


Introduction
CHD is the most common congenital defect. As surgical interventions rapidly advanced, the field also shifted its focus from survival to understanding the long-term effects of living with CHD. Reference Marelli, Ionescu-Ittu and Mackie1,Reference Warnes, Liberthson and Danielson2 In 2012, a comprehensive review of the field demonstrated that children with CHD are at an increased risk of developmental delay or disabilities. Reference Marino, Lipkin and Newburger3 This finding has been replicated; children with CHD, particularly those who have more complex forms and have undergone cardiac surgery, are at considerable risk for developing cognitive, behavioural, and emotional problems. Reference Abda, Bolduc and Tsimicalis4
In 2016, the Cardiac Neurodevelopmental Outcomes Collaborative was founded with a mission “to determine and implement best practices of neurodevelopmental services for every individual with pediatric and congenital heart disease and their families through clinical, quality improvement, and research initiatives.” 5 Starting from birth and following until transition into adulthood, Cardiac Neurodevelopmental Outcomes Collaborative recommends a comprehensive battery of neurodevelopmental assessments for children living with CHD. These batteries adapt and change over time to reflect child development and include measures of intelligence, executive function, memory, motor skills, adaptive behaviour, and socioemotional functioning. Reference Bar-On6–Reference Reynolds and Kakmphaus8 Although several components of this battery address aspects of emotional development, they do not capture the full breadth of emotional intelligence. Reference Davis and Wigelsworth7,Reference Sood, Newburger and Anixt9–Reference Ilardi, Sanz and Cassidy13
Intelligence is conceptualised as a multidimensional construct, with a general intelligence factor (g) at the apex of the model and 8–10 broad complementary abilities subsumed. Reference Caemmerer, Keith and Reynolds14 Cognitive abilities, and specifically g, have consistently demonstrated stability over time. Reference Breit, Scherrer, Tucker-Drob and Preckel15 While intelligence has been shown to be the most powerful predictor of school performance, how intelligence is defined matters. Reference Lozano-Blasco, Quílez-Robres, Usán, Salavera and Casanovas-López16 Another form of intelligence that plays an important role in academic outcomes is emotional intelligence. Reference Puertas-Molero, Ortega, Chacón Cuberos and Castro-Sánchez17 Emotional intelligence is defined as an individual’s capacity to understand, regulate, and act appropriately upon their own emotions and understand those of others. Reference Bar-On6,Reference Killgore, Smith and Olson18 Emotional intelligence in children can be developed through environmental influences, including school-based interventions and parental involvement. Reference Ozal, Ambrosini and Biolcati19,Reference Durlak, Weissberg, Dymnicki, Taylor and Schellinger20 The Emotional Quotient Inventory: Youth Version, developed by Bar-On and Parker, is a widely used, psychometrically validated measure that assesses multiple domains of emotional intelligence in adolescents. Reference Bar-On6
Despite the known neurodevelopmental differences for children with CHD, emotional intelligence has not been systematically evaluated in this population. This has left a critical gap in understanding emotional functioning and potential clinical correlates. In this study, emotional intelligence was evaluated using the Emotional Quotient Inventory: Youth Version in a cohort of children with CHD, and associations were made with key demographics and clinical characteristics.
The goals of this pilot project were to characterise emotional intelligence in children with CHD, identify demographic, clinical, surgical, and social predictors of variation in emotional intelligence, and determine the need for incorporation of a focused emotional intelligence assessment into the neurodevelopmental battery for children with CHD.
Materials and methods
Study design, enrolment, & selected assessments
This prospective, single-centre, cross-sectional study included paediatric CHD patients seen in the outpatient clinics at Arnold Palmer Hospital for Children. The study was approved by the Institutional Review Boards of Orlando Health and the University of Central Florida. Informed consent was obtained from parents or legal guardians and assent from patients where applicable. Eligible patients were screened and tested between October 2015 and February 2020. Each family received a nominal gift card as compensation for time and travel expenses. Clinical data and demographic information were obtained from patient medical records. In addition, the parent or legal guardian completed a study questionnaire.
