

In the 1950s, Michael Balint wrote one of the signature texts for general practice: The doctor, his patient and the illness. (Reference Balint1) Balint was a psychoanalytic psychiatrist who pioneered a type of small group learning for GPs which came to be known as Balint groups. Balint groups encouraged doctors to reflect on the nature of therapeutic relationships, and to consider how these might be leveraged to improve care. Balint was an advocate of whole person care, and one of his core concepts was the ‘collusion of anonymity’, which described the situation where the patient is passed from one specialist to another with nobody taking responsibility for the whole person. The concept of collusion implied avoidance, the idea that each specialist chose to complete the relevant task at hand, but avoided engaging with the patient as a person.
I was reminded of Balint when considering the multiple options available to a survivor of sexual harassment in medicine. A survivor may have multiple options available to them if they choose to report, including law, medical regulatory bodies, workplace management processes, universities, and others. However, like the anonymous patients in Balint’s text, a survivor may well find themselves being moved from organisation to organisation, without anyone engaging with them as a person. The key feature of the collusion of anonymity is that none of the providers feel they have failed to manage the problem, and it is only the patient, or in this case the survivor, who experiences the demoralising impact of being shunted from place to place without having their issues resolved. Like Balint’s patients, the result is often the patient exiting from the process, unable to tolerate the demoralisation and exhaustion of trying to engage with a process causing them harm.
In 2023, there was a summit on sexual harassment in medicine in Australia, which aimed to address this exact problem. In a workshop, leaders from the various disciplines were asked to summarise what someone might expect should a survivor open their particular door and report sexual harassment to their organisation. Unsurprisingly, although there were clear policy frameworks available for each organisation, leaders were unable to find the answers to common questions asked by survivors (see figure 31.1). Without a clear understanding of what lies behind each ‘door’, reporting can be risky, bewildering, and feel profoundly unsafe.
The collusion of anonymity among organisations managing sexual harassment in medicine.
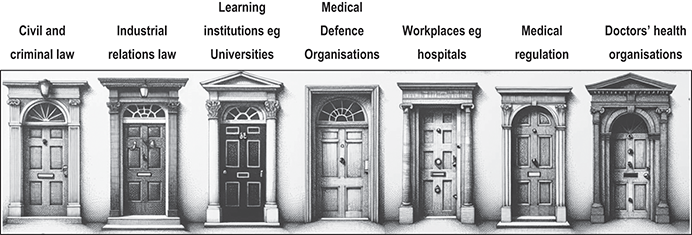
Figure 31.1 Long description
'The seven doors are each labelled with different sectors. The first door is labelled Civil and criminal law, the second door is labelled Industrial relations law, the third door is labelled Learning institutions like Universities, the fourth door is labelled Medical Defence Organisations, the fifth door is labelled Workplaces like hospitals, the sixth door is labelled Medical regulation, and the seventh door is labelled Doctors’ health organisations. Each door has a distinct architectural design.
| Civil and criminal law | Industrial relations law | Learning institutions eg Universities | Medical Defence Organisations | Workplaces eg hospitals | Medical regulation | Doctors’ health organisations |
|---|---|---|---|---|---|---|
| ||||||
In this, the final part of this book, we tackle the way forward for individual advocates and organisations so that survivors can have a better experience, and better outcomes. In doing so, we draw on examples of advocacy from a variety of perspectives. The point of advocacy is to lend one’s power to another, to facilitate change. We are aware that many will approach this book with a view to creating change, and so we wanted to conclude the book with some examples of people who have used their power in different ways to change the environment in which sexual harassment occurs.
In chapter 32, Elizabeth Teisberg and Deborah Cole consider the leadership challenge of being CEOs in organisations with poor culture. They describe how they, as managers, addressed this challenge to ensure a safer environment for their employees. In doing so, they discuss the personal and organisational strategies they use to achieve a lasting cultural shift.
In chapter 33, a number of authors reflect on their roles as advocates, using the lessons they have learned in their various contexts. Advocacy can occur on multiple levels, from one-on-one support to national or international campaigns. Using examples from their own work around sexual safety, they discuss the challenges of communicating effectively with a variety of audiences, and engaging people with different points of view.
Chapter 34 focuses on medical education. It is expected that strategies to change culture will differ according to the position advocates hold in an organisation. This chapter includes commentary by a medical student (Erlinger), doctors in training (Cox, Jewitt and Fleming) and medical educators for undergraduates and GPs in training (Stone and Moir). Together, these authors discuss the different ways change can be achieved, utilising the different forms of power and agency available to them at different stages of their careers.
Finally, in chapter 35, we focus on therapy, which is where this book began. The very first stage of recovery from sexual abuse is recognising the abuse, as it is frequently buried under natural defences like dissociation. The second stage involves breaking the silence to enable a survivor to tell their story. Sexual harassment can cause a significant psychological wound that needs expert treatment, and in this chapter, we consider what that treatment may entail, across the entire trajectory of trauma.
Together, the chapters in this part work to represent different ways of creating change. These efforts will always be more effective if the organisations around them provide transparent, consistent and trauma-informed policies that clearly align across the multiple actors in this complex policy environment. Collusions of anonymity that exhaust the survivor prevent effective management of abuse and, in doing so, maintain a culture that causes long-term harm.
Introduction
Sir Desmond Tutu said, ‘If you are neutral in situations of injustice, you have chosen the side of the oppressor.’ Too often, health care leaders have looked the other way when faced with inappropriate behaviour perpetrated by doctors. If leaders fail to create a culture of accountability and take decisive action against sexual harassment, we become complicit in the abuse.
Sexual harassment is one of the most extreme abuses of power, the ultimate act of disrespect. It is not just a legal and social issue, it is a chronic occupational health problem intrinsically linked to gender inequality. It takes a huge physical, psychological and emotional toll on impacted people. It also affects patient satisfaction and outcomes by impairing workplace productivity, safety, quality and innovation. Employees who feel unsafe or disrespected at work are less likely to share their innovative ideas and excel in their careers. At a time when health care is in desperate need of reform, we cannot afford for brilliant minds to stay silent.
A toxic culture is also felt and witnessed by patients, making them less likely to seek care and engage with clinicians. A workplace that is unsafe for women is a workplace that is unsafe for patients. As health professionals, we strive to improve the health outcomes of our patients so they can live long, fulfilling and happy lives. We cannot do that if we don’t create an environment that is respectful and inclusive with organisational systems and processes that empower people to speak up and take action when they see or encounter misconduct.
Change is difficult, particularly when dealing with an entrenched culture in medicine that warns against rocking the boat. A culture that has justified the criticism and humiliation of trainee doctors to be a rite of passage, a way to ‘toughen them up’ as they prepare for the rigours of their profession. A culture of fear and silence where complaints of sexual harassment have derailed or ended the careers of countless clinicians, mainly women.
Too many bright, capable doctors have been driven out of prestigious fields because bullying and sexual discrimination have continued to go unchallenged. Leaders have the power to ignite change, to draw a line in the sand and say ‘No more’. Good intentions are not enough. It takes strength, focus, time and collaboration. It requires you to lead with empathy while committing to decisive action underpinned by robust policies and processes, and clear measures for success.
If you talk about sexual harm among female doctors, chances are they will each have a personal story to tell. For Deborah, one in particular stands out:
When I was starting out in my health career, I would laugh nervously when a colleague said or did something inappropriate. I didn’t want to say anything for fear it would affect my career and I would be viewed as a bad sport, so I laughed. I brushed it off. I let it happen again and again and eventually I became desensitised to the culture so entrenched in hospitals, clinics and offices across Australia. Later in my career, I attended a social event with clinical colleagues. I thought because I was in my 50s and a respected health care leader, that I was safe from the behaviour I had witnessed and endured for over three decades.
There was a colleague at the function who thought it would be funny to walk up to the female doctors and shove his hand between their legs. No one was safe from his advances, including me. I felt shocked, embarrassed, angry and violated and yet, I let it go. I didn’t want to cause a scene or rock the boat so I just avoided him for the rest of the evening. Should I have confronted him? Yes. Should I have been put in that situation in the first place? Absolutely not.
For Elizabeth, another example stands out:
I was working at a university an ivy league medical school and was asked to attend an important meeting to discuss the future. When I arrived, three high level leaders were discussing the incidents of rape on the campus. Instead of demonising the actions of the perpetrators and discussing how to hold them accountable, the conversation was full of victim-blaming and demonstrated a distinct lack of empathy – The girls get so drunk, what do they expect? Boys will be boys, after all. Their main concern was not the welfare of the female students but rather the impact on the university’s reputation – How could they keep it quiet? How could they avoid a media storm?
All of the people involved in the discussion were men. Men with daughters at the same university, not that you should need a daughter to care about a woman’s suffering. I couldn’t believe what I was hearing. I was stunned and horrified. I meekly participated in the conversation that I was there to participate in but I was unhappy from that day on. Like Deborah, I often think about that day and wish I had confronted them. Wish I had stood up for the students who deserved so much better than judgement and blame. They deserved empathy and action.
In these situations we all like to think that we would speak up. Too many people don’t feel as though they can. As leaders, we need to create a workplace culture where people aren’t just enabled to speak up, but consider it an imperative – for themselves, their workplace, their patients, and the future of the profession they love. Like most things in health care, prevention and early intervention are key.
In this chapter, we share our experiences of effecting cultural change as health care leaders and educators in Australia and America. This a complex subject. We haven’t always gotten it right but when we have failed, we have learned, adapted and stayed the course. It is vital that we keep this conversation going, and that we continue to find ways to enhance accountability in health care. It is up to us to set the standard, build better systems, disrupt the status quo and lead with empathy. By learning from the past, we can create a future free from sexual harm. A future where our people are empowered to improve the health outcomes of the community in an environment that is safe, respectful, diverse and inclusive.
Barriers to Creating a Workplace Culture of Respect and Accountability
It’s difficult to have a zero-tolerance policy in the workplace when there is so much tolerance of sexual misconduct both within and outside of it. Within the hospital walls, there are hierarchical structures, unequal gender power dynamics, microcultures and a willingness to accept transgressions as ‘the way it is’. Instead of being applauded for speaking up, doctors report that seeking legal restitution can damage their personal wellbeing and standing among fellow doctors. (Reference Stone, Phillips and Douglas1)
The concept of a ‘power over’ culture rather than a ‘power with’ culture has been increasingly discussed in the health sector. A ‘power over’ culture is characterised by fear, hierarchy, judgment, silos, an ‘us versus them’ mentality and all the ‘isms’, including racism, favouritism and rankism. A ‘power with’ culture is characterised by collaboration, empathy, joy, gratitude, good mentorship, good talent management, shared decision-making, great patient experiences and positive patient outcomes. (Reference Kennedy Oehlert2) Whereas a ‘power over’ culture limits innovation and enables sexual misconduct to go unchecked, a ‘power with’ culture prioritises relationships at a strategic level and delivers the results you want.
While the modern approach to delivering health care is very team-based, that wasn’t always the case. A lot of doctors have progressed through their careers as the alpha decision-maker and aren’t used to being questioned or held to account when their behaviour doesn’t align with what’s expected. If a culture is characterised by ego rather than humility, then people are less likely to learn and improve the way they interact and operate.
Most health care settings will have a code of conduct along with a set of policies and procedures relating to sexual misconduct. However, these are often complicated, corporate documents that sit on the staff intranet and never get read after orientation. If you want to eradicate sexual harm, you need employees to understand what’s expected of them, how those expectations relate to your strategic goals and organisational values, and how your systems and processes support and guide their behaviour.
When sexual misconduct is reported, there can be a tendency to go easy on the alleged offender depending on the severity of the complaint. Over decades in health care, we have often seen managers deal with conflicting accounts of what transpired by transferring either the offender or complainant to a different department. It can be challenging to let staff go, especially when dealing with workforce shortages, but moving people around the organisation can contribute to a permissive culture where sexual misconduct is not just tolerated but enabled. Impacted people will only come forward if they feel safe doing so and if they have confidence that their complaint will be handled in a fair, compassionate and timely manner.
When dealing with sexual harassment complaints, people within your organisation will have competing priorities and concerns, including reputational damage, operational downtime, legal implications, workforce shortages, staff wellbeing and patient safety. People will also have varying views on what constitutes inappropriate behaviour based on their beliefs, upbringing and life experiences. They may have misguided beliefs that women have no place in their profession, that gender-based jokes should illicit laughs rather than condemnation and that commenting on a women’s appearance should be accepted as a compliment. It may sound obvious, but you cannot assume that people view the world as you do.
There are also powerful external influences at play. In Australia, we see footballers commit acts of violence against women and go on to enjoy thriving careers both on the field and in the media. In America, we’ve seen men accused of sexual assault and rape hold the highest positions of political power. The global media continues to objectify women and promote gender stereotypes, and women experience disproportionate levels of abuse through social media platforms.
As leaders, we cannot tackle it all, but changing our workplace culture can positively influence societal norms. When our employees are equipped to recognise and call out inappropriate behaviour in the workplace, they may be inspired to tackle it outside of their work environment. For example, they may start to reflect on how internalised misogyny impacts their perceptions, behaviours and tolerances in everyday life, or they may start to call out victim-blaming rhetoric at social gatherings or online. No matter how small your organisation or department, your efforts may have a greater impact than you realise.
The Way Forward: A Framework for Cultural Change and Workplace Accountability
We are experiencing an epoch-changing period of time. Global movements including #MeToo, #LetHerSpeak, #TimesUp, #BalanceTonPorc, #NotYourHabibti, #Teknisktfel, #QuellaVoltaChe and #YoTambien have revealed the prevalence and destructive impact of sexual abuse and gender inequality. For the most part, people are more attuned to the need for a safe and harassment-free workplace, and more willing to have tough conversations and commit to change. We can leverage the current climate to build momentum and proactively create a safer industry for the next generation of female doctors. As leaders we can say, ‘This ends with me’.
Instead of waiting for a complaint to be made, we need to address the systemic drivers of sexual harassment and stop it from occurring in the first place. When a complaint is made, we need to lead with empathy and take decisive action.
Establishing a Foundation for Change
Workplace culture strongly affects your organisation’s ability to achieve its strategic goals, which is why creating a respectful environment should be a defined part of your organisation’s strategy. When you spend time getting the fundamentals right, you lay the foundation for long-lasting and meaningful change. Start by providing direction, setting expectations and establishing accountability for results. Your employees need to know that eradicating sexual harm is a leadership priority.
Draw a Line in the Sand
Setting clear expectations is critical. Employees need to understand exactly what’s expected of them in a non-dictatorial and collaborative way to empower and inspire positive action.
Start by drawing a line in the sand. Make a strong statement that says, ‘From this point on, we will no longer tolerate inappropriate behaviour in our workplace’. If your organisation has failed to take action in the past, acknowledge your shortcomings, apologise and commit to stronger leadership. When you show vulnerability as a leader, you invite people to become more involved in the change process and more invested in the outcome.
If your organisation can manage the impact on operations, invite staff to in-person or hybrid events where you clearly outline the way forward for your organisation and encourage them to share their views and ask questions. While the events need to acknowledge where things have gone wrong in the past, the overall tone should be positive and aspirational – a chance for everyone to work together to create an industry-leading workplace that sets the standard in staff wellbeing and health care excellence.
Communicate the Why
Once the commitment is clear, help employees understand why the change is so vital and what success looks like. Paint a picture of the future state where all employees feel safe, respected and motivated to achieve their career aspirations and improve patient outcomes. Align the objectives to your organisational vision, mission and values as well as your employees’ job responsibilities. Everyone needs to understand that sexual harm is a workplace health and safety issue and will be treated accordingly.
If decades in the health sector have taught us anything, it’s that clinicians genuinely care about improving the health outcomes of their patients. When employees understand how sexual abuse impacts productivity, innovation and patient safety, they will be more motivated to lead change.
Bring Your Organisational Values to Life
A lot of health care organisations profess to be ‘values-driven’, but what does that mean? Your values need to be more than words that appear on your website and in your staff orientation pack.
If one of your values is ‘accountability’, what does that look like on a daily basis? How do your staff live that value in the way that they conduct themselves? Instead of telling your people what you think accountability looks like, ask them to develop a specific list of behaviours and scenarios that demonstrate accountability. By inviting open conversations and co-designing expected behaviours with your employees, they evolve from spectators to invested partners in the change process.
Develop Clear and Concise Policies
There can be a tendency to make policies long and complex to avoid legal ambiguity, but this can deter impacted people from making a formal complaint. Your policies and procedures need to be clear, concise and easily accessible, including a standalone policy on sexual harassment. (3)
Your sexual harassment policy should include your organisation’s zero-tolerance commitment, information on how to recognise inappropriate behaviour, a clear reporting procedure, and information on available support networks. Sexual harassment should also be referenced in your code of conduct, employment contracts, sub-contractor agreements and performance management frameworks.
The focus should be on integrating these policies and procedures into ‘business as usual’, so that expected behaviours become the norm and there is no need for leadership to rule with an iron fist. In order for this to happen, everyone needs to be engaged in the process, including the board of directors, executive team, managers, clinicians and frontline staff.
Align HR Processes
Your human resources department will often be the first point of contact for people impacted by inappropriate behaviour. The team needs to handle every report with diligence and empathy. Often in health care, the timelines are stretched out due to staff rosters which can place undue stress on the complainant at an incredibly vulnerable time. Impacted people need to know that they will be taken seriously and their complaint will be investigated quickly and thoroughly.
Recruitment processes also need to align to your zero-tolerance approach. In health care, we want highly skilled clinicians who can provide excellent patient care, but we also need to hire people whose values and behaviours align with our desired culture. When you hire or promote the arrogant misogynist with a reputation for disrespecting and bullying his registrars, you are sending a message to your employees that your commitment to creating a respectful workplace is conditional. Alternatively, when behaviour is a key driver in your recruitment and dismissal process, you create a peer-driven environment and ‘power with’ culture where your people set the high standards on your behalf.
Recruit a Team of Advocates
Catalysing cultural change requires you to capture the hearts and minds of your employees. One of the most effective ways to achieve that is to recruit advocates at all levels of your organisation. This ensures the change is not just seen as flowing from the top down but avidly supported and driven from within.
Your advocates or ‘change champions’ should represent various departments and include a diverse mix of front line, mid-level and senior employees who are trusted and respected by their peers. Ideally, you want a team who are approachable, influential, positive and known for leading by example.
Managers should gather their team of change champions to explain the importance of their role, define expectations and provide them with tools to support their success including key messages and communication tips. These empowered advocates can ensure staff understand your organisation’s expectations and complaints procedure while encouraging staff to participate in surveys and provide ongoing feedback.
Set Measures for Success
A clear set of metrics will help measure your progress and provide valuable insights into your workplace culture. The leadership team should regularly assess and report the number and severity of formal complaints while acknowledging that an increase in reporting may not indicate an increase in sexual harassment but rather an increase in impacted people feeling comfortable enough to report it.
