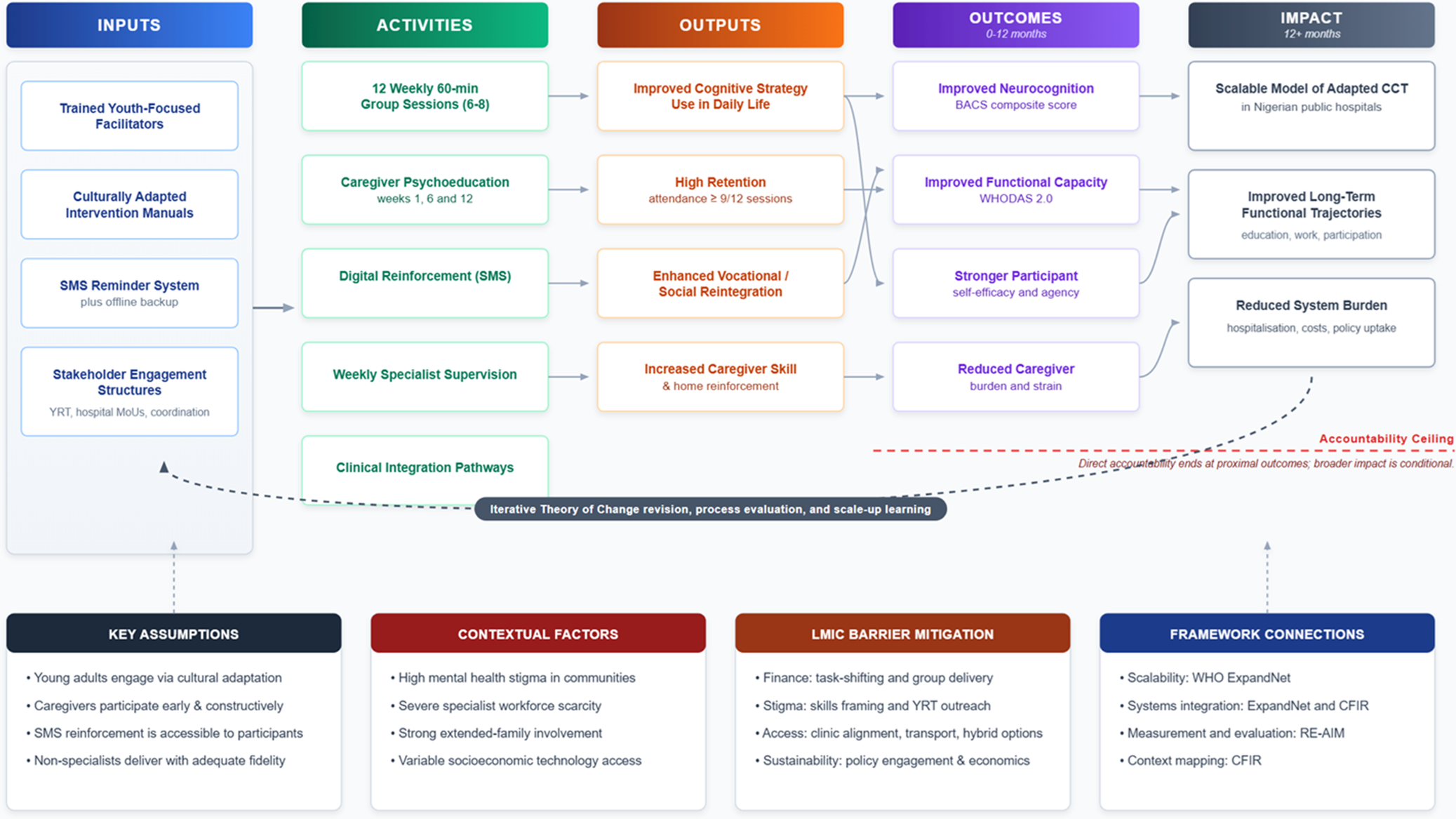
The final CognIFiEd ToC map (Figure 2) presents an implementation logic model linking Inputs, Activities, Outputs, Outcomes and Impact for task-shifted CCT in Nigerian public psychiatric services. Four cross-cutting elements are embedded within the ToC architecture: Key Assumptions, Contextual Factors, LMIC Barrier Mitigation Pathways and Implementation Framework Connections. The detailed articulation of ToC domains, causal rationales, key assumptions and indicators is presented in Table 2.
CognIFiEd Theory of Change Map.

Figure 2. Long description
The flowchart is organized into five main vertical columns connected by arrows.
1. Inputs: Includes trained youth-focused facilitators, culturally adapted intervention manuals, S M S reminder system with offline backup, and stakeholder engagement structures such as Y R T and hospital M o Us.
2. Activities: Lists 12 weekly 60-minute group sessions, caregiver psychoeducation at weeks 1, 6, and 12, digital reinforcement via S M S, weekly specialist supervision, and clinical integration pathways.
3. Outputs: Connects activities to improved cognitive strategy use, high retention (attendance greater than or equal to 9 forward slash 12 sessions), enhanced vocational or social reintegration, and increased caregiver skill.
4. Outcomes (0 to 12 months): Includes improved neurocognition (B A C S composite score), improved functional capacity (W H O D A S 2.0), stronger participant self-efficacy, and reduced caregiver burden.
5. Impact (12 plus months): Features a scalable model of adapted C C T in Nigerian public hospitals, improved long-term functional trajectories, and reduced system burden regarding hospitalization and costs.
A horizontal dashed line labeled Accountability Ceiling separates outcomes from impacts. Below the main flow, four foundational boxes list Key Assumptions, Contextual Factors, L M I C Barrier Mitigation, and Framework Connections including W H O ExpandNet, C F I R, and R E-A I M. A curved feedback loop at the bottom indicates iterative theory of change revision and scale-up learning.