The study population included English-speaking patients aged 7–17 years with a confirmed CHD diagnosis and without moderate-to-severe developmental delay. Patients within this age range were excluded if they were unable to complete study evaluations for any reason, including having a reading level at or below the 3rd grade level. Reading ability was assessed using the Woodcock-Munoz Language Survey-Revised, Test 3: Letter-Word Identification. Reference Woodcock, Munoz-Sandoval, Ruef and Alvarado21,Reference Woodcock, Munoz-Sandoval, Ruef and Alvarado22 The cutoff was selected to ensure participants met the Emotional Quotient Inventory: Youth Version testing requirement of a minimum 4th-grade reading level. All races, ethnicities, and sexes were eligible for inclusion. Initially, 273 patients were eligible and expressed interest. Non-compliance with the scheduled appointment or with the testing protocol and/or examiner scheduling conflicts resulted in 98 patients being screened. Of those, 67 patients met the reading level inclusion criteria and completed the emotional intelligence test.
Cognitive ability was assessed using the Wechsler Abbreviated Scale of Intelligence, Second Edition, full-scale IQ two-subtest format. All assessments were administered by an evaluator trained by a neuropsychologist. The Wechsler Abbreviated Scale of Intelligence, Second Edition, full-scale IQ two-subtest format is an individually administered assessment standardised based on patient age. The two-subtest version (vocabulary and matrix reasoning) was administered due to time constraints. Instructions were read to each examinee for each subtest, and the test administrator recorded responses on the accompanying answer booklet. A final composite score, in the full-scale IQ two-subtest format, was determined for every participant. The test is standardised to a mean score of 100 with a standard deviation of 15. Full-scale IQ two-subtest format scores were calculated according to the test administration and scoring manual. Reference Wechsler23 The scores were then verified by two test administrators to check for internal consistency. Scores determined as inconsistent resulted in participant exclusion from the study.
Patients then independently completed the Bar-On Emotional Quotient Inventory: Youth Version, a 60-item, self-report questionnaire that uses a 1–4 Likert scale and is standardised by patient age and sex. Reference Bar-On6 This test provides a total Emotional Quotient Inventory: Youth Version score (EQtotal) and five subscores: (1) intrapersonal, (2) interpersonal, (3) adaptability, (4) stress-management, and (5) general mood. All scores are standardised to a mean of 100 and a standard deviation of 15. The Emotional Quotient Inventory: Youth Version also generates an inconsistency index (flagged scores > 10) and a positive impression score (flagged scores > 130), which are quantitative measures of random answering and response bias, respectively. For flagged assessments, study personnel reviewed item-level responses and made score adjustments when appropriate for participants aged 7–9. Participants were excluded if they demonstrated random responding or had an inconsistency index >13. In cases of uncertainty, participants and test responses were excluded at the discretion of neuropsychologists.
The accompanying parent(s) or legal guardian(s) were asked to complete the Behaviour Assessment for Children, Second Edition Parental Rating Scale form and a study-specific, biopsychosocial questionnaire. These forms were administered to acquire data on the patient’s behavioural, social, economic, and past medical history. The Behaviour Assessment for Children, Second Edition Parental Rating Scale child version was used for patients aged 7–11 years old, while the adolescent version was used for patients aged 12–21. Reference Reynolds and Kakmphaus8 The Parental Rating Scale uses a 4-choice Likert scale with 160 items for the child form and 150 items for the adolescent form. The Behaviour Assessment for Children, Second Edition also provides a validity index to ensure the quality of completed forms. The rating form provides 14 clinical scales that convert to 4 composite scales, as follows:
-
1. Externalising Problems: Hyperactivity, Aggression, Conduct Problems
-
2. Internalising Problems: Anxiety, Depression, Somatisation
-
3. Behavioural Symptoms Index: Atypicality, Withdrawal, Attention Problems
-
4. Adaptive Skills: Adaptability, Social Skills, Leadership, Activities of Daily Living, Functional Communication
For all composite scores in the Behaviour Assessment for Children, Second Edition, the mean score is 50 with a standard deviation of 10. Scores between 60 and 69 for Externalising Problems, Internalising Problems, and Behavioural Symptoms Index are indicative of at-risk behaviours, while scores ≥70 are indicative of clinically significant findings. Adaptive skills composite scores ranging between 31 and 40 are indicative of at-risk findings, and scores ≤30 indicate clinically significant findings.
