


Introduction
Children with complex CHD, including those with hypoplastic left heart syndrome, have an increased prevalence of neurodevelopmental impairments, which span across childhood and all domains of development. Reference Brosig, Butcher and Buter1–Reference Wernovsky7 The aetiologies for developmental differences are multifactorial and include prenatal, perioperative, genetic, vascular, and socioeconomic factors. Reference Wernovsky7 Operative techniques utilised for aortic arch reconstruction during a Norwood operation, including deep hypothermic circulatory arrest, have been implicated as potential contributors to this risk. Deep hypothermic circulatory arrest is the traditional perfusion technique for the Norwood operation, allowing for a bloodless field and diminishing the risk of embolism. Deep hypothermia at a nasopharyngeal temperature of 18°C lowers the metabolic needs of the brain. However, since deep hypothermic circulatory arrest has been associated with worse neurodevelopmental outcomes in some studies, Reference Newburger, Jonas and Wernovsky8–Reference Bellinger, Wypij and duPlessis11 regional cerebral perfusion has been adopted by several centres as an alternative. With regional cerebral perfusion, the patient is still cooled, but cerebral circulation is maintained throughout arch reconstruction, often through a graft anastomosed to the innominate artery.
The first randomised trial comparing the functional neurodevelopmental outcomes of children assigned to either deep hypothermic circulatory arrest or regional cerebral perfusion was performed at the University of Michigan between 2001 and 2005. Neurodevelopmental outcomes were evaluated using the Bayley Scales of Infant Development-II, Psychomotor Development Index and Mental Development Index, before second-stage palliation and at 1 year of age. There were no significant differences found between the two groups. Reference Goldberg, Bove and Devaney4
This study used the same cohort of patients with the main objective of assessing the neurodevelopmental outcomes of children who underwent the Norwood operation with regional cerebral perfusion or deep hypothermic circulatory arrest at 5 and 10 years of age. We also aimed to determine whether the neurodevelopmental scores at age 1 were predictive of neurodevelopmental scores at school age.
Materials and methods
Study population
Children enrolled in the regional cerebral perfusion randomised controlled trial of infants with single ventricle undergoing the Norwood operation with randomisation to aortic arch reconstruction with either regional cerebral perfusion or deep hypothermic circulatory arrest conducted at the University of Michigan Congenital Heart Center were included. Reference Goldberg, Bove and Devaney4 Participants were enrolled from October 2001 through February 2005. The inclusion criteria for the study consisted of single ventricle heart disease requiring Norwood operation at age 30 days or less. Patients with a known genetic syndrome, a known history of maternal substance abuse, <2 kg and/or less than 32 weeks gestation at the time of birth were excluded from participation in the original trial. There were no additional exclusion criteria for the cohort of patients to continue in this study. At 5 years of age, participants were invited to complete a comprehensive neurodevelopmental evaluation with a neuropsychologist. At the age of 10, the parents of the participants were contacted and sent parent report instruments to measure the participant’s behaviour and executive function. Institutional Review Board guidelines were followed and informed consent was obtained from the parents for all study participants.