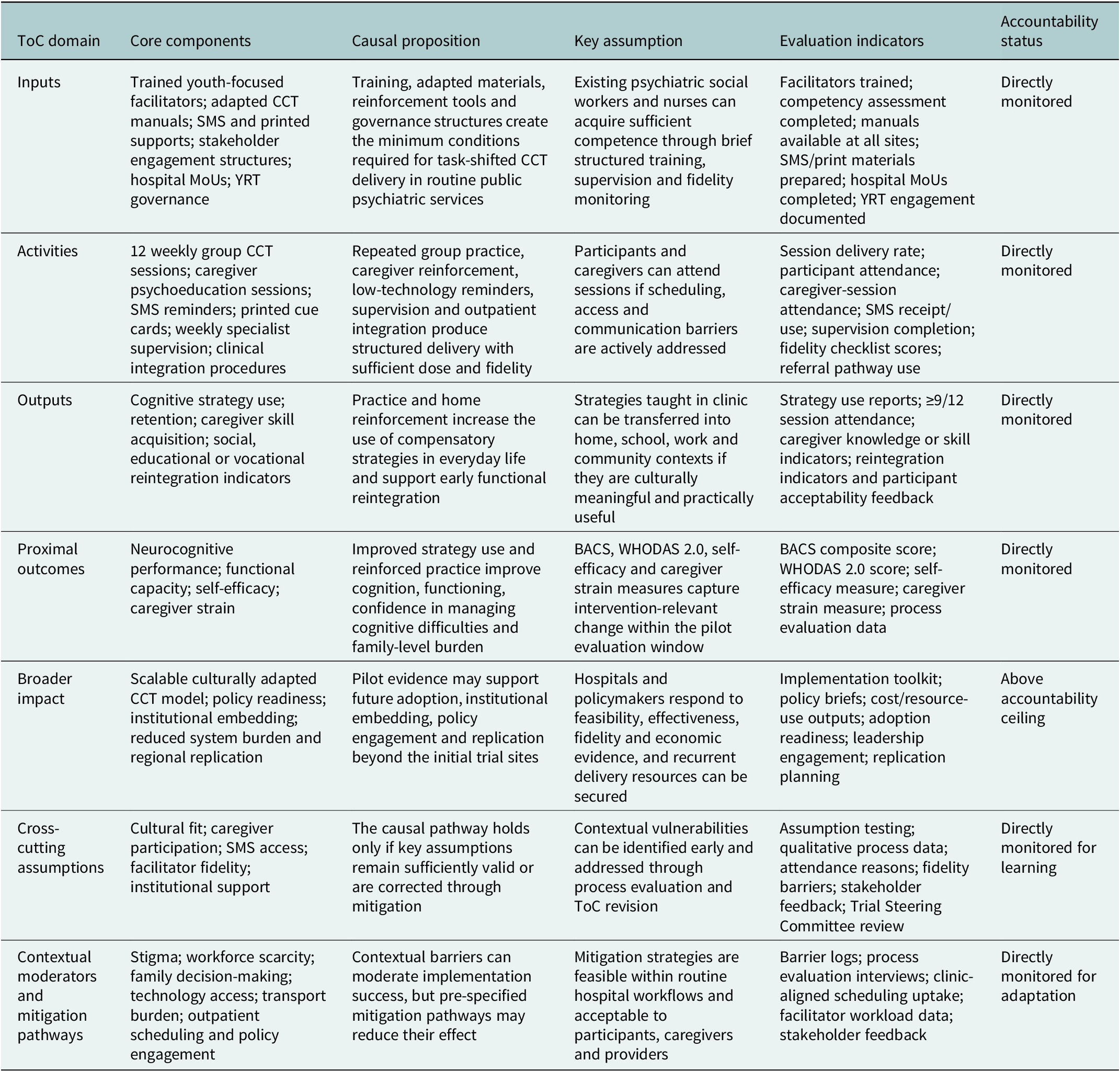
CognIFiEd theory of change domains, causal propositions, evaluation indicators and accountability status

Table 2. Long description
The table consists of six columns: T o C domain, Core components, Causal proposition, Key assumption, Evaluation indicators, and Accountability status.
* Inputs: Includes trained facilitators, C C T manuals, S M S, and printed supports. Causal proposition states these create minimum conditions for task-shifted delivery. Accountability: Directly monitored.
* Activities: Includes 12 weekly group C C T sessions, caregiver psychoeducation, and specialist supervision. Causal proposition focuses on structured delivery with sufficient dose and fidelity. Accountability: Directly monitored.
* Outputs: Includes cognitive strategy use and social reintegration. Causal proposition suggests practice increases compensatory strategy use in everyday life. Accountability: Directly monitored.
* Proximal outcomes: Includes neurocognitive performance and functional capacity. Causal proposition links improved strategy use to better cognition and reduced family burden. Accountability: Directly monitored.
* Broader impact: Includes scalable C C T models and policy readiness. Causal proposition suggests pilot evidence supports future adoption. Accountability: Above accountability ceiling.
* Cross-cutting assumptions: Includes cultural fit and institutional support. Causal proposition states the pathway holds only if assumptions remain valid. Accountability: Directly monitored for learning.
* Contextual moderators and mitigation pathways: Includes stigma, workforce scarcity, and transport burden. Causal proposition notes that barriers can moderate success but mitigation may reduce effects. Accountability: Directly monitored for adaptation.
Notes: BACS = Brief Assessment of Cognition in Schizophrenia; CCT = Compensatory Cognitive Training; MoU = memorandum of understanding; ToC = Theory of Change; WHODAS = WHO Disability Assessment Schedule; YRT = Youth Research Team. The accountability ceiling distinguishes outcomes the CognIFiEd programme will actively monitor and can reasonably attribute within the pilot trial from broader system-level impacts that may be influenced by the programme but cannot be attributed to it alone.