CHD diagnosis, complexity class, and STAT categories
The primary CHD diagnosis was used to assign each patient a CHD complexity class according to the Clancy et al. classification system. Reference Clancy, McGaurn and Wernovsky24 This classification system stratifies lesions into four classes, each associated with increasing mortality risk. Class 1 includes patients with two ventricles and no arch obstruction, Class 2 includes those with two ventricles and arch obstruction, Class 3 consists of patients with one ventricle and no arch obstruction, and Class 4 includes patients with one ventricle and arch obstruction. Diagnoses included in Class 1 include simple atrial septal defects, ventricular septal defects, transposition of great arteries, and tetralogy of Fallot, among others, while those included in Class 4 include primarily hypoplastic left heart syndrome. Operation-related information included operation in infancy, primary cardiac operation, the total number of cardiac procedures required, and the use of cardiopulmonary bypass, deep hypothermic circulatory arrest, or selective cerebral perfusion. For cardiac operations, the Society of Thoracic Surgeons - European Association for Cardio-Thoracic Surgery Congenital Heart Surgery Mortality Categories (STAT Categories) were also recorded. Reference OBrien, Clarke and Jacobs25–Reference Kumar, Gaynor and Heuerman27 The STAT Category 2023 update was utilised.
Risk factors and associated outcomes
The following factors were abstracted from patient medical records and parent questionnaire responses and included as potential risk factors: patient sex, presence of chromosomal abnormality or genetic syndrome, premature birth (<37 weeks gestation), cardiac surgery performed prior to 2 years of age, CHD severity Class 3 or 4, cyanotic heart defect, operations requiring cardiopulmonary bypass, operations requiring deep hypothermic circulatory arrest or selective cerebral perfusion, STAT Category 4 or 5, the social vulnerability index, multilingualism (fluency in 2+ languages), and maternal and/or paternal level of education. The social vulnerability index is a score based on geographical region and zip code that reflects census data in four composite categories: socioeconomic status, household characteristics, racial and ethnic minority status, and housing type and transportation. 28 Socioeconomic status includes information regarding being below 150% of the poverty level, unemployment, housing cost burden, having no high school diploma, and having no health insurance. The household characteristics category reflects if there are people in the home aged 65+, 17 or younger, a civilian with a disability, single-parent households, and English language proficiency. The housing type & transportation category includes multi-unit structures, mobile homes, crowding, no vehicle, and group quarters. The social vulnerability index score is assigned per community rather than per individual household. Outcome variables used in this study include patient history of physical therapy or a diagnosis of attention deficit hyperactivity disorder as defined by the Diagnostic and Statistical Manual, Fifth Edition. 29
Statistical analysis
All statistical testing was performed using IBM SPSS 30.0.0.0. Descriptive statistics, including mean, standard deviation, and interquartile ranges, are reported for all variables. A two-tailed t-test was used for univariate analysis to determine significance in the difference between EQtotal and all subscores in the CHD cohort and a standard population with a normative mean and standard deviation of 100 ± 15. A one-way ANOVA test with a Bonferroni post-hoc adjustment was used for univariate analysis on those risk factors with three or more distinct groups, including Clancy CHD severity and the social vulnerability index. The association between EQtotal and STAT score was evaluated using univariable regression with STAT considered an ordinal variable. Multivariable linear regression was conducted with risk factors and outcomes demonstrating a p-value < 0.1 in the univariate analysis. A p-value < 0.05 was considered significant for multivariable regression analysis.