Demographics
Demographic data including sex, race, prenatal diagnosis, cardiac anatomy, gestational age, and birth weight were collected before randomisation as summarised in the original study. Reference Goldberg, Bove and Devaney4 At the time of initial neurodevelopmental assessment, the Hollingshead Four Factor Index was used to quantify socioeconomic status based on parental education and employment, with a scale ranging from 8 (lowest socioeconomic level) to 66 (highest socioeconomic level). Reference Hollingshead12
Measures of neurologic and developmental outcome
At 5 years of age, comprehensive neurodevelopmental testing across multiple domains was performed to provide a broad assessment of neurodevelopment. Testing was administered by a psychometrician under the guidance of a neuropsychologist, both of whom were blinded to the initial perfusion technique. General intelligence was assessed with the Wechsler Intelligence Scales (WPPSI and WISC-IV); using a full scale intelligence quotient (IQ) score including verbal, performance, and processing speed scores. The average score is 100 with a standard deviation of 15 points. Reference Wechsler13 Attentiveness and impulsivity were evaluated by Conner’s Continuous Performance Test (CPT, K-CPT). Reference Conners14 Behaviour was evaluated with the Behaviour Assessment System for Children Parent Rating Scale (BASC-PRS-P and BASC-PRS-C) and the Behaviour Rating Inventory of Executive Function (BRIEF-P and BRIEF). Reference Reynolds15,Reference Gioia, Isquith, Guy and Kenworthy16 Visual memory, visual attention, and working memory/planning were assessed with the Cambridge Neuropsychological Test Automated Battery. Reference Robbins17 For those children over the age of 5, memory function was further evaluated by the Children’s Memory Scale across three domains including auditory/verbal learning, visual/nonverbal learning, and working memory/attention/concentration. Reference Cohen18 The children’s memory scale is validated for ages 5–16 years, thus the six subjects who were slightly under the age of 5 did not complete this portion of the testing. Receptive vocabulary was assessed by the Peabody Picture Vocabulary Test (PPVT-IV). Reference Dunn19 Visual-spatial, fine motor, and integrated visual motor skills were evaluated with the Wide Range Assessment of Visual Motor Abilities. Reference Adams20 At 10 years of age, behaviour and executive function were re-evaluated through parental completion of the BRIEF and BASC. The Achenbach Child Behaviour Checklist (CBC-L) was also used to evaluate behaviour and parental perception of social and emotional function. Reference Achenbach21
Data analysis
The analysis was based on an intention-to-treat approach to compare the two treatment groups (regional cerebral perfusion vs. deep hypothermic circulatory arrest). Data were reported as frequency and percentage (%) for categorical variables, and mean ± standard deviation (SD) or median and interquartile range (IQR), depending on distributional assumption, for continuous variables. Patient demographics and clinical characteristics as well as neurodevelopmental test scores at 5- and 10-year follow-up were compared between regional cerebral perfusion and deep hypothermic circulatory arrest groups using Chi-square test or Fisher’s exact test for categorical variables, and Wilcoxon rank sum test or two-sample t-test for continuous, non-parametric variables. Correlations between the Bayley Scales of Infant Development-II (Mental Development Index and Psychomotor Development Index) at 1 year of age and Wechsler Full Scale IQ at 5 years of age were examined using Pearson correlation coefficient (r). Univariate associations of demographic, sociodemographic, and clinical characteristics with Wechsler Full Scale IQ scores at 5-year follow-up and the BASC behaviour symptoms index or adaptive skills and the BRIEF global executive composite at 10-year follow-up were evaluated using two-sample t-test for categorical variables and Pearson correlation coefficient for continuous variables. All analyses were performed using SAS Version 9.4 (SAS Institute Inc., Cary, NC) based on a significance level of 0.05 using two-sided tests.
Results
Participant characteristics
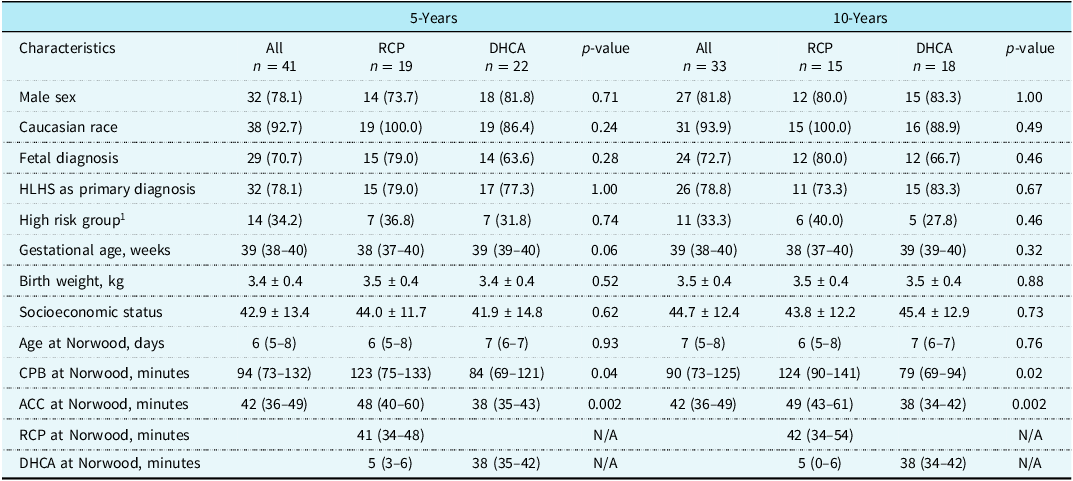
Of 77 patients enrolled in the initial randomised controlled trial, 49 (64%) were alive at 5 years of age and, of these, 41 returned for in-person evaluation. Seven patients were lost to follow-up, and one patient was too ill to participate in neurodevelopmental testing. At 10 years, 33 of the 41 patients completed the 10-year assessment. Seven patients were lost to follow-up, and one patient died. There was no significant difference between the regional cerebral perfusion and deep hypothermic circulatory arrest groups in survival at any time point. Table 1 presents the demographic and clinical characteristics of the regional cerebral perfusion and deep hypothermic circulatory arrest subgroups at 5-year and 10-year follow-ups. The median age at 5-year and 10-year follow-ups were 5.2 years (IQR 5.0–5.8) and 10.9 years (IQR 9.6–11.5), respectively, without differences between the treatment groups. There was no group difference in demographics and preoperative characteristics at either 5 or 10 years, including preoperative clinical shock or seizures.