The ToC incorporates an explicit accountability ceiling. Outcomes below this ceiling are those the CognIFiEd programme will actively monitor and for which it can reasonably claim programme-level attribution within the pilot trial window: attendance and retention, cognitive strategy use, caregiver skill acquisition, neurocognitive performance, functional capacity, self-efficacy and caregiver strain. Outcomes above the accountability ceiling, including scalable model establishment, reduced system burden, policy integration and long-term functional trajectories, are treated as broader impact aspirations. These may be influenced by CognIFiEd but depend on additional factors beyond direct programme control, including institutional adoption, budgetary decisions, political will and health system dynamics.
Causal pathway from inputs to activities
Four categories of inputs were identified as necessary preconditions for implementation. First, trained youth-focused facilitators, primarily psychiatric social workers and nurses from existing hospital workforces, constitute the core human resource for the task-shifted delivery model. Their role is supported by a 5-day competency-based training programme, structured manuals, fidelity tools and weekly specialist supervision, consistent with task-shifting evidence from LMIC mental health implementation (Singla et al., Reference Singla, Kohrt, Murray, Anand, Chorpita and Patel2017). Second, culturally adapted intervention materials, including the CCT client workbook, therapist guide and supervisor manual, provide the material infrastructure for delivery while preserving the core therapeutic mechanisms of CCT (Wiltsey Stirman et al., Reference Wiltsey Stirman, Baumann and Miller2019). Third, SMS reminders and printed materials provide low-technology reinforcement between sessions, with printed materials functioning as an equity safeguard for participants with unreliable handset access. Fourth, stakeholder engagement structures, including hospital memoranda of understanding, YRT involvement and routine coordination mechanisms, provide governance and feedback channels.
The causal logic linking inputs to activities is that implementation cannot begin or cannot be sustained with fidelity, unless human resources, adapted materials, reinforcement tools and institutional authorisation are in place. The task-shifting pathway depends particularly on the assumption that non-specialist facilitators can acquire adequate competence through brief structured training, ongoing supervision and fidelity monitoring (Singla et al., Reference Singla, Kohrt, Murray, Anand, Chorpita and Patel2017).
Activities and immediate implementation outputs
Five core activity streams were specified. The primary delivery activity is a 12-week sequence of 60-min group CCT sessions, delivered to groups of six to eight participants in outpatient settings. These sessions are designed to teach and practise compensatory strategies for prospective memory, attention, verbal learning and memory, executive functioning and problem-solving, consistent with the therapeutic targets of CCT and compensatory interventions for cognitive impairment in psychosis (Twamley et al., Reference Twamley, Vella, Burton, Heaton and Jeste2012; Allott et al., Reference Allott, Van-der-El, Bryce, Parrish, McGurk, Hetrick, Bowie, Kidd, Hamilton, Killackey and Velligan2020). Caregiver psychoeducation sessions at weeks 1, 6 and 12 are intended to strengthen home-based reinforcement and reduce conflict between clinical advice and family expectations, consistent with evidence supporting family involvement in early psychosis care (Claxton et al., Reference Claxton, Onwumere and Fornells-Ambrojo2017). Automated SMS reminders support between-session practice, while printed cue cards provide an offline alternative. Weekly 90-min facilitator supervision by a psychiatrist or clinical psychologist provides the main fidelity and clinical safety mechanism. Clinical integration procedures, including documentation in hospital records, coordination with treating clinicians and referral pathways for complex presentations, are intended to embed CCT within routine care rather than as a stand-alone research activity.
These activities are expected to generate four immediate outputs. First, participants are expected to demonstrate increased use of cognitive strategies in daily life. Second, the intervention aims to achieve adequate therapeutic exposure, operationalised as attendance at at least 9 of 12 sessions, or 75% of the intervention dose. Third, participants are expected to show early signs of social, educational or vocational reintegration through greater use of cognitive strategies outside the clinic. Fourth, caregivers are expected to acquire greater knowledge and practical skill in supporting strategy use at home.
Proximal outcomes and broader impact
Four proximal outcomes were identified as measurable within the pilot evaluation window. Improved neurocognitive performance on the Brief Assessment of Cognition in Schizophrenia (BACS) represents the primary cognitive outcome (Keefe et al., Reference Keefe, Goldberg, Harvey, Gold, Poe and Coughenour2004). Improved functional capacity on the World Health Organisation Disability Assessment Schedule 2.0 (WHODAS 2.0) captures whether cognitive strategy acquisition translates into real-world functioning (Üstün et al., Reference Üstün, Chatterji, Kostanjsek, Rehm, Kennedy, Epping-Jordan, Saxena, von Korff and Pull2010). Stronger self-efficacy reflects participants’ confidence in managing daily cognitive challenges and is treated as a potential mediator between strategy use and functional improvement. Reduced caregiver strain reflects the family-level pathway through which caregiver understanding and home reinforcement may influence intervention sustainability.
Three broader impacts were specified above the accountability ceiling. The first is the establishment of a scalable model of culturally adapted cognitive rehabilitation for young adults with FEP in Nigerian public hospitals. The second is improvement in long-term functional trajectories, including educational, vocational and social participation. The third is reduced health system burden through fewer crisis presentations, reduced hospital utilisation, improved productivity and contribution to the global evidence base for cognitive interventions in LMICs. These impacts are included in the ToC because they define the long-range implementation vision, but they are not treated as outcomes attributable to the pilot trial alone.