It’s also important to monitor the informal reports that are being managed within various departments where the impacted person does not wish to make a formal complaint. While every organisation is different, other recommended tools include annual staff surveys, pulse or spot surveys, and exit interview feedback.
Demonstrate Your Ongoing Commitment to a Safe, Respectful and Inclusive Workplace
Creating a safe and respectful workplace is not something leaders can tick off as a completed project. It is an ongoing process that requires focused effort, consistency and flexibility across all departments and levels of your organisation. Once you’ve established the foundations for change, your actions and analysis need to maintain momentum. As with any framework or strategy, it’s important to keep listening to impacted people, to keep assessing what’s working and what could improve, and to stay nimble and humble enough to make changes where necessary.
Listen to and Support Impacted People
Your employees will not speak up unless they feel safe doing so. Your organisation needs to provide people with a clear and confidential pathway for accessing comprehensive advice and support. Any issues that arise should be handled quickly by people who are trained to deal with trauma and can handle difficult conversations with empathy and without jumping to conclusions.
Impacted people need to be involved in the decision-making process and given options for handling the issue either informally or via the formal complaints process. From the moment a complaint is made through the resolution process and beyond, impacted people should remain informed and supported with access to both internal and external support networks to maintain their physical and psychological health.
Intervene Early to Avoid Escalation
Not every complaint needs to escalate and become formal. Responses need to be tailored to the severity of the actions and the desired outcome of the complainant. Many impacted people just want to be heard and for the inappropriate behaviour to stop. Their preferred result would be for the perpetrator to understand what they did wrong, apologise and commit to rectifying their behaviour moving forward.
By intervening early, you can avoid the situation escalating and the behaviour becoming more severe. Whether you follow an informal or formal pathway to achieve the desired outcome, the focus should be on instilling trust in your procedures and meeting the needs of the impacted person.
Understand the Power of Microcultures
People’s beliefs and behaviours are the result of various factors, including their culture, religion, life experiences and relationship dynamics. You need to understand the biases and unconscious biases as well as the cultural and societal factors at play. While you are striving to create an organisation-wide culture, within that there will be a diverse set of microcultures that can support or hinder your progress.
Sometimes microcultures bring a positive ethos and energy to your workplace, whereby people are natural leaders who inspire fairness, equality, collaboration and inclusion. In other instances, the microcultures can result in patriarchal attitudes that create a gender power imbalance and hostile work environment undermining your efforts to achieve equality. In a microculture of toxic masculinity, sexual harassment may be dismissed as ‘just a bit of fun’ or ‘banter’ and your efforts to eradicate it will be viewed as excessive and elicit strong resistance.
Encourage your leadership team to listen to the lived experiences of your employees so that any detrimental beliefs or behaviours can be openly discussed and challenged. Your employees may not realise that the attitudes and behaviours they have grown up with and become accustomed to may be harming those around them.
Be Prepared for Challenging Behaviour
Even your most values-aligned employees will not get it right all the time, neither will you or your leadership team. When people are stressed, they fall back to poor behaviour, and when people are used to walking past inappropriate behaviour, it takes concerted effort and courage to stop and start speaking up.
Good leadership is about encouraging your employees to reflect on how their actions are affecting others, including their colleagues and patients. In a fast-paced health care environment, this can be tough, but mindfulness and reflection are fundamental parts of long-term behavioural change. You can encourage reflection by sharing your own personal experiences with your team. Where have you fallen short in the past? What did you let slide so as not to rock the boat? How did you learn to change your approach and why? Sharing personal stories is a way to connect and alter behaviours without coming across as evangelical or dictatorial.
View Sexual Harms through the Gender Equality Lens
Achieving gender equality is a key goal in the prevention of sexual harassment against women. As you work towards eradicating sexual harms, you need to create a culture that is inclusive of all genders and has diverse representation at all levels.
In the health care industry, women are still underrepresented in leadership positions, creating unequal gender power dynamics. Organisations need to proactively address the gender pay gap, create a strong pipeline of women advancing into senior roles and introduce flexible working arrangements for parents to encourage women to return to the workforce and progress up the ranks after having children.
Inspire Leadership at All Levels
Eradicating sexual misconduct needs to be a priority across all levels of the organisation, including the board of directors, executive team, senior leaders, and administrative and clinical staff. The board and executive team need to set the tone and lead the charge, not because it’s mandated but because it’s the right thing to do. The message should be clear, ‘If you abuse or harass others, there is no place for you in our organisation no matter what your credentials are.’
Accountability cannot exist without transparency. The board needs to receive regular reports on any formal or informal reports of sexual harassment, and all staff should be informed on progress, including openly discussing staff survey results and areas in need of improvement.
The executive team and senior managers must show a united front and back up statements with daily actions. During team huddles or meetings, celebrate the cultural wins and openly discuss what needs to be improved. Every member of staff needs to be empowered and energised to create a safe and respectful environment. They need to be reminded that when they fail to act against sexual misconduct, they become part of the culture that enables it.
Be Prepared for Resistance
Every time you make an organisational change, even when it’s for the global good, you’ll encounter employee resistance. Sexual harassment is a very complex and sensitive subject that can and will evoke strong opinions and reactions. Your employees will need to examine their beliefs and behaviours, which can be confronting and uncomfortable. For impacted people, the process may uncover distressing memories or activate a trauma response. You need to be prepared for criticism, pushback and heightened emotions.
Some people will have a vested interest in maintaining the status quo and will simply refuse to adapt. Your job is to help people understand how the change benefits them and their patients. Keep clarifying expectations, communicating the why, and offering training and support as needed. When people start to see and feel the benefits of a more respectful ‘power with’ culture, their resistance to the change should dissipate. If it doesn’t, you need to help them see that your organisation is not a ‘values fit’ and therefore not the right environment for them.
Don’t Throw in the Towel
With every change project there will always be a moment when it looks like it’s failing. You’ll likely feel that all your efforts have been for nought and the challenges are just too big and insurmountable. In those moments, the desire to pull back and focus on something else is strong. Don’t. Once you’ve chosen to go down a particular path, you have to keep going. Changing your organisational culture is extremely difficult but it’s usually at that moment, when it all feels too hard, that you’re about to start making real progress.
If you’re doing something that is driven by strong values and principles, you have to keep pushing though the barriers because your employees and patients deserve to experience all that’s on the other side – a safe, inclusive and respectful workplace that continually evolves and innovates to improve the health outcomes of the community.
| Established in 1996, Dental Health Services Victoria (DHSV), now Oral Health Victoria, is responsible for delivering public oral health services in Victoria, a state in Australia. Accountable to the Victorian Minister for Health and funded by the state’s Department of Health, the agency provides emergency and general oral health care at the Royal Dental Hospital of Melbourne and purchases oral health services for public patients from over fifty not-for-profit community dental agencies across the state. |
| In 2016, DHSV launched a new five-year strategic plan for improving Victorians’ access to high-quality, equitable dental care. The plan included four strategic themes: 1) improve health outcomes for patients; 2) improve the experience of care for both patients and providers; 3) be global leaders with local partners; and 4) be a great place to work and a great organisation to work with. The board and executive team decided that the best way to achieve the strategy was to use the principles of value-based health care. Value in health care is defined as ‘the measured improvement in a person’s health outcomes for the cost of that improvement’. (Reference Teisberg, Wallace and O’Hara4) |
| Before launching new models of oral health care, DHSV CEO Dr Deborah Cole wanted to focus on it becoming a great place to work. The Victorian Auditor-General’s Office (VAGO) had recently released a report titled ‘Bullying and harassment in the health sector’ in response to several public instances of this behaviour at VAGO and other sites. The report concluded that health sector agencies lacked the leadership, policies, procedures, and staff training needed to recognise the impact of harassment and bullying ‘even when such issues resulted in significant media attention and reputational damage’. (5) |
| The DHSV leadership team facilitated discussions with staff about the organisation’s existing values, or the ‘DHSV Way’, and solicited input on standards of conduct. These conversations exposed different interpretations of ‘acceptable behaviours’ among individuals and particularly across teams. In response, the leadership team created a new code of conduct to clearly define ‘above the line’ (acceptable) behaviours and ‘below the line’ (unacceptable) behaviours. |
| Following discussions with the staff, DHSV introduced its Respectful Workplace Framework, which had six dimensions: equity, diversity, inclusion, flexibility, wellbeing, and safety. Leadership then developed a Respectful Workplace Action Plan for implementing the framework. Actions focused on ensuring staff understood both the reasons for change and their responsibility for aligning organisational systems and processes to support it. The plan also established a network of peer advocates called the Wellbeing Contact Officer Network. These staff provided a point of contact for information and mediation services for colleagues experiencing inappropriate workplace behaviour. |
| In December 2016, DHSV wrote a formal statement titled ‘Joint position statement against bullying, harassment and inappropriate behaviour’ and signed it with multiple academic partners and professional associations. The statement promised to uphold the rights of all to have a safe, inclusive, and respectful workplace and to speak up against and remove bullying and harassment from the dental profession. |
| After the signing, DHSV hosted a mandatory Respectful Workplace Learning Day for DHSV staff. The learning day introduced the revised ‘DHSV Way’ values and behaviours, provided the reasoning for the Respectful Workplace Framework, and outlined the consequences for inappropriate behaviours. The message from leadership was clear – ‘Here is the line in the sand. From this time forward, if you act against the values you will not get away with it.’ |
| The change presented multiple challenges. The CEO was labelled by some as a ‘man-hater’, ‘misandrist’ and ‘part of the woke brigade’. Some staff did not agree with the new standards of conduct and chose to leave the organisation. Those who pushed back were in the minority, and the DHSV leadership team stayed the course. |
| Over the next year, the organisation fielded numerous complaints about bullying, harassment, and other inappropriate behaviour. Staff felt they had been given permission to speak up and take a stand against inappropriate behaviour. They had the tools and support to do so and the confidence that management would support them. (Note: In July 2025, DHSV changed its name to Oral Health Victoria) |
| In America, Title IX is a statute that prohibits sex discrimination in education programs and requires universities to ‘adopt and publish grievance procedures providing for prompt and equitable resolution of student and employee complaints’. (6) Under Title IX, universities must ensure that someone who experiences sexual violence is cared for and given access to support services. |
| During a particular university assessment process, two students separately reported to Elizabeth and a teaching colleague that they had been raped at different university campuses many years prior. These admissions instantly triggered Title IX despite the rape allegations occurring outside of the statute of limitations – a specified window of time that a state has to charge the perpetrator. |
| Elizabeth and her teaching colleague were in unchartered territory having never dealt with a rape allegation before. While they felt daunted and overwhelmed, they were determined to follow the correct process and ensure that the students felt supported, heard and respected. |
| Elizabeth and her colleague immediately sought the assistance and guidance of the university’s HR department. They had clear and robust policies and procedures in place and provided advice and support throughout the process. |
| As per the university procedure, the students were approached in an empathetic and respectful manner. The focus was on delivering the outcome that the students wanted, which was ultimately to get advice. The students said they finally felt heard and appreciated the opportunity to share their story. The process gave the students a sense of closure and gave Elizabeth and her colleague confidence in the university’s values, policies and procedures. |
Conclusion
People are fundamentally good. Decades in the health care industry have shown us the absolute best in humanity. As health care leaders and educators, there is no greater honour than witnessing the outstanding dedication demonstrated by doctors, nurses and their support staff every single day.
People work in health care because they want to help people achieve and maintain optimum health. When you create a workplace free from sexual harm, you give them the best chance of fulfilling that goal. We all have a responsibility to ensure that the environment we operate within is physically and psychologically safe. When unprofessional and inappropriate behaviour is allowed to flourish, we don’t just fail one another, we fail in our duty of care to our patients and the broader community. When we create a safe, respectful and inclusive environment, everyone wins. People are empowered to innovate and find new ways to deliver high-value care. They work collaboratively to introduce the reforms our industry so desperately needs. They are able to thrive as leaders in their field, knowing that their organisation can be trusted to do the right thing when it matters most.
Introduction
Advocacy is a broad term, arising from the Latin word ‘advocare’ meaning ‘coming to the aid of someone’. (Reference Reid1) Implied in this definition is the concept of lending one’s own power to the cause of another. The power to direct the goals of any advocacy effort should remain with the individual or group that will benefit from the advocacy campaign. Advocacy can be misdirected if the voices of the individuals for whom advocacy is sought do not speak, or are not sufficiently heard. (Reference Engelhardt, Kopelman and Moskop2)
There are numerous models of advocacy, many tailored to specific causes. However, in some cases, political lobbying is presented as advocacy for a particular group. The United Nations highlights this concern, referring to it as ‘greenwashing’. Originally, this term described marketing practices used by companies claiming environmental responsibility to enhance their brand appeal. However, it also applies to governments and other organisations that mask ineffective policy decisions with advocacy language. (3) The United Nations calls for transparency, accountability and integrity – principles that should form the foundation of any advocacy programme.
At its core, advocacy is about persuasion. It requires understanding how the system sustaining the problem operates, identifying who within it must change to shift the system towards a more positive direction, determining how this shift can be achieved, and involving the necessary stakeholders to make it happen. In the end, advocacy is a complex process with multiple moving parts.
Advocacy must be contextually relevant to truly meet the needs of the people it claims to support. This book seeks to underscore the importance of context, showing how various disciplines, countries, and perspectives shape and inform pathways to change. Advocacy can take place on multiple levels: from individuals learning to advocate for their own rights, to representative groups, organisational bodies, national leadership, and international organisations, including but not limited to the United Nations and its initiatives around the Sustainable Development Goals, such as gender equality. It is also important to recognise the roles of numerous non-governmental and humanitarian organisations that represent, protect, and assist populations facing conditions of vulnerability, exclusion, or disenfranchisement. These organisations often mediate between these populations and both governmental and non-governmental powerholders. (Reference Almog-Bar and Schmid4)
The Advocacy Process
In their synthesis of the literature, Farrer et al. describe six key dimensions of effective advocacy, which we use here as a framework for this text. (Reference Farrer, Marinetti, Cavaco and Costongs5) To bring these elements to life, we have invited advocates contributing to this book to share their advocacy journeys, drawing on their personal experience to illustrate important principles and practices.
Dimension 1: The Kinds of Evidence Needed to Advocate
When we present this work, we often face a series of questions. Over time, we have come to recognise these recurring questions as attempts to reconcile the gap between people’s perceptions and the realities we are addressing. Common questions include:
Is this problem real, and if so, how significant is it?
If it is real, is it relevant to me?
If it is relevant to me, is it truly my problem or someone else’s responsibility or fault?
For audiences to engage with our message meaningfully, they first need to believe in our credibility as advocates and in the reliability of the data we present. This credibility is crucial in overcoming the cognitive dissonance that often arises when considering the occurrence of sexual harassment within their own contexts and under their watch.
This book aims to synthesise different types of evidence to create a series of compelling arguments for change. The editors recognise that advocacy involves engaging with different audiences, each of whom may respond differently to the types of evidence presented. One significant barrier in addressing sexual harassment is the scarcity of robust quantitative data that demonstrates prevalence. Gathering accurate data on such a sensitive issue, marked by shame, stigma, and invisibility, is challenging, yet it is essential to substantiate calls for change. For governments and policy makers, one area of interest is assessing the costs and benefits of policy action and inaction, (Reference Petticrew, Whitehead, Macintyre, Graham and Egan6; Reference Nutbeam and Boxall7) which in this field may include quantitative estimates related to workforce attrition, absenteeism or patient outcomes (see chapter 7). Such data answers whether the problem is ‘real’ and significant. Furthermore, it strengthens our credibility as advocates and reinforces the legitimacy of our message.
It is equally crucial to consider how these data-driven narratives can be communicated and enriched. (Reference Marmot, Friel, Bell, Houweling and Taylor8) This is particularly challenging when the data contradicts long-held opinions among advocacy audiences. Relying solely on quantitative data is often insufficient to drive engagement, as there will never be ‘enough’ evidence to satisfy everyone, and the data is likely to be criticised as ‘weak’. (Reference Farrer, Marinetti, Cavaco and Costongs5) In medicine, which values scientific rigour, there is a tendency to privilege precise data – yet ‘accuracy’ can be difficult to achieve when measuring complex social phenomena like sexual harassment. Hence, the tendency to endlessly debate prevalence statistics.
Quantitative data is most impactful when enriched with personal stories. Brief stories or ‘cameos’ can vividly illustrate specific situations or interventions to stakeholders. (Reference Priest, Waters, Valentine, Armstrong, Friel, Prasad and Solar9) Well-chosen and skilfully communicated stories can effectively challenge people’s tendency to dismiss the data, helping to address questions around whether the problem is real, relevant to them, and whether they bear some responsibility for addressing it. Narratives of lived experience counteract dismissive attitudes that label survivors as ‘overly sensitive’ or frame perpetrators as merely ‘bad apples’ whose behaviour can be managed individually rather than systemically.
However the data story is conveyed, it should be locally relevant and summarised for policy makers in a digestible format – often as a ‘one-pager’. (Reference Izumi, Schulz, Israel, Reyes, Martin and Lichtenstein10) Creating a clear, one-page narrative for change is an essential tool not only to communicate findings and recommendations, but also to focus the team on obtaining the right data to anchor key messages. This also keeps messaging consistent, ensuring that the various people and agencies working to create change remain aligned and goal-focused.
Good communication requires people with the right skills and tools, able to convey data clearly and meaningfully, avoiding unnecessary complexity and ensuring that the audience understands the message. This often involves difficult but necessary discussions about what constitutes effective data. For instance, while policymakers may be more persuaded by economic arguments that highlight the financial burden sexual harassment places on hospitals, survivors on the team may feel uncomfortable about reducing their experiences to cost figures or data points on a page. Given there are likely to be multiple stakeholders in any meeting or presentation, it is often a challenge to determine which arguments to present, and the timing of each.