Demographics and clinical characteristics of RCP versus DHCA subgroups

RCP = regional cerebral perfusion; DHCA = deep hypothermic circulatory arrest; HLHS = hypoplastic left heart syndrome; CPB = cardiopulmonary bypass; ACC = aortic cross-clamp.
1 High risk defined as pulmonary venous obstruction, <36 weeks gestational age and/or <2.5 kg at birth, or clinical shock or seizures pre-operatively. Data are presented as n (%) for categorical variables and median (interquartile range) or mean ± standard deviation for continuous variables. P-value from Chi-square test or Fisher’s exact test for categorical variables and Wilcoxon rank sum test or two-sample t-test for continuous variables.
When comparing surgical parameters, patients assigned to regional cerebral perfusion had a longer cardiopulmonary bypass time during the Norwood operation (median 123 vs. 84 minutes in the 5-year group; p = 0.04) and (median 124 vs. 79 minutes in the 10-year group; p = 0.02). This was further reflected in a greater cumulative cardiopulmonary bypass time, through all lifetime surgeries, upon Fontan completion in the 10-year follow-up (median 273 vs. 229 minutes; p = 0.03). Patients assigned to regional cerebral perfusion also required a longer aortic cross-clamp time during the Norwood operation (median 48 vs. 38 minutes in the 5-year group; p = 0.002) and (median 49 vs. 38 minutes in the 10-year group; p = 0.002). Patients randomised to regional cerebral perfusion still required a brief period of deep hypothermic circulatory arrest (mean 5 minutes) for delivery of cardioplegic solution and positioning of the arterial cannula for regional cerebral perfusion.