Key assumptions and conditional mitigation logic
Stakeholders identified four assumptions as carrying the greatest risk of non-fulfilment. First, young people with FEP will engage meaningfully with the intervention if materials are culturally relevant, non-stigmatising and practically useful. This assumption is vulnerable to competing work or educational demands, family expectations, stigma and transport costs. Second, caregivers will participate when engaged early and constructively, although employment demands, caregiver burden and transport barriers may reduce attendance. Third, SMS reinforcement will be accessible to most participants, but this assumption may fail where participants have unreliable phone access, low privacy or changing numbers. Fourth, non-specialist facilitators can deliver the intervention with adequate fidelity, provided that structured training, supervision and referral protocols are sustained.
Each assumption was linked to a pre-specified mitigation pathway. Youth engagement risks are addressed through YRT-informed materials, skills-based rather than illness-centred framing, retention monitoring and flexible scheduling. Caregiver participation risks are addressed through early invitation, brief caregiver sessions aligned with clinic attendance and emphasis on practical support rather than blame or surveillance. Technology access risks are addressed through SMS as a low-cost modality and printed cue cards as a complete offline alternative. Facilitator fidelity risks are addressed through competency-based training, weekly supervision, fidelity checklists and escalation pathways for clinical concerns. A fuller elaboration of these assumptions, including empirical grounding, vulnerabilities and mitigation strategies, is provided in Supplementary Table S3.
Contextual factors and LMIC barrier mitigation pathways
Four contextual factors were mapped as likely moderators of implementation outcomes. Community stigma surrounding mental health conditions was identified as a threat to reach, retention, disclosure and social reintegration, consistent with evidence on stigma and discrimination in Nigeria and other LMIC settings (Gureje et al., Reference Gureje, Lasebikan, Ephraim-Oluwanuga, Olley and Kola2005; Semrau et al., Reference Semrau, Evans-Lacko, Koschorke, Ashenafi and Thornicroft2015). Severe specialist workforce scarcity made task-shifting operationally necessary but raised concerns about workload, role boundaries and supervision capacity (Patel et al., Reference Patel, Saxena, Lund, Thornicroft, Baingana, Bolton, Chisholm, Collins, Cooper, Eaton, Herrman, Herzallah, Huang, Jordans, Kleinman, Medina-Mora, Morgan, Niaz, Omigbodun, Prince, Rahman, Saraceno, Sarkar, de Silva, Singh, Stein, Sunkel and UnÜtzer2018; Fadele et al., Reference Fadele, Igwe, Toluwalogo, Udokang, Ogaya and Lucero-Prisno2024). Extended-family involvement was viewed as both a facilitator of home-based reinforcement and a potential constraint on young people’s autonomy. Variable technology access created equity concerns, particularly for participants with unstable phone access, limited privacy or intermittent ability to receive messages.
Five LMIC-focused mitigation pathways were embedded in the ToC. Financial constraints are addressed through task-shifting, group-based delivery and use of existing hospital staff rather than a specialist workforce (Singla et al., Reference Singla, Kohrt, Murray, Anand, Chorpita and Patel2017). Stigma is addressed through YRT-led outreach, a skills-building frame for CCT and engagement with community and religious stakeholders where appropriate. Staff shortages are addressed through brief competency-based training, weekly supervision, fidelity tools and a reserve pool of trained facilitators. Access barriers are addressed through hospital-based scheduling, alignment of intervention sessions with outpatient appointment days and selective transport support where required. Sustainability is addressed through early engagement with hospital leadership and policymakers, integration into outpatient workflows, health economic evaluation and advocacy for inclusion in mental health service guidelines (World Health Organization, 2010).
Stakeholder reflections on the co-production process
Post-workshop qualitative feedback from surveys, facilitator field notes and inter-session summaries yielded five recurrent themes. First, participants described a shift from role-specific perspectives to a shared understanding of the wider implementation ecology, including how managerial decisions, clinical workflows, family expectations and community stigma interact. Second, structured assumption elicitation prompted stakeholders to reconsider expectations that had initially been treated as self-evident, particularly around caregiver availability, digital access and facilitator capacity. Third, YRT co-facilitation was described as changing the tone of deliberation, with young people with lived experience participating as co-analysts of implementation feasibility rather than as symbolic representatives. Fourth, reframing barriers as conditional problems with mitigation pathways helped stakeholders move from pessimism about system constraints toward practical planning. Fifth, stakeholders viewed the ToC as a living implementation hypothesis to be tested and refined during the pilot trial, rather than a fixed diagram, consistent with ToC approaches that treat causal models as revisable guides for implementation learning and evaluation (De Silva et al., Reference De Silva, Lee and Ryan2015; Breuer et al., Reference Breuer, De Silva, Shidaye, Petersen, Nakku, Jordans, Fekadu and Lund2016).
Discussion
Principal findings and contributions
This article presents, to our knowledge, the first systematic participatory ToC co-production process documented for a cognitive intervention targeting psychosis in sub-Saharan Africa. The resulting ToC specifies not only the intervention components required for task-shifted CCT but also the assumptions, contextual contingencies, causal pathways, mitigation strategies, evaluation indicators and accountability boundaries through which implementation will be tested. In this respect, the ToC extends conventional logic models by treating delivery infrastructure as part of the intervention’s causal architecture rather than as a neutral background condition (Blamey and Mackenzie, Reference Blamey and Mackenzie2007; De Silva et al., Reference De Silva, Lee and Ryan2015; Breuer et al., Reference Breuer, De Silva, Shidaye, Petersen, Nakku, Jordans, Fekadu and Lund2016).