In Table 33.1, Dabota Yvonne Buowari describes her work gathering evidence in Nigeria and other countries in Africa to drive change. She illustrates the importance of community-based participatory research, a particularly effective method in advocacy programmes. (Reference Hawe and Shiell11–Reference Davis, Lindberg, Cross, Lowe, Gunn and Dillon14) This approach empowers local participants through active involvement in the research process, enabling them to translate findings within their communities and ensuring the data genuinely reflects local experiences. (Reference Ingram, Sabo, Gomez, Piper, de Zapien and Reinschmidt12; Reference Stack and McDonald15)
| My experience as an advocate of sexual harassment (Dabota Yvonne Buowari) |
| Advocacy involves creating awareness. In my case, it focused on the problem of sexual harassment, especially as it is affected by culture and traditional beliefs in some regions of the world. I am an African and a victim of sexual harassment in the medical workplace. That is why I developed an interest in the topic. Several strategies can be taken by stakeholders in the health sector to bring sexual harassment in the medical workplace to an end. Such strategies can also be taken by stakeholders in every place where there is the probability of sexual harassment occurring and even sexual assault and rape. These include workplaces and educational institutions. Anywhere there is an employer–employee, boss–subordinate, master–servant, supervisor–supervisee, and the teacher–student relationship. There is a need to create awareness as there are usually power dynamics when sexual harassment occurs. Working in a developing country I did not have the privileges of a formal reporting system. |
| First, I conducted a survey on sexual harassment in the workplace among participants at the Medical Women’s International Association (MWIA) session at the United Nations (UN) Commission on the Status of Women (CSW). The results of this study were presented at the triennial congress of the MWIA which took place in Vienna, Austria. This sparked the interest of the then-president of the MWIA on sexual harassment. A study was conducted on sexual harassment, and the research team was made up of four members which included me. |
| The study consisted of qualitative and quantitative aspects. Thirty respondents, who gave their consent, were interviewed. The results of this study have been presented at various fora to create awareness of sexual harassment. These include the MWIA triennial congress in New York; Medical Women’s Association of Nigeria (MWAN) biennial conferences in Abuja and Asaba, Delta State, Nigeria; and the MWIA Near East and Africa regional conference in 2018 that took place in Nairobi, Kenya. |
| I have also authored some articles on sexual harassment in the medical workplace. I have continued to be an advocate of sexual harassment irrespective of any intimidation and lack of support. I do not have any support because of the society where I live and work. However, I am not discouraged. I will always be an advocate for the elimination of sexual harassment, especially among women doctors. |
In their work on sexual harassment, the editors of this book have discovered that trends are often more readily accepted than individual statistics. Therefore, we often present simplified graphs that illustrate findings across multiple studies in diverse contexts, acknowledging that each study may have its own methodological limitations. This approach mitigates the tendency of stakeholders to sidestep the issue by focusing on the methodological flaws of individual prevalence studies. As we often say, knowing that prevalence is well above zero should be sufficient data to ground our advocacy work.
The team from ‘Surviving in Scrubs’ discusses in chapter 35 how they have gathered and communicated lived experience narratives to advocate for change. One common issue they highlight is the importance of having clear reporting pathways for survivors. It is essential that the person or organisation receiving and managing the report is independent enough to assure the survivor that their report will be heard objectively and without impact on their future career. While providing options for survivors is important, there must also be transparency, so they are fully informed about what will happen next, the boundaries of confidentiality, potential costs (including time), and possible outcomes. Holding organisations accountable for their processes and outcomes is one way advocates can help survivors be heard and appropriately supported. Analysing and communicating gaps in these processes requires in-depth policy analysis, ideally presented as a diagram accompanied by a story that illustrates the real-life impact of these gaps on survivors. Although constructing these visual narratives can be complex, they provide a focused pathway for driving change.
Lived experience narratives are powerful tools to persuade and inspire change, especially when survivors share their stories themselves. However, presenting these stories requires a trauma-informed approach to avoid retraumatising survivors who may be in the audience. One effective way to handle this is by providing these narratives as supplementary material, allowing participants to engage with the content on their own terms. The goal is to empower survivors to own their stories while protecting them from potential exploitation, a frequent concern for survivors of sexual harm when engaging with media.
Ideally, a policy argument combines multiple forms of evidence. Whitehead et al. recommend advocacy organisations present a ‘jigsaw of evidence’, which is ‘not one single piece of evidence, but rather many different bits, of varying quality, creatively pieced together’. (Reference Whitehead, Petticrew, Graham, Macintyre, Bambra and Egan16) This collection of varied pieces, each with different strengths, can be assembled to form a comprehensive argument. In Table 33.2, Dabota Yvonne Buowari discusses her approach for creating change in Nigeria.
| It is important to create a system that is safe for anyone to report the incident. These reporting channels should be easy to access and safe for victims. It should be free from any form of discrimination, intimidation and stigmatisation. This is a challenge in countries with high levels of corruption and patriarchal societies. In some contexts, a victim’s report may not be acted upon without the payment of a bribe. In patriarchal societies, victims – particularly women and girls – are often not taken seriously, as decision-making is male-dominated and discrimination persists. As a result, reports from survivors may be disregarded, and female victims are frequently sidelined. |
| Policies are important to define situations, processes, and protocols. They also outline punishments for offenders. It is important that there are policies against sexual harassment at various levels of government, in health facilities, educational institutions and other workplaces. Such policies can also be included in the constitution of a country, state, county, province or constituency and should also be enshrined in the legislature. Legal support should be provided for victims, to allay anxiety, ensure safety, give confidence and provide encouragement to other victims to speak out and not keep quiet. |
| Stigmatization is one of the barriers and obstacles to sexual harassment advocacy and awareness campaigns. Intimidation and stigmatization deters victims from giving testimonies in court and becoming advocates against sexual harassment. Sexual harassment activists need to have meetings with the authorities and educational institutions to engage and remind them about any existing policies, including penalties and disciplinary action to be taken against perpetrators and also provide psychological care for victims. Advocates can help protect against the mental health impact of sexual harassment on the victims. All victims and survivors of sexual harassment should be encouraged and supported to be advocates and ambassadors for the reduction and elimination of sexual harassment. |
Dimension 2: Who Advocates for Change and Who Should Hear their Message?
Every stakeholder has the potential to be either an advocate or a target of advocacy, making it essential to map the field at the outset. Working in teams allows communication to be managed by the best-suited team member for a given situation and context. (Reference Farrer, Marinetti, Cavaco and Costongs5) Ideally, the advocacy team should include representatives from the organisations and individuals who will be integral to enacting change. Farrer et al. suggest each stakeholder should be considered with the following questions: (Reference Farrer, Marinetti, Cavaco and Costongs5)
who has the power to effect change?
who is most vulnerable to pressure?
who holds the power that is necessary to change the system?
who is an ally?
who is likely to actively oppose efforts?
This mapping process is invaluable for crafting narratives tailored to specific audiences. It is equally important to map the team involved in advocacy work. In chapter 14, we discussed VeneKlasen’s four types of power. (Reference VeneKlasen and VeneKlasen17) Understanding the sources of power within the team – including their formal, institutional roles (‘power over’), their social capital and potential for collective action (‘power with’), their individual capacities (‘power to’) and own self-knowledge, sense of agency and personal qualities (‘power within’) – can help leverage team strengths effectively.
Betty Yeoh Siew Peng, an advocate for women’s rights in Malaysia, reflects on the principles that guide her activism. She describes how she developed these principles through her personal and professional life and through her work with a range of groups, from grassroots movements and unions to dedicated advocacy organisations.
| The advocacy I’ve been working on for the last twenty years is the draft Anti-Sexual Harassment legislation. I hope that by sharing glimpses of my advocacy journey, I can inspire and enable others to support those in the fields they choose to advocate for. My mother is the matriarch in the family. She made me and my siblings do home chores. How does this connect to advocacy work? It can be said these home chores disciplined us from a young age. We became responsible and accountable to ourselves while also sharing the responsibilities of the family. Similarly, when we advocate for an issue, we must ensure that our actions align with our words and set an example through our behavior. For instance, if we call for anti-sexual harassment legislation, we cannot be sexually harassing others, be it our friends or colleagues. |
| In my younger days, due to financial constraints, I did not get a tertiary education, but my work provided me with valuable lessons. I learnt to be resourceful as I followed the good advice from my mother, that is be willing to learn from work given to me. My first formal job was with an oil and gas company. The employees were union members of the Chemical Workers Union of Malaya (CWUM). They were picketing due to a breakdown in negotiation of their collective agreement with the management. The union members were mostly production workers who did not have high education. By the time I joined the union, I was able to contribute to the worksite team because as the saying goes, ‘In the Kingdom of the Blind, the Man with One Eye is King’. With my basic education, equivalent to a General Certificate, I was slightly better educated and able to help the union worksite team compare our collective agreement (CA) with those of similar industries. |
| It was essentially research work, helping to design the best terms of service to include in our collective agreement, which the Union then had to ‘bargain’ with the company. Successful negotiations often led to better remunerations and terms/benefits for the members. This was the start of my activism, as a I learnt the importance of working in a team. Research, such as surveys and studies, is important when it comes to making change or advocating for change. |
Dimension 3: Advocacy Messages
There are core narrative arcs frequently used in advocacy. While not universal, these familiar narratives offer stakeholders a recognisable structure. In medicine, audiences often expect a certain format – such as a literature review, method, results, and discussion. Changing this narrative arc demands greater cognitive effort work for the audience, so it is essential to structure the story carefully and logically.
Common advocacy narratives are often built around themes such as:
Values and social justice
Human rights
Legal obligations
Economics
Self-interest (e.g. reputation as an employer of choice)
The chosen narrative, mode of communication, and presenters may vary considerably and should be selected thoughtfully. Presenters and participants bring different forms of influence, whether it is the authenticity of survivors, the authority of senior colleagues, or the enthusiasm of medical students. For example, Surviving in Scrubs shares stories, including anonymous ones, to help other survivors find language and voice to address their own trauma. (Reference Cox and Jewitt18) The Time’s Up movement in the US emphasised collecting defensible data on workplace harassment – an essential advocacy tool for organisations. (Reference Chawla, Gabriel, O’Leary Kelly and Rosen19) In contexts like hospitals, one of the most compelling narratives to engage health care professionals in addressing harassment is its direct impact on patient outcomes and the overall quality of care. Harassment not only harms individuals but also disrupts teamwork, communication, and morale within medical teams, ultimately affecting patients. The CanMEDS framework emphasises advocacy as a core competency for physicians, encouraging them to ‘respond to the needs of the communities or populations they serve by advocating with them for system-level change in a socially accountable manner’. (Reference Poulton and Rose20) In this context, addressing harassment is not only about creating a respectful workplace but also about fulfilling a professional duty to advocate for safe, high-quality patient care.
An important aspect of delivering advocacy messages is not just the content, but the tone. It is our experience that presenters need to ‘calibrate outrage’ – while outrage can be mobilising, it can also cause audiences to disengage. There have been moments in the narratives around sexual harassment in medicine that have used shocking content to draw attention. For example, the initial push to address this type of harassment in Australia involved a female surgeon, Dr Gabrielle McMullin, sharing a case where a registrar was propositioned by her supervisor. After recounting the case, Dr McMullin remarked, ‘Her career was ruined by this one guy asking for sex on this night. Realistically she would have been better to have given him a blowjob on that night and to have left it at that.’ (Reference Newlands, Cuming and Jackson21) Predictably, this statement divided the surgical community, but it ultimately led to significant change, including the ‘Operating with Respect’ campaign. (Reference Tobin and Truskett22) This narrative was effective because Dr McMullin used her status as a senior surgeon to deliver a powerful message to the right audience at the right time.
Louise Stone recalls meeting a senior bureaucrat to request research funding to explore the experiences of international medical graduates in Australia. The bureaucrat responded, ‘Well, I’m prepared to read a proposal as long it doesn’t take a victim mindset with more whining women’. In situations like these, the tone must be highly objective and data-based. We have found that it is crucial to keep the message within ‘the zone of proximal development’ – challenging enough to stretch the audience’s thinking, but not so confronting that it causes them to disengage.
Dimension 4: Tailoring Arguments to Different Political Standpoints
Advocacy messages must be tailored to the audience, which requires understanding where the advocate’s goals align with the organisation they are addressing. This includes recognising and addressing unhelpful narratives, such as the idea that a perpetrator is merely a ‘bad apple’ and the target of harassment needs to build resilience because they are ‘over sensitive’. (Reference Searle, Rice and McConnell23) These misconceptions often need to be confronted directly.
A common issue is the belief that sexual harassment and its management are individual rather than collective responsibilities. People vary in the extent to which they attribute responsibility to individuals versus systems, as seen in health care debates. For instance, in the United States, right-wing groups are more likely to hold individuals accountable for their own behaviour and social standing, (Reference Farrer, Marinetti, Cavaco and Costongs5) while those with left-wing views are more likely to attribute issues to inequitable social and economic systems. (Reference Knight24) Depending on the audience, advocacy narratives should be shaped in a way that ensures that organisations do not evade their obligations by placing responsibility solely on survivors.
The Working Party on Sexual Misconduct in Surgery was formed in the UK in 2022 and published their groundbreaking paper titled ‘Sexual harassment, sexual assault and rape by colleagues in the surgical workplace and how women and men are dealing with different realities’. (Reference Begeny, Arshad, Cuming, Dhariwal, Fisher and Franklin25) It has been insightful to observe this team develop an advocacy strategy using a combination of research, workshops and publications. (Reference Newlands, Jackson and Cuming26) One of their effective strategies involved working with, rather than opposing, the Royal College of Surgeons of England, beginning their advocacy with a scientific paper – a strategic choice that resonates with doctors who prioritise evidence-based approaches. Their report integrates diverse forms of evidence, with lived-experience quotes, research outcomes, evidence of organisational support and a solution-focused series of recommendations, all presented in a concise and impactful manner. (Reference Newlands, Cuming and Jackson21)
Dimension 5: Barriers Impeding Effective Advocacy in Medicine.
There are a several ingrained social assumptions about the medical profession that make it difficult for many to accept that sexual harassment is a significant issue. Hospitals are often seen as safe, controlled environments, and people may find it hard to accept that sexual harassment occurs in these settings and that doctors – typically viewed as dedicated professionals – can be perpetrators. Additionally, doctors are generally seen as privileged and therefore immune to risks of sexual harassment or abuse.
Medicine is a conservative field, characterised by lengthy training periods and steep hierarchies. Those at the top of these hierarchies may be reluctant to change, as they hold privileged positions with considerable power. Beyond individual resistance, broader societal barriers also impede progress. The current political and economic climate emphasises individualism and neoliberal values, both of which create obstacles to systemic reform. Short-term political cycles and the high-output, low-investment model of many academic institutions further delay necessary changes.
Both medicine and contemporary society have deeply entrenched, gendered cultural norms that create barriers to addressing harassment and promoting effective advocacy. Dominant gender norms shape social and professional hierarchies, reinforcing power dynamics that protect the status quo. (Reference Connell and Messerschmidt27) Additionally, the high prevalence of childhood trauma and gender-based violence can normalise harassment, making it harder to address these issues in adulthood. (Reference Anda, Felitti, Bremner, Walker, Whitfield, Perry and Giles28)
Biomedical training and research approaches often do not incorporate or prioritise social science perspectives, which can hinder the profession’s ability to respond effectively to complex issues like harassment. Furthermore, with multiple actors operating in this space, each with differing priorities and goals, aligning advocacy efforts requires significant coordination and collaboration.
Despite these barriers, there are promising developments at both the national and global levels. States and multilateral organisations are increasingly committed to advancing Sustainable Development Goals (SDGs) that focus on gender equality, safe work environments, and accountability.
In the health care sector, specific initiatives address the protection of doctors from harassment by colleagues. For instance, the International Labour Organization (ILO) adopted the Violence and Harassment Convention (C190) in 2019, which applies to all sectors, including health care. This landmark convention establishes the right to a workplace free from violence and harassment, emphasising employer accountability and preventive measures. (29) As of the end of 2024, forty-five countries had ratified the Convention, though its impact will only become evident once it is translated into local legislation and fully implemented within the sector.
Additional professional efforts have also been introduced. In 2015, the Royal Australasian College of Surgeons launched the Operating with Respect (OWR) programme in response to evidence of bullying and sexual harassment in surgical environments. This programme includes mandatory training on respectful behaviours, reporting mechanisms, and support systems. While an initial survey indicated moderate effectiveness in reducing bullying, findings also underscored the need for a broader, sustained strategy to build a respectful, safe, and inclusive environment. (Reference Gretton-Watson, Oakman and Leggat30)
The American Medical Association (AMA) has similarly developed guidelines to promote a respectful workplace, with the AMA Code of Medical Ethics providing specific guidance on addressing harassment and maintaining professional conduct among colleagues. These guidelines aim to foster a culture of respect and accountability in health care settings. (Reference Shanafelt and Noseworthy31)
The UK’s National Health Service (NHS) has implemented the Civility and Respect Framework, which aims to improve workplace culture by tackling harassment and bullying across all levels of medical hierarchies.
While these initiatives indicate a growing recognition of the need to protect health care practitioners from intra-professional harassment, achieving sustained change requires a comprehensive approach. Isolated initiatives have shown limited impact, emphasising the need for a coordinated strategy that includes policy reforms, robust accountability mechanisms, and cultural shifts within medical institutions. (Reference Gretton-Watson, Oakman and Leggat32)
| When embarking on an advocacy work, we need to know very clearly what would affect the project or proposal, including the availability of human resources, apart from money and materials. |
| I learnt about self-reliance from an organisation called the Indian Self-Employed Women’s Association (SEWA). This organisation encouraged their members to be self-reliant and autonomous, individually and collectively, including in decision-making. Self-reliance is important for women, especially among women survivors of gender-based violence. This campaign raised the awareness on the issue of Violence Against Women (VAW), for the first time, making VAW no longer an issue suffered in silence. ‘Break the Silence’ was the tagline for the campaign, and for many women who have experienced the various forms of violence, their voice was amplified. The campaign showed women’s groups a way to build community awareness as an advocacy tool. The importance for people and organisations with diverse interests to work together for a common goal. It was also important to bring in other stakeholders to play a part in any campaign. |
| Mobilisation is a very important element in any advocacy. In the past, mobilisation was in person and via placards and petitions. Nowadays, social media plays a very important role in getting messages out to various stakeholders. Another important area of advocacy work, especially by women’s groups, was to work with men. In this campaign, it was the male activists who helped to manage the childcare that enabled women with children to attend the workshop. Working with men was a key strategy in the advocacy against violence against women. Alliance building was an important strategy to carry out advocacy work. |
| The advocacy for a Domestic Violence Act (DVA) was a first for The Joint Action Group against Violence Against Women (JAG-VAW). We had to lobby the lawmakers in Parliament and the political groups to support the passing of the Domestic Violence Bill. We developed a booklet on ‘How to Lobby Your MP’ and started to train the members on lobbying skills and advocacy work. Training was an advocacy too as it provided information on issues we advocated. With these skills and knowledge, members of our group went to lobby the members of Parliament, political groups and ordinary people in the community. We learned how to hold press conferences. Every time there was a gross injustice case to women, the All Women’s Action Society (AWAM) together with the other partner organisations wrote press statements and called for a press conference to ensure the public knew of these violations. It worked very well on the issues of domestic violence when JAG-VAW was lobbying for the Domestic Violence Act. This strategy has continued to this day, better supported now by digital media. |
| The JAG-VAW organisations were also familiar with reviewing laws that affected women. The group looked into laws related to rape as the existing laws and practices then were detrimental to the survivors of rape. By 2017, the Joint Action Group for Gender Equality (JAG-GE) were asked to review and redraft the sexual harassment legislation. This is the value of advocacy work, to be able to be mainstreamed into decision-making bodies and committees where our views were listened to. |
Dimension 6: Practices and Activities that Increase the Effectiveness of Advocacy Efforts
Coordinated organisational efforts can create a multiplier effect, amplifying the impact of advocacy initiatives. It is essential to identify and mobilise advocacy leaders across all levels of the health care profession to raise awareness and drive sustained change. This includes engaging medical colleges, health boards, trusts, education bodies, and unions. (Reference Mahase33) Mobilising these diverse stakeholders ensures a comprehensive approach that can address harassment more effectively.