Developmental outcomes
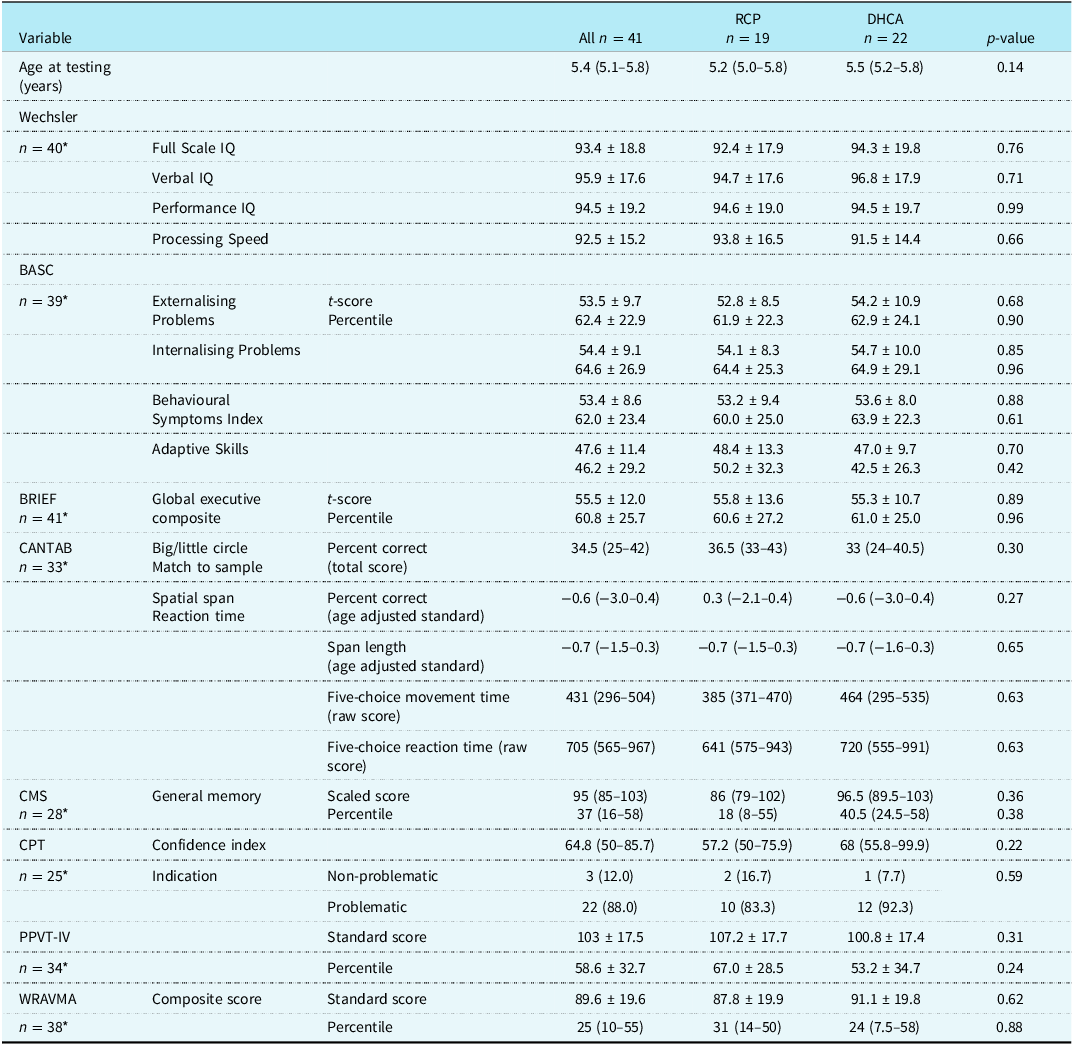
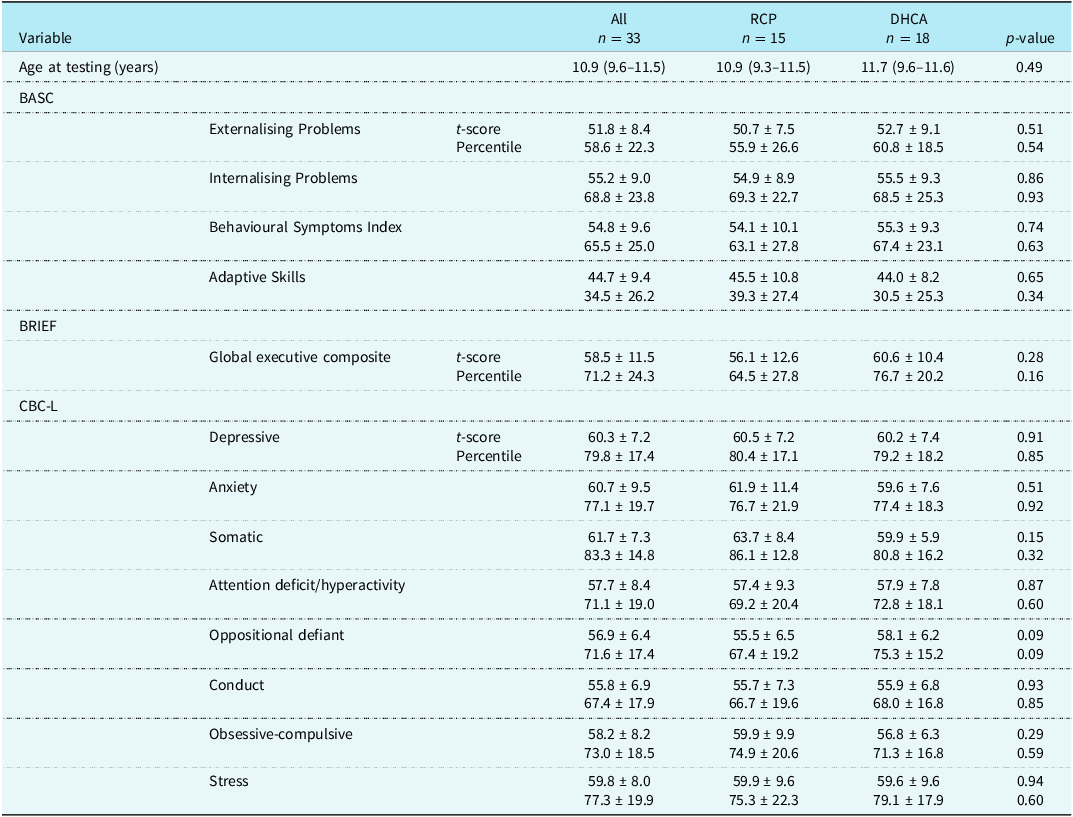
There was no significant difference between the regional cerebral perfusion and deep hypothermic circulatory arrest groups on any of the neurodevelopmental tests performed for the 5-year evaluation (Table 2). The average Wechsler Intelligence Scale score (WISC-IV) was 93 ± 19 without a significant difference between the treatment groups (92.4 ± 17.9 for regional cerebral perfusion vs. 94.3 ± 19.8 for deep hypothermic circulatory arrest, p = 0.76). This was similar across each of the WISC-IV domains. There were no significant differences between the regional cerebral perfusion and deep hypothermic circulatory arrest treatment groups in the average scores for the BASC, BRIEF, Cambridge Neuropsychological Test Automated Battery, children’s memory scale, Peabody Picture Vocabulary Test-IV, and Wide Range Assessment of Visual Motor Abilities (Table 2), and most of these scores were within the normal range. The reaction time on the Cambridge Neuropsychological Test Automated Battery was slower for the study cohort compared to the general population (median 705 vs. 416 s). Reference Cohen18 A majority (88%) of the study cohort also