Three contributions are especially salient. First, the study extends cultural adaptation beyond content modification toward health system integration, foregrounding workforce, supervision, caregiver involvement, outpatient workflow and policy engagement as determinants of whether the adapted intervention can be delivered with fidelity (Wiltsey Stirman et al., Reference Wiltsey Stirman, Baumann and Miller2019). Second, it embeds sustainability considerations at the design stage through early hospital and policymaker engagement, clinic-aligned delivery planning, health economic evaluation and an explicit accountability ceiling distinguishing programme-monitored outcomes from broader system-level aspirations (Saraceno et al., Reference Saraceno, van Ommeren, Batniji, Cohen, Gureje, Mahoney, Sridhar and Underhill2007; World Health Organization, 2010). Third, it contributes a structured implementation methodology for a field in which cognitive rehabilitation for severe mental health conditions in sub-Saharan Africa remains underdeveloped and only minimally represented in the published literature (Deste et al., Reference Deste, Kokou, Barlati, Nibbio, Del Debbio, Lucchi-Piccinini and Vita2024).
Situating the CognIFiEd ToC within global mental health ToC literature
The CognIFiEd ToC sits within a growing body of participatory ToC work in global mental health. Breuer and colleagues demonstrated the value of ToC for planning and evaluating mental health services in LMICs, particularly by using participatory workshops to make implementation assumptions explicit (Breuer et al., Reference Breuer, De Silva, Shidaye, Petersen, Nakku, Jordans, Fekadu and Lund2016). The PRIME programme further showed that ToC-informed planning can support mental health service integration in African primary care systems (Lund et al., Reference Lund, Tomlinson and Patel2016). Abayneh and colleagues extended this tradition by developing a ToC model for service user and caregiver involvement in mental health system strengthening in rural Ethiopia (Abayneh et al., Reference Abayneh, Lempp, Alem, Kohrt, Fekadu and Hanlon2020), while Kamvura and colleagues used ToC to support development of an integrated intervention for depression, diabetes and hypertension within the Friendship Bench programme in Zimbabwe (Kamvura et al., Reference Kamvura, Turner, Chiriseri, Dambi, Verhey and Chibanda2021). More recently, Hiltensperger and colleagues applied ToC to peer support implementation across high-, middle- and low-income settings (Hiltensperger et al., Reference Hiltensperger, Ryan, Adler Ben-Dor, Charles, Epple, Kalha, Korde, Kotera, Mpango, Moran, Mueller-Stierlin, Nixdorf, Ramesh, Shamba, Slade, Puschner and Nakku2024).
CognIFiEd builds on this literature in three ways. First, it applies participatory ToC development to cognitive rehabilitation for psychosis, a domain not directly addressed by PRIME or most prior African ToC studies. Second, it combines lived-experience co-production with formal consensus procedures, making stakeholder agreement visible rather than implicit. Third, it integrates ToC with RE-AIM, CFIR and WHO ExpandNet, linking causal implementation theory to evaluation constructs, contextual determinants and scale-up planning (Damschroder et al., Reference Damschroder, Aron, Keith, Kirsh, Alexander and Lowery2009; World Health Organization, 2010; Glasgow et al., Reference Glasgow, Harden, Gaglio, Rabin, Smith, Porter and Estabrooks2019). The contribution is therefore not that ToC itself is new to African mental health, but that this study applies and extends ToC methodology to a neglected intervention domain where both implementation fit and sustainability are uncertain.
The task-shifting proposition under scrutiny
A central assumption in the CognIFiEd ToC is that psychiatric social workers and nurses, equipped with structured manuals, competency-based training, fidelity tools and ongoing supervision, can deliver a manualised cognitive intervention with sufficient quality. Evidence for task-shifting is strong for common mental health conditions in LMICs, but more limited for cognitive rehabilitation targeting severe mental health conditions, where delivery quality may depend on clinical judgement, session pacing, error correction and the ability to adapt examples without diluting core mechanisms (Singla et al., Reference Singla, Kohrt, Murray, Anand, Chorpita and Patel2017; Deste et al., Reference Deste, Kokou, Barlati, Nibbio, Del Debbio, Lucchi-Piccinini and Vita2024).
The ToC therefore does not presume that task-shifting will automatically succeed. Rather, it specifies the conditions under which task-shifted delivery is plausible: protected facilitator time, brief but competency-based training, structured manuals, weekly specialist supervision, fidelity monitoring and referral pathways for complex presentations. Provider validation data and earlier adaptation work suggest that social workers and nurses may be well-positioned to deliver CCT if these supports are sustained. Ethically, however, task-shifting should not become task-dumping. Stakeholders therefore treated workload negotiation with hospital management as an implementation input rather than an optional administrative detail.
Function over form in cultural adaptation
The ToC co-production process operationalised a function over form principle, defining fidelity in terms of preservation of core therapeutic mechanisms rather than strict replication of the original delivery format (Wiltsey Stirman et al., Reference Wiltsey Stirman, Baumann and Miller2019). All five CCT cognitive domains were retained: prospective memory and organisation, attention and working memory, verbal learning and memory, executive functioning and problem-solving (Twamley et al., Reference Twamley, Vella, Burton, Heaton and Jeste2012; Allott et al., Reference Allott, Van-der-El, Bryce, Parrish, McGurk, Hetrick, Bowie, Kidd, Hamilton, Killackey and Velligan2020). Delivery was adapted to fit Nigerian public psychiatric settings: sessions were condensed to 60 min; materials were produced in Nigerian Pidgin and English using locally familiar examples; technical strategy labels were simplified and problem-solving scenarios were rewritten to reflect everyday Nigerian contexts.
This distinction is important for implementation science because fidelity and adaptation are often framed as competing imperatives. In the CognIFiEd ToC, they are treated as interdependent. Fidelity protects therapeutic mechanisms, while adaptation protects fit, acceptability and feasibility (Wiltsey Stirman et al., Reference Wiltsey Stirman, Baumann and Miller2019). Cultural vignettes developed with the YRT, including memory cues embedded in daily routines, illustrate how compensatory strategies can be made contextually meaningful without abandoning their intended function. A session-by-session overview of the adapted CCT-Nigeria curriculum is provided in Supplementary File S4.