In Table 33.5, Dabota Yvonne Buowari showcases the range of stakeholders she has targeted in her advocacy efforts in Nigeria, demonstrating the importance of a multi-stakeholder approach.
| Stakeholders have an important role to play raising awareness around sexual harassment. |
| Educational Institutions have a role to play at all levels from primary to tertiary. Sexual harassment can occur between students, between teachers, between teachers and students, and between teachers and non-academic staff. Some educational institutions have policies against sexual harassment and the capacity to develop policies and processes across the entire educational spectrum. |
| Professional Associations have been established for women doctors, but there is still a need to support other survivors, including men, lesbian, gay, bisexual and transgender (LGBT) people. Professional associations have a role to play in creating awareness of sexual harassment, including through conducting studies among their members. |
| Sexual Harassment Taskforces can be established across workplaces, educational institutions, and associations to help curb sexual harassment. The goal of a sexual harassment task force is to create awareness and develop a guideline for reporting, including outlining consequences for perpetrators. For instance, the Medical Women’s International Association (MWIA) – a global association of women doctors – created a violence against women and girls special interest group during the 2019–22 triennium. |
| Groups for Talking Therapy can be helpful. Therapy is not available in all countries, especially in low- and middle-income countries (LMIC). Health facilities and educational institutions should provide access to therapy for all survivors and victims of sexual harassment – including group therapy encourages victims to talk about the incident and how they feel about it. Engaging in talking therapy can lead to the formation of support groups for victims and survivors of sexual harassment. Participants can also act as advocates of sexual harassment. |
| The Media can be a useful advocacy tool. In organised work settings, memos, posters and emails can be used for information dissemination. Various forms of mass media can also be used as advocacy tools for creating awareness of sexual harassment at work. These can include the use of electronic, print and social media. Short videos and skits can be produced on the impact of sexual harassment and on how to report incidents, as well as for advocacy and awareness campaign against sexual harassment. The target audience will determine the type of advocacy tool and medium to be used. |
Finally, there is an art to using media to create change. Simon Fleming is a fierce advocate for cultural change in medicine, and has written an article about his approach, with the intriguing title ‘A lot of people just wish I would shut up, but I won’t – how a surgeon has made it his mission to stand up to bullies and discrimination’. (Reference Fleming34) Simon is known for his social media advocacy, and in Table 33.6 he describes his approach.
| When exploring advocacy and what works and what doesn’t work, it is nearly entirely a tale of mistakes made and lessons learned. So I write both acknowledging my privilege and recognising that advocacy is often written or spoken about from the viewpoint of dominant group members (in this context, a straight white man). There is also literature that investigates how ‘non-dominant’ people perceive, or experience allyship. (Reference Rasinski and Czopp35) As such, I will try to explore my advocacy, acknowledge my own privilege and endeavour to not speak ‘for’ others, but rather amplify voices and empower others to do similarly. |
| There is increased interest in allyship, as both a concept and in real world ‘what does it mean for me’ terms. So before I start talking about my journey, I do think it is important to define a little and to expound on the journey nearly all people take to becoming an agent for positive change. I will aim to avoid any mansplaining (better referred to as ‘correctile dysfunction’). |
| Many think of advocacy as being purely disruptive, of calling things out on social media and being the one at the conference or meeting to ask why all the panels are male/pale/stale. Yet really, of course, it is easier for me to challenge things in many/most contexts, as I am generally not the one targeted by the prejudice in the first place. (Reference Czopp and Monteith36–Reference Melaku, Beeman, Smith and Johnson40) |
| The spectrum of advocacy, for me, is a continuum, the Four As of Allyship, (Reference Taylor41–Reference Pettigrew44) which are broadly speaking Apathetic, Aware, Active, Advocate. My advocacy sits at the end of the scale – but that isn’t for everyone. It is a proactive choice, to actively, every day, be an ally, in every context. So I would ask the men reading this, ‘do you sponsor, amplify and empower? Do you resist the urge to “ladder pull”?’ If not, why not? What are you afraid of? |
| For me, like many, what I was afraid of was getting it wrong. Making mistakes. Saying the wrong thing and being called out and cancelled. What changed for me was leaning into that. Accept that if you’re going to challenge things in any context, you will get it wrong. Moreso, if you aren’t getting it wrong, I’d suggest you aren’t trying hard enough. The trick is to accept that either ‘you win or you learn’. If you are trying to do better, because you know better and you don’t get it right, apologise when you make mistakes. (Reference Taylor41–Reference Pettigrew44) Because if you decentre yourself, if you accept it’s not about you, it’s not about you feeling better or you getting closure, but rather those you aspire to support, you’ll be ok with that. And yes, it might mean you get blocked on twitter or you are never forgiven but … |
| … its not about you. |
| Rather, if you are going to use platforms like social media or really any remote media method (papers, radio, TV, etc.), your advocacy needs to be informed by listening to and seeking out interactions with those people who are not in your circle, who are on the fringes. It is through those interactions that your biases and unintentional mistakes are reduced and, more than that, positive perceptions can be garnered. Positive changes can come from your advocacy, rather than finger pointing and blame. (45; 46) |
| This is my final point: it really isn’t about you. You should be listening and reflecting far more than you should be soapboxing and monologuing. If you aren’t listening, you aren’t advocating, you’re just doing harm, with advocacy sprinkles, and that is as true in the online world as it is in the real world. |
| If you listen, if you decentre yourself and if you apologise when you screw up, whether it’s on your phone or on a podium, you will make a difference for the better. (Reference Rasinski and Czopp35; Reference Martinez, Araj, Reid, Rodriguez, Nguyen and Pinto43–Reference Pettigrew and Tropp45) |
Conclusion
Effective advocacy is a complex and dynamic endeavour, requiring a nuanced understanding of the structural and societal barriers that impede progress. To achieve meaningful impact, advocacy efforts must align with the values, priorities, and motivations of specific audiences, while drawing on the credibility, insights, and unique strengths of those delivering the message. By combining reliable data with narratives grounded in lived experience, advocacy can foster both intellectual and emotional connections to the issue.
However, advocacy alone is not enough for sustainable change. Addressing harassment within medicine and clinical settings demands a comprehensive approach that integrates coordinated initiatives, cultural transformation, and robust accountability mechanisms. This effort also benefits from a team-based approach, which not only amplifies impact but provides essential support to advocates who face considerable personal and professional costs.
Ultimately, advocacy is a lasting commitment to justice, equity, and compassion. It is a contribution to the legacy of a more inclusive and respectful profession.
Introduction
Advocacy is often motivated by deep feelings that are quite personal and can be interwoven with a social identity. The development of a social identity aligned with an advocacy movement can support the collective efficacy of the movement itself, but that process of development can involve shifts in perspective over time as an individual gains experience with different strategies, learns about the past and current efforts in the landscape, gains or loses various forms of power and agency, and develops new perspectives on the shifting conditions within which the problem emerges. This chapter is divided into three, bringing different perspectives on the problem of sexual harassment from a medical student, two doctors in training and two medical educators.
May Erlinger describes the personal and emotional journey of becoming mobilised around sexual harassment in medicine as a medical student in Australia. Working towards a career in medicine involves significant costs, part of which are invested in the development of a professional identity where one develops a sense of what a doctor is, then begins to integrate that defined role of ‘doctor’ into a sense of self. Medical students encountering sexual harassment in medicine can thus face threats to the development of that professional identity: what does it mean to discover that your chosen career is rife with toxic workplaces? What do students do with that knowledge? May discusses the ways in which she encountered sexual harassment as a concept and a problem during her time as a medical student: where it was talked about, how it was talked about, what was done about it informally and formally, and the kinds of cultural responses that occurred among medical students. May outlines the challenges and frustrations experienced by medical students in this space, particularly the sense of alienation from policy processes that medical students can feel.
Becky Cox and Chelcie Jewitt describe their own journeys in building an advocacy organisation from a grassroots effort to campaign for cultural change in medicine in the UK. They describe the process of developing their campaign, Surviving in Scrubs, and reflect on the stories they’ve received from survivors, including the challenges survivors tend to face in their own contexts. They summarise findings of their report on the survivor stories they’ve received and draw on these findings to make recommendations for broad changes health organisations might implement to address sexual harassment in medicine more effectively.
Louise Stone and Fiona Moir speak from the perspective of medical education. Both have had careers in medical training, and have deep expertise in wellbeing, safety and professionalism initiatives. In this chapter, they summarise efforts to manage sexual harassment in learning institutions, including addressing misconduct when it arises, and adapting the curriculum and assessment processes to empower students and doctors in training to detect and manage
Beginning the Journey: The Medical Student (May Erlinger, medical student)
An excited group of students pack themselves into a busy lecture theatre, the eager ones at the front and the cool kids at the back. There is a shared nervous tension palpable in the air: it is the first day of medical school. I sat somewhere in the middle, not willing to commit to an identity yet, but when I looked around the room, I noticed something that gave me excited pause: there were so many women. My joy at the ratio was augmented by the presence of the visible, high-profile leadership positions held by women, many of whom gave speeches during our first week of classes. We had a teaching session on bullying and harassment in medicine, which devolved into an informal and engaging conversation about how to respond to lewd, inappropriate, or harassing material. We were asked, in earnest, what could or should we say or do? Who would we turn to, or whether we’d say anything at all? How to reconcile what we might say we’ll do with what we might actually do?
Months later I was still ruminating the questions that had been asked of us. These questions had been posed to us in genuine earnest by powerful women. I couldn’t shake the thought … why are the women at the top of the medical field still asking how to deal with harassment from their own colleagues?
Although I was overjoyed to see that gender equality in medical school now exists in Australia, I’ve also been disheartened to see the enduring historical attitudes of sexism that infiltrate the culture of medicine. I also must note that the gender equity I was excited to see was only representative of cisgender individuals, and in my ruminations and conversations I engaged in while writing this chapter, I wasn’t able to explore the intersection of the effects of the questions posed on gender diverse (trans, gender non-conforming, and intersex) students due to the data not being available. However, even in my two pre-clinical years I learned that this system and its ingrained cultural gender biases create a foundation that silences individuals from reporting sexual harm and perpetuates sexual micro-aggressions, harassment, and abuse, which continues unabated, unreported, and usually with a lack of consequences, with these effects even more compounded for gender diverse students.
We’re told early in medical school that we need to work in teams to solve problems, that clinical reasoning is key to helping our patients, and that by listening to them they will tell us their diagnosis almost as soon as they’ve sat down. We’re taught that when a patient presents to a doctor with multiple comorbidities, is symptomatic, and very unwell, we don’t give them a pill and send them home. Instead, we tackle it as a multi-faceted and nuanced problem, with multi-disciplinary team meetings, differing opinions, and investigations and inquiries. Only then, once we’ve narrowed our differential diagnosis list, and considered which symptoms are most pressing, do we consider what treatments and managements are most important.
Medicine, and the culture of medicine, is sick. It is symptomatic and has multiple comorbidities that are intertwined and difficult to treat: engrained gender biases, an absence of consequences for the perpetrators, a culture that asks for silence as a display of strength, and a corresponding scorn for those who don’t bend to its will. My diagnosis: a resistance to systematic change and diversity of perspectives, a scarcity of supports, guidance, and pathways for individuals to feel safe, and ultimately a culture that allows and enables pervasive sexual harms of doctors by doctors. Others might diagnose Medicine with any number of other illnesses. Some may deny it’s sick at all. But in order to manage symptoms, or even cure it, we have to work as a team, to listen, and to consider our short- and long-term management options.
I cannot claim that the current and incoming cohorts of medical students will fix these problems right away; however, if we are taught that it’s sick to begin with, maybe we can begin to treat it early. As it currently stands, we feel lost trying to figure out where to start and what to do. We understand there is sickness, but just as we have to learn clinical reasoning for our patients, we must learn how Medicine became ill, what previous treatments have been attempted and failed, and what needs to still be done. A generation of doctors needs to be trained in how to push back on the traditional cultural norms and to set the tone of what kind of culture we expect of one another. In medical school, we see the beginnings of how opaque and difficult the reporting systems are, how inappropriate comments from fellow students are brushed off as banter, how senior staff bully juniors and medical students, and it’s labelled as preparation for the worse behaviour to come.
Some students are able to recognise the necessity of pushback against this culture, and they will risk being told they aren’t being team players or being labelled as difficult, while others float along seemingly unaware of the biases, or believing that traditional medical norms are integral to understanding the hierarchy. These concepts aren’t really touched on in medical school curricula, and instead student groups on either side of the fence exist in insular bubbles, not truly engaging on the topics. There are events held by medical societies, which seek to increase student wellbeing, and occasionally host awareness-raising events on the impacts of harassment and bullying, but the bulk of sharing on how to deal with these issues occurs in an informal manner or on social media.
Students warn each other, flag other students or staff, which circulates as well-meaning gossip, but realistically only results in students accepting the ‘every day’ or ‘low level’ harassment. There is an enculturated hesitancy (disguised sometimes as ‘professionalism’), which results in most students leaning heavily on the bold who will advocate on their behalf. This unfortunately builds a space where some students bear the brunt of the behaviour, and others bear the brunt of reporting, with no space to empower either. Ultimately, medical schools and teaching hospitals need to show, in practice, what zero-tolerance policies of sexual harassment/assault look like, and to develop pathways for anonymous reporting and tracking of inappropriate behaviour, that can be actioned if needed. The ethos of medicine should include space for individuals to share their experiences of sexual harm, not necessarily for punitive action to be taken, but rather to demystify and remove some of the burden one carries. When we start to have conversations about sexual harms, from medical school onwards, we begin to note the behaviour that collectively makes us uncomfortable. We highlight predatory behaviour and note that we don’t find it acceptable and won’t tolerate it, not against others and not against ourselves.
Where Harm Begins
Doctors don’t arbitrarily begin acting inappropriately once they are handed their degree; the seeds of their behaviour are planted in medical school and before, forming strong thick roots by graduation. These students who say inappropriate things or make unwelcome advances are often recognised by their peers, they are spoken about in groups, avoided at parties, on placements, or alone in rooms, but rarely are complaints escalated to the medical school. Even when a student’s inappropriate behaviour is reported, they’re usually given second chances, an opportunity to prove they didn’t mean what they did/said, and sometimes they take those opportunities to change and improve themselves, but sometimes they’re clever enough to know they have to get smarter about how they perpetuate this behaviour. Those are the students that become the doctors we are worried about. Those are the doctors that know how to get away with comments or behaviour, pretending it’s a joke, intimidating their victims, or using their status as leverage.
Students aren’t blind to the insidious professional culture that allows for unrelenting sexual harm. However, we are taught, although maybe not explicitly, to allow comments because reacting to them may be considered oversensitive. Similarly, we learn to accept a ‘reasonable’ level of discomfort. After all, we’re acutely aware of the variable power dynamics in medicine, and the weight of a senior’s word against our own. We’re taught to seek out and accept feedback. This is not a bad practice, as it allows us to grow as doctors.
However, with the power dynamics at play, feedback can and does turn dark and dangerous, and yet we’re told to accept it, and more specifically we depend on it to further our careers. We’re not taught how to critically appraise the feedback we receive, nor to question the authority figures around us. Students are enculturated early on to exhibit ‘professional’ behaviour, to rigidly adhere to the social/cultural hierarchy, and to understand that speaking out can jeopardise your standing and label you as difficult. This enculturation is compounded every additional year in medicine, as you begin to see the repercussions of non-adherence to these standards. Unless actively internally resisting, which comes at great emotional and psychological cost, year by year you are disempowered, silenced, and slowly broken to fit the mould that medicine wants you to be.
Reporting Harm in Medical School
Early on in my medical degree I had already begun wondering about the processes of reporting sexual harassment and assault, as have many students in medical schools around Australia. Through my many conversations with students, we’ve each wondered about what to do if a fellow peer makes inappropriate comments or displays inappropriate behaviours. Our thoughts turn to the long days spent in hospital, wondering whether we would dare mention to a colleague, let alone report, if a superior crossed the boundaries we each set.
I’ve had conversations with countless women and men about where the ‘threshold’ should be for reporting sexual harassment and assault in medical school – is it when we feel uncomfortable, after we’ve told them to stop, after rumours have begun, or after it’s happened to someone else? In medical school harmless chatter is interspersed with rumours of harm, making it a difficult landscape to navigate, as students wonder if there is truth to whispered discussion, because surely action would be taken if there was. So for a while these conversations exist as general warnings, with the hope that one day a voice can be strong enough, loud enough, or there are enough voices to create action. In my discussions with medical students around these issues, I’ve encountered the phrase ‘I’d only report in case it happens to someone else’ or ‘… to try and stop it happening to someone else’, more than I had ever anticipated.
Medical students seem to tolerate, and even expect, a level of discomfort, inappropriate behaviour, or assault. Each student seemed to note that they anticipated varying degrees of harassment, and accepted it as a reality, for which they would not report if it affected only themselves, but that if that same harassment or behaviour was targeting or affecting someone else, they’d be far more willing to report it. That greater will to protect others around them is perhaps because of the selfless nature of some entering medicine, or perhaps it is because of a failure of the system to create a space that allows someone to stand up for themselves. Notably there is not a lack of desire to report, to say something, to have a conversation about inappropriate or uncomfortable behaviour, or to change the culture of reporting. There is simply a lack of ability for people to ensure their own safety while reporting.
Although the processes for reporting malfeasance vary from medical school to medical school, and hospital to hospital, the need to be able to report incidents, from microaggressions to assaults, is critical. However, the many conversations I’ve had with students highlight how many failings there are within these processes. Most notably two topics are brought up in each of my conversations: anonymity, and the ability to write down and acknowledge an incident, for future evidence. The need for anonymity in reporting, or even talking about, individuals higher up in the hierarchy who have acted inappropriately is crucial to creating an environment that students feel safe in. Simply being in medical school carries additional quandaries, as the schools are a part of the universities they operate under, in conjunction with varying health services, and are independent entities as well. The interaction of many different external stakeholders creates a confused landscape with differing pathways and systems, meaning medical students are often unsure of what, how, or who to report to, and whether there is anonymity or space to have a conversation about incidents without actioning those conversations.
The lack of clarity, and feelings of safety, in reporting processes during medical school all exacerbate the harm experienced by students who are already some of the most vulnerable in the medical hierarchy. With no stakeholder willing to step forward and claim responsibility over safety (physical or psychological), it teaches students that they are immediately powerless in their careers, that their future is filled with immense uncertainty, because if there is no protection to be given when you’re most vulnerable, why would there be protection later on? Universities and hospitals need to work symbiotically to create an environment that is safe to have conversations about incidents that occur throughout our medical training. Additionally, creating a space where incidents can be acknowledged, either verbally or in writing, without needing to escalate any decisions, is important to establishing a culture where conversations are key to change.