displayed a propensity towards inattention and impulsivity according to the CPT. Table 3 summarises the neurodevelopmental test scores at 10-year follow-up. Again, there were no significant differences between the regional cerebral perfusion and deep hypothermic circulatory arrest groups. The study cohort performed within the average range for the general population (t-score mean of 50 with standard deviation of 10 for all 3 tests) on the BASC, BRIEF, and CBC-L, although scores were at the higher end of normal for anxiety (60.7 ± 9.5), somatic complaints (61.7 ± 7.3), and stress (59.8 ± 8.0) according to results from the CBC-L.
Neurodevelopmental test scores at 5 year follow-up
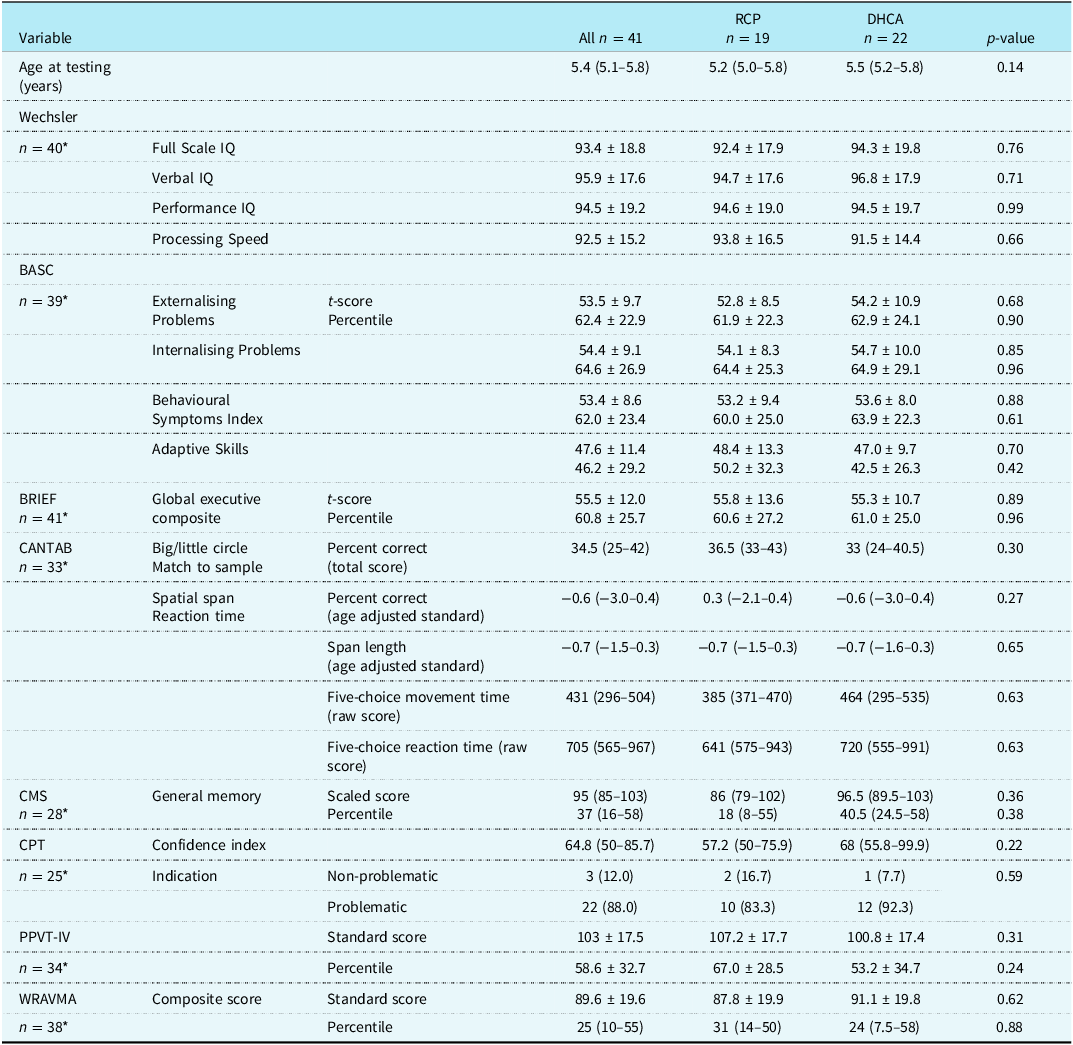
RCP = regional cerebral perfusion; DHCA = deep hypothermic circulatory arrest; IQ = intelligence quotient; BASC = behaviour assessment system for children; BRIEF = behaviour rating inventory of executive function; CANTAB = Cambridge neuropsychological test automated battery; CMS = children’s memory scale; CPT = Conner’s continuous performance test; PPVT-IV = Peabody’s picture vocabulary test; WRAVMA = wide range assessment of visual motor abilities.
* Not all patients were able to complete all testing either due to inability or ineligibility for testing based on age. Data are presented as n (%) for categorical variables and median (interquartile range) or mean ± standard deviation for continuous variables. p-value from Fisher’s exact test for categorical variables and Wilcoxon rank sum test or two-sample t-test for continuous variables.