Results
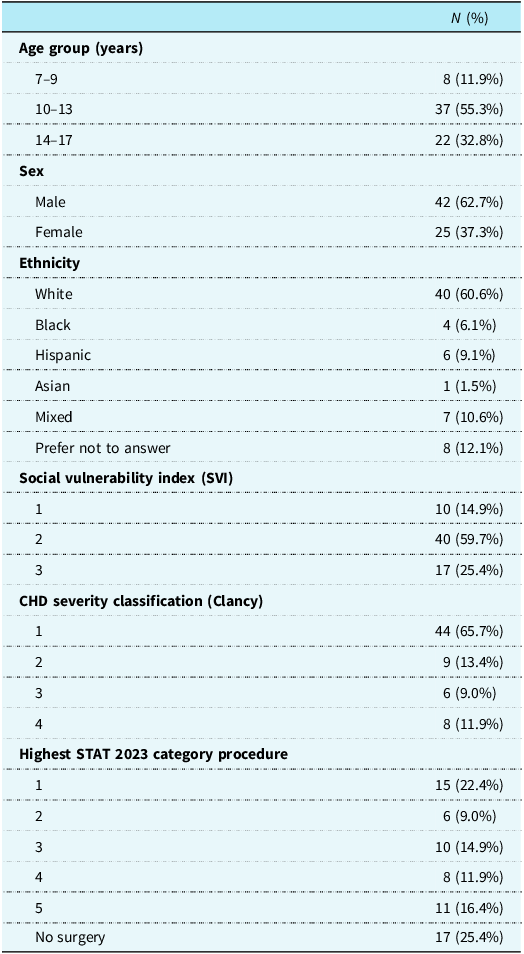
A total of 67 patients met the inclusion criteria and completed the required assessments. The patient demographics and characteristics are detailed in Table 1. The social vulnerability index captures many demographic variables, but a detailed breakdown of additional demographic information included within this category is seen in Supplemental Table 1. Table 1 additionally depicts the cohort’s CHD severity and procedural complexity.
Patient demographics and characteristics

The risk factors and associated outcomes extracted from the patient’s medical records and parental questionnaires are shown in Supplemental Table 2. The most common risk factors in this population were surgical risk factors, including undergoing surgery between birth and 2 years of age (N = 46, 68.7%) and requiring cardiopulmonary bypass during any surgery (N = 49, 74.2%).
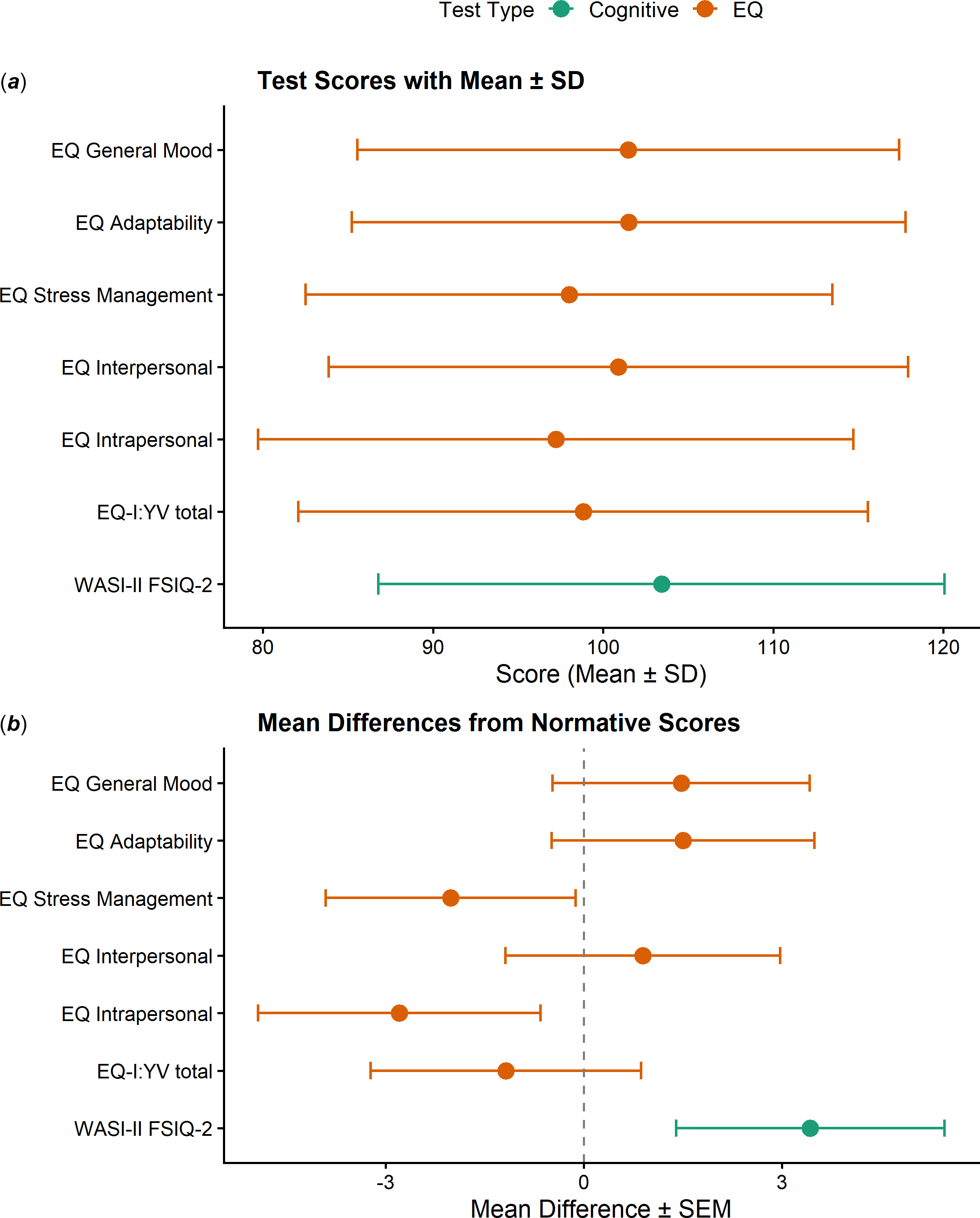
The primary outcomes assessed are the cognitive, behavioural, and EQ testing results, indicated by the Wechsler Abbreviated Scale of Intelligence, Second Edition, full-scale IQ two-subtest format, the Behaviour Assessment for Children, Second Edition, and the Emotional Quotient Inventory: Youth Version, respectively. The mean and standard deviation for all testing scores are shown in Figure 1( a ). Figure 1( b ) shows the mean of differences and standard error of the mean for cognitive and EQ testing. Numerical scores with p-values are found in Supplemental Table 3. The mean Behaviour Assessment for Children, Second Edition composite scores were within the normal range.
(a) EQ-I:YV and WASI-II testing scores summary. (b) EQ-I:YV and WASI-II testing scores mean differences and standard error of mean.

Figures 2( a ) and ( b ) stratify the EQtotal (“Total EQ” in the table) and subscores by STAT category and CHD severity, respectively. There was a near significant difference via one-way ANOVA in EQtotal between CHD severity categories (p = 0.088) as well as a near-significant difference in EQ stress management subscore between CHD severity categories (p = 0.055). Those in CHD class 3 scored on average 19.22 points lower in the EQ stress category (p = 0.104).
(a) EQ subscore and total score mean and standard deviation stratified by STAT category. (b) EQ subscore and total score mean and standard deviation stratified by CHD severity category.