The barriers that exist in medical school around reporting are only intensified once students enter placements. There are fears around retribution; there are concerns of the emotional labour, time, and stress that comes with reporting; there’s consideration of how that report will impact the perpetrator and thereby impact teaching, especially in rural communities where teaching opportunities may be sparser. Mostly there are concerns about how it may impact our future careers. Due to the nature of medical school and training, a lot of the study and work between doctors and students is done in small groups or one-on-one. So, if behaviour is reported, even anonymously, it can be easy for the perpetrator to trace back who did so, even with prolific or serial abusers.
Even still, the students that feel capable, willing, and safe to report quickly learn of the immense time (both in writing the reports, and in the large periods of waiting) reporting requires, alongside the emotional burden of recounting your story multiple times. Rural students are faced with additional challenges where there is not only social and physical isolation, but they must consider the immediate and longer-term impacts of reporting on teaching. Reporting perpetrators in small communities, some of whom may be good teachers, mean there is a decreased quantity and quality in the teaching that is made available to students on placement. These impacts can have long-lasting effects beyond the rotation, especially to long-term rural students. Students begin to internalise personal responsibility for occupational hazards because these barriers all amount to a sense of learned helplessness where students feel that no one can be bothered with them or their safety, so are simultaneously trapped and disempowered by each component of the system.
Ultimately being a medical student is a unique training experience, where you are caught between finding your footing in a densely competitive career, maintaining a sense of ‘professionalism’, feeling like you are learning the entirety of medicine, all while trying not to burn out before you’ve truly begun. This, coupled with the burden of being responsible for your own safety (and sanity), is increasingly difficult in a system that, to students, isn’t necessarily focused on creating reporting processes that are safe. With the structure of medical education being its own barrier to progress and positive change and alongside navigating the workload of study and life (with burn out always looming), even students who haven’t personally experienced or witnessed sexual harm are left with few personal resources to fight for change.
The Future of Medicine
It must be recognised that medicine suffers from institutional sexism, on every level, that was purposefully built into its framework, which contributes to a derisive and insidious culture that historically benefits and fosters opportunity predominantly for straight, cisgendered, white men. Changing this is not an easy task, but it is a necessary one. It can only happen from within, and with that, we require a new generation of medical students, primed with the skills to identify and call out gender bias and inappropriate sexual behaviours from day one. One that fosters opportunities for diverse leadership, that values bystander advocacy and people in positions of privilege using their positions to encourage change, and one that amplifies the voices of the consumers who bear witness to harm which does not instil faith in medicine and doctors to provide compassionate care. The whispers about the sexual predators in medicine, the doctors that students dread to be on placements with, become louder conversations because of strong and courageous women and men who decide that silence serves no one.
We need to build a culture where individuals are willing to stand up and denounce the behaviour, to ask for consequences, and to establish a culture where if anyone was uncomfortable, they are empowered to speak up, for themselves, and not just ‘in case it happens to someone else’. We want to strive for a culture where we actively encourage students to value their own wellbeing and safety and to be able to navigate the delicate skill of changing culture and disrespecting the rigid hierarchy that does serve some purpose in medicine. Culture is changed, in part, through conversation. These conversations about sexual harm in medical school, and in medicine, need to continue, and they need to continue openly and not in the shadows. We need to discuss the multi-layered barriers in reporting and the lack of anonymity while simultaneously having transparency in conversation. We need to discuss what sexual harms are in protected forums, because when a collective comes together to share a safe space, it is easier to mention the leering doctor, the student who touches his peers in inappropriate places, the supervisor who makes uncomfortable comments. Once those conversations begin happening, we recognise the prevalence of the issue, and that it shouldn’t be occurring this often, we begin to talk louder, to call for action from our peers, to ask for accountability from those in charge, and to change the culture.
The sick patient that is Medicine sits in front of us and needs help: it’s our job to ensure they receive the treatment they need. We need to hold our multidisciplinary team meeting to discuss our diagnoses, to consider the comorbidities, to write out our problem lists, and to discuss our short-term and long-term management plans. Not everyone in medicine will believe that the culture is sick enough to warrant treatment; some will cross their fingers and take a ‘wait-and-see’ approach; some will see this as a problem beyond their scope as a practitioner; but some will understand the urgency of treating the patient in front of them. As the medical student standing in the corner of this consultation, I’m desperately hoping the doctor sees what I do and is willing to consider me and my future colleagues’ opinions, perspectives, and ideas, so we can collaborate for effective coordinated care and give our patient the best chance to heal.
Surviving in Scrubs: Using Narratives and Lived Experience to Create Change (Becky Cox and Chelcie Jewitt, perspectives from doctors in training)
Surviving in Scrubs is a grassroots organisation that advocates for the survivors of interprofessional sexual misconduct within the health care workforce, campaigns for cultural change through the engagement of key stakeholder organisations nationally within the UK, and provides training services to educate anyone who works clinically or in health care education or management. The organization was formed in June 2022 by Dr Becky Cox, an academic GP with specialist interests in gynaecology, and Dr Chelcie Jewitt, a specialist trainee in emergency medicine, both of whom have lived experiences of sexual misconduct while working in health care.
Surviving in Scrubs came off the back of a conversation that myself and Becky had following the publication of the Sexism in Medicine survey in August 2021. This piece of work, supported by the BMA, was inspired by my own experiences of sexism and misogyny whilst working within the NHS. I was fed up of working to different goalposts compared to my male peers and I wanted to prove that there was pattern of women in medicine being repeatedly disadvantaged because of the sexist and misogynistic culture that is endemic in health care.
Unfortunately after that report was published, following the initial media attention, the reassuring conversations about sexism and sexual safety in health care came to a halt. That was when Becky and I started wondering what we could do to keep attention on these topics. We had facts and figures, but we realised that it would be survivor stories that would humanise this issue, keeping key stakeholders interested and motivated to bring about positive change. (Dr Chelcie Jewitt – co-founder Surviving in Scrubs)
The core of the Surviving in Scrubs campaign is its website (www.survivinginscrubs.co.uk). This platform enables anyone who works within health care – regardless of their job role, their location, their specialty, their level of seniority or even their gender – to submit an anonymous testimony of their own personal experiences of sexual misconduct within the health care workplace, or incidences that they have witnessed. There is no doubting the power of this collective narrative – with over 200 stories published online at the time of writing – as it has been monumental in ensuring that the sexual safety of health care staff has been frequently reported on by medical and mainstream media since Surviving in Scrubs began.
The need for Surviving in Scrubs to exist as a group is very telling of the cultural issues facing health care workers. There is a lack of support for victims within the reporting mechanisms currently in place throughout the NHS. This often leaves victims feeling isolated, alone and powerless. One of the main motivations for the co-founders in forming the campaign group was to empower the survivors of sexual misconduct by making their voices and their stories heard, as both have firsthand experience of sexism, misogyny, sexual harassment and assault throughout their career, starting as medical students.
Its amplification of survivor voices is what has made Surviving in Scrubs so successful. This grassroots movement has brought the voices and experiences of the many victims to those who are in power. Those stories have evoked emotions of distress in the masses, and it has made many of those in power think beyond the numbers and the statistics that have proved the prevalence of this issue for years (91% of female doctors have experienced sexism; 30% of female surgeons have been assaulted at work). Surviving in Scrubs speaks truth to power, which has enabled representation from the disempowered victims who have been silenced for too long.
Since its inception, Surviving in Scrubs has been invited to speak at several meetings for key stakeholders within health care – NHS England, NHS Education for Scotland, the General Medical Council (GMC), the British Medical Association (BMA), multiple royal colleges, the Medical Schools Council and several medical schools, to name a few. Health care has had an awakening to the fact that there is an issue of sexual misconduct within its ranks, but there is little knowledge or understanding of what needs to be done in order to rectify this issue.
In November 2023, Surviving in Scrubs published its first report – ‘Surviving healthcare: sexism and sexual violence in the healthcare workforce’. This report consists of the summation of the experiences recounted in 150 stories describing sexism, sexual harassment and sexual assault within the health care workforce submitted to the Surviving in Scrubs website anonymously between 2022 and 2023. The stories were submitted voluntarily by survivors and describe incidents of these behaviours, challenged faced and their impact. The key findings are described in Table 34.1.
Key findings
|
This report includes stories from a variety of health care professions, working in a multitude of specialties and health care environments, demonstrating that the damaging culture of sexual misconduct permeates through the whole of health care. A key role of Surviving in Scrubs is to ensure that the discourse around these themes is inclusive of all professionals working within health care, as is the case in clinical practice.
As part of the report, the authors have outlined a set of key recommendations for health care organisations to implement in order to bring about positive change (Table 34.2).
Key recommendations
|
Education
There is a need for effective mandatory education and training for all staff members who work within health care to ensure there is an awareness of what sexism and sexual misconduct is and how it can be recognised within the health care setting. Active bystander and allyship training should be available to all staff as well as training on how to prevent sexual misconduct and promote positive culture change.
There needs to be tailored education for managers, supervisors, and human resource staff groups on how to respond to first disclosures of sexual misconduct and how to support survivors through the reporting process, with particular attention focusing on how they should respond to reports of sexual violence. There is also an argument to provide trauma-informed consultation skills training to anyone who might act as peer or near-peer support for victims of sexual misconduct, or would be in a role where disclosures fall within their responsibilities.
Research into the Impact
Sexual misconduct within health care has only been discussed openly in the past few years, despite the behaviours and attitudes having always been endemic within health care. As such, the research regarding its prevalence and its impact is very much in its infancy. The data relating to the UK NHS workforce is so far very doctor- and, in particular, surgeon-specific, despite these professional groups not working in isolation. The ‘Surviving healthcare’ report contains stories from doctors, nurses, paramedics, psychologists, administrators, dentists, carers, optometrists, pharmacists, managers, health care assistants and health care students, proving that research needs to incorporate other professional groups. Further research needs to be through an intersectional lens, again as there is minimal data looking into how other protected characteristics are affected.
Moving on from defining the prevalence of sexual misconduct, there needs to be research looking into evidence-based interventions to address the culture effectively, and preventing the attitudes and behaviours that lead to sexual violence. It is important to note that the need for this research should not hinder the development of intervention implementation. It would be appropriate for continuous evaluation of any implementations as they occur. The criteria for assessment will also have to consider that an improvement in culture surrounding sexual misconduct would likely increase reporting of incidences as more survivors feel empowered to raise complaints.
When it comes to the impact of sexual misconduct, this could result in research from multiple angles – the psychological cost to staff, the impact to patient care, the financial cost of staff sick days, staff quitting or even the cost of legal proceedings against health care employers.
Independent Inquiry
Surviving in Scrubs is calling for an independent inquiry at a national level to investigate the prevalence, impact and drivers behind the culture of tolerance relating to sexual misconduct within health care. It would also be of paramount importance to evaluate current reporting practices and how this affects survivors, whether they decide to report or not, and if they do what barriers they face. It is important that any such inquiry is independent, removing any influence of party politics on the outcome.
Improved Support for Survivors
Alongside effective training and education for managers, supervisors and human resources staff members to improve the experience of survivors of sexual misconduct raising complaints, there needs to be improved psychological support for survivors. Ideally, this would be via dedicated access to specialist sexual violence support from independent sexual violence advocates provided by the health care employers, who will help survivors navigate the reporting process if they wish to proceed down that route.
Another intervention would be the introduction of peer or near-peer support, either through nominated advocates for sexual safety in the workplace or through in-person or virtual support groups. These interventions would work towards providing a supportive community for survivors, minimising the feelings of isolation that can occur when being a target of sexual misconduct.
Review of Current Policy
A recent investigative article from the British Medical Journal and the Guardian found that 90% of NHS Trusts in England did not have a sexual safety policy applying to interprofessional sexual misconduct. Of the 10% that do have a policy, there is need to review if they are fit for purpose. The recommendation is that the policy should act to prevent sexual misconduct from occurring with education and open discussion forming part of the workplace culture, but also when such incidents do occur, there should be an easy-to-navigate reporting system that offers psychological support for survivors. There should be clear guidance on what warrants reporting and the formal channels of doing so.
Introduction of Specialist Sexism and Sexual Misconduct Policies
At present, most trusts will incorporate issues of sexual misconduct underneath the umbrella of a bullying and harassment policy. Though it is recognised that sexual misconduct does overlap with some of the issues relating to bullying and harassment, there are nuances to sexual misconduct that warrant a specialist policy in its own right. This links back to the need for specialised support for victims.
Another aspect of these policy reforms is that all trusts should provide an honest and transparent record of the number and types of incidences that are being reported within the trust, and what action was taken. All records should be published within the public domain. The aim of this is to encourage a culture of accountability within health care organisations, and for them to demonstrate they are taking staff safety seriously.
Independent Anonymous Reporting System
Surviving in Scrubs, along with the Working Party for Sexual Misconduct in Surgery (WPSMS), is lobbying towards the implementation of an independent anonymous reporting system, available across the whole of the NHS. This is to ensure that there is a standardised reporting system so that nobody working in health care is at a disadvantage if they wish to pursue a complaint against their perpetrator.
Though there is a need for local reporting mechanisms, a national system would be beneficial for everyone. In particular, it would help the individuals who work within small teams where anonymity and therefore psychological safety of the victim could be compromised. This is particularly pertinent within some general practice settings.
Another benefit of a national reporting system is that the data would be centrally stored, enabling pattern recognition of where sexual misconduct behaviours are prevalent, which would alert the need for interventions in terms of education, training and review of policies.
Reform from Health Care Regulators
Currently, the threshold for investigating complaints of sexual misconduct submitted to regulators is too high. A vast majority of cases are dropped at the triage stage of the complaint, meaning that when survivors are brave enough to relive the trauma by raising a complaint, it is often dropped with little to no explanation. This can lead to repercussions for the survivor, such as feelings of helplessness and feeling as though they are not being believed or that their experience does not matter.
Health care regulators need to realise that they have a responsibility to staff safety as well as patient safety, and that should start with them increasing the number of complaints that they investigate. This would also warrant the need of improved support for survivors during the investigation and tribunal processes, with transparency around the tribunal process and psychological support from advocates with specific training relating to sexual misconduct.
Improved Communication
Trusts, GP practices, health care regulators and the police need to improve their communication links in cases of sexual harassment and assault. At present, if a survivor wants to pursue a criminal complaint, they need to report to the police; however, this information is not automatically shared with the NHS Trust involved, nor the regulator of the perpetrator. In a similar fashion, if the survivor reports to the regulator, this information is not shared with other organisations.
These links of communication need to be strengthened as there is a propensity for organisations to pass the buck when it comes to investigating issues, with regulators often refusing to investigate criminal issues (sexual harassment and assault), or stating that complaints do not reach their threshold for investigation and should be dealt with locally. In not communicating these issues, they are adding another burden onto the survivor, making the process of obtaining justice more complicated, forcing them to relive and retell their trauma more times than would be necessary if organisations communicated effectively.
These recommendations are not exhaustive, and as some interventions are introduced, the evidence base of what will be beneficial for survivors will increase, along with further recommendations. There is little information presently about what works best for survivors of interprofessional sexual misconduct within the health care setting. The conversation about the prevalence of sexual misconduct occurring in this space has only opened up over the past few years, so there are a lot more questions than answers about how pervasive sexual harassment actually is.
Surviving in Scrubs will continue to ask the questions about what can and should be done in order to advocate for survivors and protect potential survivors from experiencing sexual misconduct at work. However, it is the responsibility of every individual who works within health care, or within an organisation that supports health care, to strive towards a culture free from this misconduct. Changes must occur across all levels of health care: GP surgeries, community services, hospitals, universities and health care education providers, integrated care boards, NHS England, Wales, Scotland and Northern Ireland, health care colleges and representative bodies, health care regulators with support from the professional standards authority, and the Department for Health and Social Care.
Surviving in Scrubs will continue to speak truth to power, ensuring the voices of survivors are heard. However, ultimately it is these organisations that need to change as they have a responsibility to protect the safety of their staff members, even when it is from other workers.
Next Steps: Leading from Within
When asked to explore the ‘what now/what next’ question, in the context of gender-based violence, it is hard not to be struck, nearly immediately, with moral injury. It feels a little like, if we are having the conversation now, it’s already too late. The harms have already happened, are still happening. Plus it feels so … big. So unwieldy. Having someone ask how to change hundreds of years of patriarchy, hierarchy, power and silence is like having someone ask to just … tweak gravity. But that is kind of the point. The reality is, sure, the best time to change the world we inhabit was hundreds of years ago. But the next best time to change things is today.
So when asked how to change culture and what next, it feels like there are three very distinct questions there – how do we get rid of the normalisation of toxic behaviours and beliefs, how do we excavate the entrenched attitudes of the status quo and then, once we have a dug big ol’ cultural void, what do we fill it with? It’s all well and good to cry ‘burn it down’, but you need a plan about what to build on the ashes.
Most organisations or systems we exist in have survived thanks to certain tacit assumptions. They are a source of strength, a source of reassurance, a cultural blanket to wrap oneself in when things are uncertain. However, the truth is that many of these assumptions do not quite align with the values that might performatively or rhetorically be spoken about. Therefore, when thinking about culture change, many need to overcome the cognitive dissonance between what they espouse and what really happens. This places people and their (albeit anthropomorphised) organisations in a state of anxiety. ‘We must change. We must change now. Oh no. We haven’t changed yet and we don’t even know how. Or what. Or …’. This anxiety state tends to lead to a variant on the grief cycle: fear, anger, denial, more denial, a tons more denial, scapegoating, and then often some more fear and denial.
Instead, we have to lean into our culture. It’s not all bad. In fact, culture gives us strength, it gives us the ability to highlight the bits within our culture that need highlighting for change. It also gives a reassuring sense to those experiencing a fear of, or sense of, loss; we aren’t changing everything, just some bits. Just the bad, toxic, harmful bits.
So what’s next? Next we change the pieces of our culture that need change. We grow, we learn, we make mistakes and then we grow some more. We bring people along with us, as we identify those things that need changing and what we want them to change into. Whether its anonymous reporting systems, ways of declaring relationships in the workplace, websites where people can share their stories, changes in legislation or educational pieces helping people recognise issues, be a bystander or an ally, how to actively listen or any other of the myriad of ways of changing the status quo, the first step is the hardest. Accepting that there is a ‘what’s next?’ and starting to build it. Together.
Medical Education (Louise Stone and Fiona Moir, medical educators)
Throughout this book, we have touched on multiple interventions, many of which begin in medical school. Medical educators have multiple roles, and some of the tasks they perform that are relevant to sexual harassment prevention and management are summarised in Table 34.3.