Stigma as a systemic barrier
Stakeholders consistently identified stigma as a pervasive threat to implementation. Stigma was understood not only as an individual attitude but also as a systemic barrier operating across interpersonal relationships, family decision-making, community interpretation of psychosis, disclosure, service attendance and reintegration into education or work. This framing is consistent with global mental health evidence that stigma undermines help-seeking, adherence and social participation in LMICs (Gureje et al., Reference Gureje, Lasebikan, Ephraim-Oluwanuga, Olley and Kola2005; Semrau et al., Reference Semrau, Evans-Lacko, Koschorke, Ashenafi and Thornicroft2015).
The ToC responds to stigma through multiple mechanisms: framing CCT as practical skills-building rather than as deficit correction; incorporating YRT-informed messaging; engaging caregivers early and recognising the influence of community and religious actors on help-seeking and recovery narratives. YRT members played a particularly important role in challenging deficit-focused language and shifting the communication strategy toward recovery, agency and everyday functioning. This is one of the clearest examples of how lived-experience co-production altered the causal logic of implementation rather than merely validating expert assumptions.
Theory of change as accountability infrastructure
Beyond planning, the CognIFiEd ToC functions as accountability infrastructure in a specific, failure-diagnostic sense (Weiss, Reference Weiss, Connell, Kubisch, Schorr and Weiss1995; De Silva et al., Reference De Silva, Lee and Ryan2015). The four key assumptions identified through stakeholder deliberation: youth engagement contingent on cultural fit, caregiver participation contingent on early and constructive engagement, SMS reinforcement contingent on handset access and privacy and non-specialist fidelity contingent on training and supervision, become testable propositions during the pilot trial. If retention falls below the 75% therapeutic dose threshold, the ToC provides a structured way to examine whether this reflects transport barriers, caregiver non-involvement, stigma, scheduling difficulties or facilitator fidelity issues. Each explanation implies a different adaptation response. The feasibility and progression criteria that will guide Trial Steering Committee review are detailed in Supplementary File S5.
The accountability ceiling further clarifies what the programme can reasonably claim. Attendance, cognitive strategy use, neurocognitive performance, functional capacity, self-efficacy and caregiver strain are programme-monitored outcomes within the pilot evaluation window. By contrast, reduced system burden, policy uptake and long-term functional trajectories are broader impact aspirations that require further evidence and depend on political, institutional and economic conditions beyond the pilot trial. This distinction is important because it protects the ToC from becoming an over-claiming advocacy tool and instead positions it as a disciplined implementation hypothesis.
Caregiver engagement and relational implementation ecology
The participatory process highlighted the centrality of family systems to implementation success. In many Nigerian households, family members influence treatment decisions, attendance, daily routines and opportunities to practise strategies outside the clinic. Caregiver engagement is therefore not merely a logistical adjunct to the intervention; it is part of the relational ecology through which cognitive strategies may generalise into everyday life (Claxton et al., Reference Claxton, Onwumere and Fornells-Ambrojo2017).
By including caregiver psychoeducation as a core activity and caregiver strain reduction as an explicit outcome, the ToC recognises that functional recovery is partly mediated through family understanding, reinforcement and reduced conflict around cognitive difficulties. At the same time, caregiver involvement must be managed carefully so that it supports young people’s autonomy rather than reinforcing surveillance or dependence. The pilot process evaluation should therefore examine not only caregiver attendance but also how caregivers understand and use the strategies at home.
Digital health as equity-conscious reinforcement
The ToC’s digital strategy is deliberately modest. Rather than positioning mobile technology as the primary delivery channel, stakeholders selected SMS reminders as a low-cost reinforcement mechanism that can operate on basic handsets without requiring internet access. Printed cue cards function as a complete offline fallback. This design choice reflects an equity-conscious approach to digital mental health: technology is used only where it strengthens between-session practice without making participation dependent on smartphone ownership, data affordability or stable connectivity (Patel et al., Reference Patel, Saxena, Lund, Thornicroft, Baingana, Bolton, Chisholm, Collins, Cooper, Eaton, Herrman, Herzallah, Huang, Jordans, Kleinman, Medina-Mora, Morgan, Niaz, Omigbodun, Prince, Rahman, Saraceno, Sarkar, de Silva, Singh, Stein, Sunkel and UnÜtzer2018; Theobald et al., Reference Theobald, Brandes, Gyapong, El-Saharty, Proctor, Diaz and Peters2018).
This approach is particularly relevant in LMIC implementation contexts where digital innovation can inadvertently widen inequities if access is assumed rather than tested. In CognIFiEd, digital reinforcement is therefore treated as supplementary rather than essential. The pilot trial will need to assess whether SMS reminders are received, understood, private and useful, and whether offline materials adequately protect participants with limited or unstable phone access.
Sustainability from inception
Sustainability was treated as a design concern from the outset rather than a post-trial aspiration. The ToC addresses sustainability through two linked strategies: embedding CCT within existing hospital infrastructure and staffing and generating evidence that can support policy and budgetary decisions. This includes early engagement with hospital leadership and policymakers, development of training and supervision materials, health economic evaluation and advocacy for possible inclusion of task-shifted cognitive rehabilitation within mental health service guidelines (Saraceno et al., Reference Saraceno, van Ommeren, Batniji, Cohen, Gureje, Mahoney, Sridhar and Underhill2007; World Health Organization, 2010).