Neurodevelopmental test scores at 10 year follow-up
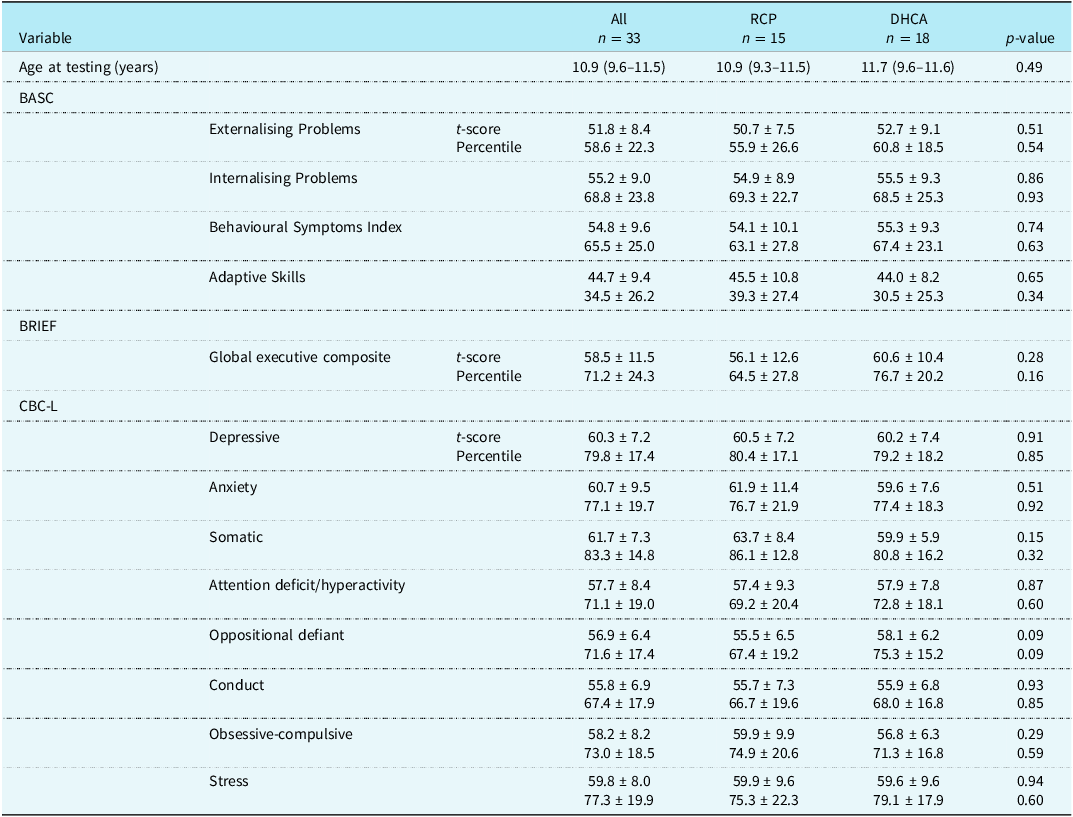
RCP = regional cerebral perfusion; DHCA = deep hypothermic circulatory arrest; BASC = behaviour assessment system for children; BRIEF = behaviour rating inventory of executive function; CBC-L = children’s behaviour checklist. Data are presented as median (interquartile range) or mean ± standard deviation. P-value from Wilcoxon rank sum test or two-sample t-test.
The Bayley Scales of Infant Development-II at 1 year of age for the entire cohort were compared to the Wechsler Full Scale IQ scores at 5 years of age. Both the Bayley’s Mental Development Index and Psychomotor Development Index yielded a modest yet significant correlation with the Wechsler Full Scale IQ scores; Mental Development Index r = 0.64 (p < .0001) and Psychomotor Development Index r = 0.68 (p < .0001) (Figure 1). Additionally, patients with a score less than 1 SD below the mean (<85) on the Bayley Scales for Infant Development-II Mental Development Index and Psychomotor Development Index had a negative predictive value of 86.7 and 94.7, respectively, on the Weschler Full Scale IQ at 5 years. However, scoring greater than 85 on the Bayley scales Mental Development Index or Psychomotor Development Index did not preclude a score on the Wechsler FSIQ more than 1 SD below the population mean.