In chapter 6, we discussed how different axes of power can operate when supervisors take multiple roles, and how these roles can be leveraged to facilitate grooming. We also outlined the importance of the hidden curriculum, and the limitations of competencies as a basis for professionalism training and assessment. We discussed the role of medical migration, and how learners living with multiple layers of disprivilege, including international medical graduates, are at higher risk of sexual harm.
Chapter 6 makes a case for reflective practice. The curriculum is becoming more and more overcrowded with content, leaving less space for students and doctors in training to make sense of their own professional identity formation and workplace experience. Medical students and doctors in training do not have time, or perhaps even the language, to consider who they are becoming as doctors, and when they experience discomfort, unease or trauma, they may not have ways of discussing their own feelings. Without time for facilitated reflection, students and doctors in training are left without models and methods of making sense of complex experiences, and this contributes to silence and shame. Reflection also allows space to consider the culture into which they train, and challenge cultural norms, including inequity, injustice, competitive behaviour, disrespect and misconduct.
In chapter 14 we discussed the importance of professionalism in the curriculum, and the challenge of teaching and assessing it throughout medical training. In this section, we wanted to reflect on the challenge of integrating three aspects of professionalism into the curriculum: teamwork, wellbeing, and trauma and its management.
Wellbeing Curriculum
Medical students and doctors in training are more likely to cope with challenging interactions if they are well. (Reference Byrnes, Ganapathy, Lam, Mogensen and Hu1) Unprofessional behaviour can be a marker of distress within training, noting that student perceptions about what is ‘unprofessional’ can differ markedly from that of faculty. (Reference Reddy, Farnan, Yoon, Leo, Upadhyay, Humphrey and Arora2) Medical training is arduous, and even high performing students with a history of impressive resilience can struggle with the workload and stresses of medicine. However, many strategies used to promote wellbeing in medical students and doctors in training are informal, including voluntary self-care activities, non-specific support mechanisms and the provision of designated pastoral care staff. While these strategies are important, they don’t require students to think critically about wellbeing for themselves or for their patients. This means some students and doctors in training will avoid the curriculum altogether, feeling these strategies are trivial, performative offerings that are not relevant to their situation or their learning.
In New Zealand, medical schools now include curricular content aiming to improve student wellbeing (Reference Moir, Usher, Wilson, Molodynski, Farrell and Bhugra3) with Auckland medical school initiating a longitudinal ‘Health and Wellbeing Curriculum’ in 2013. (Reference Yielder and Moir4; Reference Curtis, Jones, Tipene-Leach, Walker, Loring, Paine and Reid5) The curriculum is based on a framework known as ‘SAFE-DRS’ (Self-care skills, Accessing help, Focused attention, Emotional intelligence, Doctor as patient) and includes assessment, a reflective portfolio and observation by clinicians of how students are managing their stress on the wards. (Reference Yielder and Moir4) The students are encouraged to consider how these principles can be applied to themselves as well as their patients. The inclusion of patients as a focus for wellbeing improves outcomes for both (Reference Moir, Patten, Yielder, Sohn, Maser and Frank6; Reference Frank, Breyan and Elon7) and, frankly, helps to overcome the resistance some students still have to ‘soft skills’ development.
Self-care is an important skill for patients to learn, so they are able to manage their own illnesses more effectively and independently. The World Health Organization has a curriculum of self-care tools, which can provide a basis for learning in this area. (8) Giving students the language of empowerment and agency is important if they are to be able to retain their voices and their agency.
Training includes other challenging topics like diagnostic uncertainty, suicide prevention, and death and dying. Medical training is full of discomforts. Some are quite visceral (like disgust with certain smells, and fainting in the operating theatre) and others are relational, like the dislike or anger that may arise during patient interactions. Learning to name and manage these feelings, and use them as information, are critical parts of becoming a good doctor. Students will also experience ethical discomforts, which are hard to tolerate. By using reflective groups, the medical schools increase students’ ability for self-reflection (Reference Gold, Bentzley, Franciscus, Forte and De Golia9) but also acclimatise the students to talking about feelings and perceptions, in a safe environment. Reflective groups can enable students to talk honestly about their observations and experiences of clinical practice and workplace culture, including negative role modelling and disruptive clinician behaviours. (Reference Villafranca, Hamlin, Enns and Jacobsohn10; Reference Noort, Reader and Gillespie11) These moderated groups can break down silencing, enabling students to normalise conversations about difficult professional conduct in their workplace. It also trains and supports students to speak up for colleagues. (Reference Moir12)
Managing Moral Distress
Moral distress results from ‘physicians inability to act in accord with their individual and professional ethical values, due to institutional and societal constraints’. (Reference Moir13) Many students come into medicine with altruistic aspirations, but the workload and the contrast between their expectations, the values they are taught and the reality of the clinical workplace can be profoundly unsettling. (Reference Gaufberg, Batalden, Sands and Bell14; Reference Warmington and McColl15) Moral distress is associated with a sense of shame, guilt, low self-worth and poor mental health, as well as unhelpful coping mechanisms like overuse of drugs and alcohol. (Reference Dzeng and Wachter13) Managing the inevitable moral distress of working in a workplace under considerable pressure and recognising the early signs of burnout are important skills for students and doctors in training. Students who witness unprofessional behaviour can feel alienated from medical culture, especially if they live with intersectional disprivilege. (Reference Bynum, Varpio, Lagoo and Teunissen16; Reference Romanski, Bartz, Pelletier and Johnson17) In this context it is easy for students to feel they are not valued, and lose trust in their organisations and profession. (Reference Wallace, Lemaire and Ghali18) These students are less likely to report unprofessional conduct, because they do not trust the culture in which they work and the people to whom they must report.
There are two obvious ‘antidotes’ to moral distress and burnout. The first is creating authentic and meaningful roles for students, appropriate to their stage of training and professional development. (Reference Curry19; Reference Grumbach, Lucey and Johnston20) Meaningful work is essential to maintaining wellbeing, but it also helps students use their voices and their opinions. (Reference Helmich, Derksen, Prevoo, Laan, Bolhuis and Koopmans21; Reference Warmington, Johansen and Wilson22) Silent students are vulnerable, and less able to manage or report professional misconduct. The second is reflective practice, which can include reflective writing, (Reference Yielder and Moir4; Reference Wilson and Ayers23) small group discussions about student experiences, and individual or group mentoring. (Reference Uygur, Stuart, De Paor, Wallace, Duffy and O’Shea24) Reflective activities can enable students to discuss the many physical, emotional and ethical discomforts that doctors must learn to manage. To be effective, these groups should be facilitated by an expert who is not involved in grading or assessment, because the dual roles can mean students may not feel the environment is safe. (Reference Reddy, Farnan, Yoon, Leo, Upadhyay, Humphrey and Arora2) Reflective groups can strengthen the bonds between students, improving empathy and shared agency. (Reference Neff25) In the event of misconduct towards them, it may mitigate against isolation, stigma and shame, through having peer allies who can encourage reporting to supportive staff. (Reference Reddy, Farnan, Yoon, Leo, Upadhyay, Humphrey and Arora2) It can also protect against the attrition of empathy that is often seen in early training.
The Trauma Curriculum
Trauma-informed care has become an expectation of clinical practice in many jurisdictions. In medical education, we are only beginning to consider what this means. Many students and doctors in training come to medicine with vulnerabilities and past experiences that will inevitably raise discomforts during training, and even the most robust student will have experiences during training and practice that they will find traumatic. (Reference King, Steenson and Mulholland26–Reference Finkelstein and Mathers28) After all, it is not ‘normal’ or within most students’ experience to dissect a human body, or to cause pain or discomfort to others, even if these activities are authorised within the profession.
If there is one thing medical educators can bring to training, it is the ability to make the implicit, explicit. Medicine is a science, a craft and an art, and there are different skills in teaching these different aspects of the job at hand. While science is familiar, and is generally tackled easily, kinaesthetic skills are taught well by some educators, including interdisciplinary educators like nurses and physiotherapists. However, teaching the art of medicine, including professionalism, is a difficult task. It involves ‘outing’ the feelings and discomforts of others, and modelling appropriate management.
The two disciplines that have a lot of experience in this space are general practice and psychiatry. General practice has a long and proud history of teaching difficult areas of practice, including tolerating uncertainty, managing challenging interpersonal interactions and maintaining appropriate boundaries. Psychiatry has a long tradition of supervision, and good educators in this space have a range of theoretical frameworks to draw on when discussing difficult concepts like trauma. For this reason, these two disciplines are key to the teaching of trauma.
It is our view that students and doctors in training learn best when they see their learning is situated in practice. (Reference Cho, Yu, Lee and Jung29; Reference Shinkaruk, Carr, Lockyer and Hecker30) While some students accept that self-care is part of their role as doctors, others do not, perhaps due to their personal developmental trajectory. Medical educators are well aware of the theory of proximal development: the idea that to teach effectively, concepts must not be already mastered (because the student will disengage) or out of reach (because students will not be able to grasp the idea, and will become demoralised). Ideally, teaching builds on concepts already mastered and ‘stretches’ the student into areas they have not yet understood. (Reference Groot, Jonker, Rinia, Ten Cate and Hoff31; Reference Gillespie, Conn and Dornan32) Teaching skills around wellbeing, trauma and teamwork is best attempted starting with their roles in patient care, and then extending them into self-care, so the student or doctor in training can begin to incorporate personal application when ready.
Like wellbeing, students need a model and language to begin to conceptualise what is happening to them and to their patients when trauma is experienced or re-experienced. There are many ways to undertake this teaching, but one approach to trauma-informed medical education uses the framework detailed in Table 34.4. (Reference McClinton and Laurencin33) It is useful, because it holds individuals and the institution responsible for modelling and managing a trauma-informed approach to curriculum, pedagogy and clinical exposure. It is our belief that students and doctors in training will again be more able to communicate their personal trauma if the language and concepts are normalised in teaching and practice.
| Principle | Practice |
|---|---|
| Realise | Explore systemic bias as a concept and an impediment to just, fair and safe care in the training curriculum. |
| Recognise | Encourage learners to consider bias, discrimination and harms in clinical practice, and to discuss how these may be mitigated. In doing so, students should reflect on their own inherent biases. |
| Respond | Discuss and model how bias, discrimination and trauma activation can be managed to improve patient safety. |
| Resist | Use ‘universal precautions’ to resist unnecessary harms from re-traumatisation. This includes using trauma-informed language, reducing unnecessary requirements to retell stories (patients and learners) and unnecessary exposure to traumatic material in teaching and learning. |
The Teamwork Curriculum
Finally, teamwork needs a similar approach, with the teaching of models of professional interaction and teaching and practice of language around appropriate and inappropriate behaviour in clinical teams. There are many models available to teach, but one useful model has been provided by Belbin. (Reference Belbin34) Belbin asserts that people take different roles in a team, partly due to their inherent characteristics, and partly due to team requirements. Team membership is not static, but fluid, and this can be a reason why a previously functional team becomes dysfunctional. The model taught is less important than the discussions that are facilitated, again in reflective learning spaces. Learners who do not have a language or a model to understand and describe interpersonal dysfunction are left without an ability to understand or respond to toxicity in the team, and again, may withdraw and become disengaged.
Conclusion
In this chapter, we have explored the importance of curriculum around three areas which have previously been taught predominantly in the hidden curriculum: wellbeing, trauma and the interpersonal challenges of teamwork. The hidden curriculum is problematic, because it is unconscious, and may not give students a framework for understanding and responding to difficulties in training. In our view, it is inappropriate, and somewhat cruel, to expect students and doctors in training to learn these difficult skills through simple immersion. Many learners will not ‘pick it up as you go along’, which has implications for them as well as for their present and future patients. In our view, reflective practice, which has been a long-standing tool in the medical educator’s toolkit, should be cemented into the learning experience.
Medical students and doctors in training cannot make sense of the complex world of medicine if they do not have the language, concepts and opportunities to speak. If they have no space to discuss their discomforts and concerns, why would we expect them to have the ability to report sexual misconduct as witnesses or targets?
In this chapter, we have seen authors at different ages, stages and contexts discuss their approaches to sexual harassment in medicine. The chapter raises several important principles:
Lived experience, and the capacity to reflect on personal and witnessed lived experience is critical.
The most vulnerable people in the system should not bear the burden of managing change. Sexual safety is a complex, multi-faceted problem that needs leadership at all levels.
Medical training can be brutal, and this brutality can make it difficult for learners at all levels to have the space and capacity to recognise and respond to misconduct.
Professional identity formation should be discussed, examined and addressed overtly, and not hidden in an experiential curriculum.
Reflection is an important tool that is often displaced by other forms of learning, due to the over-crowded curriculum. This removes critical skill acquisition that is necessary for learners to be safe practitioners in the future.
Organisational oversight is essential to keep students and doctors in training safe. The responsibility for managing sexual harassment should not rest on the shoulders of the most vulnerable doctors in the system.
Medical training is complex and has multiple intersecting curriculums and pedagogy. It is important to keep the art of medicine within the stated curriculum, and not delegate important aspects of learning, like professional identity formation, to the hidden curriculum. Expecting doctors in training to extract learning from experience in this complex area of professional identity formation is unfair, and may mean the most vulnerable are unable to acquire critical skills necessary for their safety and the safety of others.
Introduction
In this book, many authors have discussed the prevention of sexual harms, and the reduction of risks. However, the stark reality of the field is that many doctors are living with the long-term consequences of sexual trauma. For some, this is not their first exposure to trauma. Many survivors, particularly those who live with intersectional disprivilege, have survived multiple sexual traumas, including childhood trauma.
It is often assumed that healing comes with justice. However, survivors have different goals. Some do seek justice, but others simply want safety, for themselves and their colleagues, while others seek quiet healing. Many try to keep their trauma walled off from their professional lives, despite the fact that the barrier between personal and professional has been shattered by the abuse. Unfortunately, some doctors never seek care at all. Every time we present this sort of work, survivors disclose trauma, sometimes for the first time after decades of silent suffering.
In this chapter, we focus on overcoming barriers to care and healing. Barriers can be conscious, with stigma, shame and fear of retribution preventing the reporting of sexual harassment. Other barriers are unconscious, where survivors bury their trauma and attempt to ‘soldier on’, hiding their trauma from the world and even themselves in a locked box buried deep in their minds.
In Stone’s study, a number of survivors discussed the barriers to reporting. ‘You’re just so tired all of the time, because of this emotional energy that’s expended managing the trauma, that you just almost don’t have the energy to fix your life or change anything’, said one participant. ‘You’ve got to be a survivor, and being a survivor takes a lot of energy, and it means that other things in your life suffer.’ Other participants alluded to unconscious coping mechanisms that impeded their own awareness of trauma. “I had pushed it away’, said one participant, ‘but then I got those feelings again back and remembered what it was like and I clarified in my head that it was something that he did wrong rather than me overreacting.’
The cognitive dissonance we, as authors, often encounter when presenting this work is present in survivors. It seems difficult to believe that sexual harm can happen in the cold, hard light of day in a busy teaching hospital. Survivors can invalidate their own experience in the wake of this confusion. One participant in Stone’s study described this as ‘going into numb mode’. ‘I remember wondering whether his behaviour was normal and if there was something wrong with me’, she said. ‘I had difficulty believing that his behaviour was actually real. Sometimes I felt like I was going mad and this made me feel even more unconfident and uncertain about myself.’
These quotes and others in this book suggest that there are considerable intrapersonal barriers to reporting, that may be overlooked when considering the substantial conscious barriers, such as career threat. In addition, rehabilitation involves re-entering the workforce that was the site of the original trauma. In one of our studies, a participant who returned to work described how bewildering it was to re-enter the hospital. ‘I found myself hugging the walls’, she said, ‘because the floor no longer felt safe.’ Another described the difficulty she experienced overcoming her own silence, finding herself stuttering and unable to express herself, which was immensely frustrating.
In this chapter, we focus on two specific concerns. The first is experiencing and overcoming the dissociative response to trauma. The second is learning to overcome the silencing that occurs in its wake. Both are necessary if a survivor is to heal and reclaim their personal and professional sense of self.
Doctors usually start their long careers steeped in an idealistic view of medicine. Many survivors have idealised their perpetrators, and this deep respect can be manipulated as a form of grooming. In chapter 18, Dr Lee describes this experience. ‘My whole belief system collapsed’, she says in her victim impact statement.
For weeks, I could not comprehend what had happened. I could not understand why my trust was betrayed. I wondered how I could have so stupidly misunderstood the intentions of someone I considered a mentor. I called all other staff specialists in the department by their first name, but I always called the offender Prof because … I respected him so much.
Survivors have been betrayed by their professional ‘family’ and have to reshape their ideas of themselves as people and as doctors. One of the participants in Stone’s study was very clear about the next steps the profession needed to take. ‘If we are going to manage this’, she said, ‘we need a curriculum of recovery.’ This chapter forms part of that curriculum.
Becoming Aware: Overcoming Dissociation to Manage Trauma and Shame
Sexual harassment can be deeply traumatic. However trauma is defined, the core experiences are usually disempowerment and disconnection from others. (Reference Herman1) However, survivors can also experience disempowerment and disconnection from parts of themselves, and can therefore experience difficulty understanding and communicating their needs. This sort of disconnection is profoundly distressing.
When sexual harassment occurs within a relationship of trust, such as the relationship between a senior and junior colleague, both aspects of this definition are important. Disempowerment captures the central feature of helplessness, with one’s usual defences being overwhelmed. It is worsened because there is already an inherent power differential in this relationship. Indeed, the hierarchal nature of medicine emphasises the earlier power dynamics of parent–child and the situational dynamics of doctor–patient.
This is what might be called an oppression trauma, defined by Hardy as the interlocking of socio-political oppression and trauma that is systemic, pervasive and protracted over time. The complex interlocking of intersectionality with female trainees and male consultants, or white consultants and black, indigenous or people of colour (BIPOC) junior doctors suggests systemic oppression plays a part in the trauma. (Reference Hardy2) Trauma within the profession can also be considered betrayal trauma, a concept developed by Freyd. (Reference Freyd3)
In Freyd’s theory, abused children separate the trauma from their consciousness in order to preserve the relationship with the needed caregiver. This may occur during the trauma (i.e. the child does not recognise that his parent is hurting him), after the trauma (i.e. the child is unable to remember what happened during the abuse), or both. This dissociation from the abuse facilitates the child’s survival by helping him remain connected with the important attachment figure.
The model of child sexual abuse is one way of understanding the impact of this particular attachment trauma in the medical arena. The medical profession is like a family, with its own culture, mutual dependence and hierarchies, as well as expectations of behaviour. Professional survival is often linked to the perpetrator holding considerable power, and senior colleagues may be invested with trust, respect, admiration and need by the victim. While differences are, of course, evident for an adult experiencing abuse, it is also important to recognise that vulnerability to this occurring as an adult is enhanced by a history of child sexual abuse. This adds to the complexity as not only might a perpetrator ‘recognise’ the vulnerability and exploit it, the repetition of an attachment abuse will increase the likelihood of serious consequences for the survivor.