One practical sustainability issue raised by stakeholders concerns access to hospital-based sessions. If participation requires additional hospital visits, long-term delivery may depend on transport reimbursement, which is unlikely to be sustainable at scale. Aligning CCT sessions with established outpatient appointment days may reduce this burden and improve feasibility for both participants and caregivers. The pilot process evaluation should therefore examine whether clinic-aligned scheduling is operationally feasible across sites and whether it improves attendance, retention and caregiver participation. The proposed sustainability and scale-up trajectory, including feedback loops for iterative ToC revision, is illustrated in Supplementary Figure S6.
Strengths and limitations
Several strengths and limitations warrant consideration. Key strengths include the integration of multiple implementation frameworks, the use of structured consensus procedures alongside qualitative deliberation, the equal weighting of lived-experience perspectives in voting and synthesis and the prospective alignment of ToC domains with evaluation constructs. The high workshop retention rate and stakeholder satisfaction scores suggest that the process was experienced as meaningful and feasible by a diverse group of participants.
These strengths should be interpreted alongside limitations. The stakeholder pool was drawn from South-West Nigeria and largely urban or peri-urban tertiary settings, limiting the extent to which the ToC reflects rural, northern Nigerian or primary care implementation contexts. The ToC remains a pre-implementation hypothesis whose assumptions have not yet been empirically tested in the pilot trial. Although the participatory process was designed to reduce hierarchy, groupthink and professional power differentials may still have shaped deliberation. Policymaker representation was limited, which may have constrained the robustness of scale-up pathways. Facilitators’ prior involvement in earlier CognIFiEd phases may also have shaped assumption elicitation in ways not fully captured by the reflexivity procedures. Finally, although caregiver engagement was strongly foregrounded, the optimal dose, timing and format of caregiver sessions remain to be refined during implementation.
Future directions
For researchers and implementers in comparable settings, the CognIFiEd ToC process offers four transferable lessons. First, treating ToC development as a distinct pre-pilot phase can generate testable assumptions and failure-diagnostic anchors before implementation begins. Second, structured consensus procedures, when combined with anonymous voting and small-group deliberation, may help manage power differentials in mixed stakeholder groups. Third, sustainability should be specified as a causal pathway with identifiable preconditions rather than appended as a later aspiration. Fourth, lived-experience co-facilitation can materially alter implementation logic by making visible forms of stigma, access burden and service-user priorities that expert-led processes may miss.
Within the CognIFiEd programme, the next step is to test and revise the ToC through the mixed-methods process evaluation in Work Package 5, guided by RE-AIM and CFIR. Table 3 shows how the ToC domains will be operationalised through RE-AIM evaluation constructs. Key assumptions will function as pre-specified evaluation propositions, and ToC revision will be reviewed at Trial Steering Committee intervals. Economic evaluation will be important for determining whether task-shifted CCT can be sustained within existing hospital budgets and whether evidence is sufficient to support policy uptake. Beyond Nigeria, the ToC methodology may inform cognitive rehabilitation implementation in other sub-Saharan African settings, although direct transfer should be avoided in favour of local adaptation.
Alignment of CognIFiEd ToC domains with RE-AIM evaluation constructs

Table 3. Long description
The table consists of five columns and five rows of data.
1. Reach: Focuses on recruitment, uptake, and engagement. The evaluation question asks who participates and what barriers exist. Indicators include recruitment and retention numbers, attendance logs, and demographics. Constraints include stigma, transport costs, and family gatekeeping.
2. Effectiveness: Focuses on proximal outcomes like cognition and caregiver strain. The evaluation question asks if task-shifted C C T improves functioning. Indicators include B A C S composite scores, W H O D A S 2.0, and qualitative accounts. Constraints include small pilot samples and short evaluation windows.
3. Adoption: Focuses on hospital participation and leadership support. The evaluation question asks if sites and facilitators adopt C C T as feasible. Indicators include site participation, facilitator retention, and hospital M o U s. Constraints include workload pressure and staff turnover.
4. Implementation: Focuses on delivery fidelity and supervision. The evaluation question asks if C C T is delivered as intended with adaptation. Indicators include fidelity checklists, session logs, and S M S use. Constraints include workforce scarcity and inconsistent phone access.
5. Maintenance: Focuses on institutional embedding and sustainability. The evaluation question asks if C C T can be sustained beyond the pilot. Indicators include health economic outputs, policy briefs, and toolkit development. Constraints include funding uncertainty and policy turnover.
Notes: BACS = Brief Assessment of Cognition in Schizophrenia; CCT = Compensatory Cognitive Training; RE-AIM = Reach, Effectiveness, Adoption, Implementation and Maintenance; ToC = Theory of Change; WHODAS = WHO Disability Assessment Schedule. This table was moved into the main manuscript from the former supplementary RE-AIM alignment table to make explicit how the ToC will guide process evaluation and implementation learning.
Conclusions
The CognIFiEd ToC process offers a broader lesson for implementation science in global mental health: the voltage drop often observed when evidence-based interventions move from controlled settings into low-resource health systems is not inevitable. It may reflect insufficient attention to the causal, relational, organisational and policy conditions required for interventions to work in routine care (Fixsen et al., Reference Fixsen, Naoom, Blase, Friedman and Wallace2005; Singla et al., Reference Singla, Kohrt, Murray, Anand, Chorpita and Patel2017; Skivington et al., Reference Skivington, Matthews, Simpson, Craig, Baird, Blazeby, Boyd, Craig, French, McIntosh, Petticrew, Rycroft-Malone, White and Moore2021). Structured, participatory pre-trial ToC development provides one way to make these conditions explicit before implementation begins (De Silva et al., Reference De Silva, Lee and Ryan2015; Breuer et al., Reference Breuer, De Silva, Shidaye, Petersen, Nakku, Jordans, Fekadu and Lund2016).