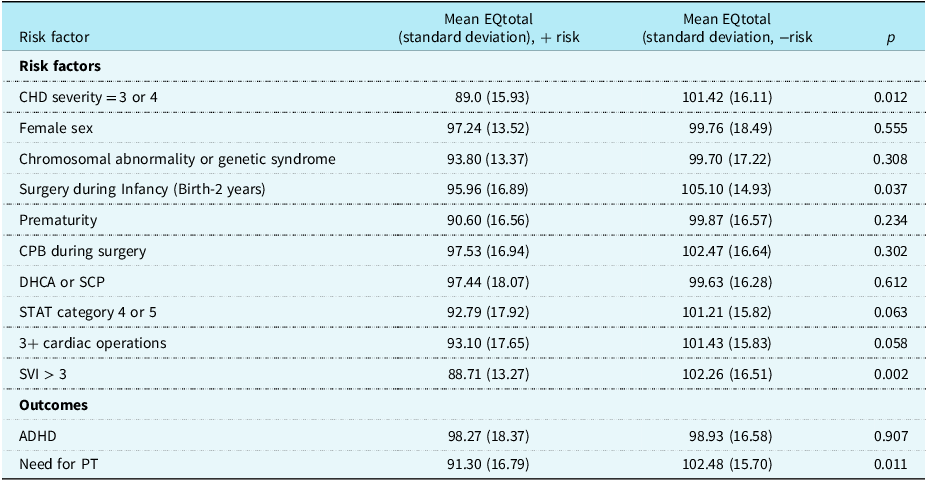
Table 2 illustrates the univariate analysis comparing the mean and standard deviation of EQtotal based on the presence or absence of each risk factor or associated outcome. An independent t-test was utilised for each risk factor and associated outcome, and the significance (p-value) of each test is reported. All risk factors with p < 0.1 were included in the multivariable linear regression model; thus, the CHD severity score of 3 or 4, surgery during infancy, social vulnerability index > 3, a STAT category > 4, and having 3+ cardiac operations were entered as potential predictors of EQtotal. Table 3 depicts the results of the multivariable linear regression. The coefficient of determination, R 2, was 0.251, indicating that 25.1% of the variability in the EQtotal score may be explained by the risk factors included. A one-way ANOVA demonstrated that EQtotal significantly decreases as social vulnerability index rises from category 1 to 3 (p < 0.001).
Univariate risk factor and associated outcome analysis

Multivariate linear regression of risk factors

The association between the aforementioned risk factors and the EQ subscores was also investigated. Risk factors significantly associated with variation in the EQ stress management subscore include CHD severity of 3 or 4 (mean difference 11.54, p = 0.012), surgery during infancy (mean difference 7.86, p = 0.053), STAT category of 4 or 5 (mean difference 9.309, p = 0.025), 3+ cardiac operations (mean difference 8.86, p = 0.029), and social vulnerability index > 3 (mean difference 8.41, p = 0.052). Those associated with EQ adaptability include CHD severity of 3 or 4 (mean difference 10.57, p = 0.03), surgery during infancy (mean difference 11.68, p = 0.06), and social vulnerability index > 3 (mean difference 12.27, p = 0.006). Female sex (mean difference −8.972, p = 0.036) and social vulnerability index > 3 (mean difference 11.99, p = 0.011) were significantly associated with interpersonal EQ. There were no significant risk factors associated with intrapersonal EQ or general mood EQ subscore.
A separate univariate analysis and subsequent multivariable linear regression were conducted to determine potential risk factors predicting variation in the Wechsler Abbreviated Scale of Intelligence, Second Edition, full-scale IQ two-subtest format score. An independent t-test was performed for the same potential risk factors included in Table 2. Those risk factors with p < 0.1 in the univariate analysis include cardiopulmonary bypass during surgery (p = 0.022), deep hypothermic circulatory arrest or selective cerebral perfusion during surgery (p = 0.004), chromosomal abnormality or genetic syndrome (p = 0.003), surgery during infancy (p = 0.074), and prematurity (p = 0.050). In the multivariable linear regression (R 2 = 0.327), the presence of a chromosomal abnormality or genetic syndrome (β = −17.085, p = 0.001), prematurity (β = −15.910, p = 0.032), and use of deep hypothermic circulatory arrest or selective cerebral perfusion (β = −14.820, p = 0.001) were significant predictors of the Wechsler Abbreviated Scale of Intelligence, Second Edition, full-scale IQ two-subtest format.
Similarly, a univariate analysis using t-tests and a multivariable linear regression were performed for each of the Behaviour Assessment for Children, Second Edition composite subscores, to determine risk factors and outcomes impacting the Behaviour Assessment for Children, Second Edition score in this population. For externalising problems, attention deficit hyperactivity disorder was the only significant outcome (p = 0.04) in the univariate analysis. For both internalising problems and adaptive skills, numerous risk factors met the threshold of p < 0.1 and were included in the multivariable linear regression; however, no risk factors were found to be significant predictors of altered scores. For the BSI score, presence of a chromosomal abnormality or genetic syndrome, attention deficit hyperactivity disorder, and use of cardiopulmonary bypass had p < 0.1 on the univariate and were included in the multivariable regression. In the multivariable regression (R 2 = 0.187), only attention deficit hyperactivity disorder was a significant predictor of higher Behaviour Assessment for Children, Second Edition BSI scores (β = 10.229, p = 0.007).