Dissociation is a powerful defence employed when fight/flight is not possible, and the parasympathetic activation of the freeze response begins. Ferenczi, (Reference Ferenczi4) in writing about child sexual abuse, describes how the child uses dissociation so that the mind is wiped clean of desires, emotions and thoughts. In doing so, the child can suppress their own needs, and focus on meeting the needs of the aggressor. This allows an attuned compliance, unconsciously attending to what the perpetrator needs as a survival tactic. Junior doctors are already well versed in self-sacrifice, suppressing their own needs in service to the patient and the team. The more professional exploitation is normalised (through inhumane working conditions for instance), the more familiar this form of dissociation becomes.
Dissociation is the escape when there is no escape, and is strongly linked to the freeze response. ‘Freezing’ occurs as the next step on from fight and flight, when helplessness and terror is overwhelming and physiologically the body shuts down. The mind then detaches from what is occurring with the consequence that the experience is compartmentalised, separated off from the rest of the mind in what Stern (Reference Stern5) describes as ‘unformulated experience’. This is experience without words, held in the body in the form of somatic flashbacks, fragmented images and potentially relationship templates.
Dissociation Is Another Form of Silencing, Where Trauma Is Wordless, and so Becomes Unspeakable.
The identification with the aggressor as described by Ferenczi also captures the way in which the victim takes in the imagined guilt and shame of the perpetrator. This process has often already begun in the grooming process leading up to an assault. Nathanson (Reference Nathanson, Stubley and Young6) writes of sexual abuse as a relational trauma which is a form of oppression and tyranny. He suggests that it is at the time of grooming that victims begin to lose their capacity to resist. He says:
It is as if the abuser subtly breaks in, steals the authority to say no and leaves a corrupt presence behind, an entity which would make sure that the door would never be locked again.
It is this corruption that is central to the oppression, stealing away the freedom to say no and to reach out to others, to disclose and to break the silence, asking for help and companionship as an essential step in any struggle for freedom. The victim feels implicated, isolated and alone.
Thus, Herman’s description of disconnection from others in trauma relates to the grooming process, the isolation in the moment of the event and the consequences and repercussions of the assault. Silencing, shame, stigmatisation, guilt and despair separate the victim from the rest of society. This is further compounded by the avoidance that is a part of the post-traumatic response, a shutting down from self and others to avoid re-triggering, dissociation and hyperarousal states.
In these multiple ways the survivor may struggle to speak out, to disclose what has occurred. Caught in their isolation and feelings of guilt and shame, lacking the words to have a narrative, or lacking the memories due to dissociation, frightened by the potential loss of the attachment figure and the consequences this will bring – silencing may take many forms.
Survivors who do manage to disclose are likely to have different needs, but general principles for healing, whatever is offered, apply.
Laub and Auerhahn (Reference Laub and Auerhahn7) suggests that trauma therapy involves the communication of ‘testimony’ to a witness willing ‘to be totally present to the survivor, and to receive as well as experience what he / she wants to transmit’.
Trying to bear what is being communicated, without action or attempts to be rid of it, is the beginnings of containment. Wilfred Bion (Reference Bion8) described this notion in terms of mothers and babies, when in the normal course of development, a baby is filled with the early, powerful anxieties, and employs projective identification to communicate what is unbearable to the mother. It is her role to try to take this in, to think about it and attempt to understand what might be going on in the baby’s mind so that she might relieve him of his distress. Over time this gives the baby the experience of someone who can bear what they feel is unbearable and thus can lessen the need to rid oneself of distress.
Where Freud and Klein made love and hate central to psychic life, Bion adds knowledge, particularly the inability to know. The inability to know results from the failure to have found someone, generally in early life, willing and able to contain unbearable feelings, feelings that cannot be put into words, but have more the quality of fragments of feelings. It is only by encountering another mind willing and able to hold these unbearable pieces of feeling that one can learn to put them together for oneself.
Traumatic experience may be understood as a rupture of the container so that knowledge is attacked, the ability to link associated experiences is lost, and the capacity for thought which allows an experience to be recognised and owned is lost. As Alford (Reference Alford9) describes in the quote above, love wants to know, and hate would break what we know into pieces to save us the horror of knowing. Not knowing empties the world of the connections that give it meaning and life its vitality.
Bion’s model of containment highlights the need for another mind to know, to be open to recognising, feeling and thinking about unbearable experiences. This includes all of the complex emotional responses to what has occurred and the mourning process that is needed to heal. Mourning involves working through sadness, despair, guilt, shame, and rage.
There is a moment in the television adaptation of Margaret Atwood’s The handmaid’s tale that captures a central question for those who have been abused, violated and oppressed by a cruel patriarchal system. June, the main protagonist, asks a group of traumatised women who have been talking about how to find a way forwards after such violence and degradation. She says: ‘Why does healing have to be the only goal? Why can’t we be as furious as we feel? Do we have that right?’
June’s suggestion that survivors may need to feel the fury – to have the right to do so – alongside the healing, brings in a broader question than the therapeutic treatment of traumatised individuals. To feel the rage is to allow this aspect of the necessary grieving that is a part of the healing process, to allow the feelings that were cut off through dissociation when it was too dangerous to feel. It is also empowering, and this is a vital aspect of its function when disempowerment is so central to oppression trauma.
Psychoanalyst Beverley Stoute (Reference Stoute10) describes Black Rage arising out of repeated acts of injustice without opportunities for redress that is at the heart of racism. This form of oppression leads to moral injury – inhumane behaviour experienced as a betrayal of what is right. Stoute suggests that indignant rage – in this case Black Rage – is an appropriate response to such injury, that it is an adaptive mental construct and a powerful and necessary defensive psychic force which serves to preserve dignity and self-worth and mitigate the impact of racial trauma.
This links with the need for justice, acknowledgement of what has happened and reparations. Herman (11) emphasises the necessity of a political movement alongside the practices of studying and treating psychological trauma. She argues that:
advances in the field occur only when they are supported by a political movement powerful enough to legitimate an alliance between investigators and patients and to counteract the ordinary social processes of silencing and denial.
The thesis put forward in Herman’s book, Trauma and recovery (Reference Stoute10) is that the process of healing from trauma is essentially embedded in a wider socio-political framework that must always be taken into account. Within this particular context, a robust process of responding to disclosures and supporting doctors in the process of ensuring safety (for themselves and their careers), healing and justice is vital.
Learning to Speak: Overcoming Silence to Manage Trauma and Shame
The problem of employee silence is widespread in hospital-based health care, (Reference Peadon, Hurley and Hutchinson12) and new professionals, including junior doctors, are especially prone to silence. (Reference Donovan, O’Sullivan, Doyle and Garvey13–14) In management and organisational research, employee silence occurs when employees individually or collectively ‘withhold ideas, information about problems, or opinions on work-related issues’ including those where they ‘do not speak up about errors, unfair treatment, or behaviours that violate personal, moral, or legal standards’. (Reference Morrison15, p81)
Junior doctors are inducted into the medical profession via formal and hidden curricula imparted during medical education and training. (16) The implicit messages they receive communicate their place in the medical professional hierarchy and let them know they are to be ‘seen and not heard’ and that the views and preferences of senior colleagues are to be privileged. (Reference Lister, Spaeth, Edwards, Martin and Ashkanasy17) They also experience and witness negative behaviours such as incivility, bullying, harassment and discrimination (Reference Llewellyn, Karageorge, Nash, Li and Neuen18) that are typically perpetrated by doctors higher in the hierarchy (Reference Talash, Corfield, Latcham, Lavelle, Williams and Machin19) and reinforce the silent status quo. (Reference Rai and Agarwal20)
The messages junior doctors receive are effective to the extent they frequently fail to speak up for patient safety and care, (Reference Brennan and Davidson21; Reference Dendle, Paul, Scott, Gillespie, Kotsanas and Stuart22) subverting their professional commitment to do no harm (Reference Loewenbrück, Wach, Müller, Youngner and Burant23) and the organisational obligation to report adverse events and errors. (24) Those who do voice concerns can become victims of symbolic violence, (Reference Bourdieu and Wacquant25) a type of reputational harm that ensures they are effectively blacklisted, unable to secure ongoing employment or progress their training, in which they have invested significant time and resources.
In an environment where speaking up about professionally and organisationally mandated issues can lead to bullying and harassment as well as tarnished reputations and stalled careers, junior doctors are even less likely to voice concerns related to their working conditions and wellbeing. Issues related to hours, pay, rosters, leave and fatigue are therefore also left unsaid, (Reference Creese, Byrne, Matthews, McDermott, Conway and Humphries26) and those related to abuse are even harder, if not impossible, to raise.
In the military, female soldiers who were victims of workplace rape lapsed into two forms of employee silence, acquiescent and quiescent silence. (Reference Pinder and Harlos27) The former is characterised by a sense of futility (speaking up is useless and nothing will change if I do). The latter is associated with suffering in silence – with hopelessness and a lack of self-efficacy to voice that makes speaking up at any point unlikely. Acquiescent silence, however, holds the promise of voice: some victims spoke up about their experiences years later, when similar reports surfaced in the public domain.
The problem of employee silence is, however, a compounding one, and left unchecked it leads to organisational silence, defined as the group-level belief that it is not safe to speak up or it is futile to do so. (Reference Morrison and Milliken28) This creates widespread ‘climates of silence’ in which silence at work becomes the self-perpetuating norm (Reference Morrison and Milliken28, p. 708).
Breaking the Vicious Circle of Silence: Restoring Agency and Confidence to Voice
Much of the literature on employee silence focuses on addressing organisational and structural barriers to voice, and in health care research professional factors have also been identified as significant. Solutions include improving mechanisms for voice, for example via protected reporting programmes such as the Freedom to Speak Up Guardians initiative in the NHS in the UK; (Reference Hughes29) programmes that teach health care professionals how to speak up (see Reference Jones, Blake, Adams, Kelly, Mannion and Maben30 for a review); and attempts to improve organisational or professional culture, the Royal Australasian College of Surgeons’ Operating with Respect programme (31) being one example of professional accountability training designed to reduce bullying and harassment.
Little attention has been paid, however, to ways employees might be supported to address the problem of silence themselves – an oversight that perpetuates the kind of individual inertia Pinder and Harlos (Reference Pinder and Harlos27) identified in their study on silent soldiers. Yet their conceptualisation of acquiescent silence hints at two ways junior doctors, who also work in highly stratified and oppressive environments, might progress from silence to voice.
That victims spoke up after someone else had suggests collective voice could be one way for junior doctors to break their silences. Associated with unions and other forms of employee representation, (32) collective voice has recently been exercised by junior doctors in several jurisdictions in Australia on the topic of systemic unrostered and unpaid overtime. The doctors joined forces in the form of class actions against their hospital employers and the first case was recently found in their favour. (Reference Yu, Jeuniewic and Brook33) Finding ways to connect junior doctors who are victims of work-related sexual assault, via class actions or other means, could provide a safer way to speak up.
That some of the soldiers in Pinder and Harlos’ (2001) study (Reference Pinder and Harlos27) eventually broke their silence, despite long-term fear and inertia, suggests interventions that enhance individual agency could also be useful, workplace coaching being one example. Coaching is an agentic activity that empowers individuals in several ways. (Reference Jones, Woods and Guillaume34) First, it provides a space where they are listened to and heard. Second, it uses questions that prompt people to find solutions to work-life problems. Third, it uses goal setting to enable people to develop accountability and track their performance.
Research on junior doctor silence, conducted by one of the authors of this chapter, suggests the movement from silence to voice occurs on a spectrum as individuals develop agency, and that the journey takes place in stages (Figure 35.1). In the first or wounded stage, junior doctors are at the silent end of the spectrum, overwhelmed by their circumstances and hurt by their experiences to the extent voice (on any topic) is impossible. In the second, pragmatic stage, junior doctors are aware of their plight but continue to believe voice is not welcome. Highly functional, they accept their situation with stoicism. In the third stage, junior doctors become critical – and cynical – about their situation. Anger can propel them to speak up about the things that matter most to their wellbeing, such as the inability to obtain parental leave. In the final, confident stage, junior doctors are more likely to raise concerns. They have learnt how to navigate the complex systems in which they are immersed, established allies who can support their efforts to raise concerns and have greater self-efficacy to voice.
The transition from silence to voice.

This trajectory supports the notion that increasing junior doctors’ sense of personal and professional agency is required if they are to break free of their deeply held beliefs that speaking up – be it about sexual harassment, other working conditions concerns or patient safety and care – is neither permitted nor welcomed. Coaching encourages individuals to become active leaders of their own lives rather than the passive recipients of life. Focused workplace coaching that aims to develop communication skills could offer junior doctors a path to voice. As the ability to speak up has also been linked with increased employee wellbeing, (Reference Brooks, Wilkinson, Brough, Gardiner and Daniels36) workplace coaching could also be a path to recovery.
Designing a Curriculum that Incorporates the Tools for Recovery
We are no longer in an era where doctors are expected to be relentlessly objective. The symbolic separation of doctors from their patients, in the form of white coats, special obscure language and other symbols of power, is breaking down. It has been interesting to watch doctors return to special clothing in the form of scrubs during the pandemic, perhaps as a way to re-establish appropriate infection control and symbolic therapeutic distance.
Doctors are taught to relentlessly suppress their personal and emotional needs. Medicine demands sacrifice. It chooses the elite thinkers, who dedicate their early lives in achieving high academic goals. It then expects over a decade of commitment to higher learning, and this includes lengthy hours, including hours that are never captured in a timesheet. In addition, doctors in training still tolerate and may expect ‘beneficial mistreatment’, the years of harsh expectations and feedback which they believe will make them better doctors.
Medical training and practice may come at considerable expense. Doctors have high rates of mental illness, alcohol and other substance misuse and relationship breakdowns. Suicide rates are high. Doctors live with high and often unachievable personal expectations. At this time in history, they also live with growing occupational violence, in workplaces that are becoming psychologically unsafe.
In order to survive the brutality of medicine, the painful procedures that must be carried out on vulnerable patients like children, the bad news that must be delivered, and the witnessing of appalling trauma that must be endured, doctors need to learn to moderate their empathy. In difficult consultations, and during difficult procedures, doctors will often revert to objective, theory-based thinking, partly to protect themselves from the trauma, and partly to ensure the patient gets what they need without the doctor being distracted by their own distress. It is therefore understandable that doctors may not have the language, experience or frameworks to manage their own trauma. Although there have been moves to destigmatise mental illness in medicine, to encourage the sharing of feelings, and to provide non-specific support mechanisms for doctors, often these are couched in terms that imply the doctor is responsible for managing their own distress. It is even a requirement in some codes of conduct that ‘doctors maintain their own wellbeing’. Some now describe this as ‘wellbeing washing’, the illusion of care that is a light dressing over a deep wound. One cartoonist described this well, when talking about the NHS. In response to a request for more support for doctors, the manager responds, ‘we’ve given them a room to cry in, what more do they want?’
In this environment, doctors who experience their own trauma may lack the words, let alone the theories, to understand what has happened to them, and to communicate it to others. Their defences have been shattered, the personal and the professional selves are no longer walled off, and underneath their thick layer of protective objectivity, they may lack the capacity to make sense of the experience. The injunction ‘it’s good to talk about things’ doesn’t help if there are no words to describe the feelings experienced, or no-one who the survivor feels is safe to hear the message.
As educators, colleagues, therapists, leaders and regulators, we need to consider how we can use the frameworks doctors already have in place to manage this wordless trauma. One way, of course, it is to teach trauma theory and trauma management early in training. Doctors revert to theory if a situation is distressing. We need to supply theory they can use. Psychological trauma should also be debriefed in a formal, objective way, perhaps with structures like root cause analysis that are already well known, so doctors have appropriate scaffolding to discuss difficult challenges. When trauma occurs, it is naïve to assume that all doctors need is kindness, compassion and non-specific support. Although these are helpful in themselves, trauma-based therapy is a difficult skill that requires expert practitioners. Assuming this form of trauma can always be managed with non-specific kindness and empathy underestimates the impact this form of trauma can have on a survivor. Doctors deserve well-trained and capable trauma-based practitioners who can help them name their experience, understand it and find ways to move beyond it to return to practice if they choose to do so.
Conclusion
While it is much more comfortable to talk about the primary prevention of sexual trauma in the medical profession, it is more realistic to accept that there are many survivors in the medical community who are still affected by their own experience. If we are to relieve their suffering, and prevent others from the silent endurance of long-term psychological harm, it is important to find ways to help survivors speak. In order to make that possible, they need the words, the narratives and the expert safe spaces to facilitate healing and rehabilitate their personal and professional sense of self.
In writing this chapter, we realise we have not produced the evidence-based guideline that many would want to see. We remember approaching a senior bureaucrat in Australia and describing what we have tried to achieve. ‘I hope it provides solutions’, she said, ‘and isn’t just another collection of complaints’. While the book is not a ‘collection of complaints’, we have not attempted to provide a solution-focused manual. In the Introduction, we wrote that this book is not a reckoning. It is also not a protocol to support specific action. The reason is simple. We do not believe there is one solution that is universally relevant.
In medicine, we often see simplified ‘solutions’ proposed to address complex health issues. These ‘solutions’ don’t work, or they only work for the privileged. We did not want to replicate that approach. Instead, we have chosen to explore the complexity of the deeply sociocultural issue of sexual harassment and abuse.
In this conclusion, we have produced several frameworks for jurisdictions and individuals to address this problem in their own culturally relevant way. We present a way of understanding the problem, drawing on the insights included throughout the book. We then outline a health promotion framework, also synthesised from the collective expertise of the authors.
Creating Cultural Change: Diagnosing the Problem
Medical culture is seriously unwell. In psychiatry, one way of understanding illness uses formulations, descriptions of why a person may be ill at this time. Formulations help guide treatment, because they support us to understand the issue in all its complexity. They are often written using the categories of predisposing factors, precipitating factors, perpetuating factors, and protective factors. We can use the same discipline to approach the problem of sexual harassment in medicine, using the insights our contributors have detailed throughout this book. This framework can be adapted to any context, to help institutions understand the most relevant interventions for their particular culture.
| Predisposing factors | Precipitating factors | Perpetuating factors | Protective factors | |
|---|---|---|---|---|
| Cultural issues in society as a whole |
|
|
|
|
| Predisposing factors | Precipitating factors | Perpetuating factors | Protective factors | |
|---|---|---|---|---|
| Cultural issues within the profession |
| Lack of challenge from colleagues, including critical failure to speak truth to power |
|
|
| Workplace and regulatory harms and limitations | Medical regulatory harms leading doctors to avoid mental health care for fear of de-registration
Workplaces and regulatory bodies casting mental health as an individual not a structural issue Using ‘resilience’ narratives to cast structural failings as individual responsibilities Increasing expectations on doctors with diminishing resources, leading to moral distress and harm | Moral licensing of perpetration because of the reputational good they offer the organisation and individual patients and team members |
|
|
| Occupational trauma and violence in medical workplaces |
|
|
|
| Predisposing factors | Precipitating factors | Perpetuating factors | Protective factors | |
|---|---|---|---|---|
| The structure of medical work |
|
|
|
|
| The structure of training |
|
|
|
|
| Discrimination in medical culture |
|
|
|
|
| Predisposing factors | Precipitating factors | Perpetuating factors | Protective factors | |
|---|---|---|---|---|
| Individual characteristics and experiences |
|
|
|
|
Creating Cultural Change: Health Promotion
Throughout the book, authors have discussed interventions at all stages of the health promotion hierarchy. A common problem in this field is to attempt to eradicate sexual harassment by using only one solution, targeting one level or stage of the health promotion trajectory. Inevitably, these single solutions will fail.