Correlations of the Bayley scales of infant development-II, MDI and PDI, at 1 year of age with Wechsler full scale IQ at 5 years of age.

Through univariate comparisons of demographic and medical factors with WISC-IV scores at 5-year follow-up, prenatal diagnosis was associated with higher scores on the WISC-IV; Wechsler Intelligence Scale full scale (97.0 ± 18.2 versus 84.1 ± 17.5; p = 0.05), verbal (99.6 ± 17.4 versus 86.0 ± 14.4; p = 0.03), and performance (98.3 ± 18.1 versus 84.5 ± 19.0; p = 0.04) IQ scores. There was also a significant association of higher socioeconomic status with higher Wechsler Intelligence Scale full scale (r = 0.33, p = 0.04), verbal (r = 0.35, p = 0.03), and performance (r = 0.35, p = 0.03) IQ scores. Of note, prenatal diagnosis was positively correlated with socioeconomic status (p = 0.002). At 10-year follow-up, there was no association of sociodemographic or clinical characteristics with either the BASC behaviour symptoms index or adaptive skills or the BRIEF global executive composite.
Discussion
This is the first published study of long-term outcomes of children with single ventricle heart disease who were randomly assigned for their newborn Norwood operation to the perfusion strategy of regional cerebral perfusion versus deep hypothermic circulatory arrest. No significant differences were found across numerous neuropsychological domains between the treatment groups.