Discussion
The aim of this study was to investigate the association between emotional intelligence and CHD using the Emotional Quotient Inventory: Youth Version test and examine risk factors associated with variations in emotional intelligence. While no significant differences were observed between both the EQtotal and EQ subscores in CHD patients compared to the test’s normative means, important differences emerged when stratified by CHD risk factors. A CHD severity score of 3 or 4 (i.e., those with single-ventricle physiology) and a social vulnerability index greater than 3 were the two most significant risk factors, associated with clinically meaningful decreases in the total EQ score of 15.83 points and 14.11 points, respectively, compared to norms. Additionally, several risk factors investigated were found to be significantly associated with declines in the stress management and adaptability of EQ subscore. These findings suggest that in patients with CHD, emotional intelligence is influenced by a complex interplay of anatomic/physiologic, neurodevelopmental, and environmental factors.
Identifying the risk factors altering emotional intelligence in patients with CHD is an important preliminary step enabling early intervention for children and families. The social vulnerability index significantly impacts the total EQ score as well as several EQ subscores, suggesting that environmental factors may exert a greater influence on emotional intelligence development than surgical risk factors alone. In contrast, the stress management subscore was more impacted by surgical risk factors, suggesting that increased cardiac interventions may impair stress regulation. Campbell et al. highlighted the need to incorporate stress management training to assist children and parents in coping with cardiac catheterisation, which can be translatable to numerous types of cardiac interventions. Reference Campbell, Clark and Kirkpatrick30 Collectively, these findings underscore the importance of providing resources for stress management at an early stage.
While the current recommended neurodevelopmental battery in patients with CHD assesses a broad range of outcomes, it lacks a comprehensive emotional intelligence assessment. Lower emotional intelligence has been associated with increased stress, anxiety, depression, substance abuse, and suicide, whereas higher emotional intelligence correlates with positive emotional states, healthier coping strategies, the ability to maintain meaningful relationships, and a substantial impact on academic and career performance. Reference Domínguez-García and Fernández-Berrocal31–Reference Sánchez-Álvarez, Berrios Martos and Extremera33 Patients with CHD experience reduced health-related quality of life and higher rates of comorbid neurodevelopmental disorders. Reference Rometsch, Greutmann and Latal34 Emotional intelligence is a modifiable construct supported by the neuroplasticity of emotional and cognitive networks; thus, it is necessary to provide children with a framework to manage emotional challenges.
Significant overlap between emotional intelligence and other neurodevelopmental outcomes commonly associated with CHD patients, such as attention deficit hyperactivity disorder, may convolute findings in the social and emotional domains; however, no significant association was found between Emotional Quotient Inventory: Youth Version scores and the presence of diagnosed attention deficit hyperactivity disorder in this population. Reference Campbell, Clark and Kirkpatrick30 The presence of diagnosed attention deficit hyperactivity disorder was, however, found to significantly impact components of the Behaviour Assessment for Children, Second Edition scores. The risk factors associated with decreased EQ scores in this population were not identified as risk factors for increased Behaviour Assessment for Children, Second Edition scores, indicating that the Behaviour Assessment for Children, Second Edition and Emotional Quotient Inventory: Youth Version assessments are assessing distinct and critically different components of neurodevelopment. The Behaviour Assessment for Children, Second Edition is a comprehensive instrument designed to evaluate a broad range of behavioural and psychiatric conditions, including attention deficit hyperactivity disorder, and is well suited for diagnostic screening. In contrast, the Emotional Quotient Inventory: Youth Version is a narrow-band measure designed to screen for emotional intelligence, identify developmental strengths and weaknesses in social skills, and measure the impact of counselling or interventions. Reference Bar-On6 As such, the Emotional Quotient Inventory: Youth Version may provide a complementary perspective on neurodevelopment that is not captured by traditional behavioural assessments. Given the increasing emphasis on social-emotional learning within educational systems, the Emotional Quotient Inventory: Youth Version may serve as a valuable tool for identifying areas of vulnerability to target with interventions involving parents, educators, and structured school-based programmes, as well as for monitoring response to intervention over time. As a pilot study, these findings highlight the potential role of emotional intelligence assessment in expanding current neurodevelopmental evaluation frameworks in children with CHD.