In the following framework, we attempt to classify the solutions and approaches described in this book into health promotion stages. We will not discuss broader issues outside of medicine, including the structure and function of law, education and other social institutions or the multiple marginalisations experienced by students before and during their training. Broader social risks are described in chapter 8, and issues around gender inequity are well-described in chapter 2. Instead, we will focus on change within medicine.
Primary Health Promotion
Primary health promotion is an attractive option, because it works on preventing misconduct occurring at all. Around the world, there have been calls for ‘zero tolerance’ of sexual harassment, with organisations using primary health promotion strategies to reduce risks, ideally until the issue is completely resolved.
In general, strategies in primary promotion fall into the following categories:
Training for Employees to Ensure Everyone Has a Common Understanding of their Obligations
The start of sexual harassment prevention is making sure all workers can recognise sexual harassment and understand their obligations under law and the organisational policy to prevent it. In some countries, there is no legal precedent for this work, as sexual harassment is not defined in law, which can make this process challenging.
To prevent sexual harm, employers need to provide all workers with clear and consistent information, instruction and training. One of the biggest issues is that different people will have different understandings of what sexual harassment is (see chapter 4) and so may respond, or not respond, to different situations. This is especially the case where staff come from different cultural backgrounds where understanding and tolerance of sexual harassment can diverge.
Common approaches to this type of health promotion are to mandate educational programmes and to ensure the knowledge is mastered using a variety of assessment tools. In doing so, organisations can guarantee that their employees are informed about sexual harassment, and can define it, but there is no such guarantee that they will recognise it when it occurs in the workplace. These approaches are compliance focused and fail to include attention of the informal systems of how such policies will be utilised in situ.
Skill Development to Recognise and Respond to Sexual Harassment
While people may recognise sexual harassment in theory, they may not recognise it in practice. Some of our editors have had experience running scenarios of discrimination and harassment, role-played by professional actors. Even when primed and supported, we have been surprised at how difficult it is for medical students to respond to these situations.
Knowledge of sexual harassment is not the same as the capability to recognise and respond to it in context. There is a clear difference here between knowledge and professional skill. There is a body of research work needed to underpin this form of training to ensure it translates into action in the workplace.
Assessing and Managing Risk
In order to manage issues around sexual harassment in medical workplaces, it is necessary to understand risk. We are still learning about individual and team risk, but initiatives like HOTSPOTS in New Zealand (described in chapter 14) attempt to map risks over time, based on a dynamic analysis of learners’ feedback. Using this model, we expect it will become possible to identify high-risk teams, and potentially high-risk individuals. Hopefully, we will also be able to detect and communicate features of highly functional and psychologically safe teams, so these skills can be transmitted to learners and educators in the future.
However, doing this work requires much more granular data about interpersonal behaviour than we have in practice. We trust that education and skills development will create a common language around sexual harassment, and therefore provide more accurate and predictive data. We also expect that further research in this area, particularly ethnographic research, may inform responses to particular workplaces, such as emergency departments, surgical theatres and mental health facilities, where sexual harassment seems to be more common.
Developing Safe Work Policies
Policy development seems to be central to providing a safe workplace. However, it should be recognised that sexual assault has been illegal in most jurisdictions for decades, and yet even extreme forms of abuse, such as rape, continue to occur. There are two important aspects of policy to consider. Firstly, the policies must be known, and this is a question of education. Secondly, they must be accepted, respected and followed. The problem here is that written policies may not reflect the hidden rules that are accepted by staff, more commonly described as ‘the way we do things around here’.
There is a parallel in urban planning, to describe the way humans (or animals) may create an alternative path to the one created for them. One phrase for these paths is a ‘free will way’, an unplanned small trail caused by human or animal traffic that shows us where we choose to travel. It is usually the shortest or the most easily navigated route to the destination, the short cut, or preferred route to a destination, and the depth of its surface erosion is often an indicator of the traffic level it receives, relative to the official route. In other words, a free will path reflects ‘the way we do things around here’.
Despite building formal policies, laws, and educational materials that look effective, predators continue to use these preferred routes and use cultural, hidden rules that leave survivors abandoned. The work that needs to be done is to understand how these hidden paths have been used, how policies have succeeded (or failed) to meet their objectives, and how inappropriate attitudes and behaviours can be challenged and changed.
Performative policies need to be changed. Employees view workplace policies as genuine when they are motivated by care and concern for employees, and are thoughtfully and consistently implemented. Insincere or inequitable policies can lead employees to question the overall ethics or values of an organisation and trigger a lack of trust. In this way, policies can actually impede reporting. Unfortunately, employees can base their trust in the organisation on the implementation of the entire policy suite. This means that when a hospital claims to value their employees, but continues to expect unpaid overtime from its junior staff, or use other exploitative practices, it undermines trust in their entire policy framework. Over time, such abuse can transform into distrust.
Finally, it should be recognised that policies intersect. A doctor in training who has experienced sexual harassment may report to a number of organisations and disciplines, described throughout Part 2. Inconsistent policies, policies that overlap or contradict each other, and policies that are deeply opaque mean that survivors distrust the process, and do not report.
Secondary Health Promotion
Survivors of sexual harassment are more likely to come from disprivileged populations. As detailed in chapter 20, international medical graduates are at higher risk. There is little written about secondary health promotion, perhaps because it is quite confronting to consider the cultural prejudice and discrimination behind the choice of doctors likely to be targeted. If we decide to implement a curriculum that assesses and addresses racist behaviour towards international medical graduates, we need to accept that our profession has deep sexist and racist roots, which is uncomfortable. It reveals the wider identities of ingroups and outgroups that maintain wider systems of patronage within the profession. Nevertheless, the strategies that work for privileged doctors may not be as effective with those who live with intersecting marginalisations.
The second issue is understanding and responding to high-risk environments. Because our measurements of prevalence are inconsistent, both in definition and methodology, it is difficult to compare learning environments. Strategies successful in an operating theatre, a highly ritualised and formal team environment, may be counterproductive in a community clinic.
Identifying High-Risk Situations
There have been prevalence studies in many medical workplaces across different countries and different contexts. There have also been studies of medicine relative to other health and social care professions that specifically identify the greater frequency of this issue for and within medicine. However, at the time of publication, there have been few high-quality studies that have compared prevalence across contexts using the same methodology and the same criteria.
We know that doctors are at risk of sexual harassment from nurses, carers and patients, as well as colleagues. One of the issues in medicine is that patients may, at times, lack capacity to regulate their behaviour. For instance, surgical patients may behave quite differently while recovering from anaesthetics. Patients with dementia or mental illness may be unable to regulate their behaviour due to illness or disability. Emergency departments can seem quite chaotic, and may have patients who are still under the influence of drugs and alcohol. In these environments, inexperienced doctors can have difficulty distinguishing the sexually aggressive patient from the unwell patient, and may therefore tolerate behaviour that would be unacceptable in other contexts.
Supporting High-Risk Targets
This is a difficult area, because population risks and individual risks are not the same. For instance, certain communities may be particularly intolerant towards doctors of a certain race. Identifying those doctors at risk is difficult. We do know that international medical graduates are at particular risk, and in the training of these doctors to manage expectations of medical practice, there needs to be similar training to help these doctors respond to racism, harassment and discrimination. Racism can also lead to witnesses discounting the experience of International Medical Graduates.
Throughout the book, authors have highlighted the importance of training everybody to respond to inappropriate behaviour. Normalising good bystander behaviour as well as strategies to manage harassment as a target is essential to ensure doctors living with multiple marginalisations are well supported. This is vital to fostering and maintaining trust within these teams and workplaces.
Managing High-Risk Perpetrators
There is little written about perpetrators in medicine. Researchers from the University of Melbourne have analysed risks to identify the higher risk from repeat perpetrators in doctors and thus the value of distinct sanction. (Reference Bismark, Spittal, Gurrin, Ward and Studdert1) Professor Searle’s work suggests there may be a difference between the predator, who chooses medicine to access targets, and the doctor whose behaviour becomes disordered over time. (Reference Searle2) While there is little written about early identification of high-risk individuals and the effectiveness of remediation, we have seen in multiple chapters of this book that perpetrators are rarely removed from the medical workforce, resulting in escalating scale and frequency of sexual assault. This is one area where more research is needed, to better understand not only how to exclude potential perpetrators from the medical workforce, through selection and assessment processes (see chapter 14), but also how medical culture supports and enables sexual harassment and abuse. Senior medical staff may lead a very socially restrictive life, with extensive work commitments precluding the development and maintenance of personal and social support. The rates of alcohol abuse, mental illness and death by suicide are disproportionately higher in doctors, and we are yet to acknowledge and understand how medicine as a culture can actually drive professional misconduct. This is a difficult, but necessary, area to research.
Tertiary Health Promotion
Unfortunately, it is unlikely that sexual harassment will be eradicated from the workplace altogether, so it is essential that organisations have the systems and processes in place to better identify issues, and to reduce the further trauma from the reporting process. Although it is obviously important to communicate the process clearly, it is also critical to make the process trauma-informed. As discussed in chapter 35, trauma-informed processes are essential. In the case of reporting, the following strategies may be helpful.
Establish a trustworthy and capable team for reporting and to support those involved in these processes. Conflicts of interest should be prevented.
Develop trauma-informed investigation processes that facilitate collection of best-evidence and do not re-traumatise survivors and witnesses through re-tellings. Separate interviewing of survivors, witnesses and alleged perpetrators and provide trauma-informed support for all participants during and after the process.
Clarify the process and its components for the survivor(s), alleged perpetrator and witnesses to clarify expectations (including what will and will not be included, and terms used). Communicate potential costs, and potential outcomes.
Create organisational communication strategies to communicate outcomes to the people and teams involved.
Design trauma-informed approaches that facilitate recovery through restoring the agency and control of survivors. Strategies should include setting the time and place of any meetings, and setting clear tasks to achieve at each meeting in collaboration with survivors. The survivor should be allowed to exit the meeting if they need to do so.
Reducing Reporting Barriers and Streamlining the Processes of Reporting
Strategies in this area involve writing processes that are clear and understood. It is important to get multiple stakeholders to identify gaps, and omission and conflicts in these process, or confusing content. This includes seeking advice from survivors, who may identify barriers to reporting. It also should include ongoing monitoring and review of policies and their review to ensure information contained is accurate and current. Organisations should ensure when and how other organisations may be involved in reporting, to ensure survivors are not confused by intersecting and contradictory policies. There should be a well-informed support person available who can advise on these processes. Ideally, this person should not be involved in teaching or management, to avoid potential conflicts and enable the survivor to consider their options independently. Whether the survivor chooses to report or not, they should be offered independent support. The process should minimise re-tellings by the survivor.
Communicating Investigation Outcomes to the Workforce
It is necessary to balance transparency and confidentiality. De-identified information should be released in a way that respects confidentiality, but ensure the workforce understands that allegations of sexual harassment are taken seriously and that there are consequences. These controls and provision of information are critical to maintaining trust.
Analysing Critical Incidents
Throughout the book, we have seen examples where policies and processes can be harmful. Policies have failed, and processes have been unexpectedly ineffective. One particular challenge is when a survivor withdraws their report.
Throughout this process, there are usually multiple, consecutive failures. The harassment has not been prevented and it may have not been recognised or reported by the survivor or the bystanders. When reports have been received, the process may not produce a satisfactory outcome. Because these processes are so complex, it is essential that they be examined carefully with a view to improving policy and process. There are, of course, processes to examine clinical failures in medicine, and a similar root cause analysis can be followed.
Providing Rehabilitation for Survivors
For the survivor, there is the difficult decision to remain within the culture that harmed them, to change speciality, or to exit the profession entirely. The loss of doctors to the profession when they are unable to re-enter the workforce has received little attention. Medical training is an extraordinary investment of resources, not only for the survivor, but also for patients and the community. Survivors who have invested heavily in their professional identities feel lost and isolated when they are no longer able to practice. They not only lose the capacity to work, they also lose the collegiality of their peers. These derailed careers also have consequences for employers, impacting their equality and inclusion policies, and efforts to attract and retain more women and those who live with intersectional disprivilege into medicine. It is important that rehabilitation emphasises the repair of wider relationships that will have been damaged in these cases and their subsequent reporting processes. This wider group might include both colleagues and patients.
Given that sexual harassment and sexual abuse constitute a failure of governance, it should be a collegiate responsibility to help the survivor regain as much function as possible. If they return to the workplace, re-entry is challenging. The workplace may seem the same, but the survivor may be changed. As Dr Dominique Lee wrote in chapter 18 ‘When I went back to work, I found myself hugging the walls because the floor no longer felt safe’. There will also be others for whom her treatment makes this a distrusted workplace.
Quaternary Health Promotion
Quaternary health promotion focuses on reducing the harm associated with reporting. Re-traumatisation is a common consequence when reporting involves multiple retellings in a variety of settings that may or may not feel safe to the survivor. In the 1970s, an Australian judge famously described women who reported rape as ‘heroines of fortitude’. In doing so, he recognised the courage it took to survive the trauma of reporting.
Managing Privacy and Confidentiality
Exposure, loss of anonymity and gossip are all painful, especially when the case is high profile and the media is involved. The people involved in any investigation should know who has been informed about the case, and who has not. Communication needs to be carefully managed, and the workforce needs to be reminded of their obligations to respect the confidentiality of the people involved. Workers’ rights to confidentiality should be protected.
Reducing Victimisation
When survivors report, their team can easily ‘take sides’, expressing their support for either the survivor or the perpetrator. The siding with individuals can create further betrayal, and damage other relationships. If the media becomes involved, both parties are harmed through the airing of opinions, and the judgments of others, including those they thought were colleagues or friends. Survivors can experience inappropriate interpersonal communications in their team, including gossip, bullying and further harassment, which limits their capacity to focus, including on their work. It is essential that teams around the survivor and the alleged perpetrator are monitored to ensure each is protected from this form of harm.
There is a particular type of victimisation which involves the adversarial nature of investigations. We are aware of survivors who have reported to regulatory bodies, and have been unable to withdraw from the process when it became deeply traumatic. Regulatory bodies need to ensure they have clear processes to manage ‘victim whisteblowers’. When mandatory reporting for professional misconduct is required, it is unacceptable to force a survivor to report their perpetrator when the report itself causes deep harm. This is a complex problem, but mandatory reporting should not override a survivor’s health and wellbeing.
Reducing Re-traumatisation
Although it is critical that reporting processes establish essential facts, it is also important to minimise discussion of the harassment to what is necessary to achieve outcomes. Multiple, unnecessary re-tellings can deepen trauma.
Restoring Safe Culture
The principles of restorative justice include preventing further harm by working with those involved to set relations right. All people impacted by the wrongdoing – survivors, perpetrators, witnesses, patients and community members – have a voice in the justice process. However, in order to make this process work, we need to actively repair trust and create safe spaces to have difficult conversations, where people can share freely without judgment.
Final Words
Doctors are committed to healing, and deeply familiar with complexity. Within the profession, there are many who are expert at deconstructing complex problems on a micro, meso and macro level. The profession should be able to tackle this problem within their own culture the way medical error was tackled in the past, creating safe spaces to honestly and openly deconstruct a problem and proffer potential solutions, setting aside defensiveness, blame and stigma. Doctors should be able to understand the trajectory of trauma, from the prelude that predisposes a doctor in training to abuse, to the restorative justice that sees a survivor return as a valued member of the profession they love. In doing so, they should draw from the expertise of many others, including experts in law, social science, therapy, management, and many others.
This book has presented a range of initiatives that are occurring across the world, at all levels. Internationally, the Sustainable Development Goals championed by the United Nations are driving gender equity, reducing the gendered hierarchies in place in most cultures and most workplaces. Although some countries have no legal sanctions for sexual harassment, increasingly, countries are improving their legal approaches to sexual trauma, and many are specifically targeting sexual harassment in the workplace. Medical organisations are recognising the cost of sexual harassment and abuse in the workplace, and beginning to address barriers to reporting, including the need to ensure there is a positive duty to create and maintain psychologically safe and trauma-informed workplaces. Finally, and perhaps most importantly, the stigma and shame experienced by survivors is breaking down, with many doctors openly discussing their experiences. Doctors’ health has finally become a topic for discussion in the profession, although many are still wary of acknowledging their issues and seeking help.
The editors have attempted to synthesise the breadth of trauma and healing that is occurring across the world. The book could not be a comprehensive representation of all experiences, but it does attempt to show how diverse experience can be. Like good qualitative research, the findings are not generalisable, but they are transferable to other settings, other professions and other cultures.
This book is not a reckoning, but it does create an opportunity to advance healing, safety and restorative justice. Medicine needs to recognise the issue and to seek to heal itself. While doctors understand trauma, and healing, they are not the only profession to face the problem of sexual harassment and abuse, but of all the professions, they are best placed to manage it most effectively using the skills deployed every day in clinical work. As a profession, medicine has done its best work when it has provided moral and cultural leadership. Facing this problem frankly and openly is part of that leadership.
As editors, we hope this book will provide the framework for other cultures, professions and jurisdictions to address their own ‘dirty little secrets’. It is time to stop performative policy, the type that offers simple solutions to complex problems. There is no value in another compulsory workshop, aspirational statement or media campaign. Instead, we hope this book enables the reader to engage meaningfully with the interpersonal, interdisciplinary and international complexities of workplace sexual safety.
Sexual trauma should never be the price a doctor pays to work in the medical profession.
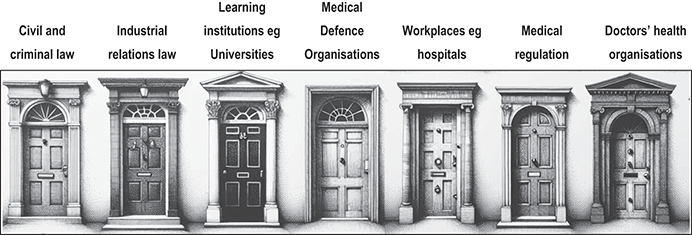

 Open access
Open access