Across five workshops, 25 stakeholders spanning clinical, experiential, managerial, community and policy perspectives co-produced an implementation logic model for task-shifted CCT in Nigerian public psychiatric services. The resulting ToC specifies inputs, activities, outputs, proximal outcomes, long-term impact aspirations, causal assumptions, contextual moderators, mitigation pathways and an accountability ceiling. It also positions lived experience not as an ethical supplement to expert planning but as a substantive input into causal reasoning.
For cognitive rehabilitation in LMIC mental health systems, this work suggests that implementation planning should be treated with the same rigour as intervention adaptation. Making the implementation logic visible, contestable and open to revision may improve the likelihood that evidence-based cognitive interventions can be delivered in ways that are acceptable, feasible, equitable and sustainable within constrained public systems.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10267.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2026.10267.
Data availability statement
The qualitative datasets generated and analysed during this study, including framework analysis outputs, structured inter-session summaries and consensus voting records, are not publicly available because of ethical restrictions and participant confidentiality protections. De-identified analytic materials may be made available from the corresponding author on reasonable request and subject to institutional ethics committee approval.
Acknowledgements
The authors gratefully acknowledge the Youth Research Team members whose co-facilitation throughout the Theory of Change workshops was central to the integrity and cultural grounding of this work. We are also grateful to Professor Elizabeth Twamley (University of California, San Diego, USA) for permission to copy, modify and distribute the Compensatory Cognitive Training Manual. We thank the management and clinical staff of Lagos State University Teaching Hospital, Federal Neuropsychiatric Hospital Yaba and Neuropsychiatric Hospital Aro, Abeokuta, Nigeria for their institutional support and for facilitating stakeholder access during data collection. We are also grateful to all workshop participants, including service users, caregivers, community representatives and policymakers, who contributed their time and expertise to the co-production process.
Author contribution
A.O.A. led conceptualisation, methodology, funding acquisition, project administration, supervision and writing of the original draft. O.E.O., B.O. and A.O. contributed to conceptualisation and methodology. O.E.O., A.O.A., B.A.O., A.O., A.A., A.E. and A.L. contributed to investigation, data curation and formal analysis. All authors contributed to writing, review and editing, approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
Funding statement
This work was supported by the Wellcome Trust Mental Health Research Award (A.O.A., grant number 226720/Z/22/Z). The funder had no role in study design; data collection, analysis or interpretation; the decision to publish or preparation of the manuscript.
Competing interest
The authors declare no competing interests.
Ethics and approvals
This study received ethical approval from the Health Research Ethics Committee of Lagos State University Teaching Hospital, Ikeja, Lagos (LREC/06/10/2373), the Ethics Committee of Federal Neuropsychiatric Hospital Yaba (FNPHY/HREC/2024/001/11/279) and the Ethics Committee of Neuropsychiatric Hospital Aro (PR/0031/25). All procedures were conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all workshop participants before participation. Youth Research Team members and service user participants received financial remuneration for time and transport at rates equivalent to research assistant roles, consistent with the study’s commitment to non-tokenistic co-production.
Consent for publication
Not applicable. No individual-level identifiable data are reported in this manuscript.



 Open access
Open access
Comments
The Editors
Global Mental Health
Cambridge University Press
Dear Editors,
We write to submit for your consideration the manuscript entitled “Developing a Theory of Change for Implementing Cognitive Interventions in Low-Resource Settings: The CognIFiEd Study” for publication in Global Mental Health.
Cognitive impairment affects more than 75% of young people with first-episode psychosis and is the strongest determinant of long-term functional disability, yet cognitive rehabilitation remains virtually absent from public mental health services across sub-Saharan Africa. The implementation gap in this context is not primarily a problem of intervention efficacy; it reflects the absence of structured, contextually grounded planning that can translate evidence into sustainable practice within severely resource-constrained health systems. This paper addresses that gap directly.
We describe the participatory development of a Theory of Change (ToC) for the CognIFiEd study, a task-shifted Compensatory Cognitive Training intervention for young adults with first-episode psychosis across three tertiary psychiatric hospitals in South-West Nigeria, funded by the Wellcome Trust Mental Health Research Award (grant number 226720/Z/22/Z).
To our knowledge, this is the first systematically documented, participatory ToC co-production process for a cognitive intervention targeting psychosis in sub-Saharan Africa. The work makes three contributions we believe are of particular relevance to readers of Global Mental Health.
First, the ToC extends cultural adaptation beyond content modification toward health system integration, treating delivery infrastructure as requiring as much deliberate design as the intervention itself. Second, by integrating WHO ExpandNet, RE-AIM, and the Consolidated Framework for Implementation Research within a single co-production process, the paper offers a replicable implementation methodology for researchers working in comparable low- and middle-income country settings. Third, the systematic inclusion of young people with lived experience of psychosis as co-producers, weighted equally to clinical and policy stakeholders in all consensus procedures, produced an implementation model grounded in the realities of recovery in Nigerian communities rather than assumptions imported from high-income settings.
The manuscript reports the process and outputs of five structured co-production workshops with 25 stakeholders, achieving 92% first-round consensus and 96% retention across all sessions. It presents a fully specified implementation logic model alongside explicit mapping of key assumptions, contextual barriers, and mitigation pathways, and discusses implications for sustainability and scale-up that extend beyond the Nigerian context.
This work aligns with Global Mental Health’s commitment to advancing implementation science in low- and middle-income settings and to research approaches that centre community voice alongside clinical evidence. The manuscript has not been published previously and is not under consideration elsewhere. All authors have approved the submitted version and agree to be accountable for the work.
We would be grateful for the opportunity to contribute this work to your journal and are happy to provide any additional information the editorial team may require.
Yours sincerely,
Abiodun Adewuya