Emotional regulation, a core component of emotional intelligence, has been shown to significantly influence executive functioning. Reference Koay and Van Meter35 Individuals with complex CHD frequently exhibit neurocognitive and neurodevelopmental impairments, including deficits in executive functioning and social cognition, which can adversely affect academic and social outcomes. Reference Opotowsky, Allen and Bucholz36 Performance-based models suggest that emotional intelligence represents a distinct construct that interfaces with, but remains separable from, general cognitive abilities. Reference Abda, Bolduc and Tsimicalis4,Reference Davis and Wigelsworth7,Reference Bru-Luna, Martí-Vilar, Merino-Soto and Cervera-Santiago12 In this study, biologic and surgical risk factors were associated with lower cognitive scores, whereas lower Emotional Quotient Inventory: Youth Version scores were more strongly associated with environmental and modifiable factors. This divergence supports the notion that emotional intelligence and cognition are distinct but overlapping neurodevelopmental domains and suggests that, in contrast to emotional intelligence, cognitive function may be more influenced by early physiologic factors such as cerebral perfusion.
While this study represents a unique evaluation of the neurodevelopmental outcomes in CHD patients, there are multiple limitations. The sample size was limited by the requirement of patients to complete the Emotional Quotient Inventory: Youth Version independently and without assistance—resulting in the exclusion of patients with moderate-to-severe neurodevelopmental deficits—the administration of testing only in English, and the requirement of a minimum 4th grade reading level, thus reducing the statistical power and generalisability of the study. The cross-sectional nature of this study prevents a longitudinal assessment of emotional intelligence in this patient population, which may show modification of Emotional Quotient Inventory: Youth Version scores according to changes in their environment and development. Lastly, it remains challenging to disentangle the effects on emotional intelligence of CHD specifically from those of having a chronic medical condition in general (with its attendant multiple hospitalisations, interventions, and medical disability).
Conclusion
These findings suggest that emotional intelligence is a unique element of neurodevelopmental vulnerability in patients with CHD, rather than a sequela or constituent of other neurodevelopmental domains and deficits attributable to CHD, which ultimately impacts a patient’s perception, understanding and regulation of emotions and alters numerous social, emotional and behavioural aspects of their life. The severity of a child’s CHD lesion and the social vulnerability index are the primary factors contributing to up to 25% of the variability in emotional intelligence scores in these patients. These risk factors differ from those for cognitive and behavioural testing, further supporting emotional intelligence as a distinct neurodevelopmental domain. The addition of a specific tool to evaluate emotional intelligence in children with CHD may enable children, their healthcare team, and their families to actively modify this domain and improve their quality of life.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951126113857.
Acknowledgements
Ricardo Argueta-Morales, MD, Orlando Health, Research Associate; Nannette, McKinney, BS, Orlando Health CRC; Karen Iacono, ARNP, Orlando Health; Lisa Gibbons, PhD, Orlando Health; Lindsay Shaw, MD, Orlando Health; Ana Leon, PhD, UCF Faculty; Tiffany Chan, UCF Medical Student; Ramone Eldemire, UCF Medical Student; Jennifer Ruiz, UCF Medical Student; Kevin Petersen, UCF Medical Student; Morgan Irwin-Weyant, UCF Medical Student; Paola Rodriguez Morales, UCF Medical Student; John D’Angelo, UCF Medical Student; Alexis Ghersi, UCF Undergraduate Student Intern; Sonia Amirzadeh, UCF Undergraduate Student Intern
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare none.





 Open access
Open access