Animal studies have suggested that regional cerebral perfusion could reduce brain injury and improve neurodevelopmental outcomes. Reference Myung, Petko and Judkins22–Reference Mavroudis, Ko and Volk24 However, these findings have not translated to humans with CHD. There have been several studies comparing early neurological outcomes between regional cerebral perfusion and deep hypothermic circulatory arrest in single ventricle heart disease. The initial study of infants from this cohort did not demonstrate statistical differences between the two treatment groups, although the RCP group had lower Bayley Mental Development Index and Psychomotor Development Index at pre-stage II operation and 12 months of age. Similarly, despite hypothesising that the use of regional cerebral perfusion would be associated with improved neurologic outcomes, to date, no studies in humans have shown differences in early neurodevelopment. Reference Goldberg, Bove and Devaney4,Reference Visconti, Rimmer and Gauvreau25,Reference Newburger, Sleeper and Bellinger26 Algra et al. also found no difference in post-operative MRI findings or neurodevelopment at two years of age. Reference Algra, Jansen and van der Tweel27 The 5- and 10-year follow-up results described through this study support the conclusion that regional cerebral perfusion is not superior to deep hypothermic circulatory arrest for neurodevelopmental outcomes in children with single ventricle heart disease.
Similar to other research measuring neurodevelopment among children with Fontan palliation, the overall cohort from the regional cerebral perfusion versus deep hypothermic circulatory arrest trial were found to have lower scores on neurodevelopmental evaluation than expected for the general population. Reference Rogers, Msall and Buck28–Reference Mahle and Wernovsky31 At 5 years old, our cohort showed a tendency towards impulsivity and inattention, consistent with other studies indicating a higher level of inattentiveness and/or impulsive behaviour for children who have undergone a Fontan palliation. Reference Gaynor, Ittenbach and Gerdes32
We did observe that there was an association between the Mental Development Index and the Psychomotor Development Index of the Bayley Scales of Infant Development, compared to full scale IQ at 5 years measured by the Wechsler. Nonetheless, there are children with low Bayley scores who had FSIQ in the normal range and others with high Bayley scores who had concerns identified on Wechsler IQ evaluation at 5 years of age. Given that, to date, it is not possible to accurately predict who will have difficulties with learning and development in school age, serial evaluations are required to ensure that evolving learning and developmental impairments are identified in time for therapeutic interventions. Reference Sood, Newburger and Anixt33 Our cohort demonstrated that both higher socioeconomic status and prenatal diagnosis were associated with improved full scale, verbal, and performance IQ scores at 5 years of age. Similar to others, we found a significant association of prenatal diagnosis with higher socioeconomic status. Reference Bartlett, Wypij and Bellinger34 These results are comparable to those reported by Bartlett in a cohort of patients with transposition of the great arteries in which patients who were prenatally diagnosed had better neurodevelopmental scores and had a higher socioeconomic status. Reference Bartlett, Wypij and Bellinger34 Given a relatively small sample size, we were not able to disentangle the relative contributions of prenatal diagnosis and socioeconomic status to neurodevelopmental outcomes during the enrolment era for the original trial.
This study has several limitations including that this is a single-centre study and that, by 10-year follow-up, only 43% of the initial cohort completed the evaluation. Another limitation is the use of a single method of regional cerebral perfusion. Based on data that was current at the time, we used a fixed flow rate of 20 ml/kg/min. More recent studies have highlighted the use of near-infrared spectroscopy and transcranial Doppler ultrasound to titrate flow rates in an effort to standardise cerebral oxygen delivery, resulting in significantly higher flow rates of 40–80 ml/kg/min. Reference Pigula, Nemoto, Griffith and Siewers35,Reference Andropoulos, Stayer, McKenzie and Fraser36 However, even with this methodology, improved outcomes have not been demonstrated. While improved outcomes with these newer techniques have yet to be demonstrated, a contemporary study of regional cerebral perfusion utilising these approaches and measuring the effect on the brain would be valuable. Given the potential impact of institutional practice variation on outcomes, our findings may have limited generalisability.
Conclusion
In this study, the only randomised controlled trial comparing regional cerebral perfusion to deep hypothermic circulatory arrest with follow-up beyond pre-school age, neurodevelopment is impaired across the study cohort, but no differences were found between the regional cerebral perfusion and deep hypothermic circulatory arrest treatment groups. Bayley Scale scores at 1 year are somewhat predictive of early school-age performance, though imperfect, emphasising the importance of ongoing serial surveillance for all children with single ventricle physiology.
Acknowledgements
None.
Financial support
No external funding was received for this study.
Competing interests
The authors have no conflicts of interests to disclose.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of Title 45 of The Code of Federal Regulations Section 46 and with the Helsinki Declaration of 1975, as revised in 2008, and has been approved by the University of Michigan Institutional Review Board.


 Open access